
Causes of Stress among Healthcare Professionals and Successful Hospital Management Approaches to Mitigate It during the COVID-19 Pandemic: A Cross-Sectional Study

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Procedures and Instruments
2.4. Statistical Analysis
3. Results
3.1. Reliability and Validity
3.1.1. Exploratory Factor Analysis
3.1.2. Exploratory Factor Analysis (EFA) of the Stress Scale
3.1.3. Exploratory Factor Analysis of the Satisfaction Scale
3.2. Construct-Related Validity
3.3. Comparison of Means and Nominal Variables of the Scale
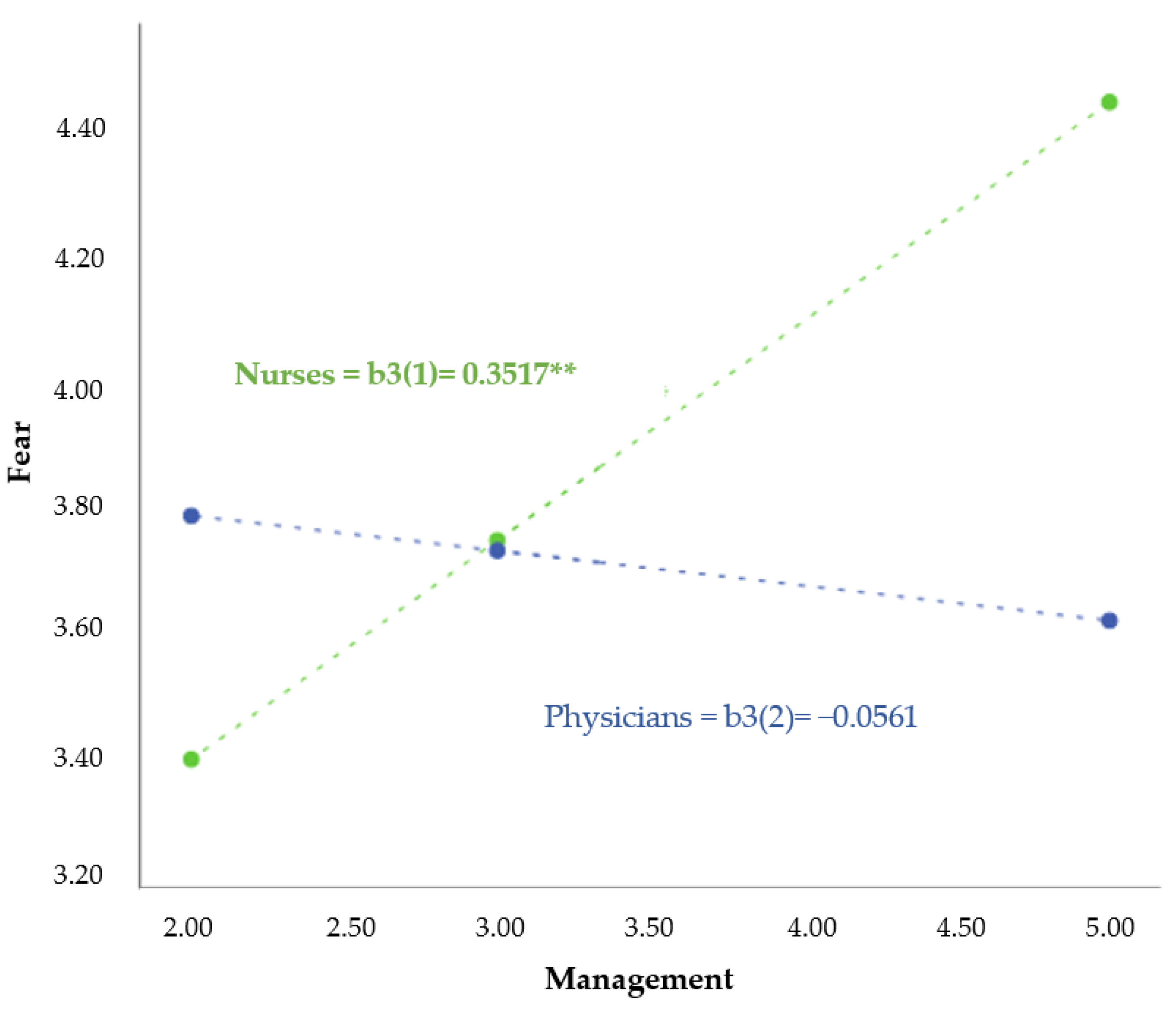
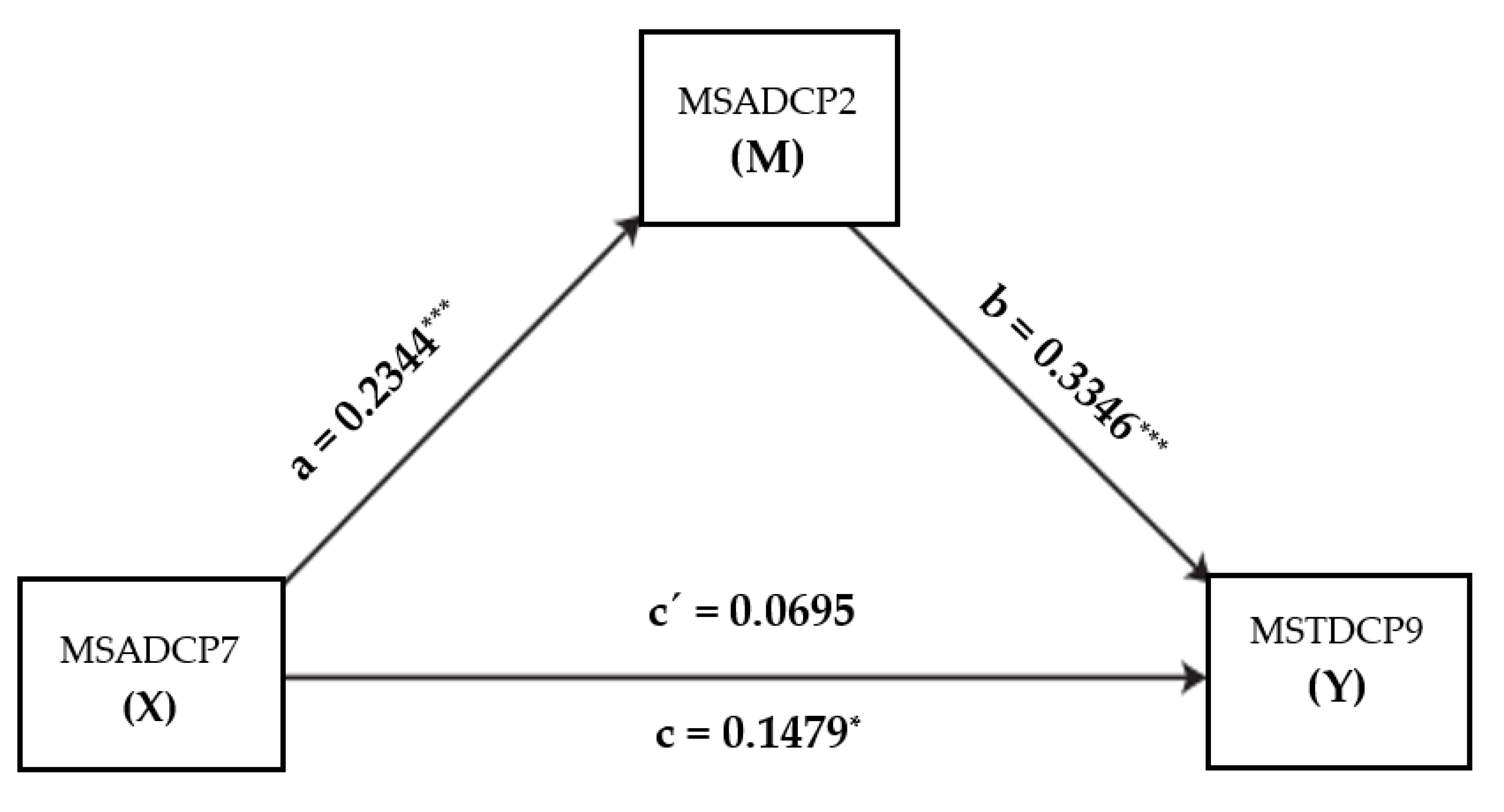
3.4. Moderation and Mediation between Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19. 11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 28 November 2021).
