
Comparing the activPAL CREA and GHLA Algorithms for the Classification of Postures and Activity in Free-Living Children



Abstract
1. Introduction
2. Materials and Methods
2.1. Data Processing
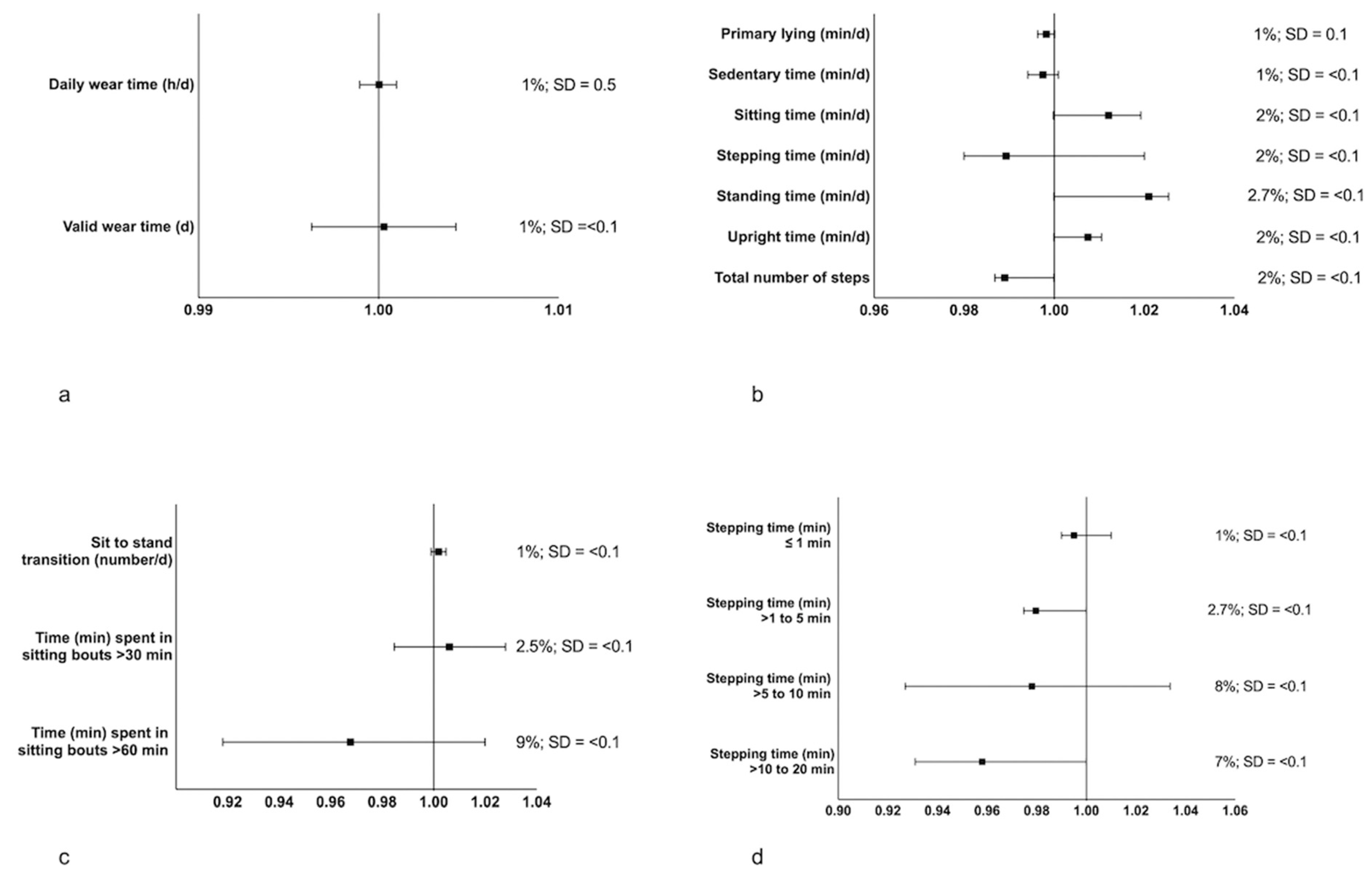
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Guidelines on Physical Activity and Sedentary Behaviour; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global Trends in Insufficient Physical Activity among Adolescents: A Pooled Analysis of 298 Population-Based Surveys with 1.6 Million Participants. Lancet Child Adolesc. Health 2020, 4, 23–35. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.M.; Altenburg, T.M.; Chinapaw, M.J.M. Sedentary Behavior Research Network (SBRN)–Terminology Consensus Project Process and Outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 75. [Google Scholar] [CrossRef] [PubMed]
- Biswas, A.; Oh, P.I.; Faulkner, G.E.; Bajaj, R.R.; Silver, M.A.; Mitchell, M.S.; Alter, D.A. Sedentary Time and Its Association with Risk for Disease Incidence, Mortality, and Hospitalization in Adults: A Systematic Review and Meta-Analysis. Ann. Intern. Med. 2015, 162, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Patterson, R.; McNamara, E.; Tainio, M.; de Sá, T.H.; Smith, A.D.; Sharp, S.J.; Edwards, P.; Woodcock, J.; Brage, S.; Wijndaele, K. Sedentary Behaviour and Risk of All-Cause, Cardiovascular and Cancer Mortality, and Incident Type 2 Diabetes: A Systematic Review and Dose Response Meta-Analysis. Eur. J. Epidemiol. 2018, 33, 811–829. [Google Scholar] [CrossRef] [PubMed]
