
Quadriceps Electromyographic Activity in Closed and Open Kinetic-Chain Exercises with Hip-Adductor Co-Contraction in Sedentary Women

Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Experimental Procedure
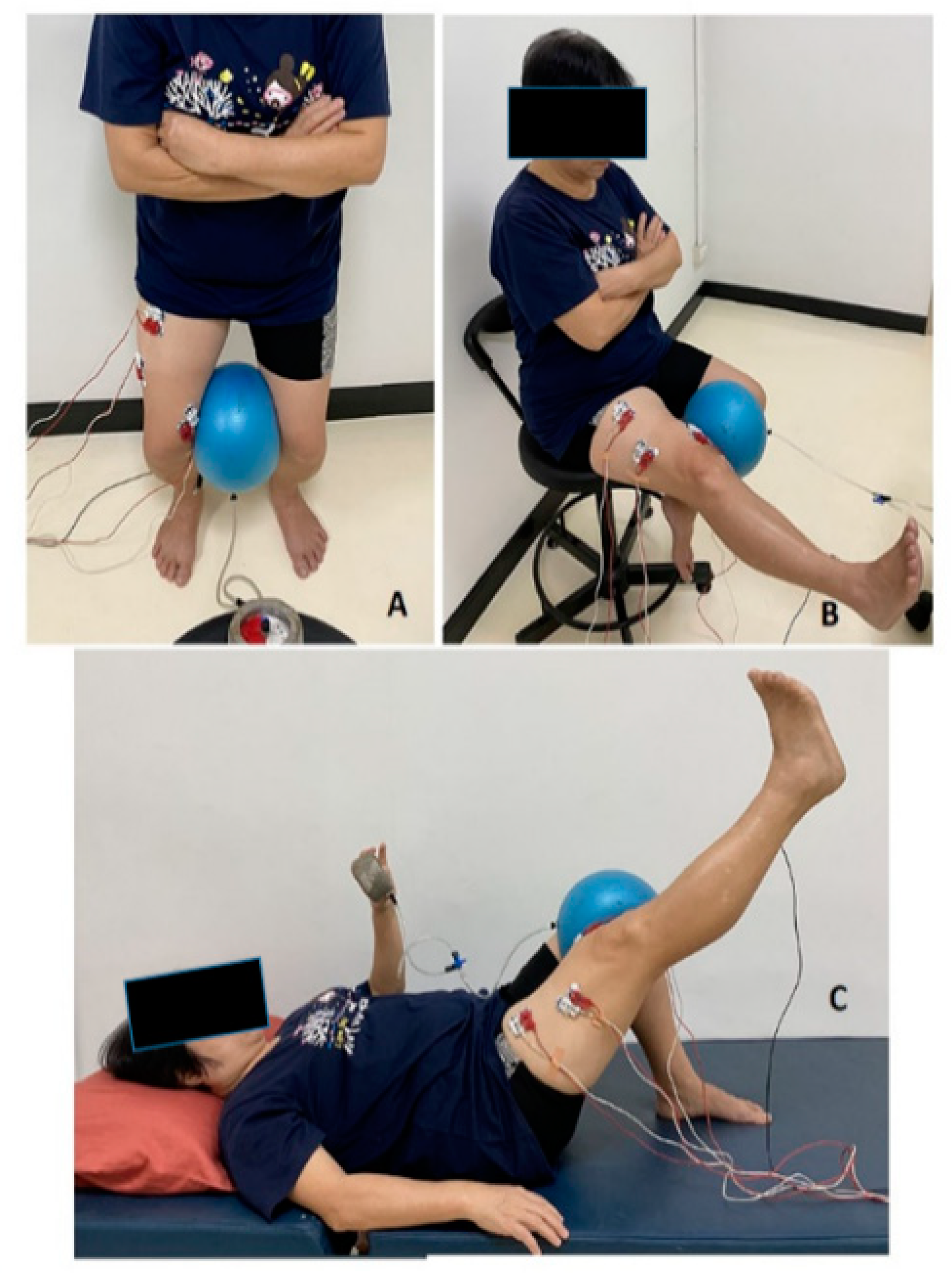
2.3. Leg-Strengthening Exercises Involving Hip Adductor Co-Contraction
2.4. Electromyographic Analysis
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Kostka, T.; Rahmani, A.; Berthouze, S.E.; Lacour, J.-R.; Bonnefoy, M. Quadriceps muscle function in relation to habitual physical activity and VO2max in men and women aged more than 65 years. J. Gerontol. Ser. A 2000, 55, B481–B488. [Google Scholar] [CrossRef] [PubMed]
- Madigan, M.L.; Lloyd, E.M. Age-related differences in peak joint torques during the support phase of single-step recovery from a forward fall. J. Gerontol. Ser. A 2005, 60, 910–914. [Google Scholar] [CrossRef] [PubMed]
- Borges, O. Isometric and isokinetic knee extension and flexion torque in men and women aged 20–70. Scand. J. Rehabil. Med. 1989, 21, 45–53. [Google Scholar] [PubMed]
- Kallman, D.A.; Plato, C.C.; Tobin, J.D. The role of muscle loss in the age-related decline of grip strength: Cross-sectional and longitudinal perspectives. J. Gerontol. 1990, 45, M82–M88. [Google Scholar] [CrossRef]
- Lynch, N.A.; Metter, E.J.; Lindle, R.S.; Fozard, J.L.; Tobin, J.D.; Roy, T.A.; Fleg, J.L.; Hurley, B.F. Muscle quality. I. Age-associated differences between arm and leg muscle groups. J. Appl. Physiol. 1999, 86, 188–194. [Google Scholar] [CrossRef]
- Lindle, R.S.; Metter, E.J.; Lynch, N.A.; Fleg, J.L.; Fozard, J.L.; Tobin, J.; Roy, T.A.; Hurley, B.F. Age and gender comparisons of muscle strength in 654 women and men aged 20–93 yr. J. Appl. Physiol. 1997, 83, 1581–1587. [Google Scholar] [CrossRef]
- Doherty, T.J. The influence of aging and sex on skeletal muscle mass and strength. Curr. Opin. Clin. Nutr. Metab. Care 2001, 4, 503–508. [Google Scholar] [CrossRef]
- Hinman, R.S.; Cowan, S.M.; Crossley, K.M.; Bennell, K.L. Age-related changes in electromyographic quadriceps activity during stair descent. J. Orthop. Res. 2005, 23, 322–326. [Google Scholar] [CrossRef]
- Øiestad, B.; Juhl, C.; Eitzen, I.; Thorlund, J. Knee extensor muscle weakness is a risk factor for development of knee osteoarthritis. A systematic review and meta-analysis. Osteoarthr. Cartil. 2015, 23, 171–177. [Google Scholar] [CrossRef]
- Malek, M.M.; Mangine, R.E. Patellofemoral pain syndromes: A comprehensive and conservative approach. J. Orthop. Sport. Phys. Ther. 1981, 2, 108–116. [Google Scholar] [CrossRef]
- Sheehy, P.; Burdett, R.G.; Irrgang, J.J.; VanSwearingen, J. An electromyographic study of vastus medialis oblique and vastus lateralis activity while ascending and descending steps. J. Orthop. Sport. Phys. Ther. 1998, 27, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Earl, J.; Schmitz, R.; Arnold, B. Activation of the VMO and VL during dynamic mini-squat exercises with and without isometric hip adduction. J. Electromyogr. Kinesiol. 2001, 11, 381–386. [Google Scholar] [CrossRef]
