
Comparison of the Effectiveness of the Ultrasonic Method and Cone-Beam Computed Tomography Combined with Intraoral Scanning and Prosthetic-Driven Implant Planning Method in Determining the Gingival Phenotype in the Healthy Periodontium

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
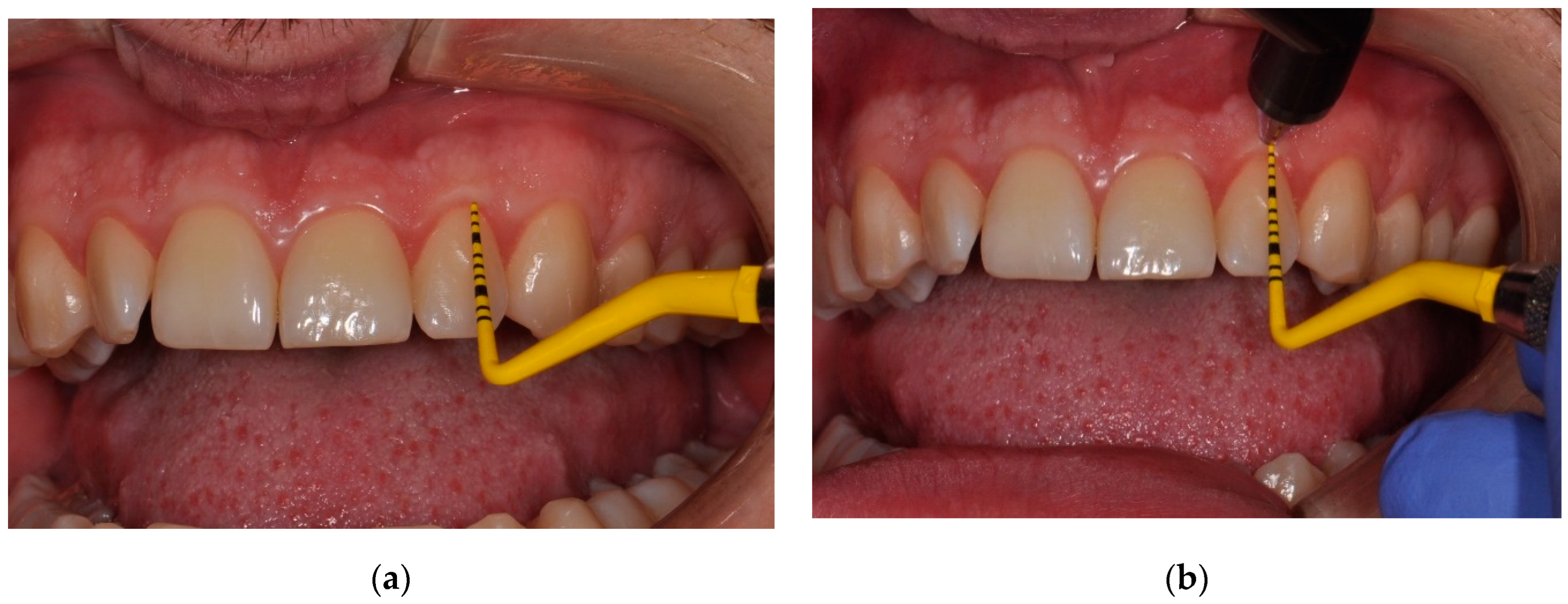
- (a)
- no general diseases,
- (b)
- good oral hygiene (Approximal Plaque Index < 15%),
- (c)
- BOP (Bleeding on probing) for the entire oral cavity <10%,
- (d)
- no loss of clinical attachment in the examined areas (Clinical Attachment Level/Loss, CAL = 0),
- (e)
- not using drugs that may affect the structure of periodontal tissues,
- (f)
- no addictions, especially nicotine use/mainly cigarette smoking,
- (g)
- not using removable prosthetic restorations and orthodontic appliances,
- (h)
- no contraindications for radiological examination.
2.1. Clinical and Radiological Assessment
- GT ≤ 0.7 mm—thin gingival phenotype,
- GT > 0.7 mm ≤ 1.0 mm—medium gingival phenotype,
- GT > 1.0 mm—thick gingival phenotype.