- Chaput, J.-P.; Willumsen, J.; Bull, F.; Chou, R.; Ekelund, U.; Firth, J.; Jago, R.; Ortega, F.B.; Katzmarzyk, P.T. 2020 WHO Guidelines on Physical Activity and Sedentary Behaviour for Children and Adolescents Aged 5–17 Years: Summary of the Evidence. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 141. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, M.S.; Carson, V.; Chaput, J.-P.; Connor Gorber, S.; Dinh, T.; Duggan, M.; Faulkner, G.; Gray, C.E.; Gruber, R.; Janson, K.; et al. Canadian 24-Hour Movement Guidelines for Children and Youth: An Integration of Physical Activity, Sedentary Behaviour, and Sleep. Appl. Physiol. Nutr. Metab. 2016, 41, S311–S327. [Google Scholar] [CrossRef]
- Department of Health and Social Care. UK Chief Medical Officers’ Physical Activity Guidelines. 2019, 66p. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/832868/ukchief-medical-officers-physical-activity-guidelines.pdf (accessed on 10 September 2022).
- Australian Government. Physical Activity and Exercise Guidelines for All Australians. Available online: https://www.health.gov.au/health-topics/physical-activity-and-exercise/physical-activity-and-exercise-guidelines-for-all-australians (accessed on 1 September 2022).
