
An Overview of the Obese-Asthma Phenotype in Children



Abstract
1. Introduction
2. Which Came First, the Chicken or the Egg?
3. Aetiopathogenesis of the Bidirectional Relationship between Obesity and Asthma
3.1. Mechanical Factors
3.2. Proinflammatory Factors
3.3. Genetic Factors
3.4. Hormonal Factors
3.5. Microbiome
3.6. Physical Activity
3.7. Steroid Therapy
4. The “Obese-Asthma” Phenotype

{kind=link}
{kind=link}
| Articles | Subjects | Description |
|---|---|---|
| Liang L 2018 KJIM [92] | Murine models | Mice on high fat diet showed allergic airway inflammation. Blockading of IL-17 decreased airway hyper-responsiveness (AHR) and airway inflammation. The administration of the anti-IL-17 antibody decreased the leptin/adiponectin ratio, inhibited airway inflammation and AHR, and increased adipokine levels. |
| Scott HA 2011, ERJ [93] | Obese (n = 68) and nonobese (n = 47) adults with asthma, and obese (n = 16) and nonobese (n = 63) healthy controls | Sputum neutrophil percentage was positively associated with BMI in females with asthma and neutrophilic asthma was present in a greater proportion of obese compared with non-obese females. |
| Telenga ED 2012 [94] | 276 asthmatic patients (53 bese) | Obese women had significantly higher blood neutrophils. After a two-week treatment with corticosteroids, less corticosteroid-induced improvement in FEV-1% predicted was observed in obese patients than in lean patients. |
| Kim HY 2014 Nat Med [95] | Murine model | In obese mice airway hypereactivity (AHR) was dependent on IL-AHR was also associated with the expansion of type 3 innate lymphoid cells producing IL-17. |
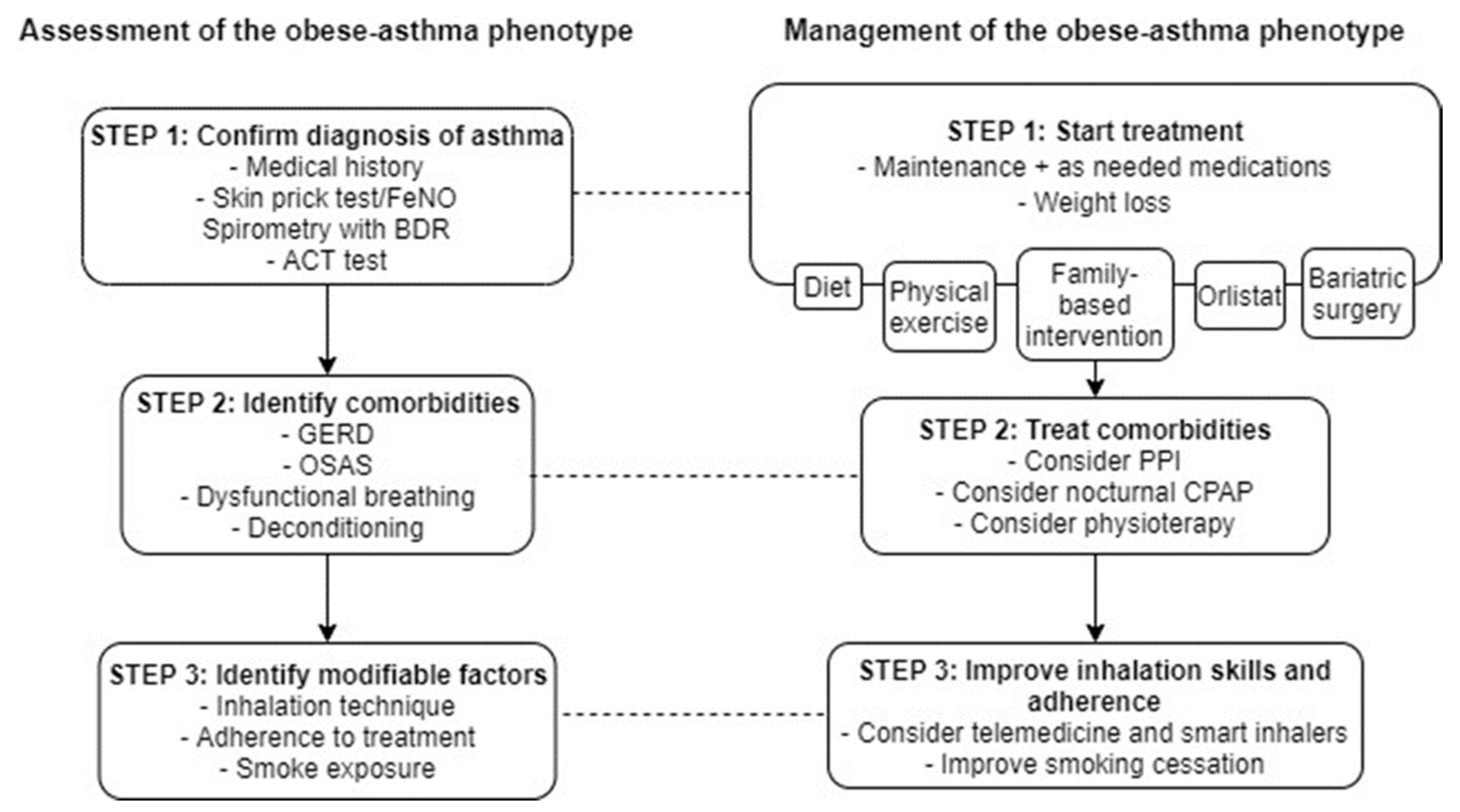
5. Treatment of the Obese-Asthma Phenotype
5.1. Exercise, Weight Loss, Diet
5.2. Pharmacotherapy
5.3. Vitamin D
6. Management of “Obese-Asthma” Comorbidities and Potential Triggers
7. Future Prospective
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pearce, N.; Aït-Khaled, N.; Beasley, R.; Mallol, J.; Keil, U.; Mitchell, E.; Robertson, C.; ISAAC Phase Three Study Group. Worldwide trends in the prevalence of asthma symptoms: Phase III of the international study of asthma and allergies in childhood (ISAAC). Thorax 2007, 62, 757–765. [Google Scholar] [CrossRef] [PubMed]
- Reddel, H.K.; Bacharier, L.B.; Bateman, E.D.; Brightling, C.E.; Brusselle, G.G.; Buhl, R.; Cruz, A.A.; Duijts, L.; Drazen, J.M.; FitzGerald, J.M.; et al. Global initiative for asthma (GINA) strategy 2021—Executive summary and rationale for key changes. Am. J. Respir. Crit. Care Med. 2022, 205, 17–35. [Google Scholar] [CrossRef] [PubMed]
- Fainardi, V.; Esposito, S.; Chetta, A.; Pisi, G. Asthma phenotypes and endotypes in childhood. Minerva Med. 2021. [Google Scholar] [CrossRef]
- Woodruff, P.G.; Modrek, B.; Choy, D.F.; Jia, G.; Abbas, A.R.; Ellwanger, A.; Koth, L.L.; Arron, J.R.; Fahy, J.V. T-helper type 2-driven inflammation defines major subphenotypes of asthma. Am. J. Respir. Crit. Care Med. 2009, 180, 388, Erratum in Am. J. Respir. Crit. Care Med. 2009, 180, 796. [Google Scholar] [CrossRef]
- Hedlin, G.; Bush, A.; Lødrup Carlsen, K.; Wennergren, G.; De Benedictis, F.M.; Melén, E.; Paton, J.; Wilson, N.; Carlsen, K.H. Problematic severe asthma in children, not one problem but many: A GA 2LEN initiative. Eur. Respir. J. 2010, 36, 196–201. [Google Scholar] [CrossRef]
- Bush, A.; Hedlin, G.; Carlsen, K.-H.; de Benedictis, F.; Lodrup-Carlsen, K.; Wilson, N. Severe childhood asthma: A common international approach? Lancet 2008, 372, 1019–1021. [Google Scholar] [CrossRef]
- Fainardi, V.; Saglani, S. An approach to the management of children with problematic severe asthma. Acta Bio Med. Atenei Parm. 2020, 91, e2020055. [Google Scholar]
- Poddighe, D.; Brambilla, I.; Licari, A.; Marseglia, G.L. Pediatric rhinosinusitis and asthma. Respir. Med. 2018, 141, 94–99. [Google Scholar] [CrossRef]
- Di Cesare, M.; Sorić, M.; Bovet, P.; Miranda, J.J.; Bhutta, Z.; Stevens, G.A.; Laxmaiah, A.; Kengne, A.-P.; Bentham, J. The epidemiological burden of obesity in childhood: A worldwide epidemic requiring urgent action. BMC Med. 2019, 17, 212. [Google Scholar] [CrossRef]
- Cottrell, L.; Neal, W.A.; Ice, C.; Perez, M.K.; Piedimonte, G. Metabolic abnormalities in children with asthma. Am. J. Respir. Crit. Care Med. 2011, 183, 441–448. [Google Scholar] [CrossRef]
- Di Palmo, E.; Filice, E.; Cavallo, A.; Caffarelli, C.; Maltoni, G.; Miniaci, A.; Ricci, G.; Pession, A. Childhood obesity and respiratory diseases: Which link? Children 2021, 8, 177. [Google Scholar] [CrossRef]
- Bantulà, M.; Roca-Ferrer, J.; Arismendi, E.; Picado, C. Asthma and obesity: Two diseases on the rise and bridged by inflammation. J. Clin. Med. 2021, 10, 169. [Google Scholar] [CrossRef]
- Liu, P.-C.; Kieckhefer, G.M.; Gau, B.-S. A systematic review of the association between obesity and asthma in children. J. Adv. Nurs. 2013, 69, 1446–1465. [Google Scholar] [CrossRef]
- Ali, Z.; Ulrik, C.S. Obesity and asthma: A coincidence or a causal relationship? A systematic review. Respir. Med. 2013, 107, 1287–1300. [Google Scholar] [CrossRef]
- Zhang, Y.; Chen, Z.; Berhane, K.; Urman, R.; Chatzi, V.L.; Breton, C.; Gilliland, F.D. The dynamic relationship between asthma and obesity in school children. Am. J. Epidemiol. 2020, 189, 583–591. [Google Scholar] [CrossRef] [PubMed]
