
Burden of Oral Cancer on the 10 Most Populous Countries from 1990 to 2019: Estimates from the Global Burden of Disease Study 2019


Abstract
:1. Introduction
2. Methods
2.1. Study Data
2.2. Statistical Analysis
3. Results
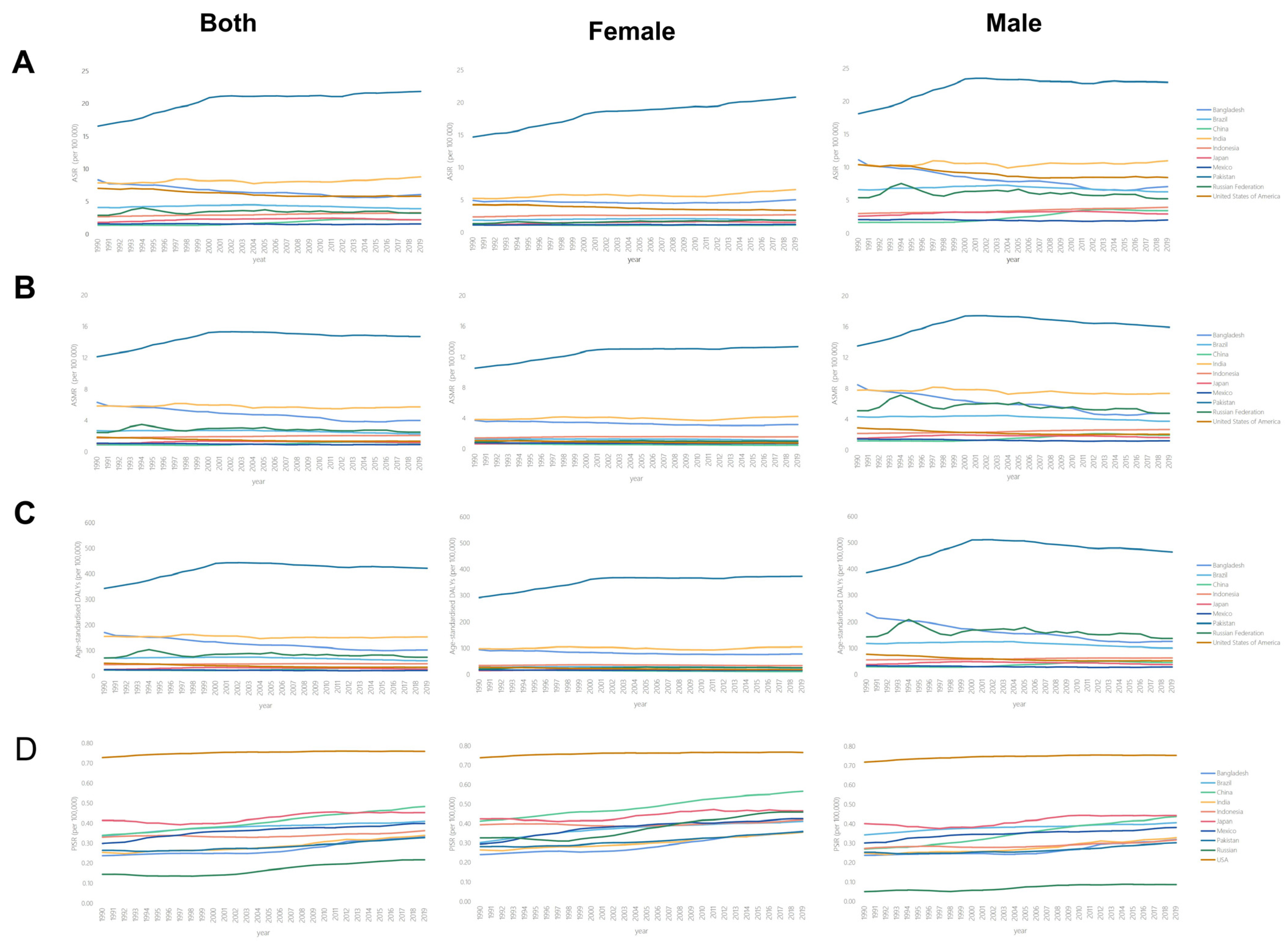
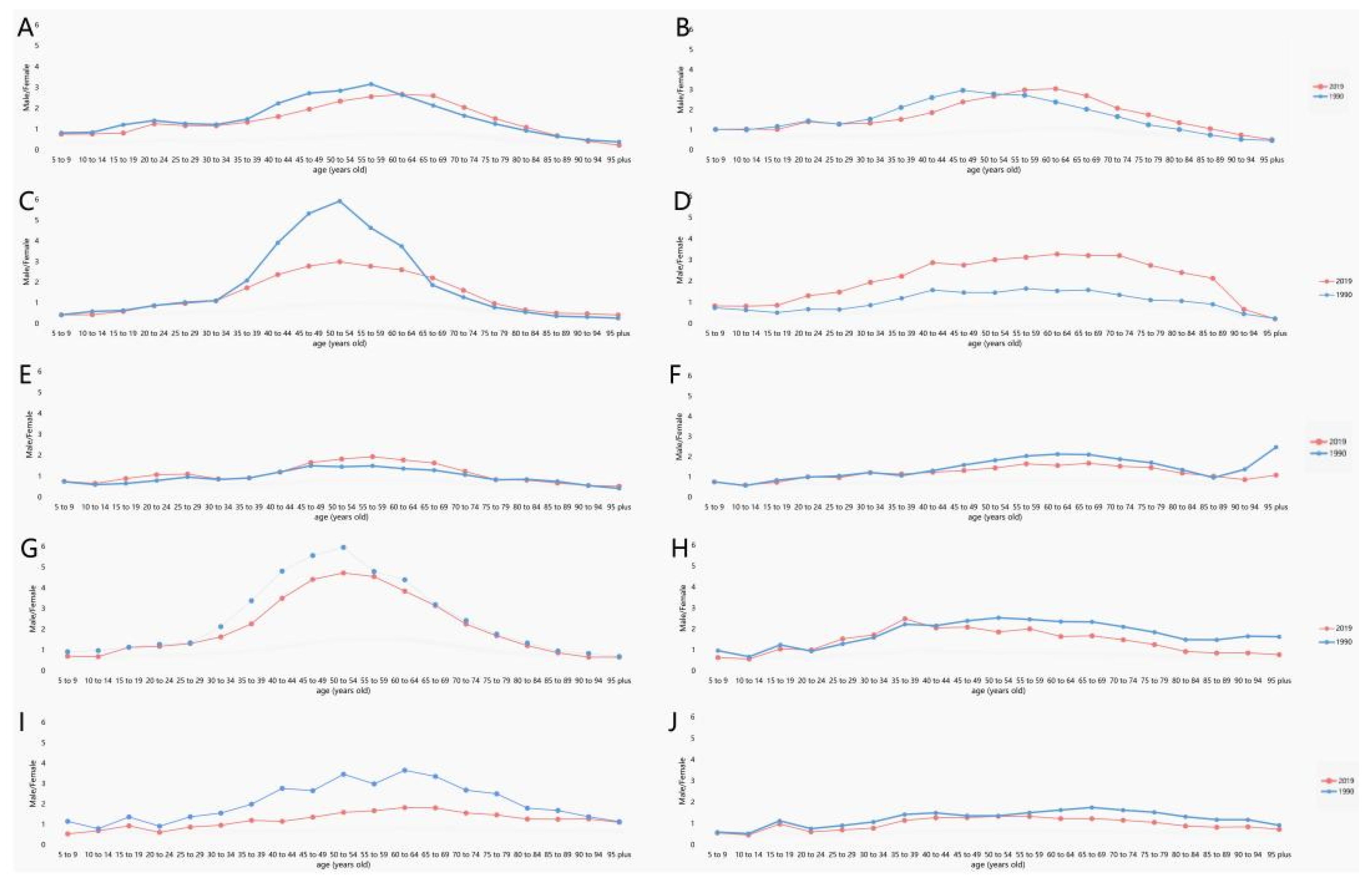
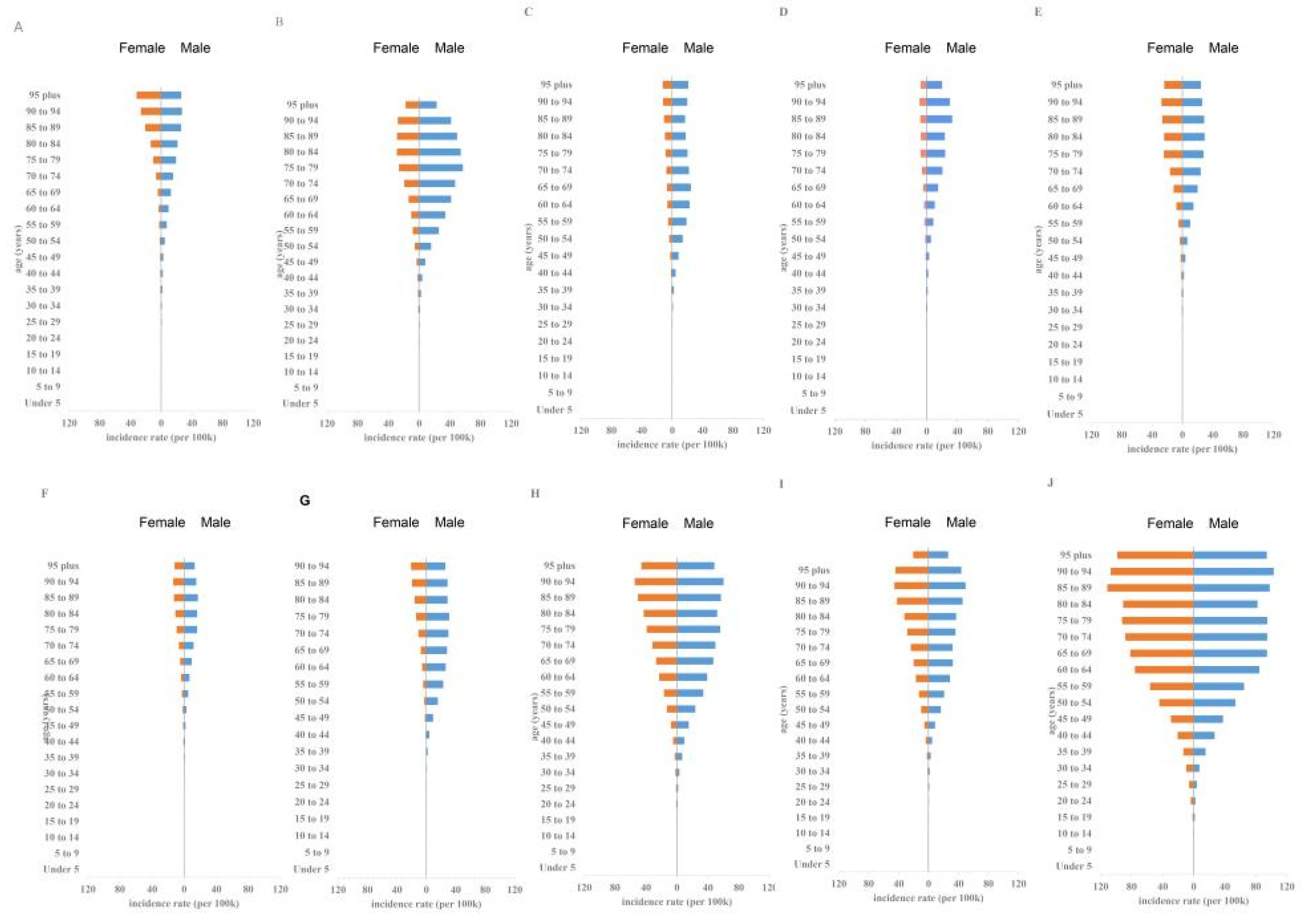
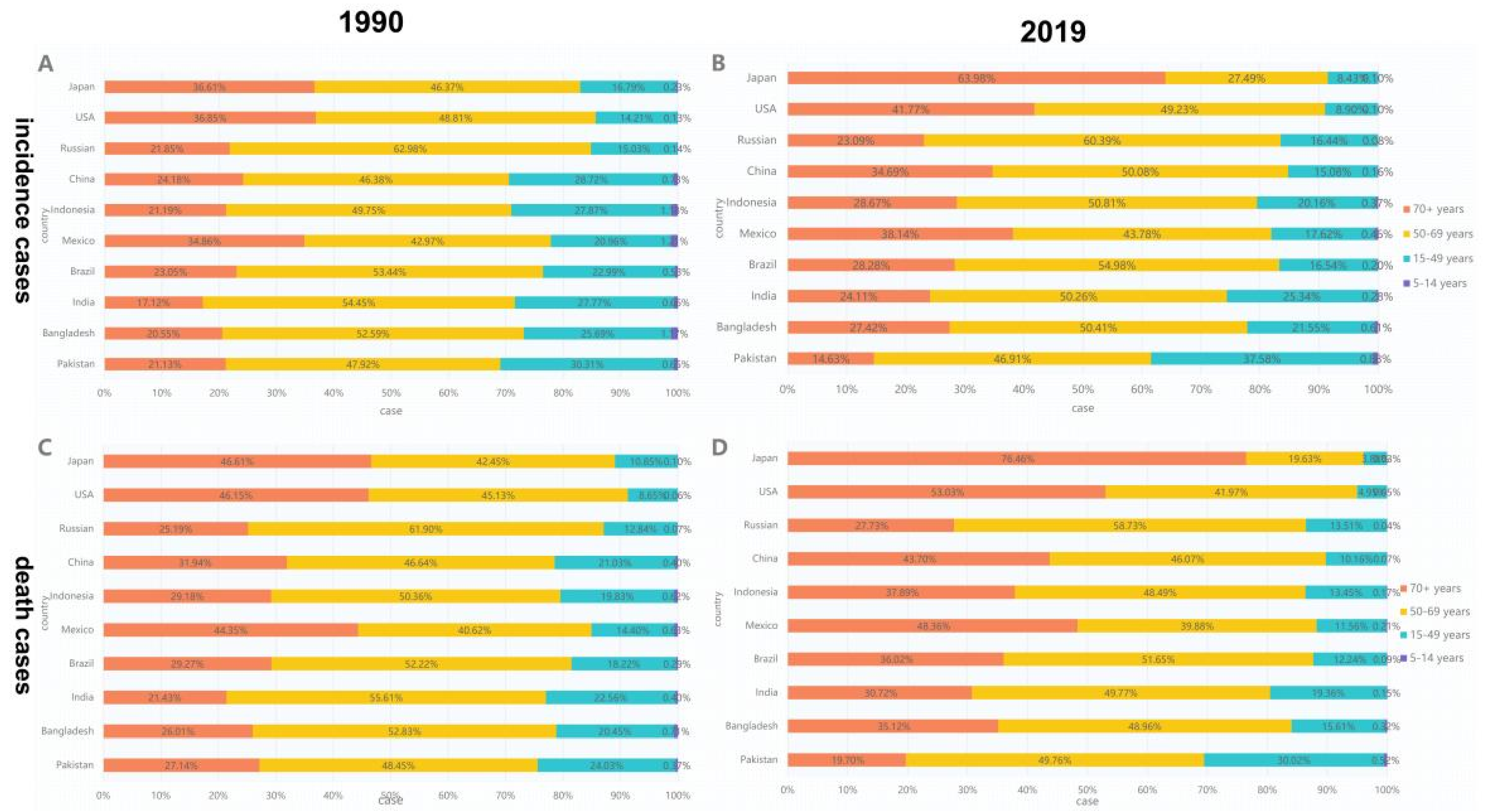
3.1. Analysis of OC Incidence in the 10 Most Populous Countries
3.2. Analysis of OC-Related Death in the 10 Most Populous Countries
3.3. Analysis of DALY and Survival Rate for OC in the 10 Countries with the Largest Populations
