
Factors That Affect the COVID-19 Pandemic in Summer 2022 Compared to Summer 2021



Abstract
:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Materials and Methods
2.1. Data Search and Extraction
- The number of new cases per million describes daily numbers of COVID-19 cases per million people;
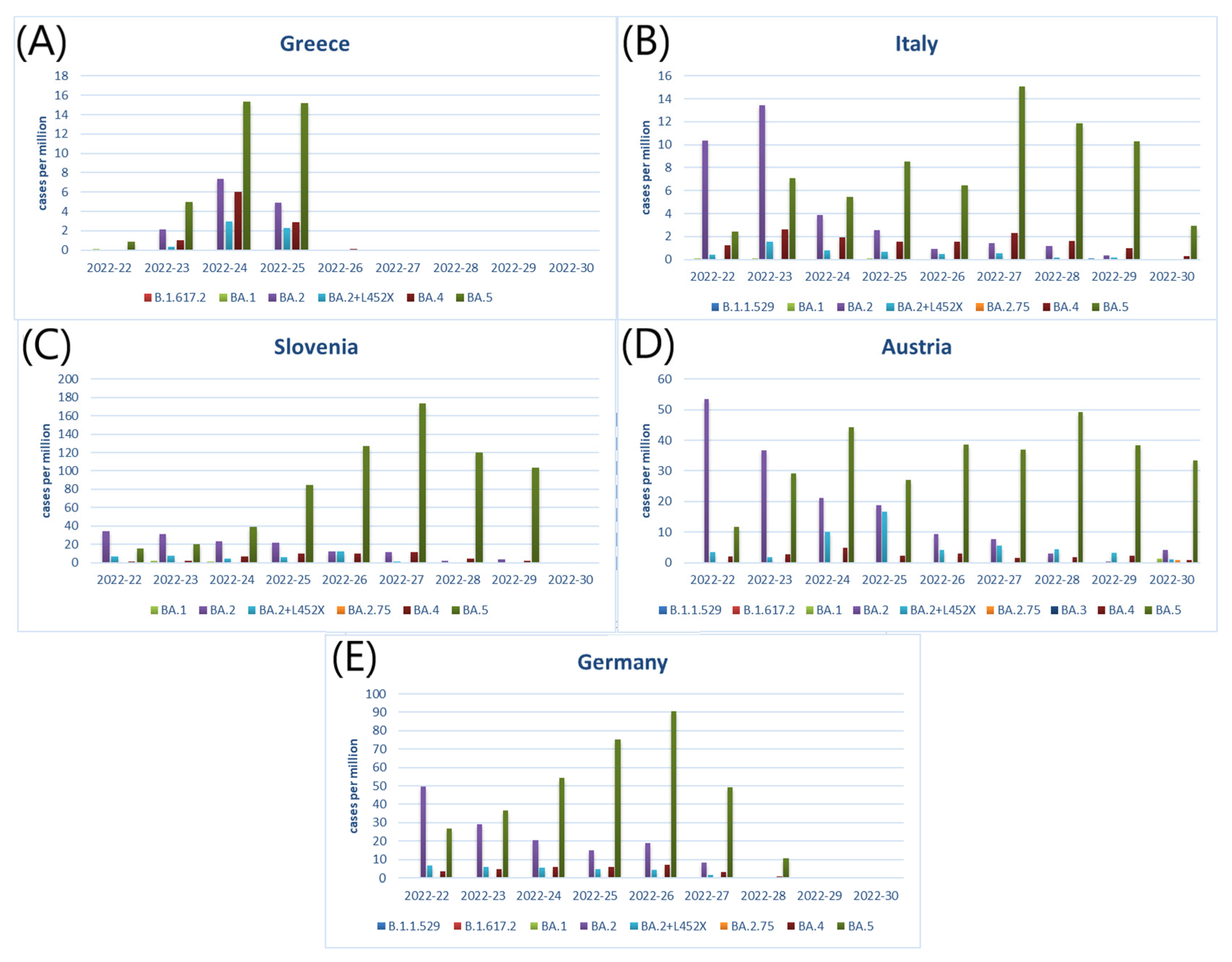
- The number of cases with different variant of SARS-CoV-2 describes the weekly numbers of COVID-19 cases with different variants of SARS-CoV-2;
- The number of people fully vaccinated per hundred describes the number of people who received all vaccine doses per hundred people;
- The total boosters per hundred describes the number of people who received booster doses per hundred people;
- Number of flights describes the number of air traffic.