2.2. Ultrasound Examination
2.3. Cone-Beam Computed Tomography/Computer-Aided Design and Prosthetic-Driven Implant Planning
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ercoli, C.; Caton, J.G. Dental prostheses and tooth-related factors. J. Clin. Periodontol. 2018, 45 (Suppl. S20), 207–218. [Google Scholar] [CrossRef] [PubMed]
- Jepsen, S.; Caton, G.; Albandar, J.M.; Bissada, N.F.; Bouchard, P.; Cortellini, P.; Demirel, K.; de Sanctis, M.; Ercoli, C.; Fan, J.; et al. Periodontal manifestations of systemic diseases and developmental and acquired conditions: Consensus report of workgroup 3 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45 (Suppl. S20), 219–229. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.M.; Bassir, S.H.; Nguyen, T.T. Effect of gingival phenotype on the maintenance of periodontal health: An American Academy of Periodontology best evidence review. J. Periodontol. 2020, 91, 311–338. [Google Scholar] [CrossRef] [PubMed]
- Cortellini, P.; Bissada, N.F. Mucogingival conditions in the natural dentition: Narrative review, case definitions, and diagnostic considerations. J. Periodontol. 2018, 89 (Suppl. S1), 204–213. [Google Scholar] [CrossRef] [PubMed]
- Hwang, D.; Wang, H.L. Flap thickness as a predictor of root coverage: A systematic review. J. Periodontol. 2006, 77, 1625–1634. [Google Scholar] [CrossRef] [PubMed]
- Anderigg, C.K.; Metzler, D.G.; Nicole, B.K. Gingival thickness in guided tissue regeneration and associated recession at facial furcation defects. J. Periodontol. 1995, 66, 397–402. [Google Scholar] [CrossRef]
- Jung, R.; Sailer, I.; Hammerle, C.H.; Attin, T.; Schmidlin, P. In vitro color changes of the covering mucosa caused by restorative materials made of titanium and ceramic. Int. J. Periodontics Restor. Dent. 2007, 27, 251–257. [Google Scholar]
- Jung, R.; Holderegger, C.; Sailer, I.; Khraisat, A.; Suter, A.; Hammerle, C. The effect of all-ceramic and porcelan-fused-to-metal restorations on marginal peri-implant soft tissue color: A randomized controlled clinical trial. Int. J. Periodontics Restor. Dent. 2008, 28, 357–365. [Google Scholar]
- Kao, R.T.; Fagan, M.C.; Conte, G.J. Thick vs. thin gingival biotypes: A key determinant in treatment planning for dental implants. J. Calif. Dent. Assoc. 2008, 36, 193–198. [Google Scholar]
- Boke, F.; Gazioglu, C.; Akkaya, S.; Akkaya, M. Relationship between orthodontic treatment and gingival health: A retrospective study. Eur. J. Dent. 2014, 8, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Puzio, M.; Błaszczyszyn, A.; Hadzik, J.; Dominiak, M. Ultrasound assessment of soft tissue augmentation around implants in the aesthetic zone using a connective tissue graft and xenogeneic collagen matrix—1-year randomized follow-up. Ann. Anat. 2018, 217, 129–141. [Google Scholar] [CrossRef] [PubMed]
- Sönmez, G.; Kamburoğlu, K.; Gülşahı, A. Accuracy of high resolution ultrasound (US) for gingival soft tissue thickness measurement in edentulous patients prior to implant placement. Dentomaxillofac. Radiol. 2020, 30, 20200309. [Google Scholar] [CrossRef]
- Puzio, M.; Hadzik, J.; Błaszczyszyn, A.; Gedrange, T.; Dominiak, M. Soft tissue augmentation around dental implants with connective tissue graft (CTG) and xenogenic collagen matrix (XCM). 1-year randomized control trail. Ann. Anat. 2020, 230, 151484. [Google Scholar] [CrossRef] [PubMed]
