

A Survey on the Actual Use of and Reasons for Heated Tobacco Products in Patients with Rheumatoid Arthritis

Abstract
:1. Introduction
Background and Objectives
2. Materials and Methods
2.1. Patient and Public Involvement
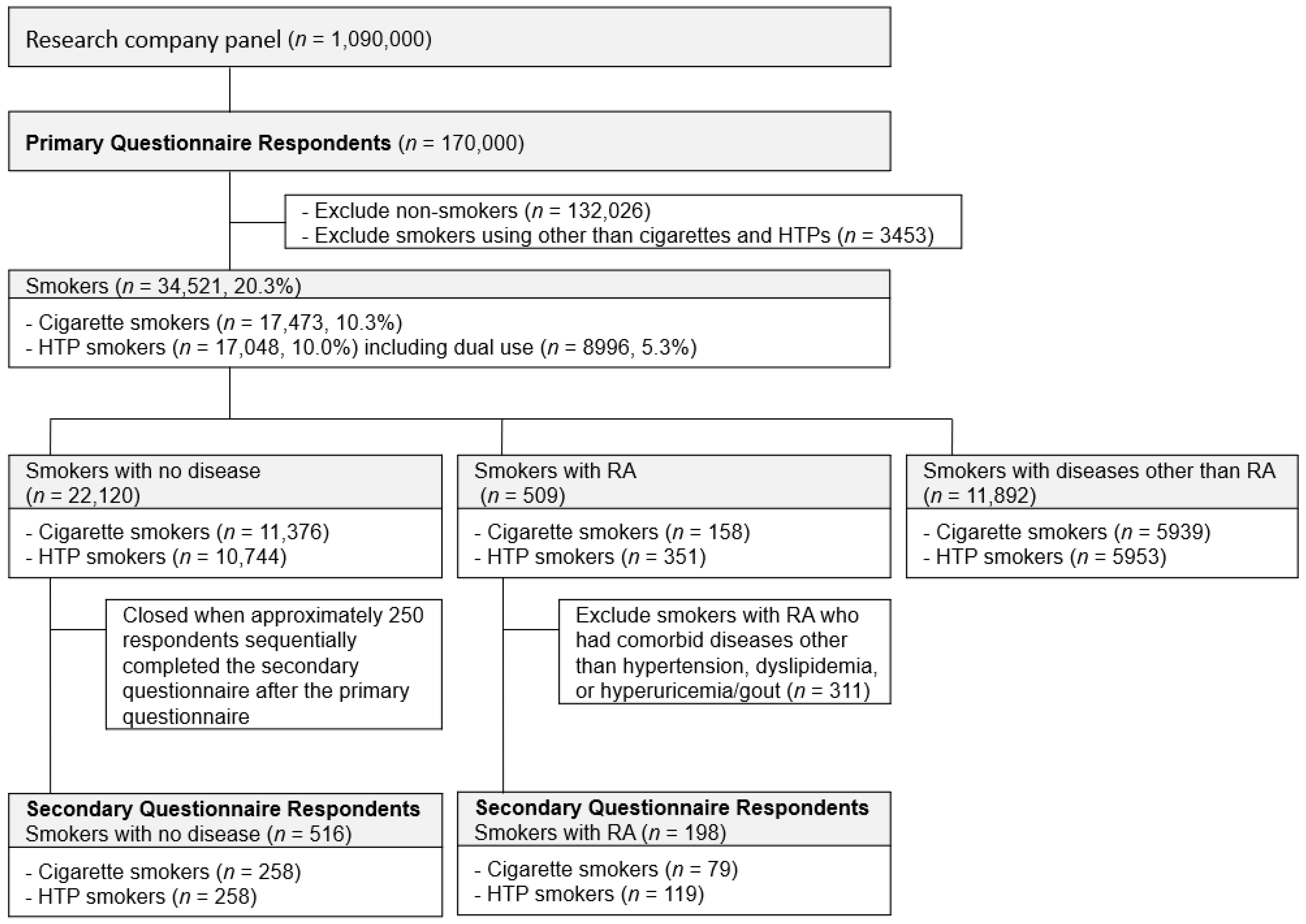
2.2. Participants
2.3. Variables
2.3.1. Current Smoking Status (Cigarettes, HTPs, Dual Use of Cigarettes and HTPs)
2.3.2. Current Disease Status
2.3.3. General Information
2.3.4. Details of HTP Use and Perceptions about HTPs
- reasons for HTP use;
- perceptions about the negative impact of HTPs on RA;
- consideration of HTP use due to RA;
- perceptions about whether RA is ameliorated by starting HTPs;
- changes in smoking frequency after starting HTPs.