- Egan, K.B.; Ettinger, A.S.; Bracken, M.B. Childhood body mass index and subsequent physician-diagnosed asthma: A systematic review and meta-analysis of prospective cohort studies. BMC Pediatr. 2013, 13, 1. [Google Scholar] [CrossRef]
- Sansone, F.; Attanasi, M.; Di Pillo, S.; Chiarelli, F. Asthma and obesity in children. Biomedicines 2020, 8, 231. [Google Scholar] [CrossRef]
- Tsai, H.J.; Wang, G.; Hong, X.; Yao, T.C.; Ji, Y.; Radovick, S.; Ji, H.; Cheng, T.L.; Wang, X. Early life weight gain and development of childhood asthma in a prospective birth cohort. Ann. Am. Thorac. Soc. 2018, 15, 1197–1204. [Google Scholar] [CrossRef]
- Contreras, Z.A.; Chen, Z.; Roumeliotaki, T.; Annesi-Maesano, I.; Baïz, N.; von Berg, A.; Bergström, A.; Crozier, S.; Duijts, L.; Ekström, S.; et al. Does early onset asthma increase childhood obesity risk? A pooled analysis of 16 European cohorts. Eur. Respir. J. 2018, 52, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Davis, A.; Lipsett, M.; Milet, M.; Etherton, M.; Kreutzer, R. An association between asthma and BMI in adolescents: Results from the California Healthy Kids Survey. J. Asthma. 2007, 44, 873–879. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.C.; Dong, G.H.; Lin, K.C.; Lee, Y.L. Gender difference of childhood overweight and obesity in predicting the risk of incident asthma: A systematic review and meta-analysis. Obes. Rev. 2013, 14, 222–231. [Google Scholar] [CrossRef]
- Lang, J.E.; Bunnell, H.T.; Lima, J.J.; Hossain, M.J.; Wysocki, T.; Bacharier, L.; Dempsey, A.; Ulrich, L.; Test, M.R.; Forrest, C.B. Effects of age, sex, race/ethnicity, and allergy status in obesity-related pediatric asthma. Pediatr. Pulmonol. 2019, 54, 1684–1693. [Google Scholar] [CrossRef]
- Barros, L.L.; Souza-Machado, A.; Corrêa, L.B.; Santos, J.S.; Cruz, C.; Leite, M.; Castro, L.; Coelho, A.C.; Almeida, P.; Cruz, A.A. Obesity and poor asthma control in patients with severe asthma. J. Asthma. 2011, 48, 171–176. [Google Scholar] [CrossRef]
- De Jesus, J.P.V.; Lima-Matos, A.S.; Almeida, P.C.A.; Lima, V.B.; de Mello, L.M.; Souza-Machado, A.; Ponte, E.V.; Cruz, Á.A. Obesity and asthma: Clinical and laboratory characterization of a common combination. J. Bras. Pneumol. 2018, 44, 207–212. [Google Scholar] [CrossRef]
- Peters, M.C.; Mauger, D.; Ross, K.R.; Phillips, B.; Gaston, B.; Cardet, J.C.; Israel, E.; Levy, B.D.; Phipatanakul, W.; Jarjour, N.N.; et al. Evidence for Exacerbation-Prone Asthma and Predictive Biomarkers of Exacerbation Frequency. Am. J. Respir. Crit. Care Med. 2020, 202, 973–982. [Google Scholar] [CrossRef]
- Peters, M.C.; Ringel, L.; Dyjack, N.; Herrin, R.; Woodruff, P.G.; Rios, C.; O’Connor, B.; Fahy, J.V.; Seibold, M.A. A transcriptomic method to determine airway immune dysfunction in T2-high and T2-low asthma. Am. J. Respir. Crit. Care Med. 2019, 199, 465–477. [Google Scholar] [CrossRef]
- Parlar-Chun, R.; Truong, G.; Isbell, T.; Delgado, Y.; Arca, M. Association of obesity with severity outcomes in hospitalized pediatric asthma exacerbations. J. Asthma. 2020, 3, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Engelkes, M.; Baan, E.J.; de Ridder, M.A.J.; Svensson, E.; Prieto-Alhambra, D.; Lapi, F.; Giaquinto, C.; Picelli, G.; Boudiaf, N.; Albers, F.; et al. Incidence, risk factors and re-exacerbation rate of severe asthma exacerbations in a multinational, multidatabase pediatric cohort study. Pediatr. Allergy Immunol. 2020, 31, 496–505. [Google Scholar] [PubMed]
- Orriëns, L.B.; Vijverberg, S.J.H.; Maitland van der Zee, A.H.; Longo, C. Nonadherence to inhaled corticosteroids: A characteristic of the pediatric obese-asthma phenotype? Pediatr. Pulmonol. 2021, 56, 948–956. [Google Scholar] [CrossRef]
- Chen, Z.; Salam, M.T.; Alderete, T.L.; Habre, R.; Bastain, T.M.; Berhane, K.; Gilliland, F.D. Effects of childhood asthma on the development of obesity among school-aged children. Am. J. Respir. Crit. Care Med. 2017, 195, 1181–1188. [Google Scholar] [PubMed]
- Shan, L.S.; Zhou, Q.L.; Shang, Y.X. Bidirectional association between asthma and obesity during childhood and adolescence: A systematic review and meta-analysis. Front. Pediatr. 2020, 8, 688. [Google Scholar] [CrossRef]
- Green, T.L. Examining the temporal relationships between childhood obesity and asthma. Econ. Hum. Biol. 2014, 14, 92–102. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Mohanan, S.; Tapp, H.; McWilliams, A.; Dulin, M. Obesity and asthma: Pathophysiology and implications for diagnosis and management in primary care. Exp. Biol. Med. 2014, 239, 1531–1540. [Google Scholar] [CrossRef] [PubMed]
- Jiang, D.; Wang, L.; Bai, C.; Chen, O. Association between abdominal obesity and asthma: A meta-analysis. Allergy Asthma Clin. Immunol. 2019, 15, 16. [Google Scholar] [CrossRef]
- Forno, E.; Weiner, D.J.; Mullen, J.; Sawicki, G.; Kurland, G.; Han, Y.Y.; Cloutier, M.M.; Canino, G.; Weiss, S.T.; Litonjua, A.A.; et al. Obesity and airway dysanapsis in children with and without asthma. Am. J. Respir. Crit. Care Med. 2017, 195, 314–323. [Google Scholar] [CrossRef] [PubMed]
- Gaffin, J.M.; Castro, M.; Bacharier, L.B.; Fuhlbrigge, A.L. The Role of Comorbidities in Difficult-to-Control Asthma in Adults and Children. J. Allergy Clin. Immunol. Pract. 2021. [Google Scholar] [CrossRef]
- Pellegrino, R.; Viegi, G.; Brusasco, V.; Crapo, R.O.; Burgos, F.; Casaburi, R.; Coates, A.; van der Grinten, C.P.; Gustafsson, P.; Hankinson, J.; et al. Interpretative strategies for lung function tests. Eur. Respir. J. 2005, 26, 948–968. [Google Scholar] [CrossRef]
