
A Cohort Study on Cancer Incidence among Women Exposed to Environmental Asbestos in Childhood with a Focus on Female Cancers, including Breast Cancer

 and
and
Abstract
1. Introduction
2. Materials and Methods
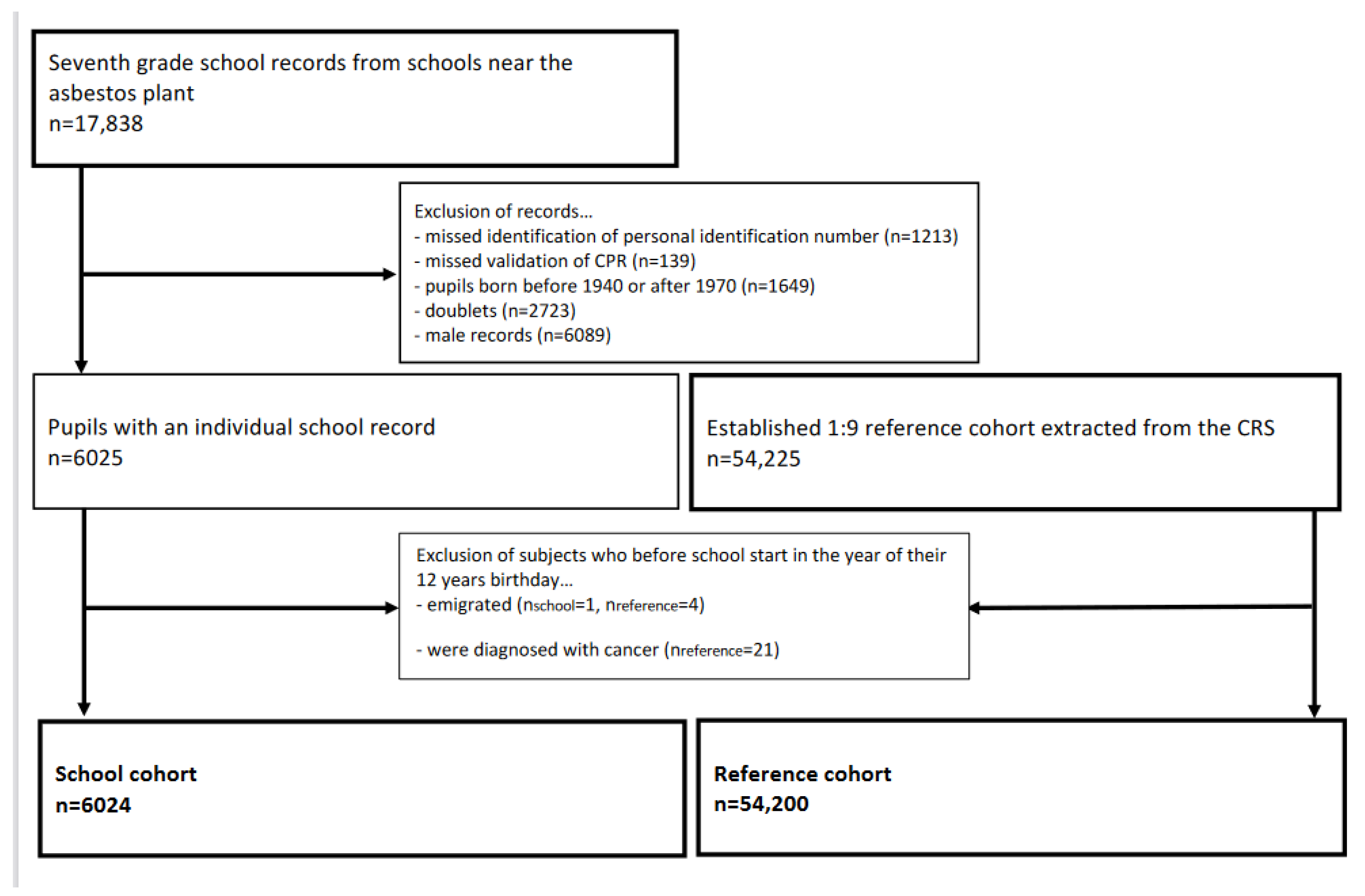
2.1. Population
2.2. Asbestos Exposure
2.3. Cancer
2.4. Smoking
2.5. Statistical Analysis
3. Results
3.1. Cancer Incidence Ratios
3.2. Hazard Ratios
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Frank, A.L.; Joshi, T.K. The global spread of asbestos. Ann. Glob. Health 2014, 80, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Selikoff, I.J.; Churg, J.; Hammond, E.C. Landmark article April 6, 1964: Asbestos exposure and neoplasia. By Irving J. Selikoff, Jacob Churg, and E. Cuyler Hammond. JAMA 1984, 252, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Stayner, L.; Welch, L.S.; Lemen, R. The worldwide pandemic of asbestos-related diseases. Annu. Rev. Public Health 2013, 34, 205–216. [Google Scholar] [CrossRef] [PubMed]
- Newhouse, M.L.; Berry, G.; Wagner, J.C.; Turok, M.E. A study of the mortality of female asbestos workers. Br. J. Ind. Med. 1972, 29, 134–141. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Goswami, E.; Craven, V.; Dahlstrom, D.L.; Alexander, D.; Mowat, F. Domestic asbestos exposure: A review of epidemiologic and exposure data. Int. J. Environ. Res. Public Health 2013, 10, 5629–5670. [Google Scholar] [CrossRef]
- Dalsgaard, S.B.; Würtz, E.T.; Hansen, J.; Røe, O.D.; Omland, Ø. Environmental asbestos exposure in childhood and risk of mesothelioma later in life: A long-term follow-up register-based cohort study. Occup. Environ. Med. 2019, 76, 407–413. [Google Scholar] [CrossRef]
- Reid, A.; Heyworth, J.; de Klerk, N.; Musk, A.W. The mortality of women exposed environmentally and domestically to blue asbestos at Wittenoom, Western Australia. Occup. Environ. Med. 2008, 65, 743–749. [Google Scholar] [CrossRef]
- Kurumatani, N.; Kumagai, S. Mapping the risk of mesothelioma due to neighborhood asbestos exposure. Am. J. Respir. Crit. Care Med. 2008, 178, 624–629. [Google Scholar] [CrossRef]
- Goldberg, S.; Rey, G.; Luce, D.; Gilg Soit Ilg, A.; Rolland, P.; Brochard, P.; Imbernon, E.; Goldberg, M. Possible effect of environmental exposure to asbestos on geographical variation in mesothelioma rates. Occup. Environ. Med. 2010, 67, 417–421. [Google Scholar] [CrossRef]
- Panou, V.; Vyberg, M.; Meristoudis, C.; Hansen, J.; Bogsted, M.; Omland, O.; Weinreich, U.M.; Roe, O.D. Non-occupational exposure to asbestos is the main cause of malignant mesothelioma in women in North Jutland, Denmark. Scand. J. Work. Environ. Health 2019, 45, 82–89. [Google Scholar] [CrossRef]
- World Health Organization, International Agency for Research on Cancer. Arsenic, metals, fibres, and dusts. IARC Monogr. Eval. Carcinog. Risks Hum. 2012, 100, 11–465. [Google Scholar]