- Wong, Y.-M.; Straub, R.K.; Powers, C.M. The VMO:VL activation ratio while squatting with hip adduction is influenced by the choice of recording electrode. J. Electromyogr. Kinesiol. 2013, 23, 443–447. [Google Scholar] [CrossRef] [PubMed]
- Miao, P.; Xu, Y.; Pan, C.; Liu, H.; Wang, C.-H. Vastus medialis oblique and vastus lateralis activity during a double-leg semisquat with or without hip adduction in patients with patellofemoral pain syndrome. BMC Musculoskelet. Disord. 2015, 16, 289. [Google Scholar] [CrossRef] [PubMed]
- Boling, M.; Padua, D.; Blackburn, J.T.; Petschauer, M.; Hirth, C. Hip adduction does not affect VMO EMG amplitude or VMO:VL ratios during a dynamic squat exercise. J. Sport Rehabil. 2006, 15, 195–205. [Google Scholar] [CrossRef][Green Version]
- Hertel, J.; E Earl, J.; Tsang, K.K.W.; Miller, S.J. Combining isometric knee extension exercises with hip adduction or abduction does not increase quadriceps EMG activity. Br. J. Sport. Med. 2004, 38, 210–213. [Google Scholar] [CrossRef]
- Strazza, A.; Mengarelli, A.; Fioretti, S.; Burattini, L.; Agostini, V.; Knaflitz, M.; Di Nardo, F. Surface-EMG analysis for the quantification of thigh muscle dynamic co-contractions during normal gait. Gait Posture 2017, 51, 228–233. [Google Scholar] [CrossRef]
- Jakobsen, T.L.; Jakobsen, M.D.; Andersen, L.L.; Husted, H.; Kehlet, H.; Bandholm, T. Quadriceps muscle activity during commonly used strength training exercises shortly after total knee arthroplasty: Implications for home-based exercise-selection. J. Exp. Orthop. 2019, 6, 29. [Google Scholar] [CrossRef]
- Emami, M.; Ghahramani, M.-H.; Abdinejad, F.; Namazi, H. Q-angle: An invaluable parameter for evaluation of anterior knee pain. Arch. Iran. Med. 2007, 10, 24–26. [Google Scholar] [PubMed]
- Finni, T.; Cheng, S. Variability in lateral positioning of surface EMG electrodes. J. Appl. Biomech. 2009, 25, 396–400. [Google Scholar] [CrossRef]
- Saiklang, P.; Puntumetakul, R.; Selfe, J.; Yeowell, G. An evaluation of an innovative exercise to relieve chronic low back pain in sedentary workers. Hum. Factors J. Hum. Factors Ergon. Soc. 2020, 64, 820–834. [Google Scholar] [CrossRef] [PubMed]
- Garner, J.C.; Blackburn, T.; Weimar, W.; Campbell, B. Comparison of electromyographic activity during eccentrically versus concentrically loaded isometric contractions. J. Electromyogr. Kinesiol. 2008, 18, 466–471. [Google Scholar] [CrossRef] [PubMed]
- Seliger, V.; Dolejš, L.; Karas, V. A dynamometric comparison of maximum eccentric, concentric, and isometric contractions using EMG and energy expenditure measurements. Eur. J. Appl. Physiol. Occup. Physiol. 1980, 45, 235–244. [Google Scholar] [CrossRef]
- Hanten, W.P.; Schulthies, S.S. Exercise effect on electromyographic activity of the vastus medialis oblique and vastus lateralis muscles. Phys. Ther. 1990, 70, 561–565. [Google Scholar] [CrossRef] [PubMed]