2.4. Statistical Analysis
3. Results
3.1. Results of the Primary Questionnaire
3.1.1. The Prevalence of HTP Smokers with RA
3.1.2. Analysis of Predictors of HTP Use
3.2. Results of the Secondary Questionnaire
3.2.1. Characteristics of Participants who Completed the Secondary Questionnaire
3.2.2. Main Results from the Secondary Questionnaire
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- National Health and Nutrition Survey. 2020. Available online: https://www.mhlw.go.jp/content/10900000/000687163.pdf (accessed on 1 September 2022).
- Gravely, S.; Fong, G.T.; Sutanto, E.; Loewen, R.; Ouimet, J.; Xu, S.S.; Quah, A.C.K.; Thompson, M.E.; Boudreau, C.; Li, G.; et al. Perceptions of Harmfulness of Heated Tobacco Products Compared to Combustible Cigarettes among Adult Smokers in Japan: Findings from the 2018 ITC Japan Survey. Int. J. Environ. Res. Public Health 2020, 17, 2394. [Google Scholar] [CrossRef] [PubMed]
- Xu, S.S.; Meng, G.; Yan, M.; Gravely, S.; Quah, A.C.K.; Ouimet, J.; O’Connor, R.J.; Sutanto, E.; Yoshimi, I.; Mochizuki, Y.; et al. Reasons for Regularly Using Heated Tobacco Products among Adult Current and Former Smokers in Japan: Finding from 2018 ITC Japan Survey. Int. J. Environ. Res. Public Health 2020, 17, 8030. [Google Scholar] [CrossRef] [PubMed]
- Marija, B.; Tran, C.T.; de la Bourdonnaye, G.; Taranu, B.; Benzimra, M.; Haziza, C. Exposure to harmful and potentially harmful constituents decreased in smokers switching to Carbon-Heated Tobacco Product. Toxicol. Lett. 2020, 330, 30. [Google Scholar] [CrossRef] [PubMed]
- Harry, T.B.; Jamie, H.B.; Loren, K.; Erikas, S.; Leonie, B.; Sarah, J.; Lion, S.; Jamie, B. Heated tobacco products for smoking cessation and reducing smoking prevalence. Cochrane Database Syst Rev. 2022, 1, CD013790. [Google Scholar]
- Nakama, C.; Tabuchi, T. Use of heated tobacco products by people with chronic diseases: The 2019 JASTIS study. PLoS ONE 2021, 16, e0260154. [Google Scholar] [CrossRef]
- O’Keeffe, L.M.; Taylor, G.; Huxley, R.R.; Mitchell, P.; Woodward, M.; Peters, S.A.E. Smoking as a risk factor for lung cancer in women and men: A systematic review and meta-analysis. BMJ Open 2018, 8, e021611. [Google Scholar] [CrossRef]
- Poorolajal, J.; Moradi, L.; Mohammadi, Y.; Cheraghi, Z.; Gohari-Ensaf, F. Risk factors for stomach cancer: A systematic review and meta-analysis. Epidemiol. Health 2020, 42, e2020004. [Google Scholar] [CrossRef]
- Inoue, M.; JPHC Study Group. Impact of lifestyle on overall cancer risk among Japanese: The Japan Public Health Center-based Prospective Study (JPHC Study). J. Epidemiol. 2010, 20, 90–96. [Google Scholar] [CrossRef]