- Chastin, S.F.M.; Dontje, M.L.; Skelton, D.A.; Čukić, I.; Shaw, R.J.; Gill, J.M.R.; Greig, C.A.; Gale, C.R.; Deary, I.J.; Der, G.; et al. Systematic Comparative Validation of Self-Report Measures of Sedentary Time against an Objective Measure of Postural Sitting (ActivPAL). Int. J. Behav. Nutr. Phys. Act. 2018, 15, 21. [Google Scholar] [CrossRef]
- Edwardson, C.L.; Winkler, E.A.H.; Bodicoat, D.H.; Yates, T.; Davies, M.J.; Dunstan, D.W.; Healy, G.N. Considerations When Using the ActivPAL Monitor in Field-Based Research with Adult Populations. J. Sport Health Sci. 2017, 6, 162–178. [Google Scholar] [CrossRef]
- Grant, P.M.; Ryan, C.G.; Tigbe, W.W.; Granat, M.H. The Validation of a Novel Activity Monitor in the Measurement of Posture and Motion during Everyday Activities. Br. J. Sports Med. 2006, 40, 992–997. [Google Scholar] [CrossRef]
- Sellers, C.; Dall, P.; Grant, M.; Stansfield, B. Validity and Reliability of the ActivPAL3 for Measuring Posture and Stepping in Adults and Young People. Gait Posture 2016, 43, 42–47. [Google Scholar] [CrossRef]
- Kozey-Keadle, S.; Libertine, A.; Lyden, K.; Staudenmayer, J.; Freedson, P.S. Validation of Wearable Monitors for Assessing Sedentary Behavior. Med. Sci. Sports Exerc. 2011, 43, 1561–1567. [Google Scholar] [CrossRef]
- Carlson, J.A.; Tuz-Zahra, F.; Bellettiere, J.; Ridgers, N.D.; Steel, C.; Bejarano, C.; LaCroix, A.Z.; Rosenberg, D.E.; Greenwood-Hickman, M.A.; Jankowska, M.M.; et al. Validity of Two Awake Wear-Time Classification Algorithms for ActivPAL in Youth, Adults, and Older Adults. J. Meas. Phys. Behav. 2021, 4, 151–162. [Google Scholar] [CrossRef] [PubMed]
- Courtney, J.B.; Nuss, K.; Lyden, K.; Harrall, K.K.; Glueck, D.H.; Villalobos, A.; Hamman, R.F.; Hebert, J.R.; Hurley, T.G.; Leiferman, J.; et al. Comparing the ActivPAL Software’s Primary Time in Bed Algorithm against Self-Report and van Der Berg’s Algorithm. Meas. Phys. Educ. Exerc. Sci. 2021, 25, 212–226. [Google Scholar] [CrossRef]
- Leister, K.R.; Garay, J.; Barreira, T. Validity of a Novel Algorithm to Detect Bedtime, Wake Time, and Sleep Time in Adults. J. Meas. Phys. Behav. 2022, 5, 76–84. Available online: https://journals.humankinetics.com/view/journals/jmpb/5/2/article-p76.xml (accessed on 5 September 2022). [CrossRef]
- Montoye, A.H.K.; Vondrasek, J.D.; Neph, S.E.; Basu, N.; Paul, L.; Bachmair, E.-M.; Stefanov, K.; Gray, S.R. Comparison of the ActivPAL CREA and VANE Algorithms for Characterization of Posture and Activity in Free-Living Adults. J. Meas. Phys. Behav. 2022, 5, 49–57. [Google Scholar] [CrossRef]
- Curran, F.; Dowd, K.P.; Peiris, C.L.; van der Ploeg, H.P.; Tremblay, M.S.; O’Donoghue, G. A Standardised Core Outcome Set for Measurement and Reporting Sedentary Behaviour Interventional Research: The CROSBI Consensus Study. Int. J. Environ. Res. Public. Health 2022, 19, 9666. [Google Scholar] [CrossRef] [PubMed]
- PAL Technologies Version History–PAL Knowledge Base. Available online: https://kb.palt.com/articles/palanalysis-version-history/ (accessed on 6 September 2022).