- Germani, D.; Belli, S.; Bruno, C.; Grignoli, M.; Nesti, M.; Pirastu, R.; Comba, P. Cohort mortality study of women compensated for asbestosis in Italy. Am. J. Ind. Med. 1999, 36, 129–134. [Google Scholar] [CrossRef]
- Reid, A.; Segal, A.; Heyworth, J.S.; de Klerk, N.H.; Musk, A.W. Gynecologic and breast cancers in women after exposure to blue asbestos at Wittenoom. Cancer Epidemiol. Prev. Biomark. 2009, 18, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Brauer, C.; Baandrup, U.; Jacobsen, P.; Krasnik, M.; Olsen, J.H.; Pedersen, J.H.; Rasmussen, T.R.; Schlunssen, V.; Sherson, D.; Svolgaard, B.; et al. Screening for asbestos-related conditions. Ugeskr. Laeger 2009, 171, 433–436. [Google Scholar] [PubMed]
- Bianchi, C.; Bianchi, T.; Ramani, L. Malignant mesothelioma of the pleura among women. La Med. Del Lav. 2004, 95, 376–380. [Google Scholar]
- Langhoff, M.D.; Kragh-Thomsen, M.B.; Stanislaus, S.; Weinreich, U.M. Almost half of women with malignant mesothelioma were exposed to asbestos at home through their husbands or sons. Dan. Med. J. 2014, 61, A4902. [Google Scholar]
- Gjerstorff, M.L. The Danish Cancer Registry. Scand. J. Public Health 2011, 39, 42–45. [Google Scholar] [CrossRef]
- International Agency for Research on Cancer. Personal habits and indoor combustions. Volume 100 E. A review of human carcinogens. IARC Monogr. Eval. Carcinog. Risks Hum. 2012, 100, 1–538. [Google Scholar]
- Norgaard, M.; Ehrenstein, V.; Vandenbroucke, J.P. Confounding in observational studies based on large health care databases: Problems and potential solutions—A primer for the clinician. Clin. Epidemiol. 2017, 9, 185–193. [Google Scholar] [CrossRef]
- Varkey, A.B. Chronic obstructive pulmonary disease in women: Exploring gender differences. Curr. Opin. Pulm. Med. 2004, 10, 98–103. [Google Scholar] [CrossRef]
- Schmidt, M.; Schmidt, S.A.; Sandegaard, J.L.; Ehrenstein, V.; Pedersen, L.; Sorensen, H.T. The Danish National Patient Registry: A review of content, data quality, and research potential. Clin. Epidemiol. 2015, 7, 449–490. [Google Scholar] [CrossRef] [PubMed]
- Berry, G.; Newhouse, M.L.; Wagner, J.C. Mortality from all cancers of asbestos factory workers in east London 1933-80. Occup. Environ. Med. 2000, 57, 782–785. [Google Scholar] [CrossRef] [PubMed]
- Pira, E.; Pelucchi, C.; Buffoni, L.; Palmas, A.; Turbiglio, M.; Negri, E.; Piolatto, P.G.; La Vecchia, C. Cancer mortality in a cohort of asbestos textile workers. Br. J. Cancer 2005, 92, 580–586. [Google Scholar] [CrossRef] [PubMed]
- Wignall, B.K.; Fox, A.J. Mortality of female gas mask assemblers. Br. J. Ind. Med. 1982, 39, 34–38. [Google Scholar] [CrossRef]
- Magnani, C.; Terracini, B.; Ivaldi, C.; Mancini, A.; Botta, M. Tumor mortality and from other causes in asbestos cement workers at the Casale Montferrato plant. La Med. Lav. 1996, 87, 133–146. [Google Scholar]
