
A Mobile Application to Help Self-Manage Pain Severity, Anxiety, and Depressive Symptoms in Patients with Fibromyalgia Syndrome: A Pilot Study

 ,
,  , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Procedure
2.2. Participants
2.3. Measures
