
Clinically Meaningful Change in 6 Minute Walking Test and the Incremental Shuttle Walking Test following Coronary Artery Bypass Graft Surgery


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Participants
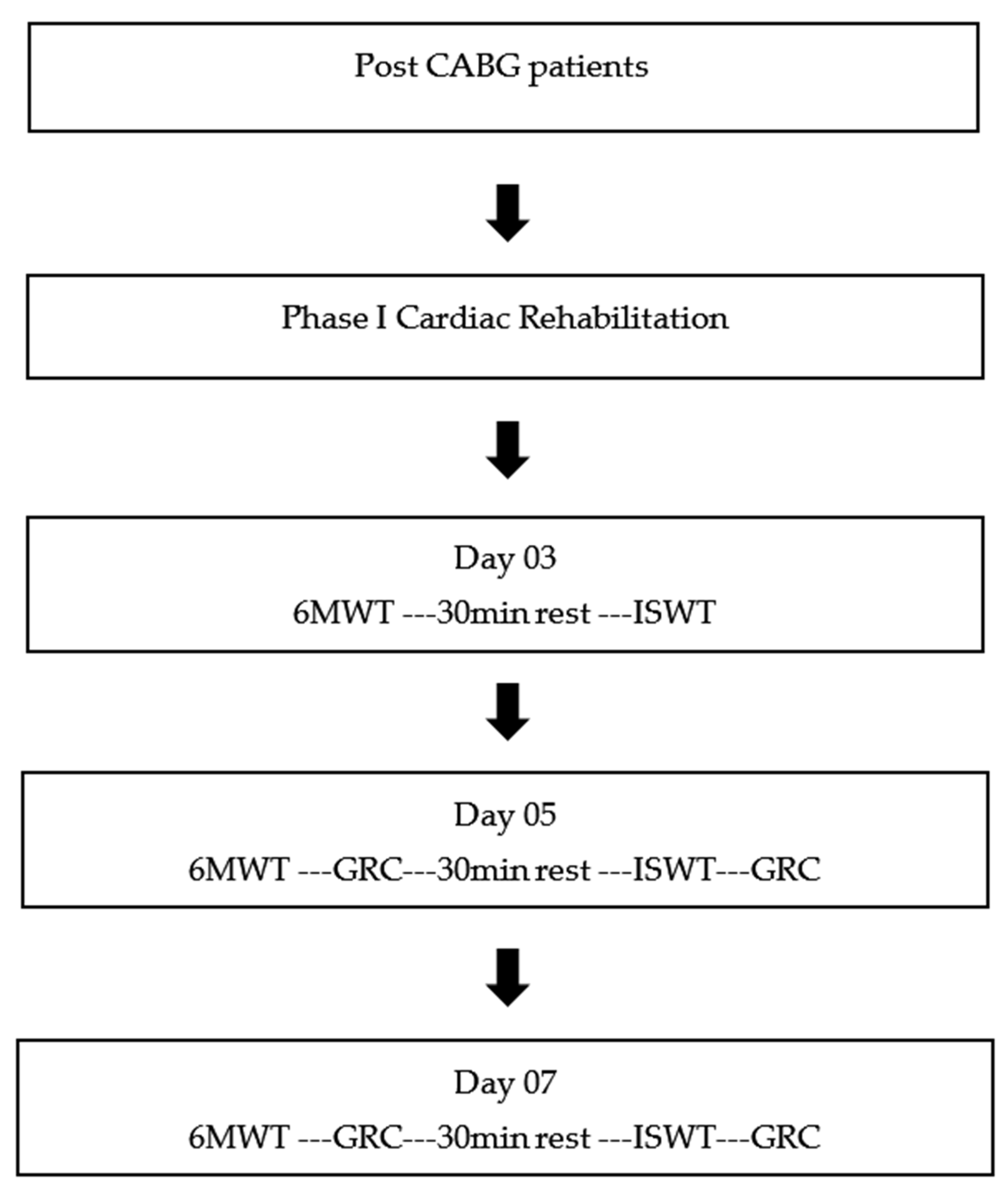
2.3. Protocol
2.4. Outcome Measures
2.4.1. 6 Min Walk Test
2.4.2. Incremental Shuttle Walk Test
2.5. Global Rating of Change—As an Anchor
2.6. Data Analysis
3. Results
3.1. Demographics/Patient Characteristics
3.2. 6 Minute Walk Test
3.2.1. MCID of 6MWT
Distribution-Based Estimation
Anchor-Based Estimation
3.3. Incremental Shuttle Walk Test
3.3.1. ISWT MCID
Distribution-Based Estimation
Anchor-Based Estimation
4. Discussion
4.1. MCID for 6MWT
4.2. MCID for ISWT
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Malakar, A.K.; Choudhury, D.; Halder, B.; Paul, P.; Uddin, A.; Chakraborty, S. A review on coronary artery disease, its risk factors, and therapeutics. J. Cell Physiol. 2019, 234, 16812–16823. [Google Scholar] [CrossRef] [PubMed]
- Prabhu, N.V.; Maiya, A.G.; Prabhu, N.S. Impact of Cardiac Rehabilitation on Functional Capacity and Physical Activity after Coronary Revascularization: A Scientific Review. Cardiol. Res. Pract. 2020, 2020, 1236968. [Google Scholar] [CrossRef] [PubMed]
- Franklin, B.A.; Quindry, J. High level physical activity in cardiac rehabilitation: Implications for exercise training and leisure-time pursuits. Prog. Cardiovasc. Dis. 2022, 70, 22–32. [Google Scholar] [CrossRef] [PubMed]
- Osailan, A.; Abdelbasset, W.K. Exercise-based cardiac rehabilitation for postcoronary artery bypass grafting and its effect on hemodynamic responses and functional capacity evaluated using the Incremental Shuttle Walking Test: A retrospective pilot analysis. J. Saudi. Heart Assoc. 2020, 32, 25–33. [Google Scholar] [CrossRef]
- Francis, T.; Kabboul, N.; Rac, V.; Mitsakakis, N.; Pechlivanoglou, P.; Bielecki, J.; Alter, D.; Krahn, M. The Effect of Cardiac Rehabilitation on Health-Related Quality of Life in Patients with Coronary Artery Disease: A Meta-analysis. Can. J. Cardiol. 2019, 35, 352–364. [Google Scholar] [CrossRef]
- Dibben, G.O.; Dalal, H.M.; Taylor, R.S.; Doherty, P.; Tang, L.H.; Hillsdon, M. Cardiac rehabilitation and physical activity: Systematic review and meta-analysis. Heart 2018, 104, 1394–1402. [Google Scholar] [CrossRef]
- Carbone, S.; Kim, Y.; Kachur, S.; Billingsley, H.; Kenyon, J.; De Schutter, A.; Milani, R.V.; Lavie, C.J. Peak oxygen consumption achieved at the end of cardiac rehabilitation predicts long-term survival in patients with coronary heart disease. Eur. Heart J. Qual. Care Clin. Outcomes 2022, 8, 361–367. [Google Scholar] [CrossRef]