- Snider, G.L. Chronic obstructive pulmonary disease: Risk factors, pathophysiology and pathogenesis. Annu. Rev. Med. 1989, 40, 411–429. [Google Scholar] [CrossRef]
- Scanlon, P.D.; Connett, J.E.; Waller, L.A.; Altose, M.D.; Bailey, W.C.; Buist, A.S.; Tashkin, D.P. Smoking cessation and lung function in mild-to-moderate chronic obstructive pulmonary disease. The Lung Health Study. Am. J. Respir. Crit. Care Med. 2000, 161, 381–390. [Google Scholar] [CrossRef]
- Honjo, K.; Iso, H.; Tsugane, S.; Tamakoshi, A.; Satoh, H.; Tajima, K.; Suzuki, T.; Sobue, T. The effects of smoking and smoking cessation on mortality from cardiovascular disease among Japanese: Pooled analysis of three large-scale cohort studies in Japan. Tob. Control 2010, 19, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Inoue-Choi, M.; Freedman, N.D.; Saito, E.; Tanaka, S.; Hirabayashi, M.; Sawada, N.; Tsugane, S.; Usui, Y.; Ito, H.; Wang, C.; et al. Low-intensity cigarette smoking and mortality risks: A pooled analysis of prospective cohort studies in Japan. Int. J. Epidemiol. 2021, 51, 1276–1290. [Google Scholar] [CrossRef]
- Ishikawa, Y.; Terao, C. The Impact of Cigarette Smoking on Risk of Rheumatoid Arthritis: A Narrative Review. Cells 2020, 9, 475. [Google Scholar] [CrossRef] [PubMed]
- Källberg, H.; Ding, B.; Padyukov, L.; Bengtsson, C.; Rönnelid, J.; Klareskog, L.; Alfredsson, L. Smoking is a major preventable risk factor for rheumatoid arthritis: Estimations of risks after various exposures to cigarette smoke. Ann. Rheum. Dis. 2011, 70, 508–511. [Google Scholar] [CrossRef]
- Costenbader, K.H.; Feskanich, D.; Mandl, L.A.; Karlson, E.W. Smoking intensity, duration, and cessation, and the risk of rheumatoid arthritis in women. Am. J. Med. 2006, 119, 503–511. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, D.; Nishimura, K.; Tamaki, K.; Tsuji, G.; Nakazawa, T.; Morinobu, A.; Kumagai, S. Impact of smoking as a risk factor for developing rheumatoid arthritis: A meta-analysis of observational studies. Ann. Rheum. Dis. 2010, 69, 70–81. [Google Scholar] [CrossRef]
- Armstrong, A.; Harskamp, C.; Dhillon, J.; Armstrong, E. Psoriasis and smoking: A systematic review and meta-analysis. Br. J. Dermatol. 2014, 170, 304–314. [Google Scholar] [CrossRef]
- Naldi, L.; Chatenoud, L.; Linder, D.; Fortina, A.B.; Peserico, A.; Virgili, A.R.; Bruni, P.L.; Ingordo, V.; Scocco, G.L.; Solaroli, C.; et al. Cigarette smoking, body mass index, and stressful life events as risk factors for psoriasis: Results from an Italian case-control study. J. Invest. Dermatol. 2005, 125, 61–67. [Google Scholar] [CrossRef]
- Kantor, R.; Kim, A.; Thyssen, J.P.; Silverberg, J.I. Association of atopic dermatitis with smoking: A systematic review and meta-analysis. J. Am. Acad. Dermatol. 2016, 75, 1119–1125.e1. [Google Scholar] [CrossRef]