3.4. Etiological Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Asthana, S.; Labani, S.; Kailash, U.; Shinha, D.N.; Mehrotra, R. Association of Smokeless Tobacco Use and Oral Cancer: A Systematic Global Review and Meta-Analysis. Nicotine Tob. Res. 2019, 21, 1162–1171. [Google Scholar] [CrossRef] [PubMed]
- Mehrtash, H.; Duncan, K.; Parascandola, M.; David, A.; Gritz, E.R.; Gupta, P.C.; Mehrotra, R.; Nordin, A.S.A.; Pearlman, P.C.; Warnakulasuriya, S.; et al. Defining a global research and policy agenda for betel quid and areca nut. Lancet Oncol. 2017, 18, e767–e775. [Google Scholar] [CrossRef]
- Zhao, D.; Xu, Q.G.; Chen, X.M.; Fan, M.W. Human Papillomavirus as an Independent Predictor in Oral Squamous Cell Cancer. Int. J. Oral Sci. 2009, 1, 119–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeng, H.; Chen, W.; Zheng, R.; Zhang, S.; Ji, J.; Zou, X.; Xia, C.; Sun, K.; Yang, Z.; Li, H.; et al. Changing cancer survival in China during 2003–15: A pooled analysis of 17 population-based cancer registries. Lancet Glob. Health 2018, 6, e555–e567. [Google Scholar] [CrossRef] [Green Version]
- Omar, E. Future Imaging Alternatives: The Clinical Non-invasive Modalities in Diagnosis of Oral Squamous Cell Carcinoma (OSCC). Open Dent. J. 2015, 9, 311–318. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.-W.; Li, J.; Cong, X.; Hu, X.-S.; Li, D.; Wu, L.-L.; Hua, H.; Yu, G.-Y.; Kerr, A.R. Incidence and mortality trends in oral and oropharyngeal cancers in China, 2005–2013. Cancer Epidemiol. 2018, 57, 120–126. [Google Scholar] [CrossRef]
- Amarasinghe, H.; Jayasinghe, R.D.; Dharmagunawardene, D.; Attygalla, M.; Scuffham, P.A.; Johnson, N.; Kularatna, S. Economic burden of managing oral cancer patients in Sri Lanka: A cross-sectional hospital -based costing study. BMJ Open 2019, 9, e027661. [Google Scholar] [CrossRef] [Green Version]
- IHME. GHDx: GBD Results Tool. Available online: http://ghdx.healthdata.org/gbd-results-tool (accessed on 7 December 2021).