- Afshar-Mohajer, N.; Wu, T.D.; Shade, R.; Brigham, E.; Woo, H.; Wood, M.; Koehl, R.; Koehler, K.; Kirkness, J.; Hansel, N.N.; et al. Obesity, tidal volume, and pulmonary deposition of fine particulate matter in children with asthma. Eur. Respir. J. 2021. [Google Scholar] [CrossRef]
- Berhane, K.; Chang, C.-C.; McConnell, R.; Gauderman, W.J.; Avol, E.; Rapapport, E.; Urman, R.; Lurmann, F.; Gilliland, F. Association of changes in air quality with bronchitic symptoms in children in California, 1993. JAMA 2016, 315, 1491–1501. [Google Scholar] [CrossRef]
- Calcaterra, V.; Verduci, E.; Ghezzi, M.; Cena, H.; Pascuzzi, M.C.; Regalbuto, C.; Lamberti, R.; Rossi, V.; Manuelli, M.; Bosetti, A.; et al. Pediatric obesity-related asthma: The role of nutrition and nutrients in prevention and treatment. Nutrients 2021, 13, 3708. [Google Scholar] [CrossRef]
- MacDonald, K.D.; Moran, A.R.; Scherman, A.J.; McEvoy, C.T.; Platteau, A.S. Maternal high-fat diet in mice leads to innate airway hyperresponsiveness in the adult offspring. Physiol. Rep. 2017, 5, e13082. [Google Scholar] [CrossRef]
- Mensink-Bout, S.M.; van Meel, E.R.; de Jongste, J.C.; Annesi-Maesano, I.; Aubert, A.M.; Bernard, J.Y.; Chen, L.W.; Cooper, C.; Crozier, S.R.; Hanke, W.; et al. Maternal diet in pregnancy and child’s respiratory outcomes: An individual participant data meta-analysis of 18,000 children. Eur. Respir. J. 2021. [Google Scholar] [CrossRef] [PubMed]
- Patro Golab, B.; Santos, S.; Voerman, E.; Lawlor, D.A.; Jaddoe, V.W.V.; Gaillard, R.; MOCO Study Group Authors. Influence of maternal obesity on the association between common pregnancy complications and risk of childhood obesity: An individual participant data meta-analysis. Lancet Child Adolesc. Health 2018, 2, 812–821. [Google Scholar] [CrossRef]
- Rusconi, F.; Popovic, M. Maternal obesity and childhood wheezing and asthma. Paediatr. Respir. Rev. 2017, 22, 66–71. [Google Scholar] [CrossRef] [PubMed]
- Sood, A.; Shore, S.A. Adiponectin, leptin, and resistin in asthma: Basic mechanisms through population studies. J. Allergy 2013, 2013, 785835. [Google Scholar] [CrossRef]
- Gomez-Llorente, M.A.; Romero, R.; Chueca, N.; Martinez-Cañavate, A.; Gomez-Llorente, C. Obesity and asthma: A missing link. Int. J. Mol. Sci. 2017, 18, 1490. [Google Scholar] [CrossRef]
- Vijayakanthi, N.; Greally, J.M.; Rastogi, D. Pediatric obesity-related asthma: The role of metabolic dysregulation. Pediatrics 2016, 137, 5. [Google Scholar] [CrossRef]
- Guler, N.; Kirerleri, E.; Ones, U.; Tamay, Z.; Salmayenli, N.; Darendeliler, F. Leptin: Does it have any role in childhood asthma? J. Allergy Clin. Immunol. 2004, 114, 254–259. [Google Scholar] [CrossRef]
- Al-Ayed, M.; Alshaybari, K.; Alshehri, D.; Jamaan, A.; Nasser, I.; Alaamri, H.; Alaseeri, W.; Mahfouz, A.A.; Ali Alsareli, S.; Asaad, A.M.; et al. Obesity and childhood asthma in male schoolchildren in Saudi Arabia: Is there a role for leptin, interleukin-4, interleukin-5, and interleukin-21? Ann. Saudi Med. 2019, 39, 295–301. [Google Scholar] [CrossRef]
- Zhang, X.; Zheng, J.; Zhang, L.; Liu, Y.; Chen, G.P.; Zhang, H.P.; Wang, L.; Kang, Y.; Wood, L.G.; Wang, G. Systemic inflammation mediates the detrimental effects of obesity on asthma control. Allergy Asthma Proc. 2018, 39, 43–50. [Google Scholar] [CrossRef]
- Castro-Rodriguez, J.A.; Forno, E.; Casanello, P.; Padilla, O.; Krause, B.J.; Uauy, R. Leptin in cord blood associates with asthma risk at age 3 in the offspring of women with gestational obesity. Ann. Am. Thorac. Soc. 2020, 17, 1583–1589. [Google Scholar] [CrossRef]
- Yuksel, H.; Sogut, A.; Yilmaz, O.; Onur, E.; Dinc, G. Role of adipokines and hormones of obesity in childhood asthma. Allergy Asthma Immunol. Res. 2012, 4, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Szczepankiewicz, D.; Skrzypski, M.; Pruszyńska-Oszmałek, E.; Kołodziejski, P.A.; Sassek, M.; Stefańska, B.; Nowak, K.W.; Szczepankiewicz, A. Interleukin 4 affects lipid metabolism and the expression of pro-inflammatory factors in mature rat adipocytes. Immunobiology 2018, 223, 677–683. [Google Scholar] [CrossRef]
- Hallstrand, T.S.; Fischer, M.E.; Wurfel, M.M.; Afari, N.; Buchwald, D.; Goldberg, J. Genetic pleiotropy between asthma and obesity in a community-based sample of twins. J. Allergy Clin. Immunol. 2005, 116, 1235–1241. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Tantisira, K.G.; Weiss, S.T. Complex interactions in complex traits: Obesity and asthma. Thorax 2001, 56 (Suppl. S2), ii64–ii73. [Google Scholar] [PubMed]
- Zhu, Z.; Guo, Y.; Shi, H.; Liu, C.-L.; Panganiban, R.A.; Chung, W.; O’Connor, L.J.; Himes, B.E.; Gazal, S.; Hasegawa, K.; et al. Shared genetic and experimental links between obesity-related traits and asthma subtypes in UK Biobank. J. Allergy Clin. Immunol. 2020, 145, 537–549. [Google Scholar] [CrossRef]
- Rastogi, D.; Suzuki, M.; Greally, J.M. Differential epigenome-wide DNA methylation patterns in childhood obesity-associated asthma. Sci Rep. 2013, 3, 2164. [Google Scholar] [CrossRef]
- Karampatakis, N.; Karampatakis, T.; Galli-Tsinopoulou, A.; Kotanidou, E.P.; Tsergouli, K.; Eboriadou-Petikopoulou, M.; Haidopoulou, K. Impaired glucose metabolism and bronchial hyperresponsiveness in obese prepubertal asthmatic children. Pediatr. Pulmonol. 2017, 52, 160–166. [Google Scholar] [CrossRef]
- Arshi, M.; Cardinal, J.; Hill, R.J.; Davies, P.S.W.; Wainwright, C. Asthma and insulin resistance in children. Respirology 2010, 15, 779–784. [Google Scholar] [CrossRef]