- Odani, S.; Tabuchi, T. Prevalence of heated tobacco product use in Japan: The 2020 JASTIS study. Tob. Control. 2021, 31, e64–e65. [Google Scholar] [CrossRef]
- Yamanaka, H.; Sugiyama, N.; Inoue, E.; Taniguchi, A.; Momohara, S. Estimates of the prevalence of and current treatment practices for rheumatoid arthritis in Japan using reimbursement data from health insurance societies and the IORRA cohort (I). Mod. Rheumatol. 2014, 24, 33. [Google Scholar] [CrossRef] [PubMed]
- Takano, Y.; Kohrogi, H.; Matsumoto, M.; Suga, M.; Ando, M. Lack of knowledge about smoking-related risks for diseases in the general public in Japan. Nihon Kokyuki Gakkai Zasshi 2001, 39, 389. [Google Scholar] [PubMed]
- Cintia, S.H.; Pablo, S.; Ayda, H.S.; Paula, B.D.; Walter, R.P.F.; Tiago, F.O.; Fernando, Q.C.; Sandra, H.P.F. Toxic mechanisms of cigarette smoke and heat-not-burn tobacco vapor inhalation on rheumatoid arthritis. Sci. Total Environ. 2022, 809, 151097. [Google Scholar]



{kind=link}
{kind=link}
| Total Smokers | Cigarette Smokers | HTP Smokers | p Value | |
|---|---|---|---|---|
| n (%) | n (%) | n (%) | ||
| Number | 34,521 (100.0) | 17,473 (50.6) | 17,048 (49.4) | |
| Sex | ||||
| Male | 25,440 (73.7) | 12,499 (45.2) | 12,941 (54.8) | <0.001 |
| Female | 9081 (26.3) | 4974 (54.8) | 4107 (45.2) | |
| Age (years) | ||||
| <60 | 27,637 (80.0) | 13,051 (47.2) | 14,586 (52.8) | <0.001 |
| ≥60 | 6884 (19.9) | 4422 (64.2) | 2462 (35.8) | |
| Residence | ||||
| Metropolitan area | 13,223 (38.3) | 6537 (49.4) | 6686 (50.6) | <0.001 |
| Other area | 21,298 (61.7) | 10,936 (51.3) | 10,362 (48.7) | |
| Equivalent household income (JPY) | ||||
| <4 MM | 9017 (26.1) | 5282 (58.6) | 3735 (41.4) | <0.001 |
| ≥4 MM | 19,438 (56.3) | 8927 (45.9) | 10,511 (54.1) | |
| Did not know/Unwilling to answer | 6066 (17.6) | 3264 (53.8) | 2802 (46.2) | |
| Current disease | ||||
| Hypertension | 4898 (14.2) | 2469 (50.4) | 2429 (49.6) | 0.754 |
| Diabetes | 2324 (6.7) | 1160 (49.9) | 1164 (50.1) | 0.484 |
| Dyslipidemia | 1882 (5.5) | 854 (45.4) | 1028 (54.6) | <0.001 |
| AD | 1765 (5.1) | 725 (41.1) | 1040 (58.9) | <0.001 |
| Hyperuricemia/Gout | 1089 (3.2) | 461 (42.3) | 628 (57.7) | <0.001 |
| Hepatic disease | 1080 (3.1) | 439 (40.6) | 641 (59.4) | <0.001 |
| CVD | 655 (1.9) | 306 (46.7) | 349 (53.3) | 0.044 |
| Psoriasis | 571 (1.7) | 195 (34.2) | 376 (65.8) | <0.001 |
| Cancer | 517 (1.5) | 202 (39.1) | 315 (60.9) | <0.001 |
| RA | 509 (1.5) | 158 (31.0) | 351 (69.0) | <0.001 |
| Kidney disease | 435 (1.3) | 162 (37.2) | 273 (62.8) | <0.001 |
| COPD | 309 (0.9) | 95 (30.7) | 214 (69.3) | <0.001 |
| Others | 2627 (7.6) | 1423 (54.2) | 1204 (45.8) | <0.001 |