- Chen, J. Pathogenicity and transmissibility of 2019-nCoV—A quick overview and comparison with other emerging viruses. Microbes Infect. 2020, 22, 69–71. [Google Scholar] [CrossRef]
- Ramírez, F.B.; Misol, R.C.; Fernández Alonso, M.D.C.; Tizón García, J.L.; Grupo de Salud Mental del PAPPS. Mental health in epidemics: A perspective from the Spanish Primary Health Care. Atención Primaria 2020, 52, 93–113. [Google Scholar] [CrossRef]
- Ruiz-Fernández, M.D.; Ramos-Pichardo, J.D.; Ibáñez-Masero, O.; Cabrera-Troya, J.; Carmona-Rega, M.I.; Ortega-Galán, M. Compassion fatigue, burnout, compassion satisfaction and perceived stress in healthcare professionals during the COVID-19 health crisis in Spain. J. Clin. Nurs. 2020, 29, 4321–4330. [Google Scholar] [CrossRef]
- Xiang, Y.-T.; Yang, Y.; Li, W.; Zhang, L.; Zhang, Q.; Cheung, T.; Ng, C.H. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry 2020, 7, 228–229. [Google Scholar] [CrossRef]
- Galbraith, N.; Boyda, D.; McFeeters, D.; Hassan, T. The mental health of doctors during the COVID-19 pandemic. BJPsych Bull. 2020, 45, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Hummel, S.; Oetjen, N.; Du, J.; Posenato, E.; de Almeida, R.M.R.; Losada, R.; Ribeiro, O.; Frisardi, V.; Hopper, L.; Rashid, A.; et al. Mental Health Among Medical Professionals During the COVID-19 Pandemic in Eight European Countries: Cross-sectional Survey Study. J. Med. Internet Res. 2021, 23, e24983. [Google Scholar] [CrossRef]
- Bohlken, J.; Schömig, F.; Lemke, M.R.; Pumberger, M.; Riedel-Heller, S.G. COVID-19-Pandemie: Belastungen des medizinischen Personals. Psychiatr. Prax. 2020, 47, 190–197. [Google Scholar] [CrossRef]
- Höhmann, U.; Lautenschläger, M.; Schwarz, L. Belastungen im Pflegeberuf: Bedingungsfaktoren, Folgen und Desiderate. In Pflege-Report 2016; Schattauer: Stuttgart, Germany, 2016; pp. 73–89. [Google Scholar]
- World Health Organization. Health Workforce Policy and Management in the Context of the COVID-19 Pandemic Response: Interim Guidance, 3 December 2020. Available online: https://apps.who.int/iris/handle/10665/337333 (accessed on 12 August 2022).
- Ruotsalainen, J.H.; Verbeek, J.H.; Mariné, A.; Serra, C. Preventing occupational stress in healthcare workers. In Cochrane Database of Systematic Reviews; Ruotsalainen, J.H., Ed.; John Wiley & Sons Ltd.: Chichester, UK, 2014. [Google Scholar] [CrossRef]
- International Labour Organization. Stress Prevention at Work Checkpoints: Practical Improvements for Stress Prevention in the Workplace; International Labour Organization: Geneva, Switzerland, 2012; Available online: https://labordoc.ilo.org/permalink/41ILO_INST/oti1e7/alma994674733402676 (accessed on 12 August 2022).
- Brugger, M.; Hengalova, R.; Stefan, J. COVID-19 and the Perceived Stressors of Austrian Long-Term Care Workers, January 2021. Available online: https://www.gpa.at/content/dam/gpa/downloads/kollektivvertrag/gesundheit,-soziales,-kirchen/sw%C3%B6/2021/Covid-19%20and%20the%20perceived%20Stressors%20of%20Austrian%20Long-Term%20Care%20Workers.pdf (accessed on 12 August 2022).
- Martinez Estalella, G.; Zabalegui, A.; Sevilla Guerra, S.; En Nombre del Comité Técnico de la Dirección Enfermera (CTDE). Management and leadership of nursing services in the emergency plan for the pandemic COVID-19: The experience of the Clinic Hospital of Barcelona. Enferm. Clin. Engl. Ed. 2021, 31, S12–S17. [Google Scholar] [CrossRef]
- Barello, S.; Caruso, R.; Palamenghi, L.; Nania, T.; Dellafiore, F.; Bonetti, L.; Silenzi, A.; Marotta, C.; Graffigna, G. Factors associated with emotional exhaustion in healthcare professionals involved in the COVID-19 pandemic: An application of the job demands-resources model. Int. Arch. Occup. Environ. Health 2021, 94, 1751–1761. [Google Scholar] [CrossRef] [PubMed]
- Lorente, L.; Vera, M.; Peiró, T. Nurses’ stressors and psychological distress during the COVID-19 pandemic: The mediating role of coping and resilience. J. Adv. Nurs. 2020, 77, 1335–1344. [Google Scholar] [CrossRef]