- Vostakolaei, F.A.; Karim-Kos, H.E.; Janssen-Heijnen, M.L.; Visser, O.; Verbeek, A.L.; Kiemeney, L.A. The validity of the mortality to incidence ratio as a proxy for site-specific cancer survival. Eur. J. Public Health 2010, 21, 573–577. [Google Scholar] [CrossRef] [Green Version]
- WHO World Health Organization. Available online: https://apps.who.int/gho/data/?showonly=GISAH&theme=main (accessed on 7 December 2021).
- GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 385, 117–171. [CrossRef]
- Hankey, B.F.; Ries, L.A.; Kosary, C.L.; Feuer, E.J.; Merrill, R.M.; Clegg, L.X.; Edwards, B.K. Partitioning linear trends in age-adjusted rates. Cancer Causes Control. 2000, 11, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Mbulo, L.; Twentyman, E.; Palipudi, K.; King, B.A. Disparities in smokeless tobacco use in Bangladesh, India, and Pakistan: Findings from the Global Adult Tobacco Survey, 2014–2017. PLoS ONE 2021, 16, e0250144. [Google Scholar] [CrossRef] [PubMed]
- NCI; National Cancer Institute and Centers for Disease Control and Prevention (Eds.) Smokeless Tobacco and Public Health: A Global Perspective; NIH Publication no. 14-7983; NCI: Rockville, MD, USA, 2014. Available online: https://cancercontrol.cancer.gov/sites/default/files/2020-06/smokelesstobaccoandpublichealth.pdf (accessed on 7 December 2021).
- WHO World Health Organization. WHO Report on the Global Tobacco Epidemic 2019: Offer Help to Quit Tobacco Use; WHO: Geneva, Switzerland, 2019; Available online: https://www.who.int/publications/i/item/WHO-NMH-PND-2019.5 (accessed on 7 December 2021).
- Astuti, P.A.S.; Assunta, M.; Freeman, B. Why is tobacco control progress in Indonesia stalled?-A qualitative analysis of interviews with tobacco control experts. BMC Public Health 2020, 20, 527. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.R.; Wang, J.; Zhao, L.Y.; Wang, Z.H.; Yu, D.M.; He, Y.N.; Ding, G.G. The drinking status and associated factors in adults in China. Zhonghua Liu Xing Bing Xue Za Zhi 2018, 39, 898–903. [Google Scholar]
- Antunes, J.; Toporcov, T.N.; Biazevic, M.G.; Boing, A.F.; Bastos, J.L. Gender and racial inequalities in trends of oral cancer mortality in Sao Paulo, Brazil. Revista de Saúde Pública 2013, 47, 470–478. [Google Scholar] [CrossRef] [Green Version]
- Lipsky, M.S.; Su, S.; Crespo, C.J.; Hung, M. Men and Oral Health: A Review of Sex and Gender Differences. Am. J. Men’s Health 2021, 15, 15579883211016361. [Google Scholar] [CrossRef]
- Choinzonov, E.L.; Pisareva, L.F.; Odintsova, I.N.; Zhuikova, L.D. Oral cavity and pharynx cancer in the region of Siberia and Far East. Vestnik Otorinolaringol. 2015, 80, 38. [Google Scholar] [CrossRef]
- Khan, Z.; Tönnies, J.; Müller, S. Smokeless Tobacco and Oral Cancer in South Asia: A Systematic Review with Meta-Analysis. J. Cancer Epidemiol. 2014, 2014, 394696. [Google Scholar] [CrossRef]
- Ibayashi, H.; Pham, T.-M.; Fujino, Y.; Kubo, T.; Ozasa, K.; Matsuda, S.; Yoshimura, T. Estimation of premature mortality from oral cancer in Japan, 1995 and 2005. Cancer Epidemiol. 2011, 35, 342–344. [Google Scholar] [CrossRef]
- Tayyaba; Akram, N.; Rehman, F.U. A new wave of oral cancer epidemic among youth in Pakistan. Oral Oncol. 2020, 100, 104480. [Google Scholar] [CrossRef]
- Sdvizhkov, A.M.; Kozhanov, L.G.; Shatskaia, N.K.; Belov, E.N. Analysis of the causes of cancer negligence and low survival in the patients with malignant neoplasms of ENT and oral cavity in the city of Moscow. Vestnik Otorinolaringol. 2014, 1, 20–23. [Google Scholar]
- Leon, D.A.; Saburova, L.; Tomkins, S.; McKee, M.; Shkolnikov, V.M. Alcohol consumption and public health in Russia. Lancet 2007, 370, 561. [Google Scholar] [CrossRef]
- Rehm, J.; Mathers, C.; Popova, S.; Thavorncharoensap, M.; Teerawattananon, Y.; Patra, J. Global burden of disease and injury and economic cost attributable to alcohol use and alcohol-use disorders. Lancet 2009, 373, 2223–2233. [Google Scholar] [CrossRef]
- WHO Global Alcohol Report—Russian Federation. Available online: http://www.who.int/substance_abuse/publications/global_alcohol_report/msbgsreur.pdf (accessed on 7 December 2021).
