
Quality of Life in Yoga Practitioners—Research Conducted on a Population of Polish Yogis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Procedure
2.3. Instruments
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Iyengar, B.K.S. Light on Yoga; Virya: Warszawa, Poland, 2011. [Google Scholar]
- De Michaelis, E.A. History of Modern Yoga; Continuum International Publishing Group: London, UK, 2005. [Google Scholar]
- Michalsen, A.; Kessler, C. Science-based yoga—stretching mind, body, and soul. Forsch. Komplementmed. 2013, 20, 176–178. [Google Scholar] [CrossRef]
- Cramer, H.; Lauche, R.; Dobos, G. Characteristics of randomized controlled trials of yoga: A bibliometric analysis. BMC Complementary Altern. Med. 2014, 2, 328. [Google Scholar] [CrossRef] [PubMed]
- Social Diagnosis 2011. Objective and Subjective Quality of Life in Poland. Available online: http://www.diagnoza.com/pliki/raporty/Diagnoza_raport_2011.pdf (accessed on 20 July 2018).
- Social Diagnosis 2015. Objective and Subjective Quality of Life in Poland. Available online: http://www.diagnoza.com/pliki/raporty/Diagnoza_raport_2015.pdf (accessed on 20 July 2018).
- Yoga Magazine. Available online: https://yoga-mag.pl/kto-w-polsce-cwiczy-joge-badania-jogi-w-polsce-2016/ (accessed on 28 July 2018).
- Kelley, G.A.; Kelley, K.S. Yoga, Health-Related Quality of Life and Mental Well-Being: A Re-analysis of a Meta-analysis using the Quality Effects Model. J. Gerontol. 2020, 16, 1732–1736. [Google Scholar] [CrossRef] [PubMed]
- El-Hashimi, D.; Gorey, K.M. Yoga-Specific Enhancement of Quality of Life Among Women with Breast Cancer: Systematic Review and Exploratory Meta-Analysis of Randomized Controlled Trials. J. Evid.-Based Integr. Med. 2019, 24, 2515690X19828325. [Google Scholar] [CrossRef] [PubMed]
- Tulloch, A.; Bombell, H.; Dean, C.; Tiedemann, A. Yoga-based exercise improves health-related quality of life and mental well-being in older people: A systematic review of randomised controlled trials. Age Ageing 2018, 1, 537–544. [Google Scholar] [CrossRef]
- Jin, X.; Wang, L.; Liu, S.; Zhu, L.; Loprinzi, P.D.; Fan, X. The Impact of Mind-body Exercises on Motor Function, Depressive Symptoms, and Quality of Life in Parkinson’s Disease: A Systematic Review and Meta-analysis. Int. J. Environ. Res. Public Health 2019, 18, 31. [Google Scholar] [CrossRef]