- Zhou, T.; Guan, R.; Sun, L. Perceived organizational support and PTSD symptoms of frontline healthcare workers in the outbreak of COVID-19 in Wuhan: The mediating effects of self-efficacy and coping strategies. Appl. Psychol. Health Well-Being 2021, 13, 745–760. [Google Scholar] [CrossRef]
- Babore, A.; Lombardi, L.; Viceconti, M.L.; Pignataro, S.; Marino, V.; Crudele, M.; Candelori, C.; Bramanti, S.M.; Trumello, C. Psychological effects of the COVID-2019 pandemic: Perceived stress and coping strategies among healthcare professionals. Psychiatry Res. 2020, 293, 113366. [Google Scholar] [CrossRef] [PubMed]
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Estryn-Behar, M.; van der Heijden, B.; Camerino, D.; Fry, C.; Le Nezet, O.; Conway, P.M.; Hasselhorn, H.-M.; the NEXT Study group. Violence risks in nursing—results from the European ‘NEXT’ Study. Occup. Med. 2008, 58, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Liu, Y.; Hu, K.; Zhang, M.; Du, M.; Huang, H.; Yue, X. Healthcare workers’ stress when caring for COVID-19 patients: An altruistic perspective. Nurs. Ethic 2020, 27, 1490–1500. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Zhang, P.; Liu, Y.; Wang, H.; Hu, K.; Du, M. Influence of perceived stress and workload on work engagement in front-line nurses during COVID-19 pandemic. J. Clin. Nurs. 2021, 30, 1584–1595. [Google Scholar] [CrossRef]
- Leo, C.G.; Sabina, S.; Tumolo, M.R.; Bodini, A.; Ponzini, G.; Sabato, E.; Mincarone, P. Burnout Among Healthcare Workers in the COVID 19 Era: A Review of the Existing Literature. Front. Public Health 2021, 9, 750529. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Publications: New York, NY, USA, 2017. [Google Scholar]
- del Líbano, M.; Ubillos, S.; Puente, A.; Gutierrez, A. Manual Práctico de Análisis Estadístico en Ciencias de la Salud: Pruebas Paramétricas y no Paramétricas; University of Burgos. Servicio de Publicaciones e Imagen Institucional: Burgos, Spain, 2019. [Google Scholar]
- Baptista dos Santos de Freitas, M.J.; Dinis Parreira, P.M.; Maroco Domingues, J.P. Avaliação das propriedades psicométricas da Escala Satisfação dos Clientes com os Cuidados de Enfermagem no Hospital. Rev. Enferm. Ref. 2016, IV, 9–17. Available online: https://www.redalyc.org/articulo.oa?id=388247711001 (accessed on 9 October 2022).
- Hernández-Lalinde, J.; Espinosa-Castro, J.-F.; Tarazona, M.E.P.; Diaz, E.; Bautista-Sandoval, M.J.; Garzón, M.E.R.; Bermudez, E. Sobre el uso adecuado del coeficiente de correlación de Pearson: Verificación de supuestos mediante un ejemplo aplicado a las ciencias de la salud. Arch. Venez. De Farmacol. Y Ter. 2018, 37, 434–443. [Google Scholar]
- Daniel, W.W.; Cross, C.L. Biostatistics: A Foundation for Analysis in the Health Sciences, 11th ed.; Wiley: New York, NY, USA, 2018. [Google Scholar]
- Alan, H.; Bacaksiz, F.E.; Sen, H.T.; Eskici, G.T.; Gumus, E.; Seren, A.K.H. “I’m a hero, but…”: An evaluation of depression, anxiety, and stress levels of frontline healthcare professionals during COVID-19 pandemic in Turkey. Perspect. Psychiatr. Care 2020, 57, 1126–1136. [Google Scholar] [CrossRef] [PubMed]
- Barello, S.; Palamenghi, L.; Graffigna, G. Burnout and somatic symptoms among frontline healthcare professionals at the peak of the Italian COVID-19 pandemic. Psychiatry Res. 2020, 290, 113129. [Google Scholar] [CrossRef]
- Bates, A.; Ottaway, J.; Moyses, H.; Perrrow, M.; Rushbrook, S.; Cusack, R. Psychological impact of caring for critically ill patients during the COVID-19 pandemic and recommendations for staff support. J. Intensiv. Care Soc. 2020, 22, 312–318. [Google Scholar] [CrossRef]
- Bettinsoli, M.L.; Di Riso, D.; Napier, J.L.; Moretti, L.; Bettinsoli, P.; Delmedico, M.; Piazzolla, A.; Moretti, B. Mental Health Conditions of Italian Healthcare Professionals during the COVID-19 Disease Outbreak. Appl. Psychol. Health Well-Being 2020, 12, 1054–1073. [Google Scholar] [CrossRef] [PubMed]
