
Disease-Specific Knowledge, Physical Activity, and Physical Functioning Examination among Patients with Chronic Non-Specific Low Back Pain


 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
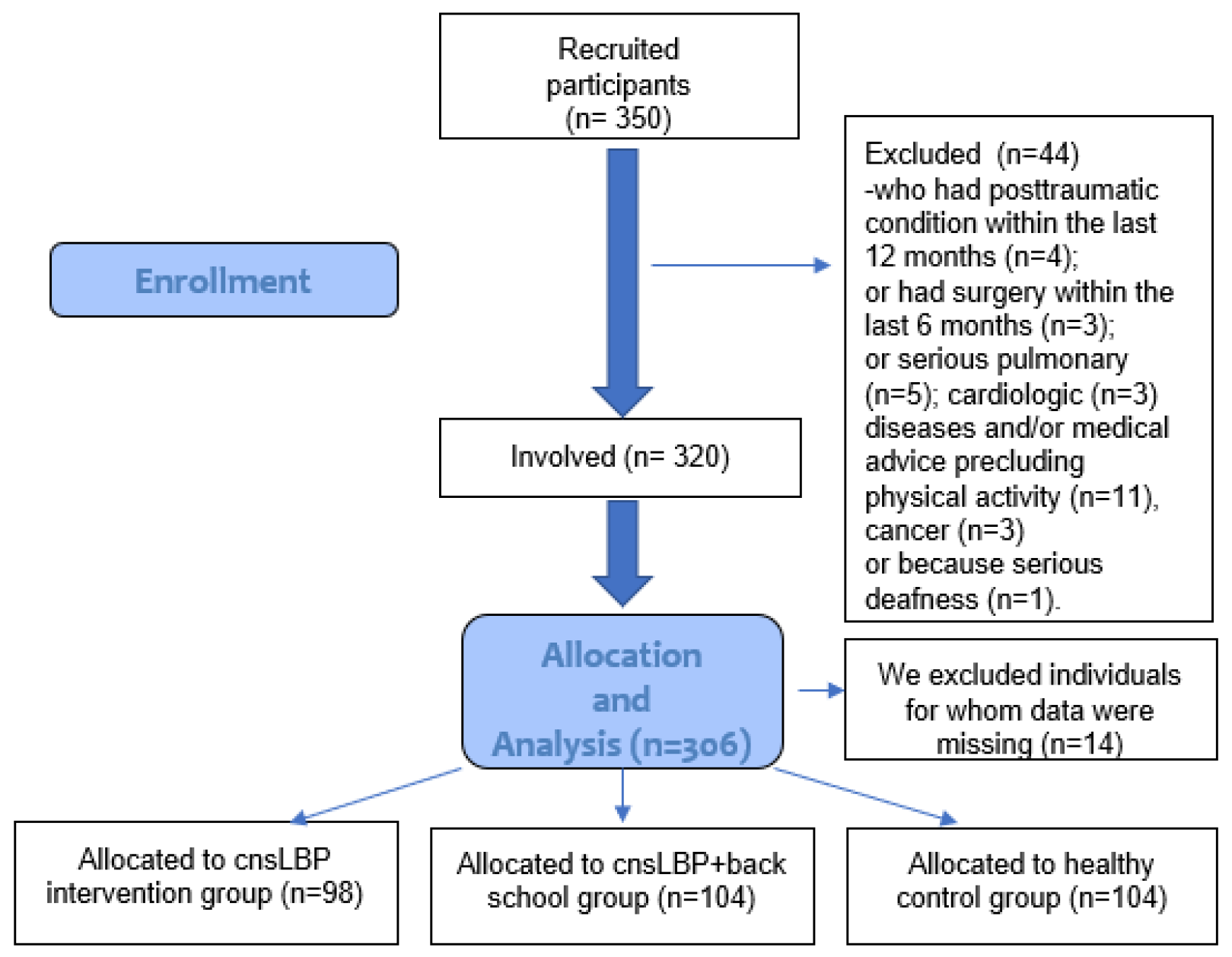
2.1. Participants
2.2. Exercise Intervention
2.3. Back School Program
2.4. Outcome Measures
2.5. Statistical Analysis
3. Results
3.1. Results of the Global Physical Activity Questionnaire
3.2. Results of Low Back Pain-Specific Knowledge
3.3. Results of Low-Back-Specific Functional Outcome
3.4. Results of the VAS Scale and Physical Activity Recommendations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hoy, D.; March, L.; Brooks, P.; Blyth, F.; Woolf, A.; Bain, C.; Williams, G.; Smith, E.; Vos, T.; Barendregt, J.; et al. The global burden of low back pain: Estimates from the Global Burden of Disease 2010 study. Ann. Rheum. Dis. 2014, 73, 968–974. [Google Scholar] [CrossRef] [PubMed]
- Bálint, G. A derékfájás diagnosztikájának és kezelésének modern elvei. LAM Lege Artis Med. 2011, 21, 5. [Google Scholar]
- Ács, P.; Stocker, M.; Füge, K.; Paár, D.; Oláh, A.; Kovács, A. Economic and public health benefits: The result of increased regular physical activity. Eur. J. Integr. Med. 2016, 8, 8–12. [Google Scholar] [CrossRef]
- Ács, P.; Kovács, A.; Paár, D.; Hoffbauer, M.; Szabó, P.; Szabó, T.; Stocker, M. Comparative analysis of the economic burdens of physical inactivity in Hungary between 2005 and 2017. BMC Public Health 2020, 20, 1174. [Google Scholar] [CrossRef]
- Ács, P.; Betlehem, J.; Oláh, A.; Bergier, J.; Melczer, C.; Prémusz, V.; Makai, A. Measurement of public health benefits of physical activity: Validity and reliability study of the international physical activity questionnaire in Hungary. BMC Public Health 2020, 20 (Suppl. S1), 1198. [Google Scholar] [CrossRef]
- Werber, A.; Zimmermann-Stenzel, M.; Moradi, B.; Neubauer, E.; Schiltenwolf, M. Awareness of the German population of common available guidelines of how to cope with lower back pain. Pain Physician 2014, 17, 217–226. [Google Scholar] [CrossRef]
- Eupa, E.W.G. EU Physical Activity Guidelines; Sport and Health: Brussels, Belgium, 2008. [Google Scholar]
- Piercy, K.L.; Troiano, R.P.; Ballard, R.M.; Carlson, S.A.; Fulton, J.E.; Galuska, D.A.; George, S.M.; Olson, R.D. The Physical Activity Guidelines for Americans. JAMA 2018, 320, 2020–2028. [Google Scholar] [CrossRef]
- Maciel, S.C.; Jennings, F.; Jones, A.; Natour, J. The Development and Validation of a Low Back Pain Knowledge Questionnaire—LKQ. Clinics 2009, 64, 1167–1175. [Google Scholar] [CrossRef]