- Joga Akademicka. Available online: https://jogaakademicka.pl/ (accessed on 15 August 2018).
- World Health Organization. WHOQOL-BREF. Introduction, Administration, Scoring and Generic Version of Assessment; World Health Organization: Geneva, Switzerland, 1996.
- Cieślik, B.; Podbielska, H. Przegląd wybranych kwestionariuszy oceny jakości życia. Inżynieria Biomed. 2015, 21, 102–135. [Google Scholar]
- Yadav, R.; Yadav, R.K.; Pandey, R.M.; Kochar, K.P. Effect of a Short-Term Yoga-Based Lifestyle Intervention on Health-Related Quality of Life in Overweight and Obese Subjects. J. Altern. Complement. Med. 2016, 22, 443–449. [Google Scholar] [CrossRef]
- Hariprasad, V.R.; Sivakumar, P.T.; Koparde, V.; Varambally, S.; Thirthalli, J.; Varghese, M.; Basavaraddi, I.V.; Gangadhar, B.N. Effects of yoga intervention on sleep and quality-of-life in elderly: A randomized controlled trial. Indian J. Psychiatry 2013, 55 (Suppl. 3), S364–S368. [Google Scholar]
- Jyotsna, V.P.; Joshi, A.; Ambekar, S.; Kumar, N.; Dhawan, A.; Sreenivas, V. Comprehensive yogic breathing program improves quality of life in patients with diabetes. Indian J. Endocrinol. Metab. 2012, 16, 423–428. [Google Scholar] [CrossRef]
- Andysz, A.; Merecz, D.; Wójcik, A.; Świątkowska, B.; Sierocka, K.; Najder, A. Effect of a 10-week yoga programme on the quality of life of woman after breast cancer surgery. Przegląd Menopauzalny 2014, 13, 186–193. [Google Scholar] [PubMed]
- Rakhshani, A.; Maharana, S.; Raghuram, N.; Nagendra, H.R.; Venkatram, P. Effects of integrated yoga on quality of life and interpersonal relationship of pregnant women. Qual. Life Res. 2010, 19, 1447–1455. [Google Scholar] [CrossRef] [PubMed]
- Nayak, G.; Kamath, A.; Kumar, P.N.; Rao, A. Effect of yoga therapy on physical and psychological quality of life of perimenopausal women in selected coastal areas of Karnataka, India. J. Mid-Life Health 2014, 5, 180–185. [Google Scholar]
- Bankar, M.A.; Chaudhari, S.K.; Chaudhari, K.D. Impact of long term Yoga practice on sleep quality and quality of life in the elderly. J. Ayurveda Integr. Med. 2013, 4, 28–32. [Google Scholar] [CrossRef] [PubMed]