- Carlson, J.; Hobbs, L.; Smith, K. Isolation of the vastus medialis oblique muscle during semi-squat and straight leg raise exercises. Am. J. Sport. Med. 2010, 2, 40–53. [Google Scholar]
- Raj, N.B.; Hussin, N.A.; Bin Simbak, N.; Safee, M.K.M.; Rao, U.M. Quadriceps muscle activity during exercise. Res. J. Pharm. Technol. 2017, 10, 3312. [Google Scholar] [CrossRef]
- Livecchi, N.M.; Armstrong, C.W.; Cordova, M.L.; Merrick, M.A.; Rankin, J.M. Vastus lateralis and vastus medialis obliquus activity during a straight-leg raise and knee extension with lateral hip rotation. J. Sport Rehabil. 2002, 11, 120–126. [Google Scholar] [CrossRef][Green Version]
- Soderberg, G.L.; Cook, T.M. An electromyographic analysis of quadriceps femoris muscle setting and straight leg raising. Phys. Ther. 1983, 63, 1434–1438. [Google Scholar] [CrossRef]
- Coqueiro, K.R.R.; Bevilaqua-Grossi, D.; Bérzin, F.; Soares, A.B.; Candolo, C.; Monteiro-Pedro, V. Analysis on the activation of the VMO and VLL muscles during semisquat exercises with and without hip adduction in individuals with patellofemoral pain syndrome. J. Electromyogr. Kinesiol. 2005, 15, 596–603. [Google Scholar] [CrossRef]
- Stensdotter, A.-K.; Hodges, P.; Mellor, R.; Sundelin, G.; Häger, C. Quadriceps activation in closed and in open kinetic chain exercise. Med. Sci. Sport. Exerc. 2003, 35, 2043–2047. [Google Scholar] [CrossRef]
- Hodges, P.W.; A Richardson, C. The influence of isometric hip adduction on quadriceps femoris activity. Scand. J. Rehabil. Med. 1993, 25, 57–62. [Google Scholar] [PubMed]
- Bose, K.; Kanagasuntheram, R.; Osman, M.B.H. Vastus medialis oblique: An anatomic and physiologic study. Orthopedics 1980, 3, 880–883. [Google Scholar] [CrossRef] [PubMed]
- Thiranagamat, R.; Lanka, S. Nerve supply of the human vastus medialis muscle. J. Anat. 1990, 170, 193–198. [Google Scholar]
- Sugisaki, N.; Kurokawa, S.; Okada, J.; Kanehisa, H. Difference in the recruitment of hip and knee muscles between back squat and plyometric squat jump. PLoS ONE 2014, 9, e101203. [Google Scholar] [CrossRef]
- Karst, G.M.; Jewett, P.D. Electromyographic analysis of exercises proposed for differential activation of medial and lateral quadriceps femoris muscle components. Phys. Ther. 1993, 73, 286–295. [Google Scholar] [CrossRef] [PubMed]
- Noehren, B.; Snyder-Mackler, L. Who’s afraid of the big bad wolf? Open-chain exercises after anterior cruciate ligament reconstruction. J. Orthop. Sport. Phys. Ther. 2020, 50, 473–476. [Google Scholar] [CrossRef] [PubMed]
- Rivera, J.E. Open versus closed kinetic chain rehabilitation of the lower extremity: A functional and biomechanical analysis. J. Sport Rehabil. 1994, 3, 154–167. [Google Scholar] [CrossRef]
- Snyder-Mackler, L. Scientific rationale and physiological basis for the use of closed kinetic chain exercise in the lower extremity. J. Sport Rehabil. 1996, 5, 2–12. [Google Scholar] [CrossRef]