- Kovács-Babócsay, B.; Makai, A.; Szilágyi, B.; Tardi, P.; Ács, P.; Velényi, A.; Rébék-Nagy, G.; Járomi, M. Egy deréktáji fájdalommal kapcsolatos betegségspecifikus tudást felmérő külföldi kérdőív hazai, magyar nyelvű validálása. Orvosi Hetil. 2019, 160, 1663–1672. [Google Scholar] [CrossRef]
- Awwad, W.M.; Alfayez, S.M.; Bin Dous, A.N.; Alrabiei, Q.A.; Altowim, A.A.; Almutair, A.S.; Arafah, O. Knowledge around back pain and spinal disorders among Saudi patients: A cross-sectional study. J. Pak. Med. Assoc. 2017, 67, 1228–1231. [Google Scholar]
- Kempf, H.-D. Rückenschule; Rowohlt Taschenbuck Verlag: Berlin, Germany, 2008. [Google Scholar]
- Durmus, D.; Unal, M.; Kuru, O. How effective is a modified exercise program on its own or with back school in chronic low back pain? A randomized-controlled clinical trial. J. Back Musculoskelet. Rehabil. 2014, 27, 553–561. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, T.; Bull, F. Development of the World Health Organization Global Physical Activity Questionnaire (GPAQ). J. Public Health 2006, 14, 66–70. [Google Scholar] [CrossRef]
- Ács, P.; Betlehem, J.; Oláh, A.; Bergier, B.; Morvay-Sey, K.; Makai, A.; Prémusz, V. Cross-cultural adaptation and validation of the Global Physical Activity Questionnaire among healthy Hungarian adults. BMC Public Health 2020, 20, 1056. [Google Scholar] [CrossRef] [PubMed]
- Valasek, T.; Varga, P.P.; Klemencsics, I.; Szoeverfi, Z.; Bozsodi, A. Az ágyéki gerinc funkciócsökkenésének mérése négy önkitöltôs, ágyékigerinc-specifikus állapotfelmérô kérdôív magyar nyelvi adaptálása és validálása. Clin. Neurosci. 2015, 68, 135–141. [Google Scholar]
- Freyd, M. The Graphic Rating Scale. J. Educ. Psychol. 1923, 14, 83–102. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Steffens, D.; Maher, C.; Pereira, L.S.M.; Stevens, M.L.; Oliveira, V.C.; Chapple, M.; Teixeira-Salmela, L.F.; Hancock, M. Prevention of Low Back Pain. JAMA Intern. Med. 2016, 176, 199. [Google Scholar] [CrossRef]
- Leeuw, M.; Goossens, M.; Linton, S.J.; Crombez, G.; Boersma, K.; Vlaeyen, J. The Fear-Avoidance Model of Musculoskeletal Pain: Current State of Scientific Evidence. J. Behav. Med. 2006, 30, 77–94. [Google Scholar] [CrossRef]
- Shiri, R.; Falah-Hassani, K. Does leisure time physical activity protect against low back pain? Systematic review and meta-analysis of 36 prospective cohort studies. Br. J. Sports Med. 2017, 51, 1410–1418. [Google Scholar] [CrossRef]
- Szilágyi, B.; Kukla, A.; Makai, A.; Ács, P.; Járomi, M. Sports therapy and recreation exercise program in type 2 diabetes: Randomized controlled trial, 3-month follow-up. J. Sports Med. Phys. Fit. 2019, 59, 676–685. [Google Scholar] [CrossRef]
- Heneweer, H.; Staes, F.; Aufdemkampe, G.; Van Rijn, M.; Vanhees, L. Physical activity and low back pain: A systematic review of recent literature. Eur. Spine J. 2011, 20, 826–845. [Google Scholar] [CrossRef] [PubMed]