- Olsson, M.; Lindhe, J. Periodontal characteristics in individuals with varying form of the upper central incisors. J. Clin. Periodontol. 1991, 18, 78–82. [Google Scholar] [CrossRef] [PubMed]
- De Rouck, T.; Eghbali, R.; Collys, K.; De Bruyn, H.; Cosyn, J. The gingival biotype revisited: Transparency of the periodontal probe through the gingival margin as a method to discriminate thin from thick gingiva. J. Clin. Periodontol. 2009, 36, 428–433. [Google Scholar] [CrossRef] [PubMed]
- Kan, J.Y.; Rungcharassaeng, K.; Umezu, K.; Kois, J.C. Dimensions of peri-implant mucosa: An evaluation of maxillary anterior single implants in humans. J. Periodontol. 2003, 74, 557–562. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, S.C.; Joly, J.C.; de Lima, A.F.M.; Tatakis, D.N. Root coverage using the coronally positioned flap with or without a subepithelial connective tissue graft. J. Periodontol. 2004, 75, 413–419. [Google Scholar] [CrossRef]
- Alpiste-Illueca, F. Dimensions of the dentogingival unit in maxillary anterior teeth: A new exploration technique (parallel profile radiograph). Int. J. Periodontics Restor. Dent. 2004, 24, 386–396. [Google Scholar]
- Bednarz, W.; Zielińska, A. Ultrasonic Biometer and its usage in an assessment of periodontal soft tissue thickness and comparison of its measurement accuracy with a bone sounding method. Dent. Med. Probl. 2011, 48, 481–489. [Google Scholar]
- Rasperini, G.; Acunzo, R.; Cannalire, P.; Farronato, K. Influence of periodontal biotype on root surface exposure during orthodontic treatment: A preliminary study. Int. J. Periodontics Restor. Dent. 2015, 35, 664–675. [Google Scholar] [CrossRef]
- Furtak, A.; Leszczyńska, E.; Sender-Janeczek, A.; Bednarz, W. The repeatability and reproducibility of gingival thickness measurement with an ultrasonic device. Dent. Med. Probl. 2018, 55, 281–288. [Google Scholar] [PubMed]
- Bednarz-Tumidajewicz, M.; Sender-Janeczek, A.; Zborowski, J.; Gedrange, T.; Konopka, T.; Prylińska-Czyżewska, A.; Dembowska, E.; Bednarz, W. An in vivo evaluation of periodontal phenotypes using cone beam computed tomography, intraoral scanning by computer aided design and prosthetic-driven implant planning. Med. Sci. Monit. 2020, 26, e924469. [Google Scholar] [CrossRef] [PubMed]
- Malpartida-Carrillo, V.; Tinedo-Lopez, P.L.; Guerrero, M.E.; Amaya-Pajares, S.P.; Özcan, M.; Rösing, C.K. Periodontal phenotype: A review of historical and current classifications evaluating different methods and characteristics. J. Esthet. Restor. Dent. 2021, 33, 432–445. [Google Scholar] [CrossRef] [PubMed]
- Kloukos, D.; Koukos, G.; Doulis, I.; Sculean, A.; Stavropoulos, A.; Katsaros, C. Gingival thickness assessmentat the mandibular incisors with four methods: A cross-sectional study. J. Periodontol. 2018, 89, 1300–1309. [Google Scholar] [CrossRef] [PubMed]
- Kakizaki, S.; Aoki, A.; Tsubokawa, M.; Lin, T.; Mizutani, K.; Koshy, G.; Sadr, A.; Oda, S.; Sumi, Y.; Izumi, Y. Observation and determination of periodontal tissue profile using optical coherence tomography. J. Periodont. Res. 2017, 53, 188–199. [Google Scholar] [CrossRef]
- Wang, G.; Le, N.M.; Hu, X.; Cheng, Y.; Jacques, S.L.; Subhash, H.; Wang, R.K. Semi-automated registration and segmentation for gingival tissue volume measurement on 3D OCT images. Biomed. Opt. Express 2020, 11, 4536–4547. [Google Scholar] [CrossRef]