- Papathanasiou, J.V.; Ilieva, E.; Marinov, B. Six-minute walk test: An effective and necessary tool in modern cardiac rehabilitation. Hellenic. J. Cardiol. 2013, 54, 126–130. [Google Scholar]
- Houchen-Wolloff, L.; Boyce, S.; Singh, S. The minimum clinically important improvement in the incremental shuttle walk test following cardiac rehabilitation. Eur. J. Prev. Cardiol. 2015, 22, 972–978. [Google Scholar] [CrossRef]
- Fiorina, C.; Vizzardi, E.; Lorusso, R.; Maggio, M.; De Cicco, G.; Nodari, S.; Faggiano, P.; Dei Cas, L. The 6-min walking test early after cardiac surgery. Reference values and the effects of rehabilitation programme. Eur. J. Cardiothorac. Surg. 2007, 32, 724–729. [Google Scholar] [CrossRef]
- Chen, Y.C.; Chen, K.C.; Lu, L.H.; Wu, Y.L.; Lai, T.J.; Wang, C.H. Validating the 6-minute walk test as an indicator of recovery in patients undergoing cardiac surgery: A prospective cohort study. Medicine 2018, 97, e12925. [Google Scholar] [CrossRef] [PubMed]
- Jolly, K.; Taylor, R.S.; Lip, G.Y.; Singh, S.; BRUM Steering Committee. Reproducibility and safety of the incremental shuttle walking test for cardiac rehabilitation. Int. J. Cardiol. 2008, 125, 144–145. [Google Scholar] [CrossRef] [PubMed]
- Copay, A.G.; Subach, B.R.; Glassman, S.D.; Polly, D.W., Jr.; Schuler, T.C. Understanding the minimum clinically important difference: A review of concepts and methods. Spine J. 2007, 7, 541–546. [Google Scholar] [CrossRef]
- Khan, I.; Pennings, J.S.; Devin, C.J.; Asher, A.M.; Oleisky, E.R.; Bydon, M.; Asher, A.L.; Archer, K.R. Clinically Meaningful Improvement Following Cervical Spine Surgery: 30% Reduction Versus Absolute Point-change MCID Values. Spine 2021, 46, 717–725. [Google Scholar] [CrossRef]
- Wells, G.; Beaton, D.; Shea, B.; Boers, M.; Simon, L.; Strand, V.; Brooks, P.; Tugwell, P. Minimal clinically important differences: Review of methods. J. Rheumatol. 2001, 28, 406–412. [Google Scholar] [PubMed]
- Crosby, R.D.; Kolotkin, R.L.; Williams, G.R. Defining clinically meaningful change in health-related quality of life. J. Clin. Epidemiol. 2003, 56, 395–407. [Google Scholar] [CrossRef]
- Lydick, E.; Epstein, R.S. Interpretation of quality-of-life changes. Qual. Life Res. 1993, 2, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Rai, S.K.; Yazdany, J.; Fortin, P.R.; Aviña-Zubieta, J.A. Approaches for estimating minimal clinically important differences in systemic lupus erythematosus. Arthritis. Res. Ther. 2015, 17, 143. [Google Scholar] [CrossRef]