- Hoogendoorn, W.E.; van Poppel, M.N.; Bongers, P.M.; Koes, B.W.; Bouter, L.M. Physical load during work and leisure time as risk factors for back pain. Scand. J. Work Environ. Health 1999, 25, 387–403. [Google Scholar] [CrossRef] [PubMed]
- Diz, J.B.M.; de Souza, J.R.L.M.; Leopoldino, A.A.O.; Oliveira, V.C. Exercise, especially combined stretching and strengthening exercise, reduces myofascial pain: A systematic review. J. Physiother. 2016, 63, 17–22. [Google Scholar] [CrossRef]
- Searle, A.; Spink, M.; Ho, A.; Chuter, V. Exercise interventions for the treatment of chronic low back pain: A systematic review and meta-analysis of randomised controlled trials. Clin. Rehabil. 2015, 29, 1155–1167. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Neurological Disorders and Stroke. Low Back Pain Fact Sheet. Available online: https://www.ninds.nih.gov/Disorders/Patient-Caregiver-Education/Fact-Sheets/Low-Back-Pain-Fact-Sheet (accessed on 11 January 2020).


{kind=link}
| Time | Topics of the Educational Program |
|---|---|
| First month | Spinal anatomy, spinal kinesiology and biomechanics, physiopathology of back disorders, cause of pain |
| Second month | Rules of spine protection, spine-friendly lifestyle ergonomics in daily living activities, and proper posture (e.g., posture at work, how to lift and transport objects correctly, etc.), LBP prevention options, LBP therapy options |
| Third month | Spine-friendly leisure, spine-friendly workplace, spine-friendly sports activities, ergonomic practical training |
| Median (IQR) | Healthy Control (n = 104) | cnsLBP + Back School (n = 104) | cnsLBP (n = 98) | p (Kruskal–Wallis Test) |
|---|---|---|---|---|
| Age (year) | 43.00 (37.25–47.50) | 43.00 (39.00–49.00) | 45.00 (41.00–58.00) | 0.017 |
| BMI (kg/m2) | 25.48 (22.62–27.42) | 25.46 (22.62–27.45) | 26.88 (22.72–27.45) | 0.227 |
| Time spent since the diagnosis (year) | 0.00 (0.00–0.00) | 4.00 (3.25–5.00) | 4.00 (4.00–5.00) | <0.001 |
| Healthy Control (n = 104) Mean (SD) | cnsLBP + Back School (n = 104) Mean (SD) | cnsLBP (n = 98) Mean (SD) | p (Kruskal–Wallis Tests) | ||||
|---|---|---|---|---|---|---|---|
| sitting time (min/day) | 681.01 | 61.16 | 603.75 | 13.67 | 697.79 | 104.16 | <0.001 |
| work total (min/week) | 57.93 | 72.86 | 4.66 | 18.24 | 22.53 | 51.29 | <0.001 |
| active transportation (min/week) | 9.59 | 26.10 | 39.09 | 70.84 | 17.18 | 47.15 | <0.001 |
| total leisure time (min/week) | 23.99 | 50.59 | 246.44 | 47.31 | 100.46 | 113.49 | <0.001 |
| total physical activity time (min/week) | 91.51 | 86.08 | 290.19 | 85.51 | 140.17 | 132.48 | <0.001 |
| VAS | RMDQ | LKQ | ||
|---|---|---|---|---|
| Healthy control (n = 104) | Median | 0.00 | 0.00 | 9.00 |