- Ferrante, D.; Bertolotti, M.; Todesco, A.; Mirabelli, D.; Terracini, B.; Magnani, C. Cancer mortality and incidence of mesothelioma in a cohort of wives of asbestos workers in Casale Monferrato, Italy. Environ. Health Perspect. 2007, 115, 1401–1405. [Google Scholar] [CrossRef]
- Magnani, C.; Dalmasso, P.; Biggeri, A.; Ivaldi, C.; Mirabelli, D.; Terracini, B. Increased risk of malignant mesothelioma of the pleura after residential or domestic exposure to asbestos: A case-control study in Casale Monferrato, Italy. Environ. Health Perspect. 2001, 109, 915–919. [Google Scholar] [CrossRef]
- Reid, A.; Franklin, P.; Olsen, N.; Sleith, J.; Samuel, L.; Aboagye-Sarfo, P.; de Klerk, N.; Musk, A.W. All-cause mortality and cancer incidence among adults exposed to blue asbestos during childhood. Am. J. Ind. Med. 2013, 56, 133–145. [Google Scholar] [CrossRef]
- Camiade, E.; Gramond, C.; Jutand, M.A.; Audignon, S.; Rinaldo, M.; Imbernon, E.; Luce, D.; Galateau-Salle, F.; Astoul, P.; Pairon, J.C.; et al. Characterization of a French series of female cases of mesothelioma. Am. J. Ind. Med. 2013, 56, 1307–1316. [Google Scholar] [CrossRef]
- Magnani, C.; Leporati, M. Mortality from lung cancer and population risk attributable to asbestos in an asbestos cement manufacturing town in Italy. Occup. Environ. Med. 1998, 55, 111–114. [Google Scholar] [CrossRef]
- Nordlund, L.A.; Carstensen, J.M.; Pershagen, G. Cancer incidence in female smokers: A 26-year follow-up. Int. J. Cancer 1997, 73, 625–628. [Google Scholar] [CrossRef]
- Malhotra, J.; Malvezzi, M.; Negri, E.; La Vecchia, C.; Boffetta, P. Risk factors for lung cancer worldwide. Eur. Respir. J. 2016, 48, 889–902. [Google Scholar] [CrossRef] [PubMed]
- Salvi, S.S.; Barnes, P.J. Chronic obstructive pulmonary disease in non-smokers. Lancet 2009, 374, 733–743. [Google Scholar] [CrossRef]
- Bianchi, C.; Giarelli, L.; Grandi, G.; Brollo, A.; Ramani, L.; Zuch, C. Latency periods in asbestos-related mesothelioma of the pleura. Eur. J. Cancer Prev. 1997, 6, 162–166. [Google Scholar]


{kind=link}
| School Cohort | Reference Cohort | ||||
|---|---|---|---|---|---|
| Characteristics | n | n | p-Value | ||
| Cohort size | 6024 | 54,200 | |||
| Birth year (%) | |||||
| 1940–1944 | 1190 | (19.8) | 10,707 | (19.8) | |
| 1945–1949 | 1452 | (24.1) | 13,067 | (24.1) | |
| 1950–1954 | 1335 | (22.2) | 12,008 | (22.2) | |
| 1955–1959 | 1071 | (17.8) | 9645 | (17.8) | |
| 1960–1964 | 754 | (12.5) | 6778 | (12.5) | |
| 1965–1970 | 222 | (3.7) | 1.995 | (3.7) | |
| Person years of follow-up | 297,637 | 2,583,877 | |||
| Median attained age (range) | 63.0 | (14.8–76.0) | 62.2 | (12.0–76.0) | 0.000 |
| Type of asbestos exposure (%) | 0.000 | ||||
| Environmental exposure (school cohort) and unknown asbestos exposure (reference cohort) | 4345 | (72.1) | 43,029 | (79.4) | |
| Occupational asbestos exposure | 138 | (2.3) | 1206 | (2.2) | |
| Familial occupational asbestos exposure | 1415 | (23.5) | 7753 | (14.3) | |
| Occupational and familial occupational asbestos exposure | 80 | (1.3) | 414 | (0.8) | |