- Perez, M.K.; Piedimonte, G. Metabolic asthma: Is there a link between obesity, diabetes, and asthma? Immunol. Allergy Clin. N. Am. 2014, 34, 777–784. [Google Scholar] [CrossRef]
- Zhuang, L.; Chen, H.; Zhang, S.; Zhuang, J.; Li, Q.; Feng, Z. Intestinal microbiota in early life and its implications on childhood health. Genom. Proteom. Bioinform. 2019, 17, 13–25. [Google Scholar] [CrossRef] [PubMed]
- Raymond, S.L.; Rincon, J.C.; Wynn, J.L.; Moldawer, L.L.; Larson, S.D. Impact of early-life exposures to infections, antibiotics, and vaccines on perinatal and long-term health and disease. Front. Immunol. 2017, 8, 729. [Google Scholar] [CrossRef]
- Bokulich, N.A.; Chung, J.; Battaglia, T.; Henderson, N.; Jay, M.; Li, H.; Lieber, A.D.; Wu, F.; Perez-Perez, G.I.; Chen, Y.; et al. Antibiotics, birth mode, and diet shape microbiome maturation during early life. Sci. Transl. Med. 2016, 8, 343ra82. [Google Scholar] [CrossRef]
- Peters, U.; Dixon, A.E.; Forno, E. Obesity and asthma. J. Allergy Clin. Immunol. 2018, 141, 1169–1179. [Google Scholar] [CrossRef]
- Williams, B.; Powell, A.; Hoskins, G.; Neville, R. Exploring and explaining low participation in physical activity among children and young people with asthma: A review. BMC Fam. Pract. 2008, 9, 40. [Google Scholar] [CrossRef] [PubMed]
- Souza de Almeida, A.H.; de Rodrigues Filho, E.A.; Lubambo Costa, E.; de Albuquerque, C.G.; Sarinho, E.S.C.; Medeiros Peixoto, D.; Dela Bianca, A.C.C.; Correia Júnior, M.A.V.; Rizzo, J.Â. Obesity is a risk factor for exercise-induced bronchospasm in asthmatic adolescents. Pediatr. Pulmonol. 2020, 55, 1916–1923. [Google Scholar] [CrossRef]
- Umławska, W. Adipose tissue content and distribution in children and adolescents with bronchial asthma. Respir. Med. 2015, 109, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Rastogi, D. Pediatric obesity-related asthma: A prototype of pediatric severe non-T2 asthma. Pediatr. Pulmonol. 2020, 55, 809–817. [Google Scholar] [CrossRef]
- Martin Alonso, A.; Fainardi, V.; Saglani, S. Severe therapy resistant asthma in children: Translational approaches to uncover sub-phenotypes. Expert Rev. Respir. Med. 2017, 11, 867–874. [Google Scholar] [CrossRef]
- Weinmayr, G.; Forastiere, F.; Bu, G.; Jaensch, A.; Strachan, D.P.; Nagel, G. Overweight/obesity and respiratory and allergic disease in children: International study of asthma and allergies in childhood (ISAAC) phase two. PLoS ONE 2014, 9, e113996. [Google Scholar] [CrossRef]
- Denlinger, L.C.; Phillips, B.R.; Ramratnam, S.; Ross, K.; Bhakta, N.R.; Cardet, J.C.; Castro, M.; Peters, S.P.; Phipatanakul, W.; Aujla, S.; et al. Inflammatory and comorbid features of patients with severe asthma and frequent exacerbations. Am. J. Respir. Crit. Care Med. 2017, 195, 302–313. [Google Scholar] [CrossRef] [PubMed]
- Dixon, A.E.; Poynter, M.E. Mechanisms of asthma in obesity pleiotropic aspects of obesity produce distinct asthma phenotypes. Am. J. Respir. Cell Mol. Biol. 2016, 54, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Kuruvilla, M.E.; Lee, F.E.H.; Lee, G.B. Understanding asthma phenotypes, endotypes, and mechanisms of disease. Clin. Rev. Allergy Immunol. 2019, 56, 219–233. [Google Scholar] [CrossRef] [PubMed]
- Unamuno, X.; Gómez-Ambrosi, J.; Rodríguez, A.; Becerril, S.; Frühbeck, G.; Catalán, V. Adipokine dysregulation and adipose tissue inflammation in human obesity. Eur. J. Clin. Investig. 2018, 48, e12997. [Google Scholar] [CrossRef] [PubMed]
- Zeyda, M.; Farmer, D.; Todoric, J.; Aszmann, O.; Speiser, M.; Györi, G. Human adipose tissue macrophages are of an anti-inflammatory phenotype but capable of excessive pro-inflammatory mediator production. Int. J. Obes. 2007, 31, 1420–1428. [Google Scholar] [CrossRef] [PubMed]
- Ferrante, A.W., Jr. The immune cells in adipose tissue. Diabetes Obes. Metab. 2013, 15 (Suppl. S3), 34–38. [Google Scholar] [CrossRef]
- Jensen, M.E.; Gibson, P.G.; Collins, C.E.; Wood, L.G. Airway and systemic inflammation in obese children with asthma. Eur. Respir. J. 2013, 42, 1012–1019. [Google Scholar] [CrossRef]
- Al-Ramli, W.; Préfontaine, D.; Chouiali, F.; Martin, J.G.; Olivenstein, R.; Lemiere, C.; Hamid, Q. TH17-associated cytokines (IL-17A and IL-17F) in severe asthma. J. Allergy Clin. Immunol. 2009, 123, 1185–1187. [Google Scholar] [CrossRef]
- Chambers, E.S.; Nanzer, A.M.; Pfeffer, P.E.; Richards, D.F.; Timms, P.M.; Martineau, A.R.; Griffiths, C.J.; Corrigan, C.J.; Hawrylowicz, C.M. Distinct endotypes of steroid-resistant asthma characterized by IL-17A high and IFN-γ high immunophenotypes: Potential benefits of calcitriol. J. Allergy Clin. Immunol. 2015, 136, 628–637.e4. [Google Scholar] [CrossRef]
- Oda, N.; Canelos, P.B.; Essayan, D.M.; Plunkett, B.A.; Myers, A.C.; Huang, S.-K. Interleukin-17F induces pulmonary neutrophilia and amplifies antigen-induced allergic response. Am. J. Respir. Crit. Care Med. 2005, 171, 12–18. [Google Scholar] [CrossRef]
- Kudo, M.; Melton, A.C.; Chen, C.; Engler, M.B.; Huang, K.E.; Ren, X.; Wang, Y.; Bernstein, X.; Li, J.T.; Atabai, K.; et al. IL-17A produced by αβ T cells drives airway hyper-responsiveness in mice and enhances mouse and human airway smooth muscle contraction. Nat. Med. 2012, 18, 547–554. [Google Scholar] [CrossRef]
- Ardain, A.; Porterfield, J.Z.; Kløverpris, H.N.; Leslie, A. Type 3 ILCs in lung disease. Front. Immunol. 2019, 10, 92. [Google Scholar] [CrossRef]