- Gremeaux, V.; Troisgros, O.; Benaïm, S.; Hannequin, A.; Laurent, Y.; Casillas, J.M.; Benaïm, C. Determining the minimal clinically important difference for the six-minute walk test and the 200-meter fast-walk test during cardiac rehabilitation program in coronary artery disease patients after acute coronary syndrome. Arch. Phys. Med. Rehabil. 2011, 92, 611–619. [Google Scholar] [CrossRef]
- Busch, J.C.; Lillou, D.; Wittig, G.; Bartsch, P.; Willemsen, D.; Oldridge, N.; Bjarnason-Wehrens, B. Resistance and balance training improves functional capacity in very old participants attending cardiac rehabilitation after coronary bypass surgery. J. Am. Geriatr. Soc. 2012, 60, 2270–2276, Erratum in J. Am. Geriatr. Soc. 2013, 9, 479. [Google Scholar] [CrossRef]
- Salzman, S.H. The 6-min walk test: Clinical and research role, technique, coding, and reimbursement. Chest 2009, 135, 1345–1352. [Google Scholar] [CrossRef]
- Nathan, S.D.; du Bois, R.M.; Albera, C.; Bradford, W.Z.; Costabel, U.; Kartashov, A.; Noble, P.W.; Sahn, S.A.; Valeyre, D.; Weycker, D.; et al. Validation of test performance characteristics and minimal clinically important difference of the 6-minute walk test in patients with idiopathic pulmonary fibrosis. Respir. Med. 2015, 109, 914–922. [Google Scholar] [CrossRef] [PubMed]
- Krleza-Jerić, K.; Lemmens, T. 7th revision of the Declaration of Helsinki: Good news for the transparency of clinical trials. Croat. Med J. 2009, 50, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Enright, P.L. The six-minute walk test. Respir. Care. 2003, 48, 783–785. [Google Scholar]
- Wise, R.A.; Brown, C.D. Minimal Clinically Important Differences in the Six-Minute Walk Test and the Incremental Shuttle Walking Test. COPD J. Chronic. Obstr. Pulm. Dis. 2005, 2, 125–129. [Google Scholar] [CrossRef]
- Shoemaker, M.J.; Curtis, A.B.; Vangsnes, E.; Dickinson, M.G. Clinically meaningful change estimates for the six-minute walk test and daily activity in individuals with chronic heart failure. Cardiopulm. Phys. Ther. J. 2013, 24, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Katijjahbe, M.A.; Granger, C.L.; Denehy, L.; Royse, A.; Royse, C.; Bates, R.; Logie, S.; Nur Ayub, M.A.; Clarke, S.; El-Ansary, D. Standard restrictive sternal precautions and modified sternal precautions had similar effects in people after cardiac surgery via median sternotomy (‘SMART’ Trial): A randomised trial. J. Physiother. 2018, 64, 97–106. [Google Scholar] [CrossRef]
- Holland, A.E.; Hill, C.J.; Conron, M.; Munro, P.; McDonald, C.F. Small changes in six-minute walk distance are important in diffuse parenchymal lung disease. Respir. Med. 2009, 103, 1430–1435. [Google Scholar] [CrossRef]