- Sirois, F.M.; Owens, J. Factors Associated With Psychological Distress in Health-Care Workers During an Infectious Disease Outbreak: A Rapid Systematic Review of the Evidence. Front. Psychiatry 2021, 11, 589545. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.-Y.; Yang, Y.-Z.; Zhang, X.-M.; Xu, X.; Dou, Q.-L.; Zhang, W.-W.; Cheng, A.S.K. The prevalence and influencing factors in anxiety in medical workers fighting COVID-19 in China: A cross-sectional survey. Epidemiol. Infect. 2020, 148, e98. [Google Scholar] [CrossRef] [PubMed]
- Aksoy, Y.E.; Koçak, V. Psychological effects of nurses and midwives due to COVID-19 outbreak: The case of Turkey. Arch. Psychiatr. Nurs. 2020, 34, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Greenglass, E.R.; Marjanovic, Z.; Fiksenbaum, L.; Coffey, S.; Shi, K.; Chen, X.F. Professional efficacy and social support in nurses during the SARS crisis in Canada and China. In New Directions in Organizational Psychology and Behavioural; Antoniou, A.S.G., Cooper, C., Eds.; Routledge: Surrey, UK, 2016; pp. 169–188. [Google Scholar]
- Demirjian, N.; Fields, B.K.; Song, C.; Reddy, S.; Desai, B.; Cen, S.Y.; Salehi, S.; Gholamrezanezhad, A. Impacts of the Coronavirus Disease 2019 (COVID-19) pandemic on healthcare workers: A nationwide survey of United States radiologists. Clin. Imaging 2020, 68, 218–225. [Google Scholar] [CrossRef]
- Elbay, R.Y.; Kurtulmuş, A.; Arpacıoğlu, S.; Karadere, E. Depression, anxiety, stress levels of physicians and associated factors in COVID-19 pandemics. Psychiatry Res. 2020, 290, 113130. [Google Scholar] [CrossRef] [PubMed]
- García-Fernández, L.; Romero-Ferreiro, V.; López-Roldán, P.D.; Padilla, S.; Calero-Sierra, I.; Monzó-García, M.; Pérez-Martín, J.; Rodriguez-Jimenez, R. Mental health impact of COVID-19 pandemic on Spanish healthcare workers. Psychol. Med. 2020, 52, 195–197. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Prasad, A.S.; Dixit, P.K.; Padmakumari, P.; Gupta, S.; Abhisheka, K. Survey of prevalence of anxiety and depressive symptoms among 1124 healthcare workers during the coronavirus disease 2019 pandemic across India. Med. J. Armed Forces India 2020, 77, S404–S412. [Google Scholar] [CrossRef] [PubMed]
- Martínez-López, J.Á.; Lázaro-Pérez, C.; Gómez-Galán, J.; Fernández-Martínez, M.D.M. Psychological Impact of COVID-19 Emergency on Health Professionals: Burnout Incidence at the Most Critical Period in Spain. J. Clin. Med. 2020, 9, 3029. [Google Scholar] [CrossRef] [PubMed]
- Nie, A.; Su, X.; Zhang, S.; Guan, W.; Li, J. Psychological impact of COVID-19 outbreak on frontline nurses: A cross-sectional survey study. J. Clin. Nurs. 2020, 29, 4217–4226. [Google Scholar] [CrossRef] [PubMed]
- Vagni, M.; Maiorano, T.; Giostra, V.; Pajardi, D. Coping With COVID-19: Emergency Stress, Secondary Trauma and Self-Efficacy in Healthcare and Emergency Workers in Italy. Front. Psychol. 2020, 11, 566912. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-S.; Choi, J.S. Factors Influencing Emergency Nurses’ Burnout During an Outbreak of Middle East Respiratory Syndrome Coronavirus in Korea. Asian Nurs. Res. 2016, 10, 295–299. [Google Scholar] [CrossRef]
- Tam, C.W.C.; Pang, E.P.F.; Lam, L.C.W.; Chiu, H.F.K. Severe acute respiratory syndrome (SARS) in Hong Kong in 2003: Stress and psychological impact among frontline healthcare workers. Psychol. Med. 2004, 34, 1197–1204. [Google Scholar] [CrossRef] [PubMed]
- Lasalvia, A.; Bonetto, C.; Porru, S.; Carta, A.; Tardivo, S.; Bovo, C.; Ruggeri, M.; Amaddeo, F. Psychological impact of COVID-19 pandemic on healthcare workers in a highly burdened area of north-east Italy. Epidemiol. Psychiatr. Sci. 2020, 30, e1. [Google Scholar] [CrossRef]
- Guttormson, J.L.; Calkins, K.; McAndrew, N.; Fitzgerald, J.; Losurdo, M.H.; Loonsfoot, B.D. Critical Care Nurses’ Experiences During the COVID-19 Pandemic: A US National Survey. Am. J. Crit. Care 2022, 31, 96–103. [Google Scholar] [CrossRef]
