
Effect of a Short-Term Intervention with Lactobacillus salivarius Probiotic on Early Childhood Caries—An Open Label Randomized Controlled Trial

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Protocol
2.2. Participants
2.2.1. Selection Criteria
2.2.2. Settings and Locations Where the Data Were Collected
2.3. Interventions
2.4. Outcome Measures
2.5. Clinical Examination and Data Collection
2.6. Sample Size
2.7. Randomization, Allocation Concealment Mechanism, Implementation and Blinding
2.8. Statistical Methods
3. Results
3.1. Participants Flow
3.2. Recruitment
3.3. Baseline Data
3.4. Numbers Analyzed
3.5. Effect on Dental Caries
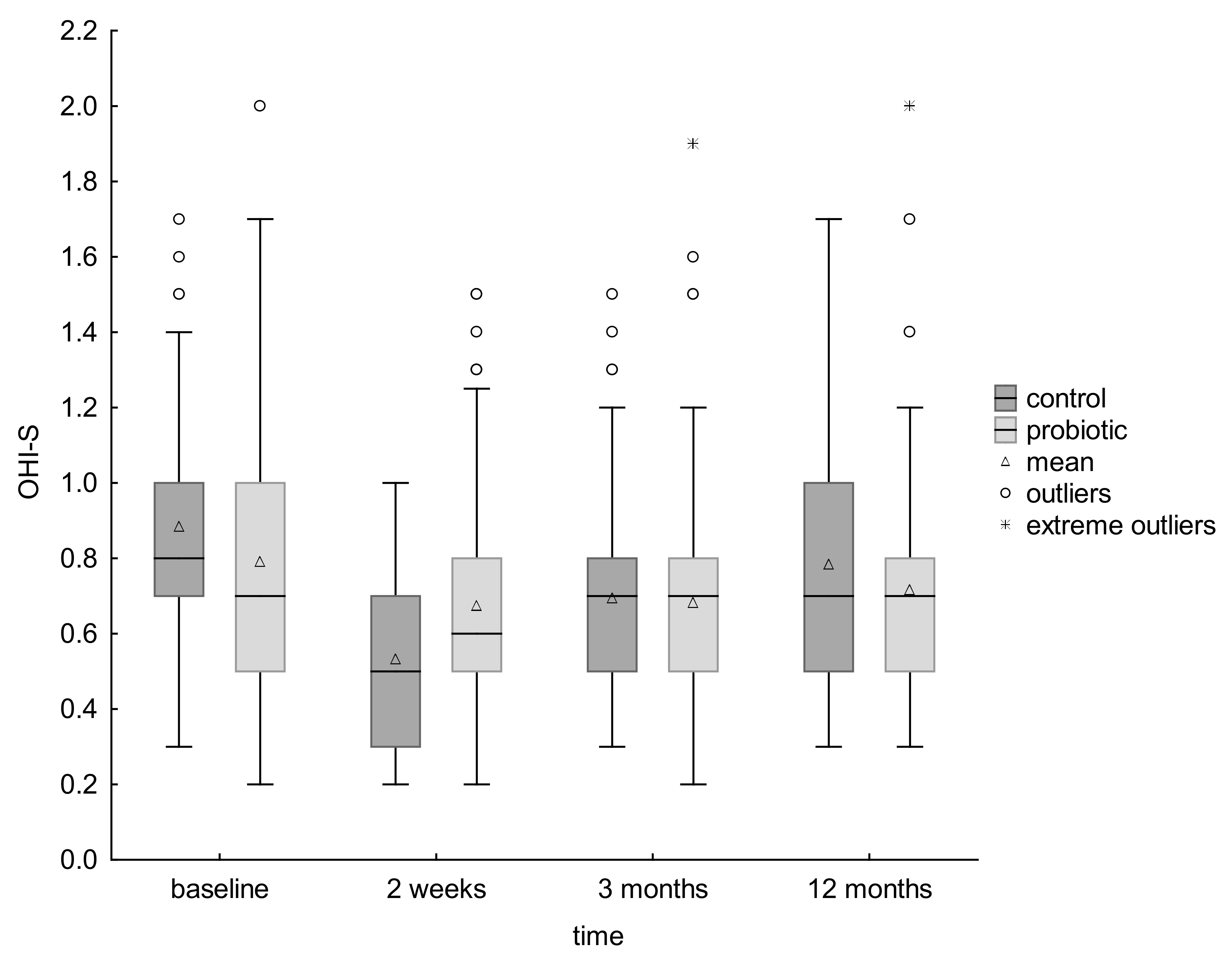
3.6. Effect on Dental Plaque
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Phantumvanit, P.; Makino, Y.; Ogawa, H.; Rugg-Gunn, A.; Moynihan, P.; Petersen, P.E.; Evans, W.; Feldens, C.A.; Lo, E.; Khoshnevisan, M.H.; et al. WHO Global Consultation on Public Health Intervention against Early Childhood Caries. Community Dent. Oral Epidemiol. 2018, 46, 280–287. [Google Scholar] [CrossRef] [PubMed]
- Kassebaum, N.J.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.; Marcenes, W. Global burden of untreated caries: A systematic review and metaregression. J. Dent. Res. 2015, 94, 650–658. [Google Scholar] [CrossRef] [PubMed]
- Paglia, L. The sweet danger of added sugars. Eur. J. Paediatr. Dent. 2019, 20, 89. [Google Scholar] [PubMed]
- Von Philipsborn, P.; Stratil, J.M.; Burns, J.; Busert, L.K.; Pfadenhauer, L.M.; Polus, S.; Holzapfel, C.; Hauner, H.; Rehfuess, E. Environmental interventions to reduce the consumption of sugar-sweetened beverages and their effects on health. Cochrane Database Syst. Rev. 2019, 6, CD012292. [Google Scholar] [CrossRef]