- Januario, A.L.; Barriviera, M.; Duarte, W.R. Soft tissue cone-beam computed tomography: A novel method for the measurement of gingival tissue and the dimensions of the dentogingival unit. J. Esthet. Restor. Dent. 2008, 20, 366–373. [Google Scholar] [CrossRef]
- Cha, S.; Lee, S.M.; Zhang, C.; Tan, Z.; Zhao, Q. Correlation between gingival phenotype in the aesthetic zone and cranio-facial profile—A CBCT-based study. Clin. Oral Investig. 2021, 25, 1363–1374. [Google Scholar] [CrossRef]
- Cesur, E.; Orhan, K.; Misirli, M.; Bilecenoglu, B. Cone beam computed tomography evaluation of the relationship between atlantodental interval and skeletal facial morphology in adolescents. Braz. J. Otorhinolaryngol. 2019, 86, 711–719. [Google Scholar] [CrossRef]
- Borges, G.J.; Ruiz, L.F.; de Alencar, A.H.; Porto, O.C.; Estrela, C. Cone-beam computed tomography as a diagnostic method for determination of gingival thickness and distance between gingival margin and bone crest. Sci. World J. 2015, 2015, 142108. [Google Scholar] [CrossRef]
- Nikiforidou, M.; Tsalikis, L.; Angelopoulos, C.; Menexes, G.; Vouros, I.; Konstantinides, A. Classification of periodontal biotypes with the use of CBCT: A cross-sectional study. Clin. Oral. Investig. 2016, 20, 2061–2071. [Google Scholar] [CrossRef] [PubMed]
- Amid, R.; Mirakhori, M.; Safi, Y.; Kadkhodazadeh, M.; Namdari, M. Assessment of gingival biotype and facial hard/soft tissue dimensions in the maxillary anterior teeth region using cone beam computed tomography. Arch. Oral. Biol. 2017, 79, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Huber, S.; Zeltner, M.; Hämmerle, C.H.F.; Jung, R.E.; Thoma, D.S. Non-interventional 1-year follow-up study of peri-implant soft tissues following previous soft tissue augmentation and crown insertion in single-tooth gaps. J. Clin. Periodontol. 2018, 45, 504–512. [Google Scholar] [CrossRef] [PubMed]
- Rojo, E.; Stroppa, G.; Sanz-Martin, I.; Gonzalez-Martín, O.; Santos Alemany, A.; Nart, J. Soft tissue volume gain around dental implants using autogenous subepithelial connective tissue grafts harvested from the lateral palate or tuberosity area: A randomized controlled clinical study. J. Clin. Periodontol. 2018, 45, 495–503. [Google Scholar] [CrossRef]
- Couso-Queiruga, E.; Tattan, M.; Ahmad, U.; Barwacz, C.; Gonzalez-Martin, O.; Avila-Ortiz, G. Assessment of gingival thickness using digital file superimposition versus direct clinical measurements. Clin. Oral. Investig. 2020, 25, 2353–2361. [Google Scholar] [CrossRef]
- Fons-Badal, C.; Alonso Pérez-Barquero, J.; Martínez- Martínez, N.; Faus-López, J.; Fons-Font, A.; Agustín-Panadero, R. A novel, fully digital approach to quantifying volume gain after soft tissue graft surgery. A pilot study. J. Clin. Periodontol. 2020, 47, 614–620. [Google Scholar] [CrossRef]
- Tattan, M.; Sinjab, K.; Lee, E.; Arnett, M.; Oh, T.-J.; Wang, H.-L.; Chan, H.-L.; Kripfgans, O.D. Ultrasonography for chairside evaluation of periodontal structures: A pilot study. J. Periodontol. 2020, 91, 890–899. [Google Scholar] [CrossRef]
- Ronay, V.; Sahrmann, P.; Bindl, A.; Attin, T.; Schmidlin, P.R. Curent status and perspectives of mucogingival soft thissue measurement methods. J. Esthet. Restor. Dent. 2011, 23, 146–156. [Google Scholar] [CrossRef]
- Gánti, B.; Bednarz, W.; Kőműves, K.; Vág, J. Reproducibility of the PIROP ultrasonic biometer for gingival thickness measurements. J. Esthet. Restor. Dent. 2018, 31, 263–267. [Google Scholar] [CrossRef]