- da Silva, F.C.T.; Barbosa, C.P. The impact of the COVID-19 pandemic in an intensive care unit (ICU): Psychiatric symptoms in healthcare professionals. Prog. Neuropsychopharmacol Biol. Psychiatry 2021, 110, 110299. [Google Scholar] [CrossRef]
- Esteban-Sepúlveda, S.; Terradas-Robledo, R.; Castro-Ribeiro, T.; García-Pagès, E.; Sobregrau-Sangrà, P.; Lacueva-Pérez, L. Pandemia COVID-19 sobre profesionales sanitarios en un hospital de tercer nivel en España: Cambios laborales durante la primera ola, salud mental a los 4 meses y seguimiento a los 9 meses. Enferm. Clin. 2022, 32, 143–151. [Google Scholar] [CrossRef]
- Nyashanu, M.; Pfende, F.; Ekpenyong, M.S. Triggers of mental health problems among frontline healthcare workers during the COVID-19 pandemic in private care homes and domiciliary care agencies: Lived experiences of care workers in the Midlands region, UK. Health Soc. Care Community 2020, 30, e370–e376. [Google Scholar] [CrossRef]
- Sakib, N.; Akter, T.; Zohra, F.; Bhuiyan, A.K.M.I.; Mamun, M.A.; Griffiths, M.D. Fear of COVID-19 and Depression: A Comparative Study Among the General Population and Healthcare Professionals During COVID-19 Pandemic Crisis in Bangladesh. Int. J. Ment. Health Addict. 2021, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Elhadi, M.; Msherghi, A.; Elgzairi, M.; Alhashimi, A.; Bouhuwaish, A.; Biala, M.; Abuelmeda, S.; Khel, S.; Khaled, A.; Alsoufi, A.; et al. Psychological status of healthcare workers during the civil war and COVID-19 pandemic: A cross-sectional study. J. Psychosom. Res. 2020, 137, 110221. [Google Scholar] [CrossRef]
- Park, J.-S.; Lee, E.-H.; Park, N.-R.; Choi, Y.H. Mental Health of Nurses Working at a Government-designated Hospital During a MERS-CoV Outbreak: A Cross-sectional Study. Arch. Psychiatr. Nurs. 2017, 32, 2–6. [Google Scholar] [CrossRef]
- Park, C.; Hwang, J.-M.; Jo, S.; Bae, S.J.; Sakong, J. COVID-19 Outbreak and Its Association with Healthcare Workers’ Emotional Stress: A Cross-Sectional Study. J. Korean Med. Sci. 2020, 35, e372. [Google Scholar] [CrossRef]
- Thornicroft, G.; Mehta, N.; Clement, S.; Evans-Lacko, S.; Doherty, M.; Rose, D.; Koschorke, M.; Shidhaye, R.; O’Reilly, C.; Henderson, C. Evidence for effective interventions to reduce mental-health-related stigma and discrimination. Lancet 2015, 387, 1123–1132. [Google Scholar] [CrossRef]
- Chuang, P.-Y.; Lou, M.-F. Psychometric evaluation of the stress scale of caring for highly infectious disease patients among health care workers - Based on SARS. Taiwan J. Public Health 2005, 24, 420–430. [Google Scholar]
- Tang, C.J.; Lin, Y.P.; Chan, E. ‘From Expert to Novice’, Perceptions of General Ward Nurses on Deployment to Outbreak Intensive Care Units during the COVID-19 Pandemic: A Qualitative Descriptive Study. J. Clin. Nurs. 2021. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number | Items |
|---|---|
| 1 | Fear of infection |
| 2 | Fear of transmitting the infection to others |
| 3 | Use of personal protective equipment during working hours |
| 4 | Rules for visiting critically ill, terminally ill, or deceased patients due to COVID-19 |
| 5 | The dynamics of the pandemic due to frequent changes in protocols |
| 6 | Lack of protective equipment |
| 7 | Working in an unfamiliar area with unfamiliar and inexperienced colleagues |
| 8 | Fear of social exclusion as potential carriers of SARS-CoV-2 due to the profession |
| 9 | The changed and increased workload |
| 10 | The extra time burden |
| 11 | The extra private burden stemming from social isolation measures, school closures, etc. |
| Number | Items |
|---|---|
| 1 | Satisfaction with the management of the pandemic |
| 2 | Incentive payment (“Corona bonus”) 1 |
| 3 | Appreciation experienced from institutions |
| 4 | Appreciation experienced from the public |
| 5 | The care provided by the occupational medicine department |
| 6 | The availability of a psychological counselling helpline |
| 7 | Support and attention from superiors in the health centre |
| 8 | Teamwork |
| 9 | Information management |