- Olczak-Kowalczyk, D.; Kaczmarek, U.; Bachanek, T.; Gozdowski, D.; Strużycka, I.; Turska-szybka, A.; Jurczak, A. Monitorowanie Stanu Zdrowia Jamy Ustnej Populacji Polskiej w Latach 2016-2020. Ocena Stanu Zdrowia Jamy Ustnej i Jego Uwarunkowań w Populacji Polskiej w Wieku 6, 10 i 15 Lat w 2018 Roku.( Monitoring the Health of the Oral Cavity of the Polish Population in 2016-2020. Assessment of Oral Health and Its Determinants in the Polish Population Aged 6, 10 and 15 in 2018); WUM: Warszawa, Polska, 2017; pp. 41–122. [Google Scholar]
- Leal, S.C.; Bronkhost, E.M.; Fan, M.; Frencken, J.E. Untreated cavitated dentine lesions: Impact on children’s quality of life. Caries Res. 2012, 46, 102–106. [Google Scholar] [CrossRef]
- Drummond, B.K.; Meldrum, A.M.; Boyd, D. Influence of dental care on children’s oral health and wellbeing. Br. Dent. J. 2013, 214, E27. [Google Scholar] [CrossRef]
- Casamassimo, P.S.; Thikkurissy, S.; Edelstein, B.L.; Maiorini, E. Beyond the dmft: The Human and Economic Cost of Early Childhood Caries. J. Am. Dent. Assoc. 2009, 140, 650–657. [Google Scholar] [CrossRef]
- Amin, M.; Nouri, R.; El Salhy, M.; Shah, P.; Azarpazhooh, A. Caries recurrence after treatment under general anaesthesia for early childhood caries: A retrospective cohort study. Eur. Arch. Paediatr. Dent. 2015, 16, 325–331. [Google Scholar] [CrossRef]
- Kirthiga, M.; Murugan, R.; Saikia, A.; Kirubakaran, R. Risk Factors for Early Childhood Caries: A Systematic Review and Meta-Analysis of Case Control and Cohort Studies. Pediatr. Dent. 2019, 41, 95–112. [Google Scholar]
- García-Godoy, F.; Hicks, M.J. Maintaining the integrity of the enamel surface: The role of dental biofilm, saliva and preventive agents in enamel demineralization and remineralization. J. Am. Dent. Assoc. 2008, 139, 25S–34S. [Google Scholar] [CrossRef]
- Banakar, M.; Moayedi, S.; Shamsoddin, E.; Vahedi, Z.; Banakar, M.H.; Mousavi, S.M.; Rokaya, D.; Bagheri Lankarani, K. Chewing Gums as a Drug Delivery Approach for Oral Health. Int. J. Dent. 2022, 2022, 9430988. [Google Scholar] [CrossRef]
- EAPD Guidelines on Prevention of Early Childhood Caries: An EAPD Policy Document. Available online: https://www.eapd.eu/uploads/1722F50D_file.pdf (accessed on 22 May 2021).