| IQR lower | 0.00 | 0.00 | 8.00 | |
| IQR upper | 0.00 | 0.00 | 9.00 | |
| cnsLBP + back school (n = 104) | Median | 0.00 | 0.00 | 21.00 |
| IQR lower | 0.00 | 0.00 | 20.00 | |
| IQR upper | 0.00 | 0.00 | 22.00 | |
| cnsLBP (n = 98) | Median | 2.00 | 3.00 | 9.00 |
| IQR lower | 2.00 | 2.75 | 8.00 | |
| IQR upper | 3.00 | 3.00 | 9.00 | |
| p value (Kruskal–Wallis test) | <0.001 | <0.001 | <0.001 | |
| Healthy Control (n = 104) | cnsLBP + Back School (n = 104) | cnsLBP (n = 98) | p (Chi-Square Test) |
|---|---|---|---|
| n = 79 | n = 104 | n = 1 | |
| 75.96% | 100.00% | 0.96% | <0.001 |
| Authors (Year) | Examined Population | Methods | Results (Points) |
|---|---|---|---|
| Maciel et al. (2009) [9] | 60 participants cnsLBP, mean age: 43 years | LKQ | 9.8 |
| Kovács-Babócsay et al. (2019) [10] | 58 participants, health care workers, mean age: 22 | LKQ | 18.92 |
| Awwad et al. (2014) [11] | 153 participants cnsLBP, mean age: 40.2 years | LKQ | 9 |
| Present research | 104 participants cnsLBP + back school, mean age: 45.06 years | LKQ | 20.87 |
| 98 participants cnsLBP, mean age: 47.68 years | 8.74 | ||
| 104 healthy participants, mean age: 42.59 years | 8.79 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hock, M.; Járomi, M.; Prémusz, V.; Szekeres, Z.J.; Ács, P.; Szilágyi, B.; Wang, Z.; Makai, A. Disease-Specific Knowledge, Physical Activity, and Physical Functioning Examination among Patients with Chronic Non-Specific Low Back Pain. Int. J. Environ. Res. Public Health 2022, 19, 12024. https://doi.org/10.3390/ijerph191912024
Hock M, Járomi M, Prémusz V, Szekeres ZJ, Ács P, Szilágyi B, Wang Z, Makai A. Disease-Specific Knowledge, Physical Activity, and Physical Functioning Examination among Patients with Chronic Non-Specific Low Back Pain. International Journal of Environmental Research and Public Health. 2022; 19(19):12024. https://doi.org/10.3390/ijerph191912024
Chicago/Turabian StyleHock, Márta, Melinda Járomi, Viktória Prémusz, Zsolt János Szekeres, Pongrác Ács, Brigitta Szilágyi, Zhe Wang, and Alexandra Makai. 2022. "Disease-Specific Knowledge, Physical Activity, and Physical Functioning Examination among Patients with Chronic Non-Specific Low Back Pain" International Journal of Environmental Research and Public Health 19, no. 19: 12024. https://doi.org/10.3390/ijerph191912024
APA StyleHock, M., Járomi, M., Prémusz, V., Szekeres, Z. J., Ács, P., Szilágyi, B., Wang, Z., & Makai, A. (2022). Disease-Specific Knowledge, Physical Activity, and Physical Functioning Examination among Patients with Chronic Non-Specific Low Back Pain. International Journal of Environmental Research and Public Health, 19(19), 12024. https://doi.org/10.3390/ijerph191912024