| 10 | Attention from the Hygiene Department of the centre |
| “The correct protection was only partial, as for a few days they recommended wearing FFP2 for longer than appropriate, increasing the risk of infection and illness”. “They didn’t ask if you wanted to work in the Covid area, they didn’t give us any other option”. “In addition to the fear of contagion, the time without contact with family members” “Children with asthma at home, and my mother” “A lot of discomfort from the personal protective equipment (PPE).” “They made me sweat a lot” “The lack of oxygen was overwhelming” “I did not feel it was right that at the beginning it was not possible to visit the deceased” “It often was our decision” “Working with unfamiliar colleagues was stressful” “At first it was very scary to work in that ward” “There was no lack of PPE at any time” “There was no lack of material, but we used it for too long” “The potential risk of infection and thus not having contact with family and friends for months was very hard” “My partner was afraid” “I had to increase my working hours from 50 to 75%” “The private extra burden was higher, due to having to take care of the children” “Lockdown + working with Covid + closed schools = more pressure and stress” |
| “In the beginning, things were not managed well at all, then better” “What management?” “I don’t think it’s right that all healthcare workers should have the same Corona bonus” “Those working directly with Covid should have received more” “Clapping doesn’t add a single euro to the bank account” “I don’t believe in the duration of this recognition by society” “We should have had regularly scheduled PCR checks” “I didn’t know there was a psychological helpline” “Nursing and administration management was not seen at any time” “Support was not sustained” “Support from the supervisor was enormous” “I didn’t feel the support of the public, but I did feel more recognition from fellow doctors” |
| Item | M 1 | Var 2 | ITC 3 | A4 |
|---|---|---|---|---|
| 1/MSTDCP 1 | 46.31 | 182.33 | 0.49 | 0.81 |
| 2/MSTDCP 2 | 44.45 | 183.84 | 0.44 | 0.82 |
| 3/MSTDCP 3 | 45.65 | 185.15 | 0.40 | 0.82 |
| 4/MSTDCP 4 | 45.35 | 183.41 | 0.42 | 0.82 |
| 5/MSTDCP 5 | 45.28 | 179.50 | 0.60 | 0.81 |
| 6/MSTDCP 6 | 45.04 | 184.53 | 0.37 | 0.83 |
| 7/MSTDCP 7 | 47.15 | 180.05 | 0.47 | 0.82 |
| 8/MSTDCP 8 | 46.18 | 176.38 | 0.51 | 0.81 |
| 9/MSTDCP 9 | 45.88 | 173.79 | 0.64 | 0.80 |
| 10/MSTDCP 10 | 45.68 | 172.53 | 0.64 | 0.80 |
| 11/MSTDCP 11 | 45.31 | 176.50 | 0.56 | 0.81 |
| Item | M 1 | Var 2 | ITC 3 | A 4 |
|---|---|---|---|---|
| 1/MSADCP1 | 46.31 | 182.33 | 0.49 | 0.81 |
| 2/MSADCP 2 | 44.45 | 183.84 | 0.44 | 0.82 |
| 3/MSADCP 3 | 45.65 | 185.15 | 0.40 | 0.82 |
| 4/MSADCP 4 | 45.35 | 183.41 | 0.42 | 0.82 |
| 5/MSADCP 5 | 45.28 | 179.50 | 0.60 | 0.81 |
| 6/MSADCP 6 | 45.04 | 184.53 | 0.37 | 0.83 |
| 7/MSADCP 7 | 47.15 | 180.05 | 0.47 | 0.82 |
| 8/MSADCP 8 | 46.18 | 176.38 | 0.51 | 0.81 |
| 9/MSADCP 9 | 45.88 | 173.79 | 0.64 | 0.80 |
| 10/MSADCP 10 | 45.68 | 172.53 | 0.64 | 0.80 |
| Component a | |||
|---|---|---|---|
| Item | 1 | 2 | 3 |
| MSTDCP9 | 0.804 | ||
| MSTDCP10 | 0.0771 | ||
| MSTDCP3 | 0.716 | ||
| MSTDCP11 | 0.586 | 0.480 | |
| MSTDCP6 | 0.797 | ||
| MSTDCP5 | 0.353 | 0.659 | |
| MSTDCP4 | 0.627 | ||
| MSTDCP7 | 0.613 | ||
| MSTDCP8 | 0.368 | 0.464 | |
| MSTDCP2 | 0.841 | ||
| MSTDCP1 | 0.826 | ||
| Factor | MSTDCP Items | α | Definitive Dimension |
|---|---|---|---|
| F1 | 3, 9, 10 | 0.75 | Mental stress arising from workload |
| F2 | 4, 5, 6, 7, 8 | 0.72 | Mental stress due to constant changes in work, protocols, and availability of material/infrastructure |
| F3 | 1, 2, 11 | 0.71 | Fear of infection, transmission, and additional private burden due to social isolation measures |
| Number | Dimension | Item |
|---|---|---|
| 1 | D3 | Fear of infection with COVID-19 |
| 2 | D3 | Fear of transmitting the infection to others |
| 3 | D1 | Wearing PPE |
| 4 | D2 | Visiting guidelines for critically ill or dying COVID-19 patients |