- Jargin, S.V. The state of medical libraries in the former Soviet Union. Health Inf. Libr. J. 2010, 27, 244–248. [Google Scholar] [CrossRef]
- Goss, P.E.; Strasser-Weippl, K.; Lee-Bychkovsky, B.L.; Fan, L.; Li, J.; Chavarri-Guerra, Y.; Liedke, P.E.; Pramesh, C.S.; Badovinac-Crnjevic, T.; Sheikine, Y.; et al. Challenges to effective cancer control in China, India, and Russia. Lancet Oncol. 2014, 15, 489–538. [Google Scholar] [CrossRef]
- Jargin, S.V. Radiotherapy in Russia: A redundant method. Lancet Oncol. 2009, 10, 8–9. [Google Scholar] [CrossRef]
- Russian Citation Index. Available online: http://elibrary.ru/project_risc.asp (accessed on 7 December 2021). (In Russian).
- RISC Science Index. Available online: http://elibrary.ru/projects/science_index/science_index_questions.asp (accessed on 7 December 2021). (In Russian).
- Chan, K.K.; Glenny, A.M.; Weldon, J.C.; Furness, S.; Worthington, H.V.; Wakeford, H. Interventions for the treatment of oral and oropharyngeal cancers: Targeted therapy and immunotherapy. Cochrane Database Syst. Rev. 2015, 12, CD010341. [Google Scholar]
- Smith, R.A.; Cokkinides, V.; von Eschenbach, A.C.; Levin, B.; Cohen, C.; Runowicz, C.D.; Sener, S.; Saslow, D.; Eyre, H.J.; American Cancer Society. American Cancer Society guidelines for the early detection of cancer. CA Cancer J. Clin. 2002, 52, 8–22. [Google Scholar] [CrossRef]
- Rashid, A.; Warnakulasuriya, S. The use of light-based (optical) detection systems as adjuncts in the detection of oral cancer and oral potentially malignant disorders: A systematic review. J. Oral Pathol. Med. 2015, 44, 307–328. [Google Scholar] [CrossRef]
- Laronde, D.M.; Corbett, K.K. Adjunctive screening devices for oral lesions: Their use by Canadian Dental Hygienists and the need for knowledge translation. Int. J. Dent. Hyg. 2017, 15, 187–194. [Google Scholar] [CrossRef]
- Fedele, S. Diagnostic aids in the screening of oral cancer. Head Neck Oncol. 2009, 1, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nation | Sex | Incident Cases No.*102 (95%UI) | Change in Absolute Number (%) | ASIR per 100,000 No. (95%UI) | 1990–2019 EAPC No. (95%CI) | ||
|---|---|---|---|---|---|---|---|
| 1990 | 2019 | 1990 | 2019 | ||||
| Japan | both | 3069.67 (2951.51–3164.97) | 6945.3 (5688.46–8073.13) | 126.26 | 1.85 (1.78–1.91) | 2.24 (1.88–2.61) | 0.68 (from 0.4 to 0.95) |
| USA | both | 21,506.15 (20,863.25–22,016.96) | 30,767.8 (26,450.35–35,861.98) | 43.07 | 7.08 (6.88–7.24) | 5.82 (5–6.8) | −0.77 (from −0.88 to −0.65) |
| Russian | both | 5321.7 (5158.93–5530.02) | 7369.72 (6377.52–8485.26) | 38.48 | 2.94 (2.85–3.06) | 3.29 (2.84–3.79) | 0.07 (from −0.24 to 0.38) |
| China | both | 12,390.24 (10,867.31–14,056.85) | 45,216.41 (37,690.41–54,179.36) | 264.94 | 1.4 (1.23–1.57) | 2.25 (1.89–2.68) | 2.33 (from 2.02 to 2.64) |