- Schaper, F.; Rose-John, S. Interleukin-6: Biology, signaling and strategies of blockade. Cytokine Growth Factor Rev. 2015, 26, 475–487. [Google Scholar] [CrossRef] [PubMed]
- Farahi, N.; Paige, E.; Balla, J.; Prudence, E.; Ferreira, R.C.; Southwood, M.; Appleby, S.L.; Bakke, P.; Gulsvik, A.; Litonjua, A.A.; et al. Neutrophil-mediated IL-6 receptor trans-signaling and the risk of chronic obstructive pulmonary disease and asthma. Hum. Mol. Genet. 2017, 26, 1584–1596. [Google Scholar] [CrossRef] [PubMed]
- Peters, M.C.; McGrath, K.W.; Hawkins, G.A.; Hastie, A.T.; Levy, B.D.; Israel, E.; Phillips, B.R.; Mauger, D.T.; Comhair, S.A.; Erzurum, S.C.; et al. Plasma interleukin-6 concentrations, metabolic dysfunction, and asthma severity: A cross-sectional analysis of two cohorts. Lancet Respir. Med. 2016, 4, 574–584. [Google Scholar] [CrossRef]
- Jevnikar, Z.; Östling, J.; Ax, E.; Calvén, J.; Thörn, K.; Israelsson, E.; Öberg, L.; Singhania, A.; Lau, L.C.; Wilson, S.J.; et al. Epithelial IL-6 trans-signaling defines a new asthma phenotype with increased airway inflammation. J. Allergy Clin. Immunol. 2019, 143, 577–590. [Google Scholar] [CrossRef] [PubMed]
- Park, H.S.; Park, J.Y.; Yu, R. Relationship of obesity and visceral adiposity with serum concentrations of CRP, TNF-α and IL-6. Diabetes Res. Clin. Pract. 2005, 69, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Jackson, D.J.; Bacharier, L.B.; Calatroni, A.; Gill, M.A.; Hu, J.; Liu, A.H.; Wheatley, L.M.; Gern, J.E.; Gruchalla, R.S.; Hershey, G.K.K.; et al. Serum IL-6: A biomarker in childhood asthma? J. Allergy Clin. Immunol. 2020, 145, 1701–1704.e3. [Google Scholar] [CrossRef]
- Raundhal, M.; Morse, C.; Khare, A.; Oriss, T.B.; Milosevic, J.; Trudeau, J.B.; Huff, R.; Pilewski, J.M.; Holguin, F.; Kolls, J.K.; et al. High IFN-γ and low SLPI mark severe asthma in mice and humans. J. Clin. Investig. 2015, 125, 3037–3050. [Google Scholar] [CrossRef]
- Rastogi, D.; Canfi, S.M.; Andrade, A. Obesity-associated asthma in children. Allergol. Select. 2020, 4, 76–85. [Google Scholar] [CrossRef]
- Holguin, F.; Bleecker, E.R.; Busse, W.W.; Calhoun, W.J.; Castro, M.; Erzurum, S.C.; Fitzpatrick, A.M.; Gaston, B.; Israel, E.; Jarjour, N.N.; et al. Obesity and asthma: An association modified by age of asthma onset. J. Allergy Clin. Immunol. 2011, 127, 1486–1493.e2. [Google Scholar] [CrossRef] [PubMed]
- Liang, L.; Hur, J.; Kang, J.Y.; Rhee, C.K.; Kim, Y.K.; Lee, S.Y. Effect of the anti-il-17 antibody on allergic inflammation in an obesity-related asthma model. Korean J. Intern. Med. 2018, 33, 1210–1223. [Google Scholar] [CrossRef] [PubMed]
- Scott, H.A.; Gibson, P.G.; Garg, M.L.; Wood, L.G. Airway inflammation is augmented by obesity and fatty acids in asthma. Eur. Respir. J. 2011, 38, 594–602. [Google Scholar] [CrossRef] [PubMed]
- Telenga, E.D.; Tideman, S.W.; Kerstjens, H.A.; Hacken, N.H.; Timens, W.; Postma, D.S.; van den Berge, M. Obesity in asthma: More neutrophilic inflammation as a possible explanation for a reduced treatment response. Allergy 2012, 67, 1060–1068. [Google Scholar] [CrossRef]
- Kim, H.Y.; Lee, H.J.; Chang, Y.J.; Pichavant, M.; Shore, S.A.; Fitzgerald, K.A.; Iwakura, Y.; Israel, E.; Bolger, K.; Faul, J.; et al. Interleukin-17-producing innate lymphoid cells and the NLRP3 inflammasome facilitate obesity-associated airway hyperreactivity. Nat. Med. 2014, 20, 54–61. [Google Scholar] [CrossRef]
- Eng, C.; Davis, A.; Meade, K.; Lenoir, M.A.; Avila, P.C. Obesity and bronchodilator response in black and hispanic children and adolescents with asthma. Chest 2015, 147, 1591–1598. [Google Scholar]
- Pradeepan, S.; Garrison, G.; Dixon, A.E. Obesity in asthma: Approaches to treatment. Curr. Allergy Asthma Rep. 2013, 13, 434–442. [Google Scholar] [CrossRef]
- Sutherland, E.R.; Goleva, E.; Strand, M.; Beuther, D.A.; Leung, D.Y.M. Body mass and glucocorticoid response in asthma. Am. J. Respir. Crit. Care Med. 2008, 178, 682–687. [Google Scholar] [CrossRef] [PubMed]
- Maltby, S.; Tay, H.L.; Yang, M.; Foster, P.S. Mouse models of severe asthma: Understanding the mechanisms of steroid resistance, tissue remodelling and disease exacerbation. Respirology 2017, 22, 874–885. [Google Scholar] [CrossRef]
- Baek, H.S.; Kim, Y.D.; Shin, J.H.; Kim, J.H.; Oh, J.W.; Lee, H.B. Serum leptin and adiponectin levels correlate with exercise-induced bronchoconstriction in children with asthma. Ann. Allergy Asthma Immunol. 2011, 107, 14–21. [Google Scholar] [CrossRef]
- Jensen, M.E.; Gibson, P.G.; Collins, C.E.; Hilton, J.M.; Wood, L.G. Diet-induced weight loss in obese children with asthma: A randomized controlled trial. Clin. Exp. Allergy. 2013, 43, 775–784. [Google Scholar] [CrossRef] [PubMed]
- Scott, H.A.; Gibson, P.G.; Garg, M.L.; Pretto, J.J.; Morgan, P.J.; Callister, R.; Wood, L.G. Dietary restriction and exercise improve airway inflammation and clinical outcomes in overweight and obese asthma: A randomized trial. Clin. Exp. Allergy 2013, 43, 36–49. [Google Scholar] [CrossRef]
- Willeboordse, M.; Kant KDGVan De Tan, F.E.S.; Mulkens, S.; Schellings, J.; Crijns, Y.; van der Ploeg, L.; van Schayck, C.P.; Dompeling, E. A Multifactorial Weight Reduction Programme for Children with Overweight and Asthma: A Randomized Controlled Trial. PLoS ONE. 2016, 11, e0157158. [Google Scholar]