- A Collaborative Effort of the American Academy of Pedodontics and the American Academy of Pediatrics. Policy on early childhood caries (ECC): Classifications, consequences, and preventive strategies. Pediatr. Dent. 2016, 38, 52–54. [Google Scholar]
- Walsh, T.; Worthington, H.V.; Glenny, A.M.; Marinho, V.C.C.; Jeroncic, A. Fluoride toothpastes of different concentrations for preventing dental caries. Cochrane Database Syst. Rev. 2019, 3, CD007868. [Google Scholar] [CrossRef]
- Twetman, S. Prevention of dental caries as a non-communicable disease. Eur. J. Oral Sci. 2018, 126 (Suppl. S1), 19–25. [Google Scholar] [CrossRef]
- Meurman, J.H.; Stamatova, I.H. Probiotics: Evidence of Oral Health Implications. Folia Med. 2018, 60, 21–29. [Google Scholar] [CrossRef]
- Lin, T.H.; Lin, C.H.; Pan, T.M. The implication of probiotics in the prevention of dental caries. Appl. Microbiol. Biotechnol. 2018, 102, 577–586. [Google Scholar] [CrossRef]
- Hedayati-Hajikand, T.; Lundberg, U.; Eldh, C.; Twetman, S. Effect of probiotic chewing tablets on early childhood caries-a randomized controlled trial. BMC Oral Health 2015, 15, 112. [Google Scholar] [CrossRef]
- Stecksén-Blicks, C.; Sjöström, I.; Twetman, S. Effect of long-term consumption of milk supplemented with probiotic lactobacilli and fluoride on dental caries and general health in preschool children: A cluster-randomized study. Caries Res. 2009, 43, 374–381. [Google Scholar] [CrossRef]
- Food and Agriculture Organization of the United Nations and WHO. Guidelines for the Evaluation of Probiotics in Food. In Proceedings of the Joint FAO/WHO Working Group Report on Drafting Guidelines for the Evaluation of Probiotics in Food, London, ON, Canada, 30 April–1 May 2002. [Google Scholar]
- Poureslami, H.; Pishbin, L.; Eslaminejad, Z.; Moqadam, F.J.; Farokhi, M.R. The effects of a dairy probiotic product, espar, on salivary calcium and mutans streptococci. J. Dent. Res. Dent. Clin. Dent. Prospects. 2013, 7, 147–151. [Google Scholar]
- Stamatova, I.; Meurman, J.H. Probiotics: Health benefits in the mouth. Am. J. Dent. 2009, 22, 329–338. [Google Scholar]
- Twetman, S. Treatment protocols: Nonfluoride management of the caries disease process and available diagnostics. Dent. Clin. N. A. 2010, 54, 527–540. [Google Scholar] [CrossRef]
- Sales-Campos, H.; Castro Soares, S.; José Freire Oliveira, C. An introduction of the role of probiotics in human infections and autoimmune diseases. Crit. Rev. Microbiol. 2019, 45, 413–432. [Google Scholar] [CrossRef]
- Ben Taheur, F.; Kouidhi, B.; Fdhila, K.; Elabed, H.; Ben Salama, R.; Mahduan, K.; Bakharouf, A.; Chaieb, K. Antibacterial and antibiofilm activity of probiotic bacteria against oral pathogens. Microb. Pathog. 2016, 97, 213–220. [Google Scholar] [CrossRef]
- Twetman, L.; Larsen, U.; Fiehn, N.E.; Stecksén-Blicks, C.; Twetman, S. Coaggregation between probiotic bacteria and caries-associated strains: An in vitro study. Acta Odontol. Scand. 2009, 67, 284–288. [Google Scholar] [CrossRef]
- Näse, L.; Hatakka, K.; Savilahti, E.; Saxelin, M.; Pönkä, A.; Poussa, T.; Korpela, R.; Meurman, J.H. Effect of long-term consumption of a probiotic bacterium, Lactobacillus rhamnosus GG, in milk on dental caries and caries risk in children. Caries Res. 2001, 35, 412–420. [Google Scholar] [CrossRef]
- Pahumunto, N.; Piwat, S.; Chankanka, O.; Akkarachaneeyakorn, N.; Rangsitsathian, K.; Teanpaisan, R. Reducing mutans streptococci and caries development by Lactobacillus paracasei SD1 in preschool children: A randomized placebo-controlled trial. Acta Odontol. Scand. 2018, 76, 331–337. [Google Scholar] [CrossRef]
- Stensson, M.; Koch, G.; Coric, S.; Abrahamsson, T.R.; Jenmalm, M.C.; Birkhed, D.; Wendt, L.K. Oral administration of Lactobacillus reuteri during the first year of life reduces caries prevalence in the primary dentition at 9 years ofage. Caries Res. 2014, 48, 111–117. [Google Scholar] [CrossRef]