- Yuksel, S.; Ayhan, S.; Nabiyev, V.; Domingo-Sabat, M.; Vila-Casademunt, A.; Obeid, I.; Perez-Grueso, F.S.; Acaroglu, E.; European Spine Study Group (ESSG). Minimum clinically important difference of the health-related quality of life scales in adult spinal deformity calculated by latent class analysis: Is it appropriate to use the same values for surgical and nonsurgical patients? Spine J. 2019, 19, 71–78. [Google Scholar] [CrossRef]
- Singh, S.J.; Puhan, M.A.; Andrianopoulos, V.; Hernandes, N.A.; Mitchell, K.E.; Hill, C.J.; Lee, A.L.; Camillo, C.A.; Troosters, T.; Spruit, M.A.; et al. An official systematic review of the European Respiratory Society/American Thoracic Society: Measurement properties of field walking tests in chronic respiratory disease. Eur. Respir. J. 2014, 44, 1447–1478. [Google Scholar] [CrossRef]


{kind=link}
| Exercise Program | Specifications |
|---|---|
| Deep breathing exercises | 10 repetitions twice a day |
| Nebulization, chest percussions and huffing & coughing | Twice a day |
| Active range of motion exercises with minimal resistance | 10 reptations, twice a day |
| Incentive spirometry | 15 repetitions after every 2 h |
| Walk | with/without walking aids |
| Climbing one flight of the stairs (4 Steps) | on 4th post operative day |
| Variable | Category | Patients (n = 89) A | 6MWT | ISWT | ||
|---|---|---|---|---|---|---|
| Patients Reporting “No Improvement” (n = 64) | Patients Reporting “Improvement” (n = 25) | Patients Reporting “No Improvement” (n = 6) | Patients Reporting “Improvement” (n =8 3) | |||
| Sex | Males | 62.9% | 68% | 60.9% | 70.8% | 60.0% |
| Females | 37.1% | 32% | 39.1% | 29.2% | 40.0% | |
| Diagnosis | TVCAD | 24.7% | 24.0% | 25% | 37.5% | 20.0% |
| Stenosis of LAD | 52.8% | 52.0% | 53.1% | 45.8% | 55.4% | |
| Stenosis of proximal Cx artery | 15.7% | 16.0% | 15.6% | 12.5% | 16.9% | |
| Others | 6.7% | 8.0% | 6.3% | 4.2% | 7.7% | |
| Diabetics | Positive | 47.2% | 48% | 46.9% | 58.3% | 43.1% |
| Negative | 52.8% | 52% | 53.1% | 41.7% | 56.9% | |
| HTN | Positive | 59.6% | 64% | 57.8% | 58.3% | 60.0% |
| Negative | 40.4% | 36% | 42.2% | 41.7% | 40.0% | |
| BMI | Under weight | 10.1% | 8% | 10.9% | 16.7% | 7.7% |
| Normal | 41.6% | 32% | 45.3% | 37.5% | 43.1% | |
| Overweight | 29.2% | 32% | 28.1% | 25.0% | 30.8% | |
| Obese | 19.1% | 28% | 15.6% | 20.8% | 18.5% | |
| Use of supplemental oxygen | No | 86.5% | 100% | 81.3% | 91.7% | 84.6% |
| Type of Graft | Venous | 41.6% | 36% | 43.8% | 45.8% | 40.0% |
| Arterial | 58.4% | 64% | 56.3% | 54.2% | 60.0% | |
| Type of CABG | Complete CABG | 60.7% | 48% | 65.6% | 75.0% | 55.4% |