- Kloukos, D.; Kakali, L.; Koukos, G.; Sculean, A.; Stavropoulos, A.; Katsaros, C. Labial gingival thickness assessment at mandibular incisors of orthodontic patients with ultrasound and cone-beam ct: A cross-sectional study. ResearchSquare, 2020; preprint. [Google Scholar] [CrossRef]
- Gürlek, Ö.; Sönmez, Ş.; Güneri, P.; Nizam, N. A novel soft tissue thickness measuring method using cone beam computed tomography. J. Esthet. Restor. Dent. 2018, 30, 516–522. [Google Scholar] [CrossRef] [PubMed]
- Zucchelli, G.; Mele, M.; Stefanini, M.; Mazzotti, C.; Marzadori, M.; Montebugnoli, L.; de Sanctis, M. Patient morbidity and root coverage outcome after subepithelial connective tissue and de-epithelialized grafts: A comparative randomized-controlled clinical trial. J. Clin. Periodontol. 2010, 37, 728–738. [Google Scholar] [CrossRef] [PubMed]
- Müller, H.P.; Schaller, N.; Eger, T.; Heinecke, A. Thickness of masticatory mucosa. J. Clin. Periodontol. 2000, 27, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Shah, R.; Sowmya, N.K.; Mehta, D.S. Prevalence of gingival biotype and its relationship to clinical parameters. Contemp. Clin. Dent. 2015, 6, 167–171. [Google Scholar] [CrossRef] [PubMed]
- La Rocca, A.; Alemany, A.; Levi, P., Jr.; Juan, M.; Molina, J.; Weisgold, A. Anterior maxillary and mandibular biotype: Relationship between gingival thickness and width with respect to underlying bone thickness. Implant Dent. 2012, 21, 507–515. [Google Scholar] [CrossRef]
- Cairo, F.; Cortellini, P.; Pilloni, A.; Nieri, M.; Cincinelli, S.; Amunni, F.; Pagavino, G.; Tonetti, M.S. Clinical efficacy of coronally advanced flap with or without connective tissue graft for the treatment of multiple adjacent gingival recessions in the aesthetic area: A randomized controlled clinical trial. J. Clin. Periodontol. 2016, 43, 849–856. [Google Scholar] [CrossRef] [PubMed]
- Tavelli, L.; Barootchi, S.; Greenwell, H.; Wang, H.L. Is a soft tissue graft harvested from the maxillary tuberosity the approach of choice in an isolated site? J. Periodontol. 2019, 90, 821–825. [Google Scholar] [CrossRef] [PubMed]
- Claffey, N.; Shanley, D. Relationship of gingival thickness and bleeding to loss of probing attachment in shallow sites following nonsurgical periodontal therapy. J. Clin. Periodontol. 1986, 13, 654–657. [Google Scholar] [CrossRef]
- Pietruska, M.; Skurska, A.; Podlewski, Ł.; Milewski, R.; Pietruski, J. Clinical evaluation of Miller class I and II recessions treatment with the use of modified coronally advanced tunne ltechnique with either collagen matrix or subepithelial connective tissue graft: A randomized clinical study. J. Clin. Periodontol. 2019, 46, 86–95. [Google Scholar] [CrossRef]
- Stein, J.; Lintel-Höping, N.; Hammächer, C.; Kasaj, A.; Tamm, M.; Hanisch, O. The gingival biotype: Measurement of soft and hard tissue dimensions-a radiographic morphometric study. J. Clin. Periodontol. 2013, 40, 1132–1139. [Google Scholar] [CrossRef]
- Eghbali, A.; De Bruyn, H.; Cosyn, J.; Kerckaert, I.; Van Hoof, T. Ultrasonic assessment of mucosal thickness around implants: Validity, reproducibility, and stability of connective tissue grafts atthe buccal aspect. Clin. Implant Dent. Relat. Res. 2016, 18, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Belák, S.; Žižka, R.; Starosta, M.; Zapletalová, J.; Šedý, J.; Štefanatný, M. The influence of gingival phenotype on the morphology of the maxillary central papilla. BMC Oral Health 2021, 21, 43. [Google Scholar] [CrossRef] [PubMed]