- Taipale, T.; Pienihäkkinen, K.; Alanen, P.; Jokela, J.; Söderling, E. Administration of Bifidobacterium animalis subsp. lactis BB-12 in early childhood: A post-trial effect on caries occurrence at four years of age. Caries Res. 2013, 47, 364–372. [Google Scholar] [CrossRef]
- Villavicencio, J.; Villegas, L.M.; Arango, M.C.; Arias, S.; Triana, F. Effects of a food enriched with probiotics on Streptococcus mutans and Lactobacillus spp. salivary counts in preschool children: A cluster randomized trial. J. Appl. Oral Sci. 2018, 26, e20170318. [Google Scholar] [CrossRef]
- Burton, J.P.; Drummond, B.K.; Chilcott, C.N.; Tagg, J.R.; Thomson, W.M.; Hale, J.D.F.; Wescombe, P.A. Influence of the probiotic Streptococcus salivarius strain M18 on indices of dental health in children: A randomized double-blind, placebo-controlled trial. J. Med. Microbiol. 2013, 62, 875–884. [Google Scholar] [CrossRef]
- Hasslöf, P.; West, C.E.; Videhult, F.; Brandelius, C.; Stecksén-Blicks, C. Early intervention with probiotic Lactobacillus paracasei F19 has no long-term effect on caries experience. Caries Res. 2013, 47, 559–565. [Google Scholar] [CrossRef] [PubMed]
- Angarita-Díaz, M.P.; Forero-Escobar, D.; Cerón-Bastidas, X.A.; Cisneros-Hidalgo, C.A.; Dávila-Narvaez, F.; Bedoya-Correa, C.M.; Freitas, S.; Cabrera-Arango, C.L.; Melo-Colina, R. Effects of a functional food supplemented with probiotics on biological factors related to dental caries in children: A pilot study. Eur. Arch. Paediatr. Dent. 2020, 21, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Nadelman, P.; Magno, M.B.; Masterson, D.; da Cruz, A.G.; Maia, L.C. Are dairy products containing probiotics beneficial for oral health? A systematic review and meta-analysis. Clin. Oral Investig. 2018, 22, 2763–2785. [Google Scholar] [CrossRef] [PubMed]
- Cagetti, M.G.; Mastroberardino, S.; Milia, E.; Cocco, F.; Lingström, P.; Campus, G. The use of probiotic strains in caries prevention: A systematic review. Nutrients 2013, 5, 2530–2550. [Google Scholar] [CrossRef] [Green Version]
- Laleman, I.; Detailleur, V.; Slot, D.E.; Slomka, V.; Quirynen, M.; Teughels, W. Probiotics reduce mutans streptococci counts in humans: A systematic review and meta-analysis. Clin. Oral Investig. 2014, 18, 1539–1552. [Google Scholar] [CrossRef] [PubMed]
- Gruner, D.; Paris, S.; Schwendicke, F. Probiotics for managing caries and periodontitis: Systematic review and meta-analysis. J. Dent. 2016, 48, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Sivamaruthi, B.S.; Kesika, P.; Chaiyasut, C. A Review of the Role of Probiotic Supplementation in Dental Caries. Probiotics Antimicrob. Proteins 2020, 12, 1300–1309. [Google Scholar] [CrossRef] [PubMed]
- Twetman, S.; Keller, M.K. Probiotics for caries prevention and control. Adv. Dent. Res. 2012, 24, 98–102. [Google Scholar] [CrossRef]
- Twetman, S. Are we ready for caries prevention through bacteriotherapy? Braz. Oral Res. 2012, 26, 64–70. [Google Scholar] [CrossRef]
- Hoare, A.; Marsh, P.D.; Diaz, P.L. Ecological therapeutic opportunities for oral diseases. Microbiol. Spectr. 2017, 5, 4. [Google Scholar] [CrossRef]
- Kilian, M.; Chapple, I.L.; Hannig, M.; Marsh, P.D.; Meuric, P.D.; Meuric, V.; Pedersen, A.; Tonetti, M.S.; Wade, W.G.; Zaura, E. The oral microbiome—An update for oral healthcare professionals. Br. Dent. J. 2016, 221, 657–666. [Google Scholar] [CrossRef]
- Alamoudi, N.M.; Almabadi, E.S.; El Ashiry, E.A.; El Derwi, D.A. Effect of Probiotic Lactobacillus reuteri on Salivary Cariogenic Bacterial Counts among Groups of Preschool Children in Jeddah, Saudi Arabia: A Randomized Clinical Trial. J. Clin. Pediatr. Dent. 2018, 42, 331–338. [Google Scholar] [CrossRef]