- Lepley, L.K. Deficits in quadriceps strength and patient-oriented outcomes at return to activity after ACL reconstruction: A review of the current literature. Sport. Health 2015, 7, 231–238. [Google Scholar] [CrossRef]
- Augustsson, J.; Esko, A.; Thomeé, R.; Svantesson, U. Weight training of the thigh muscles using closed versus open kinetic chain exercises: A comparison of performance enhancement. J. Orthop. Sport. Phys. Ther. 1998, 27, 3–8. [Google Scholar] [CrossRef][Green Version]
- Witvrouw, E.; Lysens, R.; Bellmans, J.; Peers, K.; Vanderstraeten, G. Open versus closed kinetic chain exercises for patellofemoral pain: A prospective, randomized study. Am. J. Sport. Med. 2000, 28, 687–694. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Exercises | Muscles | Non-HA | HA | Mean Difference (95%CI) | p-Value |
|---|---|---|---|---|---|
| SQ | RF | 24.10 ± 12.43 | 43.66 ± 22.78 | 19.56 (11.97 to 27.15) | <0.001 # |
| VMO | 45.28 ± 12.72 | 84.69 ± 28.61 | 39.42 (29.36 to 49.48) | <0.001 # | |
| VL | 41.52 ± 18.32 | 61.79 ± 28.72 | 20.27 (13.96 to 26.57) | <0.001 # | |
| KE | RF | 42.85 ± 23.26 | 52.22 ± 22.07 | 9.37 (−0.42 to 19.17) | 0.06 |
| VMO | 52.60 ± 23.23 | 57.96 ± 26.76 | 5.36 (−4.76 to 15.49) | 0.29 | |
| VL | 59.60 ± 32.11 | 61.53 ± 20.11 | 1.93 (−8.24 to 12.10) | 0.70 | |
| SLR | RF | 61.87 ± 21.25 | 48.62 ± 21.64 | −13.26 (−20.96 to −5.56) | 0.41 |
| VMO | 40.00 ± 18.42 | 52.29 ± 26.52 | 12.29 (4.78 to 19.81) | 0.65 | |
| VL | 46.25 ± 19.07 | 56.27 ± 27.87 | 10.03 (2.58 to 17.48) | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thongduang, P.; Chatchawan, U.; Puntumetakul, R.; Yamauchi, J.; Peungsuwan, P. Quadriceps Electromyographic Activity in Closed and Open Kinetic-Chain Exercises with Hip-Adductor Co-Contraction in Sedentary Women. Int. J. Environ. Res. Public Health 2022, 19, 12929. https://doi.org/10.3390/ijerph191912929
Thongduang P, Chatchawan U, Puntumetakul R, Yamauchi J, Peungsuwan P. Quadriceps Electromyographic Activity in Closed and Open Kinetic-Chain Exercises with Hip-Adductor Co-Contraction in Sedentary Women. International Journal of Environmental Research and Public Health. 2022; 19(19):12929. https://doi.org/10.3390/ijerph191912929
Chicago/Turabian StyleThongduang, Parinyathip, Uraiwan Chatchawan, Rungthip Puntumetakul, Junichiro Yamauchi, and Punnee Peungsuwan. 2022. "Quadriceps Electromyographic Activity in Closed and Open Kinetic-Chain Exercises with Hip-Adductor Co-Contraction in Sedentary Women" International Journal of Environmental Research and Public Health 19, no. 19: 12929. https://doi.org/10.3390/ijerph191912929
APA StyleThongduang, P., Chatchawan, U., Puntumetakul, R., Yamauchi, J., & Peungsuwan, P. (2022). Quadriceps Electromyographic Activity in Closed and Open Kinetic-Chain Exercises with Hip-Adductor Co-Contraction in Sedentary Women. International Journal of Environmental Research and Public Health, 19(19), 12929. https://doi.org/10.3390/ijerph191912929