- Garg, S.; Ramya, C.S.; Shankar, V.; Kutty, K. Efficacy of short-term Yoga therapy program on quality of life in patients with psychosomatic ailments. Indian J. Psychiatry 2015, 57, 78–80. [Google Scholar] [CrossRef] [PubMed]
- Yoga in Australia: Results of a National Survey 2008. Available online: https://researchbank.rmit.edu.au/eserv/rmit:6110/Penman.pdf (accessed on 16 September 2018).
- Sohl, S.J.; Wallston, K.A.; Watkins, K.; Birdee, G.S. Yoga for Risk Reduction of Metabolic Syndrome: Patient-Reported Outcomes from a Randomized Controlled Pilot Study. Evid.-Based Complement. Altern. Med. 2016, 2016, 3094589. [Google Scholar] [CrossRef]
- Cramer, H.; Lauche, R.; Langhorst, J.; Dobos, G.; Paul, A. Quality of life and mental health in patients with chronic diseases who regularly practice yoga and those who do not: A case-control study. Evid.-Based Complement. Altern. Med. 2013, 2013, 702914. [Google Scholar] [CrossRef]
- Viscegalia, E.; Lewis, S. Yoga therapy as an adjunctive treatment for schizophrenia: A randomized, controlled pilot study. J. Altern. Complement. Med. 2011, 17, 601–607. [Google Scholar] [CrossRef]
- Rahmani, S.; Zahirrodin, A.; Moradi, M.; Hoveida, S.; Nejat, S. Examining the effectiveness of Mindfulness-based Stress Reduction Program and Conscious Yoga on quality of life in patients with diabetes type 2. Iran. J. Diabetes Obes. 2014, 6, 168–175. [Google Scholar]
- Wolff, M.; Sundquist, K.; Lönn, L.S.; Midlöv, P. Impact of yoga on blood pressure and quality of life in patients with hypertension—A controlled trial in primary care, matched for systolic blood pressure. BMC Cardiovasc. Disord. 2013, 13, 111. [Google Scholar] [CrossRef]
- Jorge, M.P.; Santaella, D.F.; Pontes, I.M.; Shiramizu, V.K.; Nascimento, E.B.; Cabral, A.; Lemos, T.M.; Silva, R.H.; Ribeiro, A.M. Hatha Yoga practice decreases menopause symptoms and improves quality of life: A randomized controlled trial. Complement. Ther. Med. 2016, 26, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Birdee, G.S.; Ayala, S.G.; Wallston, K.A. Cross-sectional analysis of health-related quality of life and elements of yoga practice. BMC Complement. Altern. Med. 2017, 17, 83. [Google Scholar] [CrossRef] [PubMed]