- Rodríguez, G.; Ruiz, B.; Faleiros, S.; Vistoso, A.; Marró, M.L.; Sánchez, J.; Urzúa, I.; Cabello, R. Probiotic Compared with Standard Milk for High-caries Children: A Cluster Randomized Trial. J. Dent. Res. 2016, 95, 402–407. [Google Scholar] [CrossRef]
- Jindal, G.; Pandey, R.K.; Singh, R.K.; Pandey, N. Can early exposure to probiotics in children prevent dental caries? A current perspective. J. Oral Biol. Craniofac. Res. 2012, 2, 110–115. [Google Scholar] [CrossRef] [Green Version]
- Nishihara, T.; Suzuki, N.; Yoneda, M.; Hirofuji, T. Effects of Lactobacillus salivarius-containing tablets on caries risk factors: A randomized open-label clinical trial. BMC Oral Health 2014, 14, 110. [Google Scholar] [CrossRef]
- Sañudo, A.I.; Luque, R.; Díaz-Ropero, M.P.; Fonollá, J.; Bañuelos, Ó. In vitro and in vivo anti-microbial activity evaluation of inactivated cells of Lactobacillus salivarius CECT 5713 against Streptococcus mutans. Arch. Oral Biol. 2017, 84, 58–63. [Google Scholar] [CrossRef]
- Krzyściak, W.; Kościelniak, D.; Papież, M.; Vyhouskaya, P.; Zagórska-Świeży, K.; Kołodziej, I.; Bystrowska, B.; Jurczak, A. Effect of a Lactobacillus Salivarius Probiotic on a Double-Species Streptococcus Mutans and Candida Albicans Caries Biofilm. Nutrients 2017, 9, 1242. [Google Scholar] [CrossRef]
- Hansson, L.; Hedner, T.; Dahlöf, B. Prospective randomized open blinded end-point (PROBE) study. A novel design for intervention trials. Prospective Randomized Open Blinded End-Point. Blood Press. 1992, 1, 113–119. [Google Scholar] [CrossRef]
- WHO. Oral Health Surveys: Basic Methods, 5th ed.; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- Staszczyk, M.; Kępisty, M.; Kołodziej, I.; Kościelniak, D.; Gregorczyk-Maga, I.; Jurczak, A.; Ciepły, J. Ocena stanu i trend próchnicy u dzieci 5, 7 i 12-letnich z województwa małopolskiego w porównaniu do populacji polskiej. Nowa Stomatol. 2018, 2, 55–65. [Google Scholar] [CrossRef]
- Rechmann, P.; Kinsel, R.; Featherstone, J.D.B. Integrating Caries Management by Risk Assessment (CAMBRA) and Prevention Strategies into the Contemporary Dental Practice. Compend. Contin. Educ. Dent. 2018, 39, 226–233. [Google Scholar]
- Dikmen, B. Icdas II Criteria (International Caries Detection and Assessment System). J. Istanb. Univ. Fac. Dent. 2015, 49, 63. [Google Scholar] [CrossRef]
- Greene, J.C.; Vermillion, J.R. The simplified oral hygiene index. J. Am. Dent. Assoc. 1964, 68, 7–13. [Google Scholar] [CrossRef]
- Peres, M.A.; Traebert, J.; Marcenes, W. Calibration of examiners for dental caries epidemiologic studies. Cad. Saude Publica 2001, 17, 153–159. (In Portuguese) [Google Scholar] [CrossRef]
- Enck, P.; Klosterhalfen, S. Placebos and the Placebo Effect in Drug Trials. Handb. Exp. Pharmacol. 2019, 260, 399–431. [Google Scholar] [CrossRef]
- Požgain, I.; Požgain, Z.; Degmečić, D. Placebo and nocebo effect: A mini-review. Psychiatr. Danub. 2014, 26, 100–107. [Google Scholar]
- Leonard, G.; Lafrenaye, S.; Goffaux, P. Randomized placebo-controlled cross-over designs in clinical trials: A gold standard to be reassessed. Curr. Med. Res. Opin. 2012, 28, 245–248. [Google Scholar] [CrossRef] [Green Version]
- Ballou, S.; Kaptchuk, T.J.; Hirsch, W.; Nee, J.; Iturrino, J.; Hall, K.; Kelley, J.M.; Cheng, V.; Kirsch, I.; Jacobson, E.; et al. Open-label versus double-blind placebo treatment in irritable bowel syndrome: Study protocol for a randomized controlled trial. Trials 2017, 18, 234. [Google Scholar] [CrossRef]
- Riley, P.; Moore, D.; Ahmed, F.; Sharif, M.O.; Worthington, H.V. Xylitol-containing products for preventing dental caries in children and adults. Cochrane Database Syst. Rev. 2015, 26, CD010743. [Google Scholar] [CrossRef]
- Janakiram, C.; Deepan Kumar, C.V.; Joseph, J. Xylitol in preventing dental caries: A systematic review and meta-analyses. J. Nat. Sci. Biol. Med. 2017, 8, 16–21. [Google Scholar] [CrossRef]