| No current disease | 22,120 (64.1) | 11,376 (51.4) | 10,744 (48.6) | <0.001 |
| Smokers with No Disease | p Value | Smokers with RA | p Value | |||
|---|---|---|---|---|---|---|
| Cigarette Smokers (n = 258) | HTP Smokers (n = 258) | Cigarette Smokers (n = 79) | HTP Smokers (n = 119) | |||
| n (%) | n (%) | n (%) | n (%) | |||
| Sex | ||||||
| Male | 221 (85.7) | 228 (88.4) | 0.359 | 41 (51.9) | 74 (62.2) | 0.151 |
| Female | 37 (14.3) | 30 (11.6) | 38 (48.1) | 45 (37.8) | ||
| Age (years) | ||||||
| <60 | 203 (78.7) | 236 (91.5) | <0.001 | 47 (59.5) | 92 (77.4) | 0.007 |
| ≥60 | 55 (21.3) | 22 (8.5) | 32 (40.5) | 27 (22.7) | ||
| Residence | ||||||
| Metropolitan area | 104 (40.3) | 98 (38.0) | 0.588 | 23 (29.1) | 49 (41.2) | 0.084 |
| Other areas | 154 (59.7) | 160 (62.0) | 56 (70.9) | 70 (58.8) | ||
| Equivalent household income (JPY) | ||||||
| <4 MM | 80 (31.0) | 53 (20.5) | <0.001 | 24 (30.4) | 23 (19.3) | 0.032 |
| ≥4 MM | 126 (48.8) | 169 (65.5) | 39 (49.3) | 79 (66.4) | ||
| Did not know/Unwilling to answer | 52 (20.2) | 36 (14.0) | 16 (20.3) | 17 (14.3) | ||
| Drinking habit | ||||||
| Absent | 68 (26.4) | 40 (15.5) | 0.002 | 31 (39.2) | 29 (24.4) | 0.026 |
| Present | 190 (73.6) | 218 (84.5) | 48 (60.8) | 90 (75.7) | ||
| Number of cigarettes/HTPs smoked per day | ||||||
| ≤10 | 96 (37.2) | 94 (36.4) | 0.855 | 28 (35.4) | 43 (36.1) | 0.921 |
| >11 | 162 (62.8) | 164 (63.6) | 51 (64.6) | 76 (63.8) | ||
| Education level | ||||||
| Junior high school/High school/Other | 106 (41.1) | 76 (29.5) | 0.005 | 44 (55.7) | 38 (31.9) | 0.003 |
| University/Technical school/Graduate school | 136 (52.7) | 165 (64.0) | 34 (43.0) | 71 (59.7) | ||
| Unwilling to answer | 3 (1.2) | 2 (0.8) | 0 (0.0) | 5 (4.2) | ||
| Presence of cohabitants | ||||||
| Absent | 62 (24.0) | 43 (16.7) | 0.038 | 21 (26.6) | 12 (10.1) | 0.002 |
| Present | 196 (76.0) | 215 (83.3) | 58 (73.4) | 107 (89.9) | ||
| Smokers with RA | p Value | ||
|---|---|---|---|
| Cigarette Smokers (n = 79) | HTP Smokers (n = 119) | ||
| Disease duration | n (%) | n (%) | |
| <5 years | 37 (46.8) | 40 (33.6) | 0.091 |
| ≥5 years | 41 (51.9) | 73 (61.3) | |
| Did not know | 1 (1.3) | 6 (5.0) | |
| Disease activity | |||
| Mild | 45 (57.0) | 70 (58.8) | 0.795 |
| Moderate to Most severe | 34 (43.0) | 49 (41.2) | |
| Prior hospitalization due to RA | |||
| Yes | 16 (20.3) | 40 (33.6) | 0.041 |
| No | 63 (79.7) | 79 (66.4) | |
| (a) Reasons for HTP Use | HTP Smokers with No Disease (n = 258) | HTP Smokers with RA (n = 119) | pValue |
| What is the best reason to use HTPs? | n (%) | n (%) | |
| Less harmful to health | 70 (27.1) | 29 (24.4) | 0.571 |
| Less smoke and odor | 136 (52.7) | 63 (52.9) | |
| Taste | 17 (6.6) | 19 (16.0) | |