- School closing (scale 0–3) describes the school and university closing;
- Workplace closing (scale 0–3) describes workplace closing;
- Cancelation of public events (scale 0–2) describes public events cancelling;
- Restrictions on gatherings (scale 0–4) describes the limits on gatherings;
- Close public transport (scale 0–2) describes public transport closing;
- Stay at home requirements (scale 0–3) describes recommendations to “stay at home”;
- Restrictions on internal movement (scale 0–2) describes restrictions on internal travels between cities and regions;
- International travel controls (scale 0–4) describes restrictions on international travel;
- Testing policy (scale 0–3) describes the government policy on accessing of PCR testing;
- Contact tracing (scale 0–2) describes government policy on contact tracing after a positive COVID-19 diagnosis;
- Facial coverings (scale 0–4) describes government policy on the use of facial coverings;
- Vaccination policy (scale 0–5) describes government policy on vaccine availability for different groups;
- Protection of elderly people (scale 0–3) describes government policy on protecting elderly people.
2.2. Statistical Analysis
3. Results
3.1. Countries Selection
3.2. The Distribution of SARS-CoV-2 Variants in 5 Selected Countries in the EU
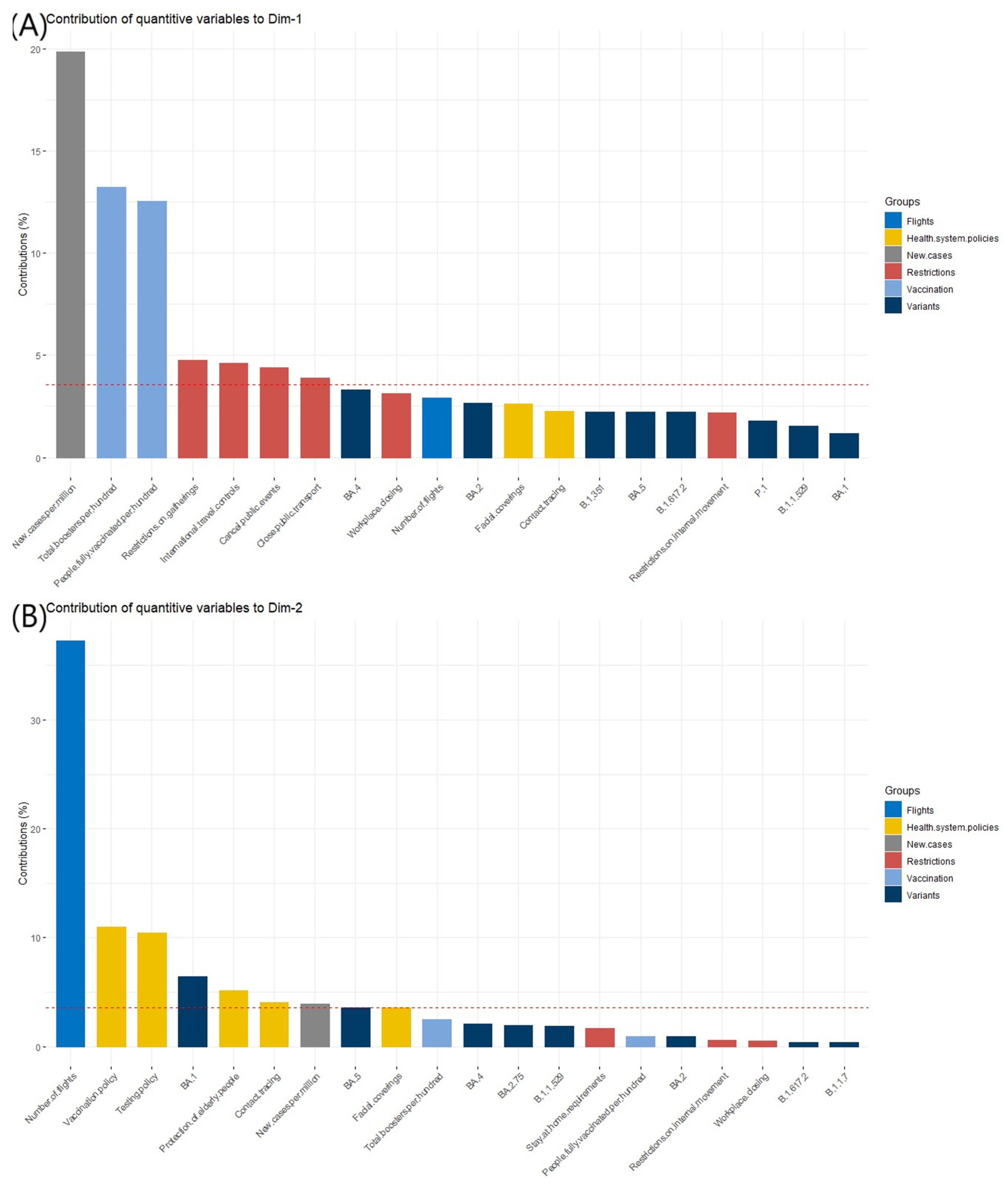
3.3. Contributing Variables to the Dimensions Definition
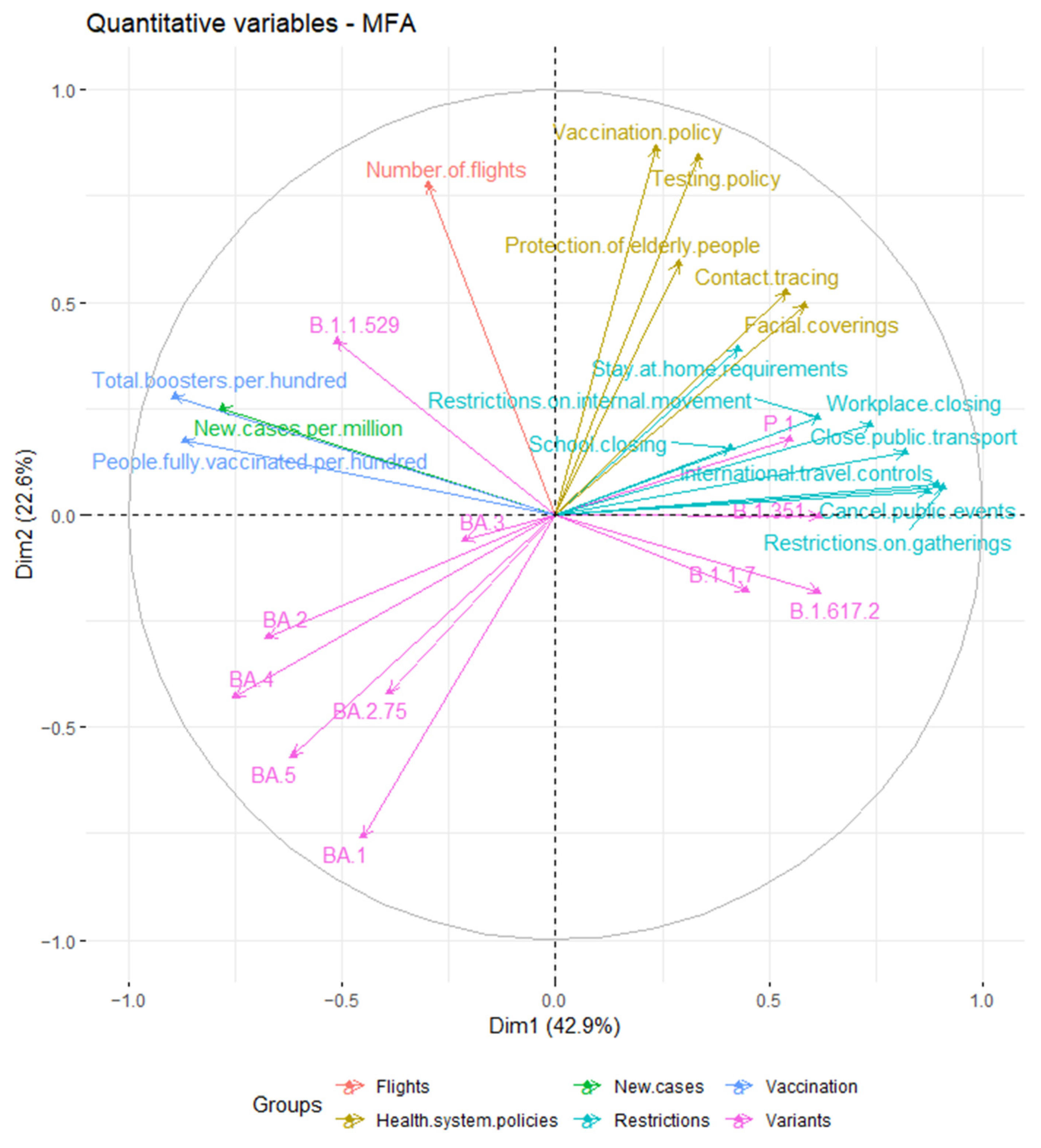
3.4. The Relationships between Analyzed Variables
3.5. The Comparison of Countries Profiles in Summer 2022 and Summer 2021
4. Discussion
4.1. Findings
4.2. Research Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Khosravizadeh, O.; Ahadinezhad, B.; Maleki, A.; Najafpour, Z.; Golmohammadi, R. Social Distance Capacity to Control the COVID-19 Pandemic: A Systematic Review on Time Series Analysis. Int. J. Risk Saf. Med. 2022, 33, 5–22. [Google Scholar] [CrossRef] [PubMed]
- Kwok, H.F. The Significance of Advanced COVID-19 Diagnostic Testing in Pandemic Control Measures. Int. J. Biol. Sci. 2022, 18, 4610–4617. [Google Scholar] [CrossRef] [PubMed]
- Cardwell, K.; O’Neill, S.M.; Tyner, B.; Broderick, N.; O’Brien, K.; Smith, S.M.; Harrington, P.; Ryan, M.; O’Neill, M. A Rapid Review of Measures to Support People in Isolation or Quarantine during the COVID-19 Pandemic and the Effectiveness of Such Measures. Rev. Med. Virol. 2022, 32, e2244. [Google Scholar] [CrossRef] [PubMed]
- Jiang, S.; Wu, S.; Zhao, G.; He, Y.; Bao, L.; Liu, J.; Qin, C.; Hou, J.; Ding, Y.; Cheng, A.; et al. Comparison of Wild Type DNA Sequence of Spike Protein from SARS-CoV-2 with Optimized Sequence on The Induction of Protective Responses Against SARS-CoV-2 Challenge in Mouse Model. Hum. Vaccines Immunother. 2022, 18, 2016201. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Wang, M.; Lin, W.; Dong, W.; Xu, J. “Mutation Blacklist” and “Mutation Whitelist” of SARS-CoV-2. J. Biosaf. Biosecur. 2022, 4, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Tracking SARS-CoV-2 Variants. Available online: https://www.who.int/activities/tracking-SARS-CoV-2-variants (accessed on 17 August 2022).