- Marghalani, A.A.; Guinto, E.; Phan, M.; Dhar, V.; Tinanoff, N. Effectiveness of Xylitol in Reducing Dental Caries in Children. Pediatr. Dent. 2017, 39, 103–110. [Google Scholar]
- Ritter, A.V.; Walter, R. Sturdevant’s Art and Science of Operative Dentistry, 7th ed.; Elsevier: Amsterdam, The Netherlands, 2018. [Google Scholar]
- Ismail, A.I.; Pitts, N.B.; Tellez, M. Authors of the International Caries Classification and Management System (ICCMS). The International Caries Classification and Management System (ICCMS™) An Example of a Caries Management Pathway. BMC Oral Health 2015, 15, S9. [Google Scholar] [CrossRef] [PubMed]
- Ismail, A.; Lim, S.; Tellez, M. Tooth Surface Level Caries Progression in the Primary Dentition among Preschool Children. Caries Res. 2015, 49, 442–448. [Google Scholar] [CrossRef] [PubMed]
- Motallaei, M.N.; Yazdanian, M.; Tebyanian, H.; Tahmasebi, E.; Alam, M.; Abbasi, K.; Seifalian, A.; Ranjbar, R.; Yazdanian, A. The Current Strategies in Controlling Oral Diseases by Herbal and Chemical Materials. Evid. Based Complement. Altern. Med. 2021, 2021, 3423001. [Google Scholar] [CrossRef] [PubMed]
- González-Cabezas, C. The chemistry of caries: Remineralization and demineralization events with direct clinical relevance. Dent. Clin. North Am. 2010, 54, 469–478. [Google Scholar] [CrossRef]
- Bellini, H.T.; Arneberg, P.; von der Fehr, F.R. Oral hygiene and caries. A review. Acta Odontol. Scand. 1981, 39, 257–265. [Google Scholar] [CrossRef]
- Figuero, E.; Nóbrega, D.F.; García-Gargallo, M.; Tenuta, L.M.A.; Herrera, D.; Carvalho, J.C. Mechanical and chemical plaque control in the simultaneous management of gingivitis and caries: A systematic review. J. Clin. Periodontol. 2017, 44, S116–S134. [Google Scholar] [CrossRef]
- Stone, V.N.; Xu, P. Targeted antimicrobial therapy in the microbiome era. Mol. Oral Microbiol. 2017, 32, 446–454. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Characteristic | Control Group | Probiotic Group | Dropouts | Control vs. Probiotic | Probiotic vs. Dropouts | Examine Groups vs. Dropouts |
|---|---|---|---|---|---|---|
| Participants, n | 70 | 57 | 13 | |||
| Male, n (%) | 39 (55.71%) | 31 (54.39%) | 8 (61.54%) | p = 0.88 b | p = 0.64 b | p = 0.66 b |
| Female, n (%) | 31 (44.29%) | 26 (45.61%) | 5 (38,.46%) | p = 0.88 b | p = 0.64 b | p = 0.66 b |
| Age, mean ± SD | 4.51 ± 0.94 | 4.59 ± 0.92 | 4.46 ± 1.45 | p = 0.76 a | p = 0.9 a | p = 0.98 a |
| ICDAS 1–6 > 0, n (%) | 35 (50%) | 28 (49.12%) | 6 (46.15%) | p = 0.93 b | p = 0.85 b | p = 0.81 b |
| d(ICDAS 1–6) mft, mean ± SD | 5.67 ± 6.68 | 5.93 ± 6.68 | 5.23 ± 6.29 | p = 0.83 a | p = 0.66 a | p = 0.70 a |
| OHI-S, mean ± SD | 0.88 ± 0.32 | 0.79 ± 0.43 | 0.86 ± 0.48 | p = 0.04a | p = 0.72 a | p = 0.93 a |
| Effect | Cohen’s d | Mann-Whitney Test | Q3 | Q1 | Max | Min | SD | Median | Mean | n | Group | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| no effect | 0.016 | p = 0.925 | 9.75 | 0 | 20 | 0 | 6.68 | 3 | 5.671 | 70 | control | d(ICDAS 1–6) mft, baseline | |
| 12 | 0 | 20 | 0 | 6.68 | 3 | 5.93 | 57 | probiotic | |||||
| small | 0.217 | p = 0.214 | 11.75 | 0 | 21 | 0 | 6.75 | 6 | 7.043 | 70 | control | d(ICDAS 1–6) mft, | 12 months |
| 11 | 0 | 20 | 0 | 6.26 | 4 | 5.825 | 57 | probiotic | |||||
| large | 1.087 | p < 0.001 | 2 | 0 | 7 | 0 | 1.63 | 1 | 1.371 | 70 | control | Δ d(ICDAS 1–6) mft, | 12 months—baseline |
| 0 | 0 | 4 | −6 | 1.18 | 0 | −0.105 | 57 | probiotic | |||||
| no effect | 0.074 | p = 0.661 | 6 | 0 | 14 | 0 | 4.38 | 1 | 3.429 | 70 | control | d(ICDAS 1–2) mft, baseline | |
| 7 | 0 | 15 | 0 | 4.75 | 2 | 3.947 | 57 | probiotic | |||||
| small | 0.135 | p = 0.434 | 7 | 0 | 18 | 0 | 5.04 | 4 | 4.643 | 70 | control | d(ICDAS 1–2) mft, | 12 months |