- Clarke, R.; Heath, G.; Nagakumar, P.; Pattison, H.; Farrow, C. “He’s not fat, he just has asthma”: A qualitative study exploring weight management in families living with pediatric asthma. J. Asthma. 2021, 1, 1–12. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services. Physical Activity Guidelines for Americans, 2nd ed.; U.S. Department of Health and Human Services: Washington, DC, USA, 2018. Available online: https://health.gov/sites/default/files/2019-09/Physical_Activity_Guidelines_2nd_edition.pdf (accessed on 20 December 2021).
- Leinaar, E.; Alamian, A.; Wang, L. A systematic review of the relationship between asthma, overweight, and the effects of physical activity in youth. Ann. Epidemiol. 2016, 26, 504–510.e6. [Google Scholar] [CrossRef]
- Lu, K.D.; Forno, E.; Radom-Aizik, S.; Cooper, D.M. Low fitness and increased sedentary time are associated with worse asthma—The national youth fitness survey. Pediatr. Pulmonol. 2020, 55, 1116–1123. [Google Scholar] [CrossRef]
- Onur, E.; Kabaroĝlu, C.; Günay, Ö.; Var, A.; Yilmaz, Ö.; Dündar, P.; Tikiz, C.; Güvenç, Y.; Yüksel, H. The beneficial effects of physical exercise on antioxidant status in asthmatic children. Allergol. Immunopathol. 2011, 39, 90–95. [Google Scholar] [CrossRef]
- Willeboordse, M.; Van De Kant, K.D.G.; Van Der Velden, C.A.; Van Schayck, C.P. Associations between asthma, overweight and physical activity in children: A cross-sectional study. BMC Public Health 2016, 16, 919. [Google Scholar] [CrossRef]
- Borrell, L.N.; Nguyen, E.A.; Roth, L.A.; Oh, S.S.; Tcheurekdjian, H.; Sen, S.; Davis, A.; Farber, H.J.; Avila, P.C.; Brigino-Buenaventura, E.; et al. Childhood obesity and asthma control in the GALA II and SAGE II studies. Am. J. Respir. Crit. Care Med. 2013, 187, 697–702. [Google Scholar] [CrossRef]
- Trompette, A.; Gollwitzer, E.S.; Yadava, K.; Sichelstiel, A.K.; Sprenger, N.; Ngom-Bru, C.; Blanchard, C.; Junt, T.; Nicod, L.P.; Harris, N.L.; et al. Gut microbiota metabolism of dietary fiber influences allergic airway disease and hematopoiesis. Nat. Med. 2014, 20, 159–166. [Google Scholar] [CrossRef]
- Nagel, G.; Weinmayr, G.; Kleiner, A.; García-Marcos, L.; Strachan, D.P.; Aït-Khaled, N. ISAAC Phase Two Study Group. Effect of diet on asthma and allergic sensitisation in the international study on allergies and asthma in childhood (ISAAC) phase two. Thorax 2010, 65, 516–522. [Google Scholar] [CrossRef]
- Lang, J.E.; Mougey, E.B.; Allayee, H.; Blake, K.V.; Lockey, R. Nutrigenetic response to omega-3 fatty acids in obese asthmatics (NOOA): Rationale and methods. Contemp. Clin. Trials 2013, 34, 326–335. [Google Scholar] [CrossRef] [PubMed]
- Mickleborough, T.D.; Murray, R.L.; Ionescu, A.A.; Lindley, M.R. Fish oil supplementation reduces severity of exercise-induced bronchoconstriction in elite athletes. Am. J. Respir. Crit. Care Med. 2003, 168, 1181–1189. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.; Poirier, P.; Boulet, L. Effect of bariatric surgery on airway response and lung function in obese subjects with asthma. Respir. Med. 2012, 106, 651–660. [Google Scholar]
- Hasegawa, K.; Tsugawa, Y.; Chang, Y. Risk of an asthma exacerbation after bariatric surgery in adults. J. Allergy Clin. Immunol. 2015, 136, 288–294.e8. [Google Scholar] [CrossRef] [PubMed]
- Styne, D.M.; Arslanian, S.A.; Connor, E.L.; Farooqi, I.S.; Murad, M.H.; Silverstein, J.H.; Yanovski, J.A. Pediatric obesity—Assessment, treatment, and prevention: An endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 2017, 102, 709–757. [Google Scholar] [CrossRef]
- Calixto, M.C.; Lintomen, L.; André, D.M.; Leiria, L.O.; Ferreira, D.; Lellis-Santos, C.; Anhê, G.F.; Bordin, S.; Landgraf, R.G.; Antunes, E. Metformin attenuates the exacerbation of the allergic eosinophilic inflammation in high fat-diet-induced obesity in mice. PLoS ONE 2013, 8, e76786. [Google Scholar] [CrossRef]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M.; Endocrine Society. Evaluation, treatment, and prevention of vitamin D deficiency: An endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef]
- Tashiro, H.; Shore, S.A. Obesity and severe asthma. Allergol. Int. 2019, 68, 135–142. [Google Scholar] [CrossRef]
- Lautenbacher, L.A.; Jariwala, S.P.; Markowitz, M.E.; Rastogi, D. Vitamin D and pulmonary function in obese asthmatic children. Pediatr. Pulmonol. 2016, 51, 1276–1283. [Google Scholar] [CrossRef]
- Di Genova, L.; Penta, L.; Biscarini, A.; Di Cara, G.; Esposito, S. Children with obesity and asthma: Which are the best options for their management? Nutrients 2018, 10, 1634. [Google Scholar] [CrossRef]
- O’Sullivan, B.P.; James, L.; Majure, J.M.; Bickel, S.; Phan, L.T.; Serrano Gonzalez, M.; Staples, H.; Tam-Williams, J.; Lang, J.; Snowden, J.; et al. Obesity-related asthma in children: A role for vitamin D. Pediatr. Pulmonol. 2021, 56, 354–361. [Google Scholar] [CrossRef]
- Tachimoto, H.; Mezawa, H.; Segawa, T.; Akiyama, N.; Ida, H.; Urashima, M. Improved control of childhood asthma with low-dose, short-term vitamin D supplementation: A randomized, double-blind, placebo-controlled trial. Allergy 2016, 71, 1001–1009. [Google Scholar] [CrossRef]
- Must, A.; Phillips, S.M.; Naumova, E.N. Occurrence and timing of childhood overweight and mortality: Findings from the third harvard growth study. J. Pediatr. 2012, 160, 743–750. [Google Scholar] [CrossRef]
- Shaw, D.E.; Sousa, A.R.; Fowler, S.J.; Fleming, L.J.; Roberts, G.; Corfield, J.; Pandis, I.; Bansal, A.T.; Bel, E.H.; Auffray, C.; et al. Clinical and inflammatory characteristics of the European U-BIOPRED adult severe asthma cohort. Eur. Respir. J. 2015, 46, 1308–1321. [Google Scholar] [CrossRef]