| No employment history records | 46 | (0.8) | 1798 | (3.3) | |
| Proxy for smoking (%) | 355 | (5.9) | 2249 | (4.2) | 0.000 |
| School Cohort | Reference Cohort | ||||
|---|---|---|---|---|---|
| Characteristics | n | n | (%/Range) | p-Value | |
| Cancer cases * (% of all cohort) | 912 | (15.1) | 7991 | (14.7) | |
| Birth-year (%) | 0.523 | ||||
| 1940–1944 | 295 | (32.4) | 2530 | (31.7) | |
| 1945–1949 | 262 | (28.7) | 2493 | (31.2) | |
| 1950–1954 | 187 | (20.5) | 1502 | (18.8) | |
| 1955–1959 | 106 | (11.6) | 923 | (11.6) | |
| 1960–1964 | 50 | (5.5) | 466 | (5.8) | |
| 1965–1970 | 12 | (1.3) | 77 | (1.0) | |
| Median attained age (range) | 63.9 | (15.0–76.0) | 64.4 | (16.1–76.0) | 0.122 |
| Type of asbestos exposure (%) | 0.000 | ||||
| Environmental exposure (school cohort) and unknown asbestos exposure (reference cohort) | 672 | (73.7) | 6380 | (79.8) | |
| Occupational asbestos exposure | 23 | (2.5) | 209 | (2.6) | |
| Familial occupational asbestos exposure | 198 | (21.7) | 1277 | (16.0) | |
| Occupational and familial occupational asbestos exposure | 17 | (1.9) | 88 | (1.1) | |
| No Supplementary Pension Fund Register data | 2 | (0.2) | 37 | (0.5) | |
| Proxy for smoking (%) | 63 | (6.9) | 572 | (7.2) | |
| Cancer Site | O/E | SIR | 95% CI |
|---|---|---|---|
| External female genital organs and vagina | 11/6.48 | 1.70 | 0.94 to 3.06 |
| Other and unspecified female genital organs | 1/0.23 | 4.39 | 0.62 to 31.14 |
| Breast | 343/348.30 | 0.98 | 0.89 to 1.09 |
| Ovary, fallopian tube and broad ligament | 34/46.94 | 0.72 | 0.52 to 1.01 |
| Cervix uteri | 50/45.23 | 1.11 | 0.84 to 1.46 |
| Corpus uteri | 61/47.18 | 1.29 | 1.01 to 1.66 |
| Mesothelioma | 6/0.83 | 7.26 | 3.26 to 16.15 |
| Lung, bronchus and trachea | 121/109.28 | 1.11 | 0.93 to 1.32 |
| Cancer Site | External Female Genital Organs and Vagina (n = 66) | ||||
|---|---|---|---|---|---|
| n | Hazard Ratio | (95% CI) | p Value | ||
| Environmental asbestos exposure | 11 | 1.74 | (0.91–3.34) | 0.091 | |
| Familial occupational asbestos exposure | 12 | - | - | - | |
| Occupational asbestos exposure | 3 | - | - | - | |
| Proxy for smoking | 6 | - | - | - | |
| Cancer site | Breast (n = 3353) | ||||
| n | Hazard ratio | (95% CI) | p Value | ||
| Environmental asbestos exposure | 343 | 1.00 | (0.89–1.12) | 0.987 | |
| Familial occupational asbestos exposure | 574 | 1.07 | (0.98–1.17) | 0.145 | |
| Occupational asbestos exposure | 127 | 1.03 | (0.86–1.23) | 0.747 | |
| Proxy for smoking | 191 | 0.91 | (0.78–1.05) | 0.184 | |
| Cancer site | Ovary, fallopian tube and broad ligament (n = 438) | ||||
| n | Hazard ratio | (95% CI) | p Value | ||
| Environmental asbestos exposure | 34 | 0.76 | (0.54–1.08) | 0.130 | |
| Familial occupational asbestos exposure | 60 | 1.31 | (0.99–1.72) | 0.055 | |
| Occupational asbestos exposure | 15 | 0.25 | (0.15–0.41) | 0.000 | |