- Gkogkos, A.; Kloukos, D.; Koukos, G.; Liapis, G.; Sculaen, A.; Katsaros, C. Clinical and radiographic gingival thickness assessment at mandibular incisors: An ex vivo study. Oral. Health Prev. Dent. 2020, 18, 607–617. [Google Scholar] [CrossRef] [PubMed]
- Kus-Bartoszek, A.; Lipski, M.; Safranow, K.; Drozdzik, A. The attached gingiva thickness in the mandibular anterior region during the early transitional dentition phase. Quintessence Int. 2021, 220–227. [Google Scholar] [CrossRef]
- Sun, M.; Liu, X.; Xia, T.; Meng, H. Non-invasive evaluation of labial gingival and alveolar crest thickness in the maxillary anterior teeth region by 15-MHz B-mode ultrasonography. BMC Oral Health 2021, 21, 10. [Google Scholar] [CrossRef] [PubMed]
- Zimbran, A.; Dudea, A.; Dudea, D. Evaluation of periodontal tissues using 40MHz ultrasonography. Preliminary report. Med. Ultrason. 2013, 15, 6–9. [Google Scholar] [CrossRef]
- Izzetti, R.; Vitali, S.; Aringhieri, G.; Oranges, T.; Dini, V.; Nisi, M.; Graziani, F.; Gabriele, M.; Caramella, D. Discovering a new anatomy: Exploration of oral mucosa with ultra-high frequency ultrasound. Dentomaxillofac. Radiol. 2020, 49, 20190318. [Google Scholar] [CrossRef] [PubMed]
- Nowzari, H.; Molayem, S.; Chiu, C.H.; Rich, S.K. Cone beam computed tomographic measurement of maxillary central incisors to determine prevalence of facial alveolar bone width ³2 mm. Clin. Implant Dent. Relat. Res. 2012, 14, 595–602. [Google Scholar] [CrossRef]
- Temple, K.E.; Schoolfield, J.; Noujeim, M.E.; Huynh-Ba, G.; Lasho, D.J.; Mealey, B.L. A cone beam computed tomography (CBCT) study of buccal plate thickness of the maxillary and mandibular posterior dentition. Clin. Oral. Implant Res. 2016, 27, 1072–1078. [Google Scholar] [CrossRef]
- Tolentino, E.; Yamashita, F.C.; de Albuquerque, S.; Walewski, L.A.; Iwaki, L.C.V.; Takeshita, W.M.; Silva, M.C. Reliability and accuracy of linear measurements in cone-beam computed tomography using different software programs and voxel sizes. J. Conserv. Dent. 2018, 21, 607–612. [Google Scholar] [CrossRef]
- Erozan, Ç.; Ozan, O. Evaluation of the precision of different intraoral scanner-Computer Aided Design (CAD) software combinations in digital dentistry. Med. Sci. Monit. 2020, 26, e918529. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.-W.; Hwang, H.-S.; Cho, I.-S.; Baek, S.H.; Cho, J.H. Registration accuracy between intraoral scanned and cone-beam computed tomography-scanned crowns in various registration methods. Am. J. Orthod. Dentofacial. Orthop. 2020, 157, 348–356. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-S.; Jeon, Y.-S.; Strauss, F.-J.; Jung, H.-I.; Gruber, R. Digital scanning is more accurate than using a periodontal probe to measure the keratinized tissue width. Sci. Rep. 2020, 10, 3665. [Google Scholar] [CrossRef] [PubMed]
- Zweers, J.; Thomas, R.Z.; Slot, D.E.; Weisgold, A.S.; Van der Weijden, F.G. Characteristics of periodontal biotype, its dimensions, associations and prevalence: A systematic review. J. Clin. Periodontol. 2014, 41, 958–971. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | n | Mean | Median | Minimum | Maximum | Lower Quartile | Upper Quartile | SD |
|---|---|---|---|---|---|---|---|---|
| FGTu | 180 | 0.98 | 0.95 | 0.43 | 1.63 | 0.83 | 1.10 | 0.23 |
| SGTu | 180 | 1.11 | 1.11 | 0.60 | 1.90 | 0.92 | 1.30 | 0.25 |
| CGTu | 180 | 0.69 | 0.69 | 0.32 | 1.36 | 0.59 | 0.76 | 0.16 |