| 8 | 0 | 15 | 0 | 4.72 | 3 | 4.07 | 57 | probiotic | |||||
| intermediate | 0.517 | p = 0.002 | 3 | 0 | 11 | −5 | 2.5 | 0 | 1.214 | 70 | control | Δ d(ICDAS 1–2) mft, | 12 months—baseline |
| 0 | 0 | 5 | −4 | 1.45 | 0 | 0.123 | 57 | probiotic | |||||
| no effect | 0.029 | p = 0.865 | 7 | 0 | 14 | 0 | 4.61 | 3 | 3.971 | 70 | control | d(ICDAS 3–6) mft, baseline | |
| 7 | 0 | 15 | 0 | 4.86 | 2 | 4.053 | 57 | probiotic | |||||
| small | 0.215 | p = 0.218 | 10 | 0 | 21 | 0 | 6.35 | 6 | 6.5 | 70 | control | d(ICDAS 3–6) mft, | 12 months |
| 10 | 0 | 19 | 0 | 5.89 | 2 | 5.228 | 57 | probiotic | |||||
| intermediate | 0.593 | p < 0.001 | 4.75 | 0 | 10 | −5 | 2.84 | 2 | 2.529 | 70 | control | Δ d(ICDAS 3–6) mft, | 12 months—baseline |
| 2 | 0 | 8 | −1 | 1.99 | 0 | 1.175 | 57 | probiotic | |||||
| no effect | 0.015 | p = 0.931 | 5 | 0 | 13 | 0 | 4.05 | 1 | 3.157 | 70 | control | d(ICDAS 4–6) mft, baseline | |
| 6 | 0 | 14 | 0 | 4.41 | 1 | 3.544 | 57 | probiotic | |||||
| small | 0.278 | p = 0.11 | 10 | 0 | 21 | 0 | 6.29 | 5.5 | 6.214 | 70 | control | d(ICDAS 4–6) mft, | 12 months |
| 8 | 0 | 14 | 0 | 5.08 | 2 | 4.351 | 57 | probiotic | |||||
| intermediate | 0.697 | p < 0.001 | 6 | 0 | 12 | −3 | 3.49 | 2 | 3.057 | 70 | control | Δ d(ICDAS 4–6) mft, | 12 months—baseline |
| 1 | 0 | 8 | −6 | 2.01 | 0 | 0.807 | 57 | probiotic | |||||
| NNT (Harm or Benefit) | Absolute Risk AR (95% CI) | ARR or ARI | Relative Risk RR (95% CI) | Prevented Fraction (PF) | Odds Ratio OR | (95% CI) | Binominal Proportions Test | Control Group | Probiotic Group | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 70 | 57 | n | |||||||||||||
| NNT (Benefit) = 114 | 0.88% | (−16.61%, 18.36%) | 0.9825 | (0.6902, 1.3985) | p = 0.92 | 3% | 0.9655 | (0.4797, 1.9432) | p = 0.92 | p = 0.92 | 35 | −50% | 28 (49,12%) | ICDAS 1–6 > 0, baseline, n (%) | |
| NNT (Benefit) = 6.74 | 14.84% | (−2.25%, 31.93%) | 0.7742 | (0.5701, 1.0515) | p = 0.1013 | 46% | 0.5404 | (0.2640, 1.1062) | p = 0.092 | p = 0.09 | 46 (65.71%) | 29 (50.88%) | ICDAS 1–6 > 0. 12 months. n (%) | ||
| NNT (Benefit) = 7.16 | 13.96% | (4.78%, 23.14%) | 0.1116 | (0.0149, 0.8391) | p = 0.0331 | 90% | 0.0958 | (0.012, 0.7663) | p = 0.027 | p = 0.075 | 11 (15.71%) | 1 (1.75%) | ΔICDAS 1–6 > 0. 12 months—baseline. n (%) | ||
| NNT (Harm) = 147.8 | 0.68% | (−16.57%, 17.92%) | 10.163 | (0.6727, 1.5355) | p = 0.94 | 0% | 1.0282 | (0.5060, 2.0892) | p = 0.94 | p = 0.94 | 29 (41.43%) | 24 (42.11%) | ICDAS 1–2 > 0. baseline. n (%) | ||
| NNT (Harm) = 10.53 | 9.50% | (−5.30%, 24.30%) | 15.115 | (0.7947, 2.8748) | p = 0.21 | 0% | 17.111 | (0.7426, 3.9425) | p = 0.21 | p = 0.21 | 13 (18.57%) | 16 (28.07%) | ICDAS 1–2 > 0. 12 months. n (%) | ||
| NNT (Benefit) = 18.56 | 5.39% | (−1.54%, 12.32%) | 0.2456 | (0.0295, 2.043) | p = 0.19 | 77% | 0.2321 | (0.0263, 2.0467) | p = 0.19 | p = 0.15 | 5 (7.14%) | 1 (1.75%) | ΔICDAS 1–2 > 0. 12 months—baseline. n (%) | ||
| NNT (Benefit) = 21.22 | 4.71% | (−12.70%, 22.12%) | 0.9030 | (0.6175, 1.3204) | p = 0.60 | 13% | 0.872 | (0.4098, 1.6698) | p = 0.60 | p = 0.60 | 34 (48.57%) | 25 (43.86%) | ICDAS 3–6 > 0. baseline. n (%) | ||
| NNT (Benefit) = 3.23 | 30.95% | (14.35%, 47.56%) | 0.5185 | (0.3453, 0.7786) | p = 0.0015 | 72% | 0.2778 | (0.1330, 0.5801) | p = 0.0007 | p = 0.00052 | 45 (64.29%) | 19 (33.33%) | ICDAS 3–6 > 0. 12 months. n (%) | ||
| NNT (Benefit) = 4.27 | 23.43% | (9.34%, 37.53%) | 0.3439 | (0.1605, 0.7365) | p = 0.006 | 75% | 0.2520 | (0.0994, 0.6386) | p = 0.0037 | p = 0.0025 | 25 (35.71%) | 7 (12.28%) | ΔICDAS 3–6 > 0. 12 months—baseline. n (%) | ||
| NNT (Benefit) = 7.24 | 13.81% | (−3.21%, 30.74%) | 0.7071 | (0.4540, 1.1013) | p = 0.12 | 44% | 0.5606 | (0.2719, 1.1558) | p = 0.12 | p = 0.12 | 33 (47,14%) | 19 (33.33%) | ICDAS 4–6 > 0. baseline. n (%) | ||