| Proxy for smoking | 22 | 0.89 | (0.58–1.37) | 0.593 | |
| Cancer site | Cervix uteri (n = 438) | ||||
| n | Hazard ratio | (95% CI) | p Value | ||
| Environmental asbestos exposure | 50 | 1.11 | (0.83–1.50) | 0.472 | |
| Familial occupational asbestos exposure | 78 | 1.08 | (0.85–1.39) | 0.525 | |
| Occupational asbestos exposure | 24 | 1.55 | (1.03–2.35) | 0.036 | |
| Proxy for smoking | 20 | 0.75 | (0.48–1.18) | 0.215 | |
| Cancer site | Corpus uteri (n = 474) | ||||
| n | Hazard ratio | (95% CI) | p Value | ||
| Environmental asbestos exposure | 61 | 1.32 | (1.02–1.75) | 0.045 | |
| Familial occupational asbestos exposure | 77 | 1.00 | (0.78–1.28) | 0.988 | |
| Occupational asbestos exposure | 16 | 0.91 | (0.55–1.50) | 0.713 | |
| Proxy for smoking | / | / | / | / | |
| Cancer site | Mesothelioma (n = 13) | ||||
| n | Hazard ratio | (95% CI) | p Value | ||
| Environmental asbestos exposure | 6 | 7.41 | (2.49–22.06) | 0.000 | |
| Familial occupational asbestos exposure | 1 | - | - | - | |
| Occupational asbestos exposure | 0 | - | - | - | |
| Proxy for smoking | / | / | / | / | |
| Cancer site | Lung, bronchus, and trachea (n = 1064) | ||||
| n | Hazard ratio | (95% CI) | p Value | ||
| Environmental asbestos exposure | 121 | 1.04 | (0.86–1.26) | 0.677 | |
| Familial occupational asbestos exposure | 216 | 1.23 | (1.06–1.43) | 0.007 | |
| Occupational asbestos exposure | 57 | 1.38 | (1.06–1.80) | 0.018 | |
| Proxy for smoking | 200 | 3.55 | (3.05–4.15) | 0.000 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dalsgaard, S.B.; Würtz, E.T.; Hansen, J.; Røe, O.D.; Omland, Ø. A Cohort Study on Cancer Incidence among Women Exposed to Environmental Asbestos in Childhood with a Focus on Female Cancers, including Breast Cancer. Int. J. Environ. Res. Public Health 2022, 19, 2086. https://doi.org/10.3390/ijerph19042086
Dalsgaard SB, Würtz ET, Hansen J, Røe OD, Omland Ø. A Cohort Study on Cancer Incidence among Women Exposed to Environmental Asbestos in Childhood with a Focus on Female Cancers, including Breast Cancer. International Journal of Environmental Research and Public Health. 2022; 19(4):2086. https://doi.org/10.3390/ijerph19042086
Chicago/Turabian StyleDalsgaard, Sofie Bünemann, Else Toft Würtz, Johnni Hansen, Oluf Dimitri Røe, and Øyvind Omland. 2022. "A Cohort Study on Cancer Incidence among Women Exposed to Environmental Asbestos in Childhood with a Focus on Female Cancers, including Breast Cancer" International Journal of Environmental Research and Public Health 19, no. 4: 2086. https://doi.org/10.3390/ijerph19042086
APA StyleDalsgaard, S. B., Würtz, E. T., Hansen, J., Røe, O. D., & Omland, Ø. (2022). A Cohort Study on Cancer Incidence among Women Exposed to Environmental Asbestos in Childhood with a Focus on Female Cancers, including Breast Cancer. International Journal of Environmental Research and Public Health, 19(4), 2086. https://doi.org/10.3390/ijerph19042086