- McLellan, G.; Arthur, R.; Donnelly, S.; Bakshi, A.; Fairclough, S.J.; Taylor, S.L.; Buchan, D.S. Feasibility and Acceptability of a Classroom-Based Active Breaks Intervention for 8–12-Year Old Children. Res. Q. Exerc. Sport 2021, 93, 813–824. [Google Scholar] [CrossRef]
- DeShaw, K.J.; Ellingson, L.; Bai, Y.; Lansing, J.; Perez, M.; Welk, G. Methods for Activity Monitor Validation Studies: An Example with the Fitbit Charge. J. Meas. Phys. Behav. 2018, 1, 130–135. [Google Scholar] [CrossRef]
- Feito, Y.; Garner, H.; Bassett, D. Evaluation of ActiGraph’s Low-Frequency Filter in Laboratory and Free-Living Environments. Med. Sci. Sports Exerc. 2014, 47, 211–217. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Statistical Methods for Assessing Agreement between Two Methods of Clinical Measurement. Lancet Lond. Engl. 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Dixon, P.M.; Saint-Maurice, P.F.; Kim, Y.; Hibbing, P.; Bai, Y.; Welk, G.J. A Primer on the Use of Equivalence Testing for Evaluating Measurement Agreement. Med. Sci. Sports Exerc. 2018, 50, 837–845. [Google Scholar] [CrossRef]
- Buchan, D.S.; Boddy, L.M.; McLellan, G. Comparison of Free-Living and Laboratory Activity Outcomes from ActiGraph Accelerometers Worn on the Dominant and Non-Dominant Wrists. Meas. Phys. Educ. Exerc. Sci. 2020, 24, 247–257. [Google Scholar] [CrossRef]
- Buchan, D.S. Equivalence of Activity Outcomes Derived from Three Research Grade Accelerometers Worn Simultaneously on Each Wrist. J. Sports Sci. 2022, 40, 797–807. [Google Scholar] [CrossRef] [PubMed]
- Rowlands, A.V.; Plekhanova, T.; Yates, T.; Mirkes, E.M.; Davies, M.; Khunti, K.; Edwardson, C.L. Providing a Basis for Harmonization of Accelerometer-Assessed Physical Activity Outcomes Across Epidemiological Datasets. J. Meas. Phys. Behav. 2019, 2, 131–142. [Google Scholar] [CrossRef]
- O’Brien, M.W. Implications and Recommendations for Equivalence Testing in Measures of Movement Behaviors: A Scoping Review. J. Meas. Phys. Behav. 2021, 4, 353–362. [Google Scholar] [CrossRef]
- PAL Technologies Average Valid Day Summaries–PAL Knowledge Base. Available online: https://kb.palt.com/articles/average-valid-day-summaries/ (accessed on 25 October 2022).
- Dunstan, D.W.; Kingwell, B.A.; Larsen, R.; Healy, G.N.; Cerin, E.; Hamilton, M.T.; Shaw, J.E.; Bertovic, D.A.; Zimmet, P.Z.; Salmon, J.; et al. Breaking Up Prolonged Sitting Reduces Postprandial Glucose and Insulin Responses. Diabetes Care 2012, 35, 976–983. [Google Scholar] [CrossRef]
- Hadgraft, N.T.; Winkler, E.; Climie, R.E.; Grace, M.S.; Romero, L.; Owen, N.; Dunstan, D.; Healy, G.; Dempsey, P.C. Effects of Sedentary Behaviour Interventions on Biomarkers of Cardiometabolic Risk in Adults: Systematic Review with Meta-Analyses. Br. J. Sports Med. 2021, 55, 144–154. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Domain & Reporting Statistic | Outcome | CREA Algorithm | GHLA Algorithm | MPE ± SD | MAPE ± SD | ICC (95% CI) |
|---|---|---|---|---|---|---|
| Device Wear Time | Daily wear time (h/d) | 23.9 ± 0.5 | 23.9 ± 0.5 | −0.01 ± 0.37 | 0.02 ± 0.20 | 0.99 (0.99, 0.99) |