| Appearance/Fashion | 8 (3.1) | 4 (3.4) | |
| More smoking area | 23 (8.9) | 4 (3.4) | |
| Other | 4 (1.6) | 0 (0) | |
| (b) Perceptions Regarding the Negative Impact of HTPs on RA | Smokers with RA | pValue | |
| Cigarette Smokers (n = 79) | HTP Smokers (n = 119) | ||
| Do you think cigarettes and HTPs differ in their negative impact on RA? | n (%) | n (%) | |
| Yes—Cigarettes are more harmful | 36 (45.6) | 66 (55.5) | 0.173 |
| Yes—HTPs are more harmful | 4 (5.1) | 17 (14.3) | |
| No | 39 (49.4) | 36 (30.3) | |
| (c) Consideration of HTP Use Due to RA | Smokers with RA | pValue | |
| Cigarette Smokers (n = 79) | HTP Smokers (n = 119) | ||
| Have you ever considered using HTPs due to RA? | n (%) | n (%) | |
| Yes | 20 (25.3) | 52 (43.7) | 0.008 |
| No | 59 (74.7) | 67 (56.3) | |
| (d) Perceptions about whether RA Is Ameliorated by Starting HTPs | Smokers with RA | pValue | |
| Cigarette Smokers (n = 79) | HTP Smokers (n = 100) * | ||
| Do you feel that the use of HTPs relieves RA? (If you are not using HTPs, answer based on what you think might occur.) | n (%) | n (%) | |
| Yes | 17 (21.5) | 42 (42.0) | 0.008 |
| No | 62 (78.5) | 58 (58.0) | |
| (e) Changes in Smoking Frequency after Starting HTPs | Smokers with RA | pValue | |
| Cigarette Smokers (n = 79) | HTP Smokers (n = 100) * | ||
| After starting HTPs, did your smoking frequency change?/Do you think your smoking frequency will change once you start using HTPs? | n (%) | n (%) | |
| Yes—Increased/Will increase | 5 (6.3) | 33 (33.0) | < 0.001 |
| Yes—Decreased/Will decrease | 27 (34.2) | 33 (33.0) | |
| No | 47 (59.5) | 34 (34.0) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Isaji, H.; Yamada, K. A Survey on the Actual Use of and Reasons for Heated Tobacco Products in Patients with Rheumatoid Arthritis. Int. J. Environ. Res. Public Health 2022, 19, 12465. https://doi.org/10.3390/ijerph191912465
Isaji H, Yamada K. A Survey on the Actual Use of and Reasons for Heated Tobacco Products in Patients with Rheumatoid Arthritis. International Journal of Environmental Research and Public Health. 2022; 19(19):12465. https://doi.org/10.3390/ijerph191912465
Chicago/Turabian StyleIsaji, Hisaaki, and Kiyofumi Yamada. 2022. "A Survey on the Actual Use of and Reasons for Heated Tobacco Products in Patients with Rheumatoid Arthritis" International Journal of Environmental Research and Public Health 19, no. 19: 12465. https://doi.org/10.3390/ijerph191912465
APA StyleIsaji, H., & Yamada, K. (2022). A Survey on the Actual Use of and Reasons for Heated Tobacco Products in Patients with Rheumatoid Arthritis. International Journal of Environmental Research and Public Health, 19(19), 12465. https://doi.org/10.3390/ijerph191912465