| 5 | D2 | Pandemic dynamics due to changing standards/guidelines |
| 6 | D2 | Temporary lack of PPE |
| 7 | D2 | Working in an unfamiliar speciality with non-expert colleagues |
| 8 | D2 | Being excluded by others as a potential carrier of infection due to working in a COVID-19 area |
| 9 | D1 | The workload in terms of content |
| 10 | D1 | The workload in terms of time |
| 11 | D3 | The extra private burden |
| Component a | ||
|---|---|---|
| Item | 1 | 2 |
| MSADCP10 | 0.818 | |
| MSADCP9 | 0.799 | |
| MSADCP1 | 0.774 | |
| MSADCP7 | 0.712 | |
| MSADCP6 | 0.689 | |
| MSADCP8 | 0.648 | 0.321 |
| MSADCP5 | 0.570 | |
| MSADCP4 | 0.859 | |
| MSADCP3 | 0.332 | 0.800 |
| MSADCP2 | 0.372 | 0.572 |
| Factor | Items | α | Definitive Dimension |
|---|---|---|---|
| F1 | 1,5,6,7,9,10 | 0.85 | Mental satisfaction associated with management and the measures taken for physical security and psychological protection |
| F2 | 2,3,4,8 | 0.70 | Mental satisfaction related to perceived support and extra financial compensation |
| Number | Dimension | Item |
|---|---|---|
| 1 | D1 | Coronavirus crisis management |
| 2 | D2 | Corona bonus/incentive payment |
| 3 | D2 | The experienced appreciation |
| 4 | D2 | Public support |
| 5 | D1 | Care provided by the occupational medicine department |
| 6 | D1 | Availability of a psychological support hotline |
| 7 | D1 | With the psychological/mental support of my superiors |
| 8 | D2 | Team cohesion |
| 9 | D1 | With information management |
| 10 | D1 | With the supervision of the specialised hygiene centre |
| Stress Scale | F1-MSTDCP | F2-MSTDCP | F3-MSTDCP | Satisfaction Scale | F1-MSADCP | F2-MSADCP | |
|---|---|---|---|---|---|---|---|
| Stress Scale | 1 | ||||||
| F1-MSTDCP | 0.76 ** | 1 | |||||
| F2-MSTDCP | 0.85 ** | 0.52 ** | 1 | ||||
| F3-MSTDCP | 0.76 ** | 0.48 ** | 0.46 ** | 1 | |||
| Satisfaction Scale | 0.37 ** | 0.31 ** | 0.35 ** | 0.24 ** | 1 | ||
| F1-MSADCP | 0.34 ** | 0.26 ** | 0.34 ** | 0.23 * | 0.95 ** | 1 | |
| F2-MSADCP | 0.35 ** | 0.35 ** | 0.24 ** | 0.25 ** | 0.85 ** | 0.63** | 1 |
| Department | n | Mean | SD |
|---|---|---|---|
| Emergency Department (ED) | 34 | 52.47 | 14.88 |
| Intensive Care Unit (ICU) | 48 | 50.77 | 12.39 |
| COVID Ward/Station | 77 | 50.92 | 15.31 |
| Outpatient Tent | 17 | 41.11 | 14.74 |
| Department | n | Mean | SD |
|---|---|---|---|
| Emergency Department (ED) | 23 | 35.82 | 17.30 |
| Intensive Care Unit (ICU) | 38 | 28.53 | 10.52 |
| COVID Ward/Station | 51 | 27.70 | 11.69 |
| Outpatient Tent | 1 | 26.50 | 11.78 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Herraiz-Recuenco, L.; Alonso-Martínez, L.; Hannich-Schneider, S.; Puente-Alcaraz, J. Causes of Stress among Healthcare Professionals and Successful Hospital Management Approaches to Mitigate It during the COVID-19 Pandemic: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 12963. https://doi.org/10.3390/ijerph191912963
Herraiz-Recuenco L, Alonso-Martínez L, Hannich-Schneider S, Puente-Alcaraz J. Causes of Stress among Healthcare Professionals and Successful Hospital Management Approaches to Mitigate It during the COVID-19 Pandemic: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(19):12963. https://doi.org/10.3390/ijerph191912963
Chicago/Turabian StyleHerraiz-Recuenco, Lourdes, Laura Alonso-Martínez, Susanne Hannich-Schneider, and Jesús Puente-Alcaraz. 2022. "Causes of Stress among Healthcare Professionals and Successful Hospital Management Approaches to Mitigate It during the COVID-19 Pandemic: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 19: 12963. https://doi.org/10.3390/ijerph191912963
APA StyleHerraiz-Recuenco, L., Alonso-Martínez, L., Hannich-Schneider, S., & Puente-Alcaraz, J. (2022). Causes of Stress among Healthcare Professionals and Successful Hospital Management Approaches to Mitigate It during the COVID-19 Pandemic: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 19(19), 12963. https://doi.org/10.3390/ijerph191912963
{kind=link}
{kind=link}