- Hewett, Z.L.; Pumpa, K.L.; Smith, C.A.; Fahey, P.P.; Cheema, B.S. Effect of a 16-week Bikram yoga program on perceived stress, self-efficacy and health-related quality of life in stressed and sedentary adults: A randomised controlled trial. J. Sci. Med. Sport 2018, 21, 352–357. [Google Scholar] [CrossRef] [PubMed]
- Byrka, K. Łańcuchowe Zmiany Zachowań w Kontekście Ochrony Środowiska i Promocji Zdrowia; Wydawnictwo Naukowe PWN: Warszawa, Poland, 2015. [Google Scholar]
- Birdee, G.S.; Sohl, S.J.; Wallston, K. Development and psychometric properties of the yoga self-efficacy scale (YSES). BMC Complement. Altern. Med. 2016, 6, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | SG | CG | p | |||
|---|---|---|---|---|---|---|
| N | % | N | % | |||
| Sex | Female | 124 | 82.7 | 124 | 82.7 | 1.000 a |
| Male | 26 | 17.3 | 26 | 17.3 | ||
| Total | 150 | 100.0 | 150 | 100.0 | ||
| Age | M | 42.53 | 41.43 | 0.053 b | ||
| SD | 4.697 | 4.729 | ||||
| Me | 43.0 | 40.0 | ||||
| Min | 35.0 | 31.0 | ||||
| Max | 50.0 | 51.0 | ||||
| Q1 | 38.0 | 37.0 | ||||
| Q3 | 46.0 | 45.0 | ||||
| Family status | Married | 105 | 70.0 | 122 | 81.3 | 0.057 a |
| Cohabitation | 17 | 11.3 | 13 | 8.7 | ||
| Single | 28 | 18.7 | 15 | 10.0 | ||
| Total | 150 | 100.0 | 150 | 100.0 | ||
| Place of residence | Village | 18 | 12.0 | 32 | 21.3 | 0.057 a |
| City with a population under 10,000 | 4 | 2.7 | 10 | 6.7 | ||
| City with a population between 10,000 to 50,000 | 13 | 8.7 | 11 | 7.3 | ||
| City with population between 50,000 to 100,000 | 10 | 6.7 | 5 | 3.3 | ||
| City with a population above 100,000 | 105 | 70.0 | 92 | 61.3 | ||
| Total | 150 | 100.0 | 150 | 100.0 | ||
| Group | Test Result | ||||
|---|---|---|---|---|---|
| Study Group | Control Group | ||||
| Education | Higher | N | 127 | 101 | χ2 = 11.422 df = 1 p = 0.001 |
| % | 84.7 | 67.3 | |||
| Other than higher | N | 23 | 49 | ||
| % | 15.3 | 32.7 | |||
| Total | N | 150 | 150 | ||
| % | 100.0 | 100.0 | |||
| WHOQOL 1 | WHOQOL 2 | WHOQOL 3 | WHOQOL 4 | WHOQOL 5 | WHOQOL 6 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SG | CG | SG | CG | SG | CG | SG | CG | SG | CG | SG | CG | |
| M | 16.99 | 15.74 | 15.01 | 14.03 | 15.29 | 15.31 | 15.20 | 14.21 | 4.15 | 3.97 | 4.03 | 3.70 |
| SD | 1.85 | 2.32 | 2.17 | 2.41 | 2.85 | 2.73 | 1.81 | 2.04 | 0.62 | 0.68 | 0.64 | 0.89 |