| MIDCABG | 39.3% | 52% | 34.4% | 25.0% | 44.6% | |
| Variables | Patients (n = 89) | 6MWT | ISWT | ||
|---|---|---|---|---|---|
| Patients Reporting “No Improvement” (n = 64) | Patients Reporting “Improvement” (n = 25) | Patients Reporting “No Improvement” (n = 6) | Patients Reporting “Improvement” (n = 83) | ||
| Age (years) | 58.4 ± 8.3 | 57.40 ± 7.78 | 58.89 ± 8.5 | 57.70 ± 8.06 | 58.75 ± 8.45 |
| Height (meters) | 1.7 ± 0.07 | 1.71 ± 0.07 | 1.70 ± 0.06 | 1.72 ± 1.70 | 67.18 ± 0.07 |
| Weight (kg) | 80.6 ± 6.9 | 79.56 ± 7.2 | 81.07 ± 6.7 | 80.54 ± 7.05 | 80.69 ± 6.93 |
| Ejection Fraction (%) | 58.8 ± 5.9 | 60.36 ± 6.1 | 58.31 ± 5.7 | 59.45 ± 5.83 | 58.67 ± 5.98 |
| Duration of Surgery (hours) | 3.7 ± 0.52 | 3.72 ± 0.54 | 3.78 ± 0.51 | 3.87 ± 0.44 | 3.72 ± 0.54 |
| Duration of ICU stay in (days) | 2.0 ± 0.0 | 2.0 ± 0.0 | 2.0 ± 0.0 | 2.00 ± 0.0 | 2.00 ± 0.0 |
| Duration of arousal from anesthesia (hours) | 3.1 ± 0.74 | 3.28 ± 0.79 | 3.14 ± 0.73 | 3.00 ± 0.72 | 3.24 ± 0.75 |
| Day 03 | Day 05 | Day 07 | |||||
|---|---|---|---|---|---|---|---|
| Vitals after 6MWT | |||||||
| Pre-Test (Mean ± SD) | Post Test (Mean ± SD) | Pre-Test (Mean ± SD) | Post Test (Mean ± SD) | Pre-Test (Mean ± SD) | Post Test (Mean ± SD) | ||
| Heart rate (b/m) | 73.78 ± 6.5 | 84.74 ± 5.75 | 73.48 ± 6.02 | 82.76 ± 5.20 | 72.89 ± 5.70 | 79.57 ± 2.63 | |
| Respiratory rate (b/m) | 16.70 ± 0.89 | 25.95 ± 2.52 | 16.91 ± 0.82 | 25.42 ± 2.76 | 16.73 ± 0.93 | 25.22 ± 1.72 | |
| Blood Pressure | Systolic (mmHg) | 133.21 ± 8.9 | 164 ± 18.18 | 133.48 ± 9.30 | 150.58 ± 41.11 | 133.48 ± 9.30 | 155.50 ± 24.02 |
| Diastolic (mmHg) | 86.62 ± 2.4 | 94.17 ± 2.88 | 86.78 ± 2.22 | 90.49 ± 4.62 | 86.55 ± 2.21 | 90.08 ± 4.43 | |
| SPO2(%) | 92.16 ± 4.0 | 80.66 ± 6.13 | 92.22 ± 4.43 | 87.84 ± 4.54 | 93.73 ± 3.63 | 91.74 ± 4.72 | |
| Fatigue after 6MWT | |||||||
| No fatigue at all | 0 (0%) | 0 (0%) | 0 (0%) | ||||
| Slightly Fatigue | 17 (19.1%) | 50 (56.2%) | 68 (76.4%) | ||||
| Moderately fatigue | 56 (62.9%) | 32 (36.0%) | 14 (15.7%) | ||||
| Severe Fatigue | 16 (18.0%) | 7 (7.9%) | 7 (7.9%) | ||||
| Dyspnea after 6MWT | |||||||
| No Breathlessness At all | 0 (0%) | 0 (0%) | 0 (0%) | ||||
| Very very slight breathlessness | 0 (0%) | 0 (0%) | 1 (1.1%) | ||||
| Very Slight breathlessness | 0 (0%) | 0 (0%) | 19 (21.3%) | ||||
| Slight Breathlessness | 0 (0%) | 1 (1.1%) | 1 (1.1%) | ||||
| Moderate Breathlessness | 38 (42.7%) | 36 (40.4%) | 35 (39.3%) | ||||
| Somewhat Severe Breathlessness | 36 (40.4%) | 39 (43.8%) | 15 (16.9%) | ||||
| Severe Breathlessness | 9 (10.1%) | 12 (13.5%) | 6 (6.7%) | ||||
| Maximum Breathlessness | 6 (6.7%) | 1 (1.1%) | 12 (13.5%) | ||||