| FGTt | 180 | 0.81 | 0.80 | 0.50 | 1.90 | 0.70 | 0.90 | 0.18 |
| SGTt | 180 | 1.57 | 1.56 | 0.63 | 2.45 | 1.38 | 1.74 | 0.31 |
| CGTt | 180 | 0.88 | 0.90 | 0.30 | 1.70 | 0.70 | 1.00 | 0.24 |
| PD | 180 | 1.23 | 1.00 | 1.00 | 2.00 | 1.00 | 1.38 | 0.38 |
| CAL | 180 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 |
| WKT | 180 | 5.37 | 5.25 | 2.00 | 8.50 | 4.00 | 6.38 | 1.28 |
| Variables | Bias | −95% CI | 95% CI | SD | −95% LOA | 95% LOA | % Agreement | p |
|---|---|---|---|---|---|---|---|---|
| FGTu | 0.00 | 0.00 | 0.01 | 0.03 | −0.05 | 0.06 | 95.00 | 0.032 |
| SGTu | 0.00 | −0.00 | 0.01 | 0.03 | −0.06 | 0.06 | 95.00 | 0.073 |
| CGTu | −0.01 | −0.01 | −0.00 | 0.03 | −0.06 | 0.05 | 98.90 | 0.036 |
| FGTt | 0.00 | −0.00 | 0.00 | 0.03 | −0.05 | 0.05 | 92.80 | 0.782 |
| SGTt | 0.04 | 0.03 | 0.05 | 0.08 | −0.12 | 0.20 | 100.00 | 0.000 |
| CGTt | −0.00 | −0.01 | 0.00 | 0.04 | −0.08 | 0.07 | 85.60 | 0.240 |
| PD | 0.00 | −0.04 | 0.04 | 0.28 | −0.55 | 0.55 | 92.20 | 0.999 |
| CAL | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 100.00 | 1.000 |
| WKT | −0.04 | −0.09 | 0.02 | 0.39 | −0.79 | 0.71 | 85.00 | 0.179 |
| Variables | Bias | −95% CI | 95% CI | SD | −95% LOA | 95% LOA | % Agreement | p |
|---|---|---|---|---|---|---|---|---|
| FGTu | 0.00 | −0.00 | 0.01 | 0.03 | −0.07 | 0.07 | 96.70 | 0.771 |
| SGTu | 0.19 | 0.15 | 0.25 | 0.35 | −0.50 | 0.89 | 95.00 | 0.000 |
| CGTu | 0.00 | −0.00 | 0.01 | 0.04 | −0.07 | 0.07 | 97.80 | 0.938 |
| FGTt | −0.00 | −0.03 | 0.02 | 0.15 | −0.29 | 0.29 | 90.60 | 0.957 |
| SGTt | 0.01 | −0.00 | 0.01 | 0.06 | −0.12 | 0.13 | 100.00 | 0.192 |
| CGTt | −0.00 | −0.01 | 0.00 | 0.04 | −0.09 | 0.08 | 80.60 | 0.128 |
| PD | 0.00 | −0.02 | 0.03 | 0.17 | −0.32 | 0.33 | 97.20 | 0.656 |
| CAL | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 100.00 | 1.000 |
| WKT | 0.01 | −0.03 | 0.05 | 0.26 | −0.49 | 0.52 | 93.30 | 0.565 |
| Variables | Bias | −95% CI | 95% CI | SD | −95% LOA | 95% LOA | % of Agreement | p |
|---|---|---|---|---|---|---|---|---|
| FGTu | −0.01 | −0.01 | −0.00 | 0.04 | −0.08 | 0.07 | 98.30 | 0.007 |
| SGTu | −0.08 | −0.10 | −0.05 | 0.19 | −0.44 | 0.29 | 95.00 | 0.000 |
| CGTu | 0.02 | 0.01 | 0.02 | 0.03 | −0.04 | 0.08 | 96.10 | 0.000 |
| FGTt | 0.01 | −0.00 | 0.02 | 0.07 | −0.14 | 0.15 | 92.80 | 0.201 |
| SGTt | 0.01 | 0.00 | 0.02 | 0.06 | −0.11 | 0.13 | 95.60 | 0.006 |
| CGTt | 0.00 | −0.00 | 0.01 | 0.03 | −0.06 | 0.06 | 96.10 | 0.537 |
| PD | −0.01 | −0.05 | 0.03 | 0.26 | −0.52 | 0.50 | 95.60 | 0.669 |
| CAL | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 100.00 | 1.000 |
| WKT | 0.18 | 0.10 | 0.26 | 0.54 | −0.88 | 1.24 | 92.20 | 0.000 |
| Ultrasound Method | CBCT/CAD/PDIP | Bias | −95% CI | 95% CI | SD | −95% LOA | 95% LOA | % Agreement | p |
|---|---|---|---|---|---|---|---|---|---|
| FGTu | FGTt | 0.17 | 0.13 | 0.21 | 0.25 | −0.33 | 0.66 | 93.30 | 0.000 |
| SGTu | SGTt | −0.45 | −0.50 | −0.41 | 0.32 | −1.08 | 0.17 | 95.00 | 0.000 |
| CGTu | CGTt | −0.19 | −0.22 | −0.15 | 0.25 | −0.68 | 0.30 | 95.60 | 0.000 |
| Gingival Phenotype | Variables | N | Thin GP | Thin GP/Medium GP p | N | Medium GP | Medium GP/Thick GP p | N | Thick GP | Thin GP/Thick GP p |
|---|---|---|---|---|---|---|---|---|---|---|
| Acc to FGTu | FGTu | 21 | 0.67 (0.60 ÷ 0.69) | 84 | 0.88 ± 0.07 0.89 (0.82 ÷ 0.94) | 75 | 1.19 ± 0.17 1.13 (1.06 ÷ 1.35) | |||