| Indonesia | both | 2870.26 (2411.22–3416.52) | 7305.53 (5315.64–9875.54) | 154.53 | 2.72 (2.28–3.18) | 3.38 (2.48–4.55) | 0.68 (from 0.65 to 0.72) |
| Mexico | both | 708.43 (686.68–724.99) | 1913.03 (1647.8–2194.88) | 170.04 | 1.62 (1.56–1.67) | 1.63 (1.41–1.87) | −0.18 (from −0.28 to −0.07) |
| Brazil | both | 3898.95 (3761.12–4027.84) | 9582.82 (8998.64–100,77.52) | 145.78 | 4.16 (3.99–4.3) | 3.97 (3.73–4.18) | −0.18 (from −0.34 to −0.02) |
| India | both | 39,064.72 (34,407.2–44,178.57) | 104,838 (86,183.93–124,704.23) | 168.37 | 7.93 (6.94–9.02) | 8.82 (7.22–10.44) | 0.23 (from 0.12 to 0.33) |
| Bangladesh | both | 4244.93 (3096.55–5470.38) | 8217.35 (5596.69–11,584.18) | 93.58 | 8.37 (6.09–10.86) | 6.12 (4.19–8.55) | −1.2 (from −1.36 to −1.05) |
| Pakistan | both | 10,225.93 (8702.81–12,031.65) | 28,579.23 (22,906.63–35,934.93) | 179.48 | 16.6 (14.02–19.55) | 21.93 (17.83–27.56) | 0.85 (from 0.66 to 1.04) |
| Nation | Sex | Death Cases No.*102 (95%UI) | Change in Absolute Number(%) | ASMR per 100,000 No. (95%UI) | 1990–2019 EAPC No. (95%CI) | ||
|---|---|---|---|---|---|---|---|
| 1990 | 2019 | 1990 | 2019 | ||||
| Japan | both | 1771.13 (1686.56–1818.07) | 4677.72 (3885.97–5115.54) | 164.11 | 1.08 (1.03–1.11) | 1.22 (1.07–1.3) | 0.26 (from −0.04 to 0.57) |
| USA | both | 5968 (5729.59–6122.36) | 7821.12 (7373.7–8132.81) | 31.05 | 1.92 (1.85–1.97) | 1.4 (1.32–1.45) | −1.14 (from −1.31 to −0.97) |
| Russian | both | 4502.4 (4358.54–4662.54) | 5853.09 (4950.58–6852.39) | 30.00 | 2.51 (2.43–2.61) | 2.57 (2.18–3.01) | −0.32 (from −0.65 to 0.01) |
| China | both | 7403.22 (6437.56–8357.89) | 22,641.75 (18,908.09–27,077) | 205.84 | 0.92 (0.81–1.03) | 1.16 (0.98–1.38) | 1.43 (from 1.14 to 1.73) |
| Indonesia | both | 1717.05 (1437.36–1989.34) | 4203.71 (3115.71–5690.08) | 144.82 | 1.82 (1.52–2.09) | 2.15 (1.59–2.9) | 0.57 (from 0.52 to 0.61) |
| Mexico | both | 457.42 (439.65–469.14) | 1109 (957.6–1263.61) | 142.45 | 1.14 (1.08–1.17) | 0.98 (0.84–1.11) | −0.67 (from −0.78 to −0.56) |
| Brazil | both | 2428.36 (2332.38–2512.56) | 5563.6 (5201.97–5882.51) | 129.11 | 2.76 (2.62–2.86) | 2.34 (2.18–2.48) | −0.54 (from −0.68 to −0.41) |
| India | both | 26,609.06 (23,261.73–30,578.45) | 65,571.05 (54,391.75–78,443.01) | 146.42 | 5.9 (5.14–6.78) | 5.81 (4.84–6.94) | −0.22 (from −0.32 to −0.11) |
| Bangladesh | both | 3032.04 (2203.98–3934.21) | 5186.07 (3579.12–7217.8) | 71.04 | 6.37 (4.63–8.2) | 4.06 (2.83–5.6) | −1.67 (from −1.81 to −1.53) |
| Pakistan | both | 7141.28 (6091.77–8406.48) | 17,566.52 (14,062.12–22,168.62) | 145.99 | 12.18 (10.34–14.32) | 14.72 (11.9–18.34) | 0.52 (from 0.29 to 0.74) |
| Nation | Sex | DALY No.*102 (95%UI) | Change in Absolute Number (%) | Age-Standardized DALY Rate per 100,000 No. (95%UI) | 1990–2019 EAPC No. (95%CI) | ||
|---|---|---|---|---|---|---|---|
| 1990 | 2019 | 1990 | 2019 | ||||