- Maio, S.; Baldacci, S.; Bresciani, M.; Simoni, M.; Latorre, M.; Murgia, N.; Spinozzi, F.; Braschi, M.; Antonicelli, L.; Brunetto, B.; et al. RItA: The Italian severe/uncontrolled asthma registry. Allergy 2018, 73, 683–695. [Google Scholar] [CrossRef]
- Moore, W.C.; Meyers, D.A.; Wenzel, S.E.; Teague, W.G.; Li, H.; Li, X.; D’Agostino, R., Jr.; Castro, M.; Curran-Everett, D.; Fitzpatrick, A.M.; et al. Identification of asthma phenotypes using cluster analysis in the severe asthma research program. Am. J. Respir. Crit. Care Med. 2010, 181, 315–323. [Google Scholar] [CrossRef]
- Perotin, J.M.; Schofield, J.P.R.; Wilson, S.J.; Ward, J.; Brandsma, J.; Strazzeri, F.; Bansal, A.; Yang, X.; Rowe, A.; Corfield, J.; et al. Epithelial dysregulation in obese severe asthmatics with gastro-oesophageal reflux. Eur. Respir. J. 2019, 53, 1900453. [Google Scholar] [CrossRef]
- Rogers, L. Role of sleep apnea and gastroesophageal reflux in severe asthma. Immunol. Allergy Clin. N. Am. 2016, 36, 461–471. [Google Scholar] [CrossRef]
- Davies, S.E.; Bishopp, A.; Wharton, S.; Turner, A.M.; Adel, H.M. The association between asthma and obstructive sleep apnea (OSA): A systematic review. J. Asthma. 2018, 56, 118–129. [Google Scholar] [CrossRef]
- Tsou, P.Y.; Cielo, C.; Xanthopoulos, M.S.; Wang, Y.H.; Kuo, P.L.; Tapia, I.E. Impact of obstructive sleep apnoea on severe asthma exacerbations. Pediatr. Pulmonol. 2021, 56, 1103–1113. [Google Scholar] [CrossRef]
- Wang, Y.; Meagher, R.B.; Ambati, S.; Ma, P.; Phillips, B.G. Patients with obstructive sleep apnea have suppressed levels of soluble cytokine receptors involved in neurodegenerative disease, but normal levels with airways therapy. Sleep Breath. 2021, 25, 1641–1653. [Google Scholar] [CrossRef]
- Simard, B.; Turcotte, H.; Marceau, P.; Biron, S.; Hould, F.S.; Lebel, S.; Marceau, S.; Boulet, L.P. Asthma and sleep apnea in patients with morbid obesity: Outcome after bariatric surgery. Obes Surg. 2004, 14, 1381–1388. [Google Scholar] [CrossRef]
- Veidal, S.; Jeppegaard, M.; Sverrild, A.; Backer, V.; Porsbjerg, C. The impact of dysfunctional breathing on the assessment of asthma control. Respir. Med. 2017, 123, 42–47. [Google Scholar] [CrossRef]
- Freitas, P.D.; Ferreira, P.G.; da Silva, A.; Trecco, S.; Stelmach, R.; Cukier, A.; Carvalho-Pinto, R.; Salge, J.M.; Fernandes, F.L.; Mancini, M.C.; et al. The effects of exercise training in a weight loss lifestyle intervention on asthma control, quality of life and psychosocial symptoms in adult obese asthmatics: Protocol of a randomized controlled trial. BMC Pulm. Med. 2015, 15, 124. [Google Scholar] [CrossRef]
- Wu, T.D.; Brigham, E.P.; Peng, R.; Koehler, K.; Rand, C.; Matsui, E.C.; Diette, G.B.; Hansel, N.N.; McCormack, M.C. Overweight/obesity enhances associations between secondhand smoke exposure and asthma morbidity in children. J. Allergy Clin. Immunol. Pract. 2018, 6, 2157–2159.e5. [Google Scholar] [CrossRef]
- Thomas, M.; McKinley, R.K.; Freeman, E.; Foy, C. Prevalence of dysfunctional breathing in patients treated for asthma in primary care: Cross sectional survey. Br. Med. J. 2001, 322, 1098–1100. [Google Scholar] [CrossRef]
- Sedeh, F.B.; Von Bülow, A.; Backer, V.; Bodtger, U.; Petersen, U.S.; Vest, S.; Hull, J.H.; Porsbjerg, C. The impact of dysfunctional breathing on the level of asthma control in difficult asthma. Respir. Med. 2020, 163, 105894. [Google Scholar] [CrossRef]
- Shim, Y.M.; Burnette, A.; Lucas, S.; Herring, R.C.; Weltman, J.; Patrie, J.T.; Weltman, A.L.; Platts-Mills, T.A. Physical deconditioning as a cause of breathlessness among obese adolescents with a diagnosis of asthma. PLoS ONE 2013, 8, e61022. [Google Scholar]
- Panagiotou, M.; Koulouris, N.G.; Rovina, N. Physical activity: A missing link in asthma care. J. Clin. Med. 2020, 9, 706. [Google Scholar] [CrossRef]
- Kobayashi, Y.; Bossley, C.; Gupta, A.; Akashi, K.; Tsartsali, L.; Mercado, N.; Barnes, P.J.; Bush, A.; Ito, K. Passive smoking impairs histone deacetylase-2 in children with severe asthma. Chest 2014, 145, 305–312. [Google Scholar] [CrossRef]
- Mackay, D.; Haw, S.; Ayres, J.G.; Fischbacher, C.; Pell, J.P. Smoke-free legislation and hospitalizations for childhood asthma. N. Engl. J. Med. 2010, 363, 1139–1145. [Google Scholar] [CrossRef]
- Kitsantas, P.; Aguisanda, F. Association of asthma with obesity among adolescents exposed to environmental tobacco smoke. J. Asthma. 2016, 53, 25–29. [Google Scholar] [CrossRef]
- Marseglia, G.L.; Avanzini, M.A.; Caimmi, S.; Caimmi, D.; Marseglia, A.; Valsecchi, C.; Poddighe, D.; Ciprandi, G.; Pagella, F.; Klersy, C.; et al. Passive exposure to smoke re-sults in defective interferon-gamma production by adenoids in children with recurrent respiratory infections. J. Interferon Cytokine Res. 2009, 29, 427–432. [Google Scholar] [CrossRef]
- Schroder, K.; Hertzog, P.J.; Ravasi, T.; Hume, D.A. Interferon-gamma: An overview of signals, mechanisms and functions. J. Leukoc. Biol. 2004, 75, 163–189. [Google Scholar] [CrossRef]
- Gentile, D.; Howe-Adams, J.; Trecki, J.; Patel, A.; Angelini, B.; Skoner, D. Association between environmental tobacco smoke and diminished dendritic cell interleukin 10 production during infancy. Ann. Allergy Asthma Immunol. 2004, 92, 433–437. [Google Scholar] [CrossRef]