| SGTu | 21 | 0.85 (0.72 ÷ 1.00) | 0.000 * | 84 | 1.10 ± 0.23 1.12 (0.93 ÷ 1.27) | 0.000 * | 75 | 1.20 ± 0.25 1.23 (0.98 ÷ 1.37) | 0.009 * | |
| CGTu | 21 | 0.59 (0.47 ÷ 0.72) | 0.013 * | 84 | 0.70 ± 0.16 0.69 (0.61 ÷ 0.76) | 0.009 * | 75 | 0.70 ± 0.15 0.71 (0.62 ÷ 0.77) | 0.823 | |
| WKT | 21 | 5.00 (4.00 ÷ 6.25) | 0.759 | 84 | 5.36 ± 1.26 5.25 (4.00 ÷ 6.25) | 0.712 | 75 | 5.40 ± 1.31 5.25 (4.00 ÷ 6.50) | 0.858 | |
| Acc to SGTu | FGTu | 8 | 0.69 (0.62 ÷ 0.88) | 0.012 * | 58 | 0.96 ± 0.24 0.92 (0.82 ÷ 1.88) | 0.145 | 114 | 1.01 ± 0.22 0.98 (0.86 ÷ 1.12) | 0.001 * |
| SGTu | 8 | 0.65 (0.64 ÷ 0.66) | 58 | 0.87 ± 0.08 0.88 (0.80 ÷ 0.95) | 114 | 1.26 ± 0.16 1.27 (1.14 ÷ 1.37) | ||||
| CGTu | 8 | 0.55 (0.41 ÷ 0.66) | 0.125 | 58 | 0.62 ± 0.14 0.63 (0.52 ÷ 0.72) | 0.000 ** | 114 | 0.74 ± 0.15 0.73 (0.64 ÷ 0.81) | 0.001 * | |
| WKT | 8 | 4.50 (3.50 ÷ 6.50) | 0.870 | 58 | 4.92 ± 1.22 5.00 (4.00 ÷ 5.75) | 0.000 ** | 114 | 5.62 ± 1.22 6.00 (5.00 ÷ 6.50) | 0.245 | |
| Acc to FGTt | FGTt | 65 | 0.65 ± 0.06 0.70 (0.60 ÷ 0.70) | 101 | 0.85 ± 0.08 0.82 (0.80 ÷ 0.90) | 14 | 1.19 (1.10 ÷ 1.23) | |||
| SGTt | 65 | 1.37 ± 0.25 1.38 (1.25 ÷ 1.58) | 0.000 ** | 101 | 1.63 ± 0.26 1.58 (1.45 ÷ 1.80) | 0.000 * | 14 | 1.96 (1.80 ÷ 2.23) | 0.000 * | |
| CGTt | 65 | 0.80 ± 0.22 0.80 (0.67 ÷ 0.92) | 0.009 ** | 101 | 0.90 ± 0.25 0.90 (0.70 ÷ 1.00) | 0.004 * | 14 | 1.09 (0.90 ÷ 1.25) | 0.000 * | |
| WKT | 65 | 4.95 ± 1.23 5.00 (4.00 ÷ 6.00) | 0.009 ** | 101 | 5.48 ± 1.26 5.25 (4.25 ÷ 6.50) | 0.005 * | 14 | 6.50 (6.00 ÷ 7.00) | 0.000 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bednarz-Tumidajewicz, M.; Furtak, A.; Zakrzewska, A.; Rąpała, M.; Gerreth, K.; Gedrange, T.; Bednarz, W. Comparison of the Effectiveness of the Ultrasonic Method and Cone-Beam Computed Tomography Combined with Intraoral Scanning and Prosthetic-Driven Implant Planning Method in Determining the Gingival Phenotype in the Healthy Periodontium. Int. J. Environ. Res. Public Health 2022, 19, 12276. https://doi.org/10.3390/ijerph191912276
Bednarz-Tumidajewicz M, Furtak A, Zakrzewska A, Rąpała M, Gerreth K, Gedrange T, Bednarz W. Comparison of the Effectiveness of the Ultrasonic Method and Cone-Beam Computed Tomography Combined with Intraoral Scanning and Prosthetic-Driven Implant Planning Method in Determining the Gingival Phenotype in the Healthy Periodontium. International Journal of Environmental Research and Public Health. 2022; 19(19):12276. https://doi.org/10.3390/ijerph191912276
Chicago/Turabian StyleBednarz-Tumidajewicz, Magdalena, Aneta Furtak, Aneta Zakrzewska, Małgorzata Rąpała, Karolina Gerreth, Tomasz Gedrange, and Wojciech Bednarz. 2022. "Comparison of the Effectiveness of the Ultrasonic Method and Cone-Beam Computed Tomography Combined with Intraoral Scanning and Prosthetic-Driven Implant Planning Method in Determining the Gingival Phenotype in the Healthy Periodontium" International Journal of Environmental Research and Public Health 19, no. 19: 12276. https://doi.org/10.3390/ijerph191912276
APA StyleBednarz-Tumidajewicz, M., Furtak, A., Zakrzewska, A., Rąpała, M., Gerreth, K., Gedrange, T., & Bednarz, W. (2022). Comparison of the Effectiveness of the Ultrasonic Method and Cone-Beam Computed Tomography Combined with Intraoral Scanning and Prosthetic-Driven Implant Planning Method in Determining the Gingival Phenotype in the Healthy Periodontium. International Journal of Environmental Research and Public Health, 19(19), 12276. https://doi.org/10.3390/ijerph191912276