| Min | 10.86 | 8.57 | 9.33 | 8.00 | 5.33 | 8.00 | 9.50 | 8.00 | 2.00 | 1.00 | 2.00 | 1.00 |
| Max | 20.00 | 20.00 | 20.00 | 20.00 | 20.00 | 20.00 | 19.00 | 19.50 | 5.00 | 5.00 | 5.00 | 5.00 |
| Q25 | 16.00 | 14.29 | 14.00 | 12.00 | 13.33 | 13.33 | 14.00 | 13.00 | 4.00 | 4.00 | 4.00 | 3.00 |
| Me | 17.14 | 15.71 | 15.33 | 14.00 | 16.00 | 16.00 | 15.50 | 14.00 | 4.00 | 4.00 | 4.00 | 4.00 |
| Q75 | 18.29 | 17.14 | 16.67 | 15.33 | 17.33 | 17.33 | 16.50 | 15.50 | 5.00 | 4.00 | 4.00 | 4.00 |
| U | 7579.00 | 8554.00 | 11141.50 | 7919.50 | 9794.50 | 9194.50 | ||||||
| p | <0.001 * | <0.001 * | 0.884 | <0.001 * | 0.023 * | 0.002 * | ||||||
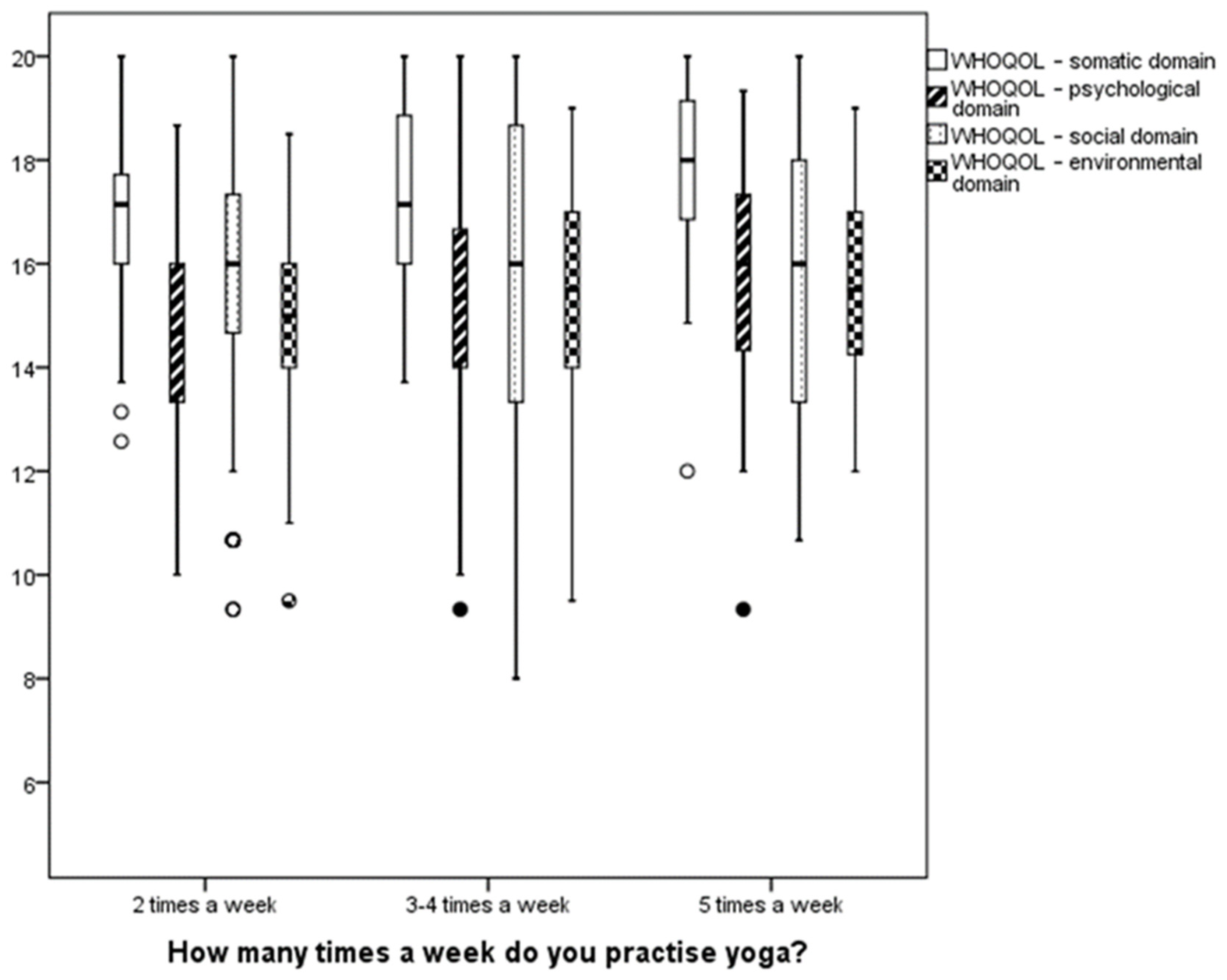
| Scale | Test Result |
|---|---|
| WHOQOL 1 | χ2 = 9.957 df = 4 p = 0.041 * |
| WHOQOL 2 | χ2 = 9.636 df = 4 p = 0.047 * |
| WHOQOL 3 | χ2 = 11.129 df = 4 p = 0.025 * |
| WHOQOL 4 | χ2 = 4.153 df = 4 p = 0.386 |
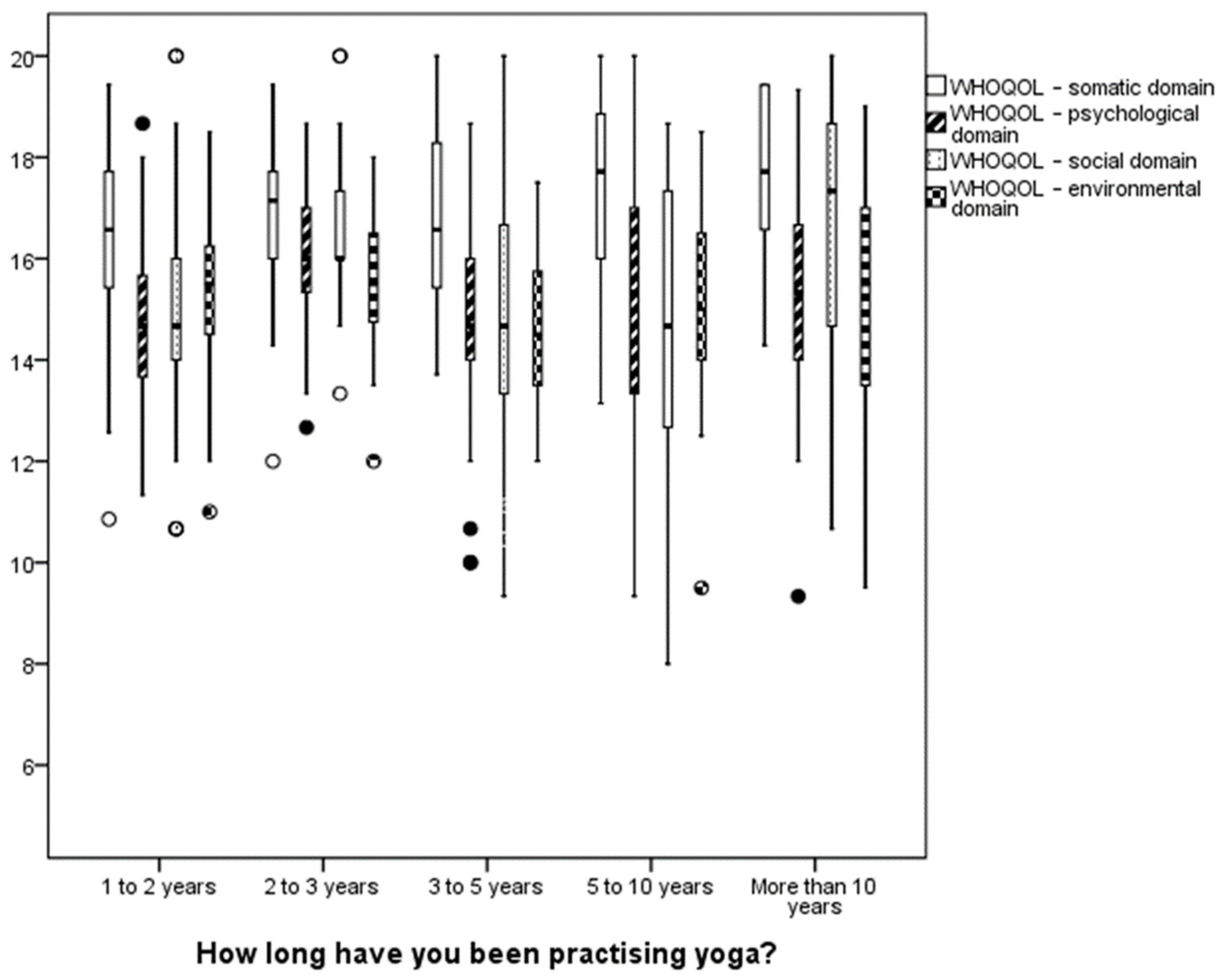
| Scale | Test Result |
|---|---|
| WHOQOL 1 | χ2 = 5.886 df = 2 p = 0.053 |
| WHOQOL 2 | χ2 = 4.484 df = 2 p = 0.106 |
| WHOQOL 3 | χ2 = 1.053 df = 2 p = 0.591 |
| WHOQOL 4 | χ2 = 1.407 df = 2 p = 0.495 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piekorz, Z.; Radzimińska, A.; Lewandowski, A.; Ossowski, R. Quality of Life in Yoga Practitioners—Research Conducted on a Population of Polish Yogis. Int. J. Environ. Res. Public Health 2022, 19, 12023. https://doi.org/10.3390/ijerph191912023
Piekorz Z, Radzimińska A, Lewandowski A, Ossowski R. Quality of Life in Yoga Practitioners—Research Conducted on a Population of Polish Yogis. International Journal of Environmental Research and Public Health. 2022; 19(19):12023. https://doi.org/10.3390/ijerph191912023
Chicago/Turabian StylePiekorz, Zuzanna, Agnieszka Radzimińska, Andrzej Lewandowski, and Roman Ossowski. 2022. "Quality of Life in Yoga Practitioners—Research Conducted on a Population of Polish Yogis" International Journal of Environmental Research and Public Health 19, no. 19: 12023. https://doi.org/10.3390/ijerph191912023
APA StylePiekorz, Z., Radzimińska, A., Lewandowski, A., & Ossowski, R. (2022). Quality of Life in Yoga Practitioners—Research Conducted on a Population of Polish Yogis. International Journal of Environmental Research and Public Health, 19(19), 12023. https://doi.org/10.3390/ijerph191912023