| Variables | Day 03 (Mean ± SD) | Day 05 (Mean ± SD) | Day 07 (Mean ± SD) | |
|---|---|---|---|---|
| No. of Laps | 4.90 ± 1.25 | 5.60 ± 1.37 | 6.25 ± 1.53 | |
| Total Distance covered (meters) | 294.26 ± 75.25 | 336.50 ± 82.59 | 376.51 ± 92.57 | |
| Time Taken (minutes) | 5.68 ± 0.76 | 5.77 ± 0.82 | 5.91 ± 0.45 | |
| No. of Times the patients stopped during test | 1.60 ± 0.54 | 1.33 ± 0.50 | 1.33 ± 0.51 | |
| GRC after 7 days of intervention | Improvement | 64 (71.9%) | ||
| No improvement | 25 (28.1%) | |||
| Distribution Based Estimation (n = 89) | |||||
|---|---|---|---|---|---|
| 6mwd at Baseline | Baseline SD | ICC | SEM | MDD | |
| 294.26 | 75.25 | 0.97 | 13.03 | 36.11 | |
| Anchor Based Estimation (n = 89) | |||||
| Estimate of MCID for change in 6MWD (meters) | 195 m | ||||
| AUC (95% CI) | 0.651 (0.510–0.792) | ||||
| Sensitivity | 0.98 | ||||
| 1-Specificity | 0.76 | ||||
| Day 03 | Day 05 | Day 07 | |||||
|---|---|---|---|---|---|---|---|
| Vitals after 6MWT | |||||||
| Pre-Test (Mean ± SD) | Post Test (Mean ± SD) | Pre-Test (Mean ± SD) | Post Test (Mean ± SD) | Pre-Test (Mean ± SD) | Post Test (Mean ± SD) | ||
| Heart rate (b/m) | 73.31 ± 6.4 | 84.66 ± 5.7 | 73.33 ± 6.03 | 83.24 ± 5.4 | 73.12 ± 5.6 | 81.82 ± 6.7 | |
| Respiratory rate (b/m) | 16.60 ± 0.85 | 26.53 ± 2.43 | 17.04 ± 0.79 | 24.87 ± 2.5 | 16.66 ± 0.95 | 25.32 ± 1.3 | |
| B.P | Systolic (mmHg) | 132.65 ± 10.3 | 174.26 ± 14.05 | 133.48 ± 9.3 | 168.32 ± 19.8 | 134.04 ± 9.7 | 152.15 ± 21.6 |
| Diastolic (mmHg) | 86.62 ± 2.4 | 94 ± 3.09 | 86.86 ± 2.2 | 91.44 ± 4.5 | 87.10 ± 1. 9 | 90.08 ± 4.43 | |
| SO2(%) | 92.16 ± 4.09 | 89.56 ± 5.23 | 92.48 ± 4.02 | 88.78 ± 4.7 | 92.90 ± 3.4 | 88.57 ± 4.2 | |
| Fatigue after 6MWT | |||||||
| No fatigue at all | 0 (0%) | 0 (0%) | 0 (0%) | ||||
| Slightly Fatigue | 20 (22.5%) | 27 (30.3%) | 55 (61.8%) | ||||
| Moderately fatigue | 34 (38.2%) | 57 (64%) | 34 (38.2%) | ||||
| Severe Fatigue | 35 (39.3%) | 5 (5.6%) | 0 (0%) | ||||
| Dyspnea after 6MWT | |||||||
| No Breathlessness At all | 0 (0%) | 0 (0%) | 0 (0%) | ||||
| Very Very slight breathlessness | 0 (0%) | 0 (0%) | 3 (3.4%) | ||||
| Very Slight breathlessness | 0 (0%) | 0 (0%) | 25 (28.1%) | ||||
| Slight Breathlessness | 0 (0%) | 1 (1.1%) | 4 (4.5%) | ||||
| Moderate Breathlessness | 38 (42.7%) | 36 (40.4%) | 27 (30.3%) | ||||
| Somewhat Severe Breathlessness | 39 (43.8%) | 39 (43.8%) | 6 (6.7%) | ||||
| Severe Breathlessness | 10 (11.2%) | 12 (13.5%) | 1 (1.1%) | ||||
| Maximum Breathlessness | 2 (2.2%) | 1 (1.1%) | 23 (25.8%) | ||||
| Variables | Day 03 (Mean ± SD) | Day 05 (Mean ± SD) | Day 07 (Mean ± SD) | |