| Japan | Both | 43,566.76 (42,191.13–44,497.11) | 77,039.22 (68,375–81,994.44) | 76.83 | 26.15 (25.32–26.71) | 27.73 (25.76–29.06) | −0.01 (from −0.36 to 0.33) |
| USA | Both | 150,227.05 (145,568.37–154,556.87) | 180,924.75 (172,524.53–188,143.83) | 20.43 | 51.04 (49.55–52.48) | 35.02 (33.42–36.44) | −1.36 (from −1.54 to −1.19) |
| Russian | Both | 130,291.33 (125,473.55–135,933.69) | 163,106.13 (136,536.75–192,130.02) | 25.19 | 71.78 (69.1–74.96) | 74.92 (62.72–88.3) | −0.26 (from −0.62 to 0.11) |
| China | Both | 222,647.1 (192,534.07–252,402.8) | 575,805.4 (479,521.98–690,743.25) | 158.62 | 23.63 (20.48–26.66) | 28.27 (23.59–33.71) | 1.24 (from 0.96 to 1.52) |
| Indonesia | Both | 51,800.63 (43,542.12–60,910.65) | 113,143.08 (83,375.61–153,308.74) | 118.42 | 45.54 (38.08–52.9) | 48.92 (36.22–66.05) | 0.24 (from 0.19 to 0.29) |
| Mexico | Both | 11,956.54 (11,666.31–12,191.73) | 27,215.25 (23,357.09–31,173.64) | 127.62 | 25.54 (24.78–26.14) | 22.56 (19.36–25.77) | −0.56 (from −0.67 to −0.45) |
| Brazil | Both | 71,379.4 (68,985.46–73,775.73) | 148,871.92 (141,013.9–157,204.72) | 108.56 | 72.01 (69.33–74.39) | 60.82 (57.54–64.22) | −0.61 (from −0.79 to −0.44) |
| India | Both | 847,614.72 (745,309.09–961,913.07) | 1,922,663.79 (158,5385.47–2,318,025.04) | 126.83 | 156.3 (137.01–178.41) | 154.9 (128.07–186.18) | −0.13 (from −0.22 to −0.05) |
| Bangladesh | Both | 93,543.29 (68,249.51–121,318.94) | 144,651.02 (98,686.77–204,783.04) | 54.64 | 171.71 (124.61–224.07) | 103.95 (71.3–146.15) | −1.81 (from −1.93 to −1.68) |
| Pakistan | Both | 222,000.03 (188,451.19–262,435.79) | 594,088.79 (471,317.46–754,897.27) | 167.61 | 343.14 (293.41–405.54) | 421.87 (338.19–535.02) | 0.57 (from 0.32 to 0.81) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, S.-Z.; Xie, L.; Shang, Z.-J. Burden of Oral Cancer on the 10 Most Populous Countries from 1990 to 2019: Estimates from the Global Burden of Disease Study 2019. Int. J. Environ. Res. Public Health 2022, 19, 875. https://doi.org/10.3390/ijerph19020875
Zhang S-Z, Xie L, Shang Z-J. Burden of Oral Cancer on the 10 Most Populous Countries from 1990 to 2019: Estimates from the Global Burden of Disease Study 2019. International Journal of Environmental Research and Public Health. 2022; 19(2):875. https://doi.org/10.3390/ijerph19020875
Chicago/Turabian StyleZhang, Shu-Zhen, Long Xie, and Zheng-Jun Shang. 2022. "Burden of Oral Cancer on the 10 Most Populous Countries from 1990 to 2019: Estimates from the Global Burden of Disease Study 2019" International Journal of Environmental Research and Public Health 19, no. 2: 875. https://doi.org/10.3390/ijerph19020875
APA StyleZhang, S.-Z., Xie, L., & Shang, Z.-J. (2022). Burden of Oral Cancer on the 10 Most Populous Countries from 1990 to 2019: Estimates from the Global Burden of Disease Study 2019. International Journal of Environmental Research and Public Health, 19(2), 875. https://doi.org/10.3390/ijerph19020875