| Valid wear time days | 4.9 ± 1.5 | 4.9 ± 1.5 | −0.09 ± 0.33 | 0.40 ± 3.45 | 0.99 (0.99, 0.99) | |
| Posture Outcomes | Primary lying (min/d) | 606.6 ± 56.1 | 605.6 ± 57.1 | 0.16 ± 1.86 | 0.19 ± 1.50 | 0.99 (0.99, 0.99) |
| Sedentary time (min/d) | 515.6 ± 73.1 | 514.9 ± 77.7 | 0.13 ± 5.97 | 1.35 ± 2.57 | 0.99 (0.99, 0.99) | |
| Sitting time (min/d) | 347.3 ± 77.6 | 351.3 ± 78.8 | −1.13 ± 1.50 | 3.76 ± 6.14 | 0.98 (0.97, 0.98) | |
| Stepping time (min/d) | 132.7 ± 33.1 | 131.4 ± 33.1 | 1.00 ± 0.16 | 1.28 ± 1.87 | 0.99 (0.99, 0.99) | |
| Standing time (min/d) | 175.6 ± 50.1 | 179.8 ± 51.2 | −2.22 ± 4.24 | 3.43 ± 2.94 | 0.98 (0.97, 0.99) | |
| Upright time (min/d) | 308.3 ± 69.8 | 311.1 ± 71.9 | −0.86 ± 2.94 | 1.96 ± 2.02 | 0.99 (0.98, 0.99) | |
| Total number of steps | 10,587.2 ± 2780.7 | 10,481.6 ± 2784.9 | 1.01 ± 0.17 | 1.25 ± 2.00 | 0.99 (0.99, 0.99) | |
| Sitting bouts | Sit–stand transitions (number/d) | 92 ± 22 | 92 ± 22 | −0.22 ± 0.07 | 1.67 ± 2.01 | 0.99 (0.99, 0.99) |
| Time (min) spent in sitting bouts > 30 min | 92.9 ± 66.3 | 92.8 ± 66.3 | −0.70 ± 3.22 | 7.92 ± 16.92 | 0.94 (0.93, 0.96) | |
| Time (min) spent in sitting bouts > 60 min | 26.1 ± 44.3 | 25.7 ± 45.4 | 3.21 ± 0.96 * | 10.32 ± 29.37 | 0.96 (0.95, 0.97) | |
| Stepping bouts | Stepping time (min) ≤ 1 min | 82.6 ± 19.6 | 82.2 ± 19.6 | 0.41 ± 0.63 | 1.23 ± 1.85 | 0.99 (0.99, 0.99) |
| Stepping time (min) > 1 to 5 min | 39.1 ± 14.8 | 38.3 ± 15.1 | 1.61 ± 1.22 | 3.46 ± 4.57 | 0.99 (0.99, 0.99) | |
| Stepping time (min) > 5 to 10 min | 7.8 ± 7.3 | 7.8 ± 6.9 | 2.18 ± 8.76 † | 142.3 ± 287.1 | 0.78 (0.72, 0.83) | |
| Stepping time (min) > 10 to 20 min | 3.0 ± 4.6 | 2.8 ± 4.5 | 1.98 ± 4.50 ‡ | 2.58 ± 9.92 | 0.98 (0.97, 0.98) | |
| Stepping time (min) > 20 min | 0.3 ± 1.4 | 0.3 ± 1.4 | 0.26 ± 0.16 | 0.02 ± 0.31 | 0.97 (0.96, 0.98) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buchan, D.S.; Ugbolue, U.C. Comparing the activPAL CREA and GHLA Algorithms for the Classification of Postures and Activity in Free-Living Children. Int. J. Environ. Res. Public Health 2022, 19, 15962. https://doi.org/10.3390/ijerph192315962
Buchan DS, Ugbolue UC. Comparing the activPAL CREA and GHLA Algorithms for the Classification of Postures and Activity in Free-Living Children. International Journal of Environmental Research and Public Health. 2022; 19(23):15962. https://doi.org/10.3390/ijerph192315962
Chicago/Turabian StyleBuchan, Duncan S., and Ukadike C. Ugbolue. 2022. "Comparing the activPAL CREA and GHLA Algorithms for the Classification of Postures and Activity in Free-Living Children" International Journal of Environmental Research and Public Health 19, no. 23: 15962. https://doi.org/10.3390/ijerph192315962
APA StyleBuchan, D. S., & Ugbolue, U. C. (2022). Comparing the activPAL CREA and GHLA Algorithms for the Classification of Postures and Activity in Free-Living Children. International Journal of Environmental Research and Public Health, 19(23), 15962. https://doi.org/10.3390/ijerph192315962