|---|---|---|---|---|
| No. of Laps | 3.11 ± 0.81 | 3.80 ± 0.82 | 4.47 ± 0.97 | |
| Total Distance covered (meters) | 31.12 ± 8.17 | 38.08 ± 8.24 | 44.71 ± 9.78 | |
| Time Taken (seconds) | 54.26 ± 10.54 | 62.47 ± 7.72 | 81.46 ± 8.05 | |
| No. of Times the patients stopped during test | 1.50 ± 0.57 | 1.0 ± 0.0 | 2.0 ± 0.0 | |
| GRC scale after 7 days of intervention | Improvement | 65 (48.07%) | ||
| No improvement | 24 (35.62%) | |||
| Median (IQR) | Mean Rank | Z Value | p Value | |||
|---|---|---|---|---|---|---|
| Improvement (n = 65) | No Improvement (n = 24) | Improvement (n = 65) | No Improvement (n = 24) | |||
| ISWD at day 03 | 30 (15) | 30 (14) | 43.02 | 50.35 | −1.21 | 0.224 |
| ISWD at day 05 | 40 (15) | 30 (10) | 47.83 | 37.33 | −1.76 | 0.077 |
| ISWD at day 07 | 50 (10) | 32 (10) | 53.37 | 22.33 | −5.16 | 0.000 |
| Distribution Based Estimation (n = 89) | |||||
|---|---|---|---|---|---|
| ISWD at Baseline | Baseline SD | ICC | SEM | MDD | |
| 31.12 | 8.17 | 0.76 | 3.99 | 9.94 | |
| Anchor based estimation (n = 89) | |||||
| Estimate of MCID for change in ISWD (meters) | 42.5 m | ||||
| AUC (95% CI) | 0.849 (0.759–0.939) | ||||
| Sensitivity | 0.70 | ||||
| 1-Specificity | 0.20 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sheraz, S.; Ayub, H.; Ferraro, F.V.; Razzaq, A.; Malik, A.N. Clinically Meaningful Change in 6 Minute Walking Test and the Incremental Shuttle Walking Test following Coronary Artery Bypass Graft Surgery. Int. J. Environ. Res. Public Health 2022, 19, 14270. https://doi.org/10.3390/ijerph192114270
Sheraz S, Ayub H, Ferraro FV, Razzaq A, Malik AN. Clinically Meaningful Change in 6 Minute Walking Test and the Incremental Shuttle Walking Test following Coronary Artery Bypass Graft Surgery. International Journal of Environmental Research and Public Health. 2022; 19(21):14270. https://doi.org/10.3390/ijerph192114270
Chicago/Turabian StyleSheraz, Suman, Humera Ayub, Francesco V. Ferraro, Aisha Razzaq, and Arshad Nawaz Malik. 2022. "Clinically Meaningful Change in 6 Minute Walking Test and the Incremental Shuttle Walking Test following Coronary Artery Bypass Graft Surgery" International Journal of Environmental Research and Public Health 19, no. 21: 14270. https://doi.org/10.3390/ijerph192114270
APA StyleSheraz, S., Ayub, H., Ferraro, F. V., Razzaq, A., & Malik, A. N. (2022). Clinically Meaningful Change in 6 Minute Walking Test and the Incremental Shuttle Walking Test following Coronary Artery Bypass Graft Surgery. International Journal of Environmental Research and Public Health, 19(21), 14270. https://doi.org/10.3390/ijerph192114270