- Joshi, G.; Poduri, R. Omicron, a New SARS-CoV-2 Variant: Assessing the Impact on Severity and Vaccines Efficacy. Hum. Vaccines Immunother. 2022, 18, 2034458. [Google Scholar] [CrossRef] [PubMed]
- Dhawan, M.; Priyanka; Choudhary, O.P. Emergence of Omicron Sub-Variant BA.2: Is It a Matter of Concern amid the COVID-19 Pandemic? Int. J. Surg. 2022, 99, 106581. [Google Scholar] [CrossRef]
- Desingu, P.A.; Nagarajan, K.; Dhama, K. Emergence of Omicron Third Lineage BA.3 and Its Importance. J. Med. Virol. 2022, 94, 1808–1810. [Google Scholar] [CrossRef]
- Mahase, E. COVID-19: What We Know about the BA.4 and BA.5 Omicron Variants. BMJ 2022, 378, o1969. [Google Scholar] [CrossRef]
- COVID-19 Vaccine Tracker|European Centre for Disease Prevention and Control. Available online: https://qap.ecdc.europa.eu/public/extensions/COVID-19/vaccine-tracker.html#uptake-tab (accessed on 17 August 2022).
- Chen, J. Novel Statistics Predict the COVID-19 Pandemic Could Terminate in 2022. J. Med. Virol. 2022, 94, 2845–2848. [Google Scholar] [CrossRef]
- Coccia, M. COVID-19 Pandemic over 2020 (Withlockdowns) and 2021 (with Vaccinations): Similar Effects for Seasonality and Environmental Factors. Environ. Res. 2022, 208, 112711. [Google Scholar] [CrossRef] [PubMed]
- Worldometer—Real Time World Statistics. Available online: http://www.worldometers.info/ (accessed on 4 August 2022).
- Homepage|European Centre for Disease Prevention and Control. Available online: https://www.ecdc.europa.eu/en (accessed on 17 August 2022).
- COVID-19 Government Response Tracker. Available online: https://www.bsg.ox.ac.uk/research/research-projects/covid-19-government-response-tracker (accessed on 17 August 2022).
- Our World in Data. Available online: https://ourworldindata.org (accessed on 17 August 2022).
- EUROCONTROL|Supporting European Aviation. Available online: https://www.eurocontrol.int/ (accessed on 17 August 2022).
- Abdi, H.; Williams, L.J.; Valentin, D. Multiple Factor Analysis: Principal Component Analysis for Multitable and Multiblock Data Sets: Multiple Factor Analysis. WIREs Comput. Stat. 2013, 5, 149–179. [Google Scholar] [CrossRef]
- Bécue-Bertaut, M.; Pagès, J. Multiple Factor Analysis and Clustering of a Mixture of Quantitative, Categorical and Frequency Data. Comput. Stat. Data Anal. 2008, 52, 3255–3268. [Google Scholar] [CrossRef]
- Jarvis, C.I.; Gimma, A.; van Zandvoort, K.; Wong, K.L.M.; Abbas, K.; Villabona-Arenas, C.J.; O’Reilly, K.; Quaife, M.; Rosello, A.; Kucharski, A.J.; et al. The Impact of Local and National Restrictions in Response to COVID-19 on Social Contacts in England: A Longitudinal Natural Experiment. BMC Med. 2021, 19, 52. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wang, Z.; Wang, J.; Li, M.; Wang, S.; He, X.; Zhou, C. Evolution and Control of the COVID-19 Pandemic: A Global Perspective. Cities 2022, 130, 103907. [Google Scholar] [CrossRef]
- Han, E.; Tan, M.M.J.; Turk, E.; Sridhar, D.; Leung, G.M.; Shibuya, K.; Asgari, N.; Oh, J.; García-Basteiro, A.L.; Hanefeld, J.; et al. Lessons Learnt from Easing COVID-19 Restrictions: An Analysis of Countries and Regions in Asia Pacific and Europe. Lancet 2020, 396, 1525–1534. [Google Scholar] [CrossRef]