| NNT (Benefit) = 2.67 | 37.52% | (21.86%, 53.18%) | 0.3594 | (0.2095, 0.6168) | p = 0.0002 | 82% | 0.1886 | (0.0852, 0.4176) | p < 0.0001 | p = 0.00002 | 41 (58.57%) | 12 (21.05%) | ICDAS 4–6 > 0. 12 months. n (%) | ||
| NNT (Benefit) = 2.83 | 35.39% | (23.57%, 47.21%) | 0.0472 | (0.0066, 0.3375) | p = 0.0023 | 97% | 0.0302 | (0.0039, 0.2315) | p = 0.0008 | p = 0.000001 | 26 (37.14%) | 1 | (1.75%) | Δ ICDAS 4–6 > 0, 12 months—baseline, n (%) | |
| Variable | B | Standard Error | p | Odds Ratio | 95% CI for Odds Ratio | |
|---|---|---|---|---|---|---|
| Low Limit | Upper Limit | |||||
| Age | 0.176 | 0.234 | 0.451 | 1.193 | 0.754 | 1.886 |
| Sex | 0.351 | 0.430 | 0.415 | 1.420 | 0.611 | 3.299 |
| Group control vs. probiotic | −1.407 | 0.477 | 0.003 | 0.245 | 0.096 | 0.625 |
| Variable | B | Standard Error | p | Odds Ratio | 95% CI for Odds Ratio | |
|---|---|---|---|---|---|---|
| Low Limit | Upper Limit | |||||
| Age | 0.201 | 0.263 | 0.443 | 1.223 | 0.731 | 2.047 |
| Sex | 0.270 | 0.486 | 0.579 | 1.310 | 0.505 | 3.398 |
| Group control vs. probiotic | −3.533 | 1.041 | 0.001 | 0.029 | 0.004 | 0.225 |
| Variable | B | Standard Error | p | Odds Ratio | 95% CI for Odds Ratio | |
|---|---|---|---|---|---|---|
| Low Limit | Upper Limit | |||||
| Age | −0.172 | 0.450 | 0.703 | 0.842 | 0.349 | 2.034 |
| Sex | −0.207 | 0.848 | 0.807 | 0.813 | 0.154 | 4.282 |
| Group control vs. probiotic | 1.453 | 1.112 | 0.191 | 4.276 | 0.484 | 37.786 |
| OHI-S | n | Mean | SD | Median | Q1 | Q3 | Min | Max | Friedman Test | Durbin-Conover Post Hoc Test a | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Control Group | Baseline | 70 | 0.88 | 0.32 | 0.80 | 0.7 | 1.0 | 0.3 | 1.7 | χ2 = 107.833 p = 0.00 | Baseline—2 weeks Baseline—3 months Baseline—12 months 2 weeks—3 months 2 weeks—12 months 3 months—12 months |
| 2 weeks | 70 | 0.53 | 0.21 | 0.50 | 0.3 | 0.7 | 0.20 | 1.00 | |||
| 3 months | 70 | 0.69 | 0.30 | 0.70 | 0.5 | 0.8 | 0.30 | 1.50 | |||
| 12 months | 70 | 0.78 | 0.33 | 0.70 | 0.5 | 1 | 0.30 | 1.70 | |||
| Probiotic Group | Baseline | 57 | 0.79 | 0.43 | 0.70 | 0.5 | 1 | 0.2 | 2.0 | χ2= 14.9821 p = 0.002 | Baseline—2 weeks Baseline—3 months 3 months—12 months |
| 2 weeks | 57 | 0.67 | 0.35 | 0.60 | 0.5 | 0.8 | 0.20 | 1.50 | |||
| 3 months | 57 | 0.68 | 0.34 | 0.70 | 0.5 | 0.8 | 0.20 | 1.90 | |||
| 12 months | 57 | 0.72 | 0.31 | 0.70 | 0.5 | 0.8 | 0.30 | 2.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Staszczyk, M.; Jamka-Kasprzyk, M.; Kościelniak, D.; Cienkosz-Stepańczak, B.; Krzyściak, W.; Jurczak, A. Effect of a Short-Term Intervention with Lactobacillus salivarius Probiotic on Early Childhood Caries—An Open Label Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 12447. https://doi.org/10.3390/ijerph191912447
Staszczyk M, Jamka-Kasprzyk M, Kościelniak D, Cienkosz-Stepańczak B, Krzyściak W, Jurczak A. Effect of a Short-Term Intervention with Lactobacillus salivarius Probiotic on Early Childhood Caries—An Open Label Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2022; 19(19):12447. https://doi.org/10.3390/ijerph191912447
Chicago/Turabian StyleStaszczyk, Małgorzata, Małgorzata Jamka-Kasprzyk, Dorota Kościelniak, Beata Cienkosz-Stepańczak, Wirginia Krzyściak, and Anna Jurczak. 2022. "Effect of a Short-Term Intervention with Lactobacillus salivarius Probiotic on Early Childhood Caries—An Open Label Randomized Controlled Trial" International Journal of Environmental Research and Public Health 19, no. 19: 12447. https://doi.org/10.3390/ijerph191912447
APA StyleStaszczyk, M., Jamka-Kasprzyk, M., Kościelniak, D., Cienkosz-Stepańczak, B., Krzyściak, W., & Jurczak, A. (2022). Effect of a Short-Term Intervention with Lactobacillus salivarius Probiotic on Early Childhood Caries—An Open Label Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 19(19), 12447. https://doi.org/10.3390/ijerph191912447