- Hossny, E.M.; El-Sayed, S.S.; El-Hadidi, E.S.; Moussa, S.R. Serum interleukin-18 expression in children with bronchial asthma. World Allergy Organ J. 2009, 2, 63–68. [Google Scholar] [CrossRef]
- Hartmann-Boyce, J.; Hong, B.; Livingstone-Banks, J.; Wheat, H.; Fanshawe, T.R. Additional behavioural support as an adjunct to pharmacotherapy for smoking cessation. Cochrane Database Syst Rev. 2019, 6, CD009670. [Google Scholar] [CrossRef]
- Cook, J.; Beresford, F.; Fainardi, V.; Hall, P.; Housley, G.; Jamalzadeh, A.; Nightingale, M.; Winch, D.; Bush, A.; Fleming, L.; et al. Managing the pedia.atric patient with refractory asthma: A multidisciplinary approach. J. Asthma Allergy. 2017, 10, 123–130. [Google Scholar] [CrossRef]
- Lv, S.; Chief, D.; Xiaohong, N.; Physician, D.C.; Wang, Z.; Cai, X.; Chen, Y.; Cai, X.; Qian, X. A randomized controlled trial of a mobile application-assisted nurse-led model used to improve treatment outcomes in children with asthma. J. Adv. Nurs. 2019, 75, 3058–3067. [Google Scholar] [CrossRef]
- Fedele, D.; Lucero, R.; Janicke, D. Protocol for the development of a behavioral family lifestyle intervention supported by mobile health to improve weight self-management in children with asthma and obesity. JMIR Res. Protoc. 2019, 8, e13549. [Google Scholar] [CrossRef]
- Janicke, D.M.; Steele, R.G.; Gayes, L.A.; Lim, C.S.; Clifford, M.; Schneider, E.M.; Carmody, J.K.; Westen, S. Systematic review and meta-analysis of comprehensive behavioral family lifestyle interventions addressing pediatric obesity. J Pediatric Psychol. 2014, 39, 809–825. [Google Scholar] [CrossRef]
- Nichols, M.; Teufel, R.; Miller, S.; Madisetti, M.; Giovanni, C.S.; Chike-Harris, K.; Jones, L.; Prentice, M.; Ruggiero, K.; Kelechi, T. Managing asthma and obesity related symptoms (MATADORS): An mHealth intervention to facilitate symptom self-management among youth. Int. J. Environ. Res. Public Health 2020, 17, 7750. [Google Scholar] [CrossRef]


| Authors | Type of Study | Recruited Sample | Population | Main Outcomes |
|---|---|---|---|---|
| Davis A et al., 2007 [20] | Cross-sectional study | 471.969 adolescents | Adolescents | Current and lifetime asthma prevalence increased as BMI percentile increased starting with the 25th to 35th percentile group and with the 45th to 55th percentile group, respectively. |
| Tsai HJ et al., 2018 [18] | Prospective study | 1928 children (enrolled at birth and followed prospectively). | Mean age 7.8 ± 3.3 years | Excessive early life weight gain and overweight were both associated with an increased risk of asthma in childhood. |
| Contreras ZA et al., 2018 [19] | Analysis of 16 European cohorts | 21,130 children | Mean age 4.1 ± 0.6 years | Early onset wheezing and asthma were associated with higher incidence of childhood obesity. Obese children have a double risk of developing asthma with a risk proportional to BMI values, particularly in boys. |
| Lang JE et al., 2019 [22] | Retrospective cohort study | 507,496 children | Children and adolescents aged 2–17 years | Obesity increased asthma risk in all age groups but especially in the prepubertal school-aged group (7–11 years) without allergic rhinitis. |
| Barross LL et al., 2011 [23] | Cross-sectional study | 508 subjects | Adults | There was a positive association between BMI and uncontrolled asthma. Between severe asthmatics, the obese had higher rate of hospitalization and emergency room accesses. |
| De Jesus JPV et al., 2018 [24] | Cross-sectional study | 925 subjects | Adults | Compared to non-obese asthmatics, obese asthmatics have: • poorer asthma control • lower spirometric values • poorer quality of life • more frequent asthma exacerbation requiring oral corticosteroids |
| “Classic” Asthma Phenotype | “Obese Asthma” Phenotype | |
|---|---|---|
| Prick tests for inhaled allergens | Positive | Negative |
| Biomarkers: | ||
| - FeNO | High | Low |
| - Blood eosinophils | High | Low |
| - IgE levels | High | Low |
| Inflammation pattern | Th2 polarization | No Th2 polarization (Th1 or Th17 polarization) |
| Cells involved | Th2 lymphocytes, type 2 innate lymphoid cells, eosinophils, mast cells | Neutrophils, type 3 innate lymphoid cells, macrophages |
| Inflammatory cytokines | IL-4, IL-5, IL-13 | IL-6, IL-17, IL-21, IL-22, IFN-gamma |
| Airway inflammation | Mainly eosinofilic | Mainly neutrofilic |
| Disease control/Response to steroid therapy | Generally good | Generally poor |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fainardi, V.; Passadore, L.; Labate, M.; Pisi, G.; Esposito, S. An Overview of the Obese-Asthma Phenotype in Children. Int. J. Environ. Res. Public Health 2022, 19, 636. https://doi.org/10.3390/ijerph19020636
Fainardi V, Passadore L, Labate M, Pisi G, Esposito S. An Overview of the Obese-Asthma Phenotype in Children. International Journal of Environmental Research and Public Health. 2022; 19(2):636. https://doi.org/10.3390/ijerph19020636
Chicago/Turabian StyleFainardi, Valentina, Lucrezia Passadore, Marialuisa Labate, Giovanna Pisi, and Susanna Esposito. 2022. "An Overview of the Obese-Asthma Phenotype in Children" International Journal of Environmental Research and Public Health 19, no. 2: 636. https://doi.org/10.3390/ijerph19020636
APA StyleFainardi, V., Passadore, L., Labate, M., Pisi, G., & Esposito, S. (2022). An Overview of the Obese-Asthma Phenotype in Children. International Journal of Environmental Research and Public Health, 19(2), 636. https://doi.org/10.3390/ijerph19020636