- Bakhati, D.; Agrawal, S. COVID-19 Pandemic Lockdown—Is It Affecting Our Skin Hygiene and Cosmetic Practice? J. Cosmet. Dermatol. 2022, 21, 1830–1836. [Google Scholar] [CrossRef]
- Tolentino, L.; Guthrie, B.; Baker, M.G.; Beck, N.K.; Chan, N.; Duchin, J.S.; Gomez, A.; Simckes, M.; Wasserman, C.; Cohen, M.A.; et al. Trends in the Use of Face Coverings in Publicly Accessible Spaces During the COVID-19 Pandemic, King County, Washington, November 2020–May 2021. Public Health Rep. 2022, 137, 841–848. [Google Scholar] [CrossRef]
- Andrejko, K.L.; Pry, J.M.; Myers, J.F.; Fukui, N.; De Guzman, J.L.; Openshaw, J.; Watt, J.P.; Lewnard, J.A.; Jain, S.; Abdulrahim, Y.; et al. Effectiveness of Face Mask or Respirator Use in Indoor Public Settings for Prevention of SARS-CoV-2 Infection—California, February–December 2021. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 212–216. [Google Scholar] [CrossRef]
- Collie, S.; Champion, J.; Moultrie, H.; Bekker, L.-G.; Gray, G. Effectiveness of BNT162b2 Vaccine against Omicron Variant in South Africa. N. Engl. J. Med. 2022, 386, 494–496. [Google Scholar] [CrossRef]
- Grewal, R.; Kitchen, S.A.; Nguyen, L.; Buchan, S.A.; Wilson, S.E.; Costa, A.P.; Kwong, J.C. Effectiveness of a Fourth Dose of COVID-19 MRNA Vaccine against the Omicron Variant among Long Term Care Residents in Ontario, Canada: Test Negative Design Study. BMJ 2022, 378, e071502. [Google Scholar] [CrossRef] [PubMed]
- Abu-Raddad, L.J.; Chemaitelly, H.; Ayoub, H.H.; AlMukdad, S.; Yassine, H.M.; Al-Khatib, H.A.; Smatti, M.K.; Tang, P.; Hasan, M.R.; Coyle, P.; et al. Effect of MRNA Vaccine Boosters against SARS-CoV-2 Omicron Infection in Qatar. N. Engl. J. Med. 2022, 386, 1804–1816. [Google Scholar] [CrossRef] [PubMed]
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Rickeard, T.; Gallagher, E.; Gower, C.; Kall, M.; Groves, N.; O’Connell, A.-M.; et al. COVID-19 Vaccine Effectiveness against the Omicron (B.1.1.529) Variant. N. Engl. J. Med. 2022, 386, 1532–1546. [Google Scholar] [CrossRef] [PubMed]
- SARS-CoV-2 Variants Dashboard. Available online: https://www.ecdc.europa.eu/en/covid-19/situation-updates/variants-dashboard (accessed on 20 August 2022).


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sobczak, M.; Pawliczak, R. Factors That Affect the COVID-19 Pandemic in Summer 2022 Compared to Summer 2021. Int. J. Environ. Res. Public Health 2022, 19, 12561. https://doi.org/10.3390/ijerph191912561
Sobczak M, Pawliczak R. Factors That Affect the COVID-19 Pandemic in Summer 2022 Compared to Summer 2021. International Journal of Environmental Research and Public Health. 2022; 19(19):12561. https://doi.org/10.3390/ijerph191912561
Chicago/Turabian StyleSobczak, Marharyta, and Rafał Pawliczak. 2022. "Factors That Affect the COVID-19 Pandemic in Summer 2022 Compared to Summer 2021" International Journal of Environmental Research and Public Health 19, no. 19: 12561. https://doi.org/10.3390/ijerph191912561
APA StyleSobczak, M., & Pawliczak, R. (2022). Factors That Affect the COVID-19 Pandemic in Summer 2022 Compared to Summer 2021. International Journal of Environmental Research and Public Health, 19(19), 12561. https://doi.org/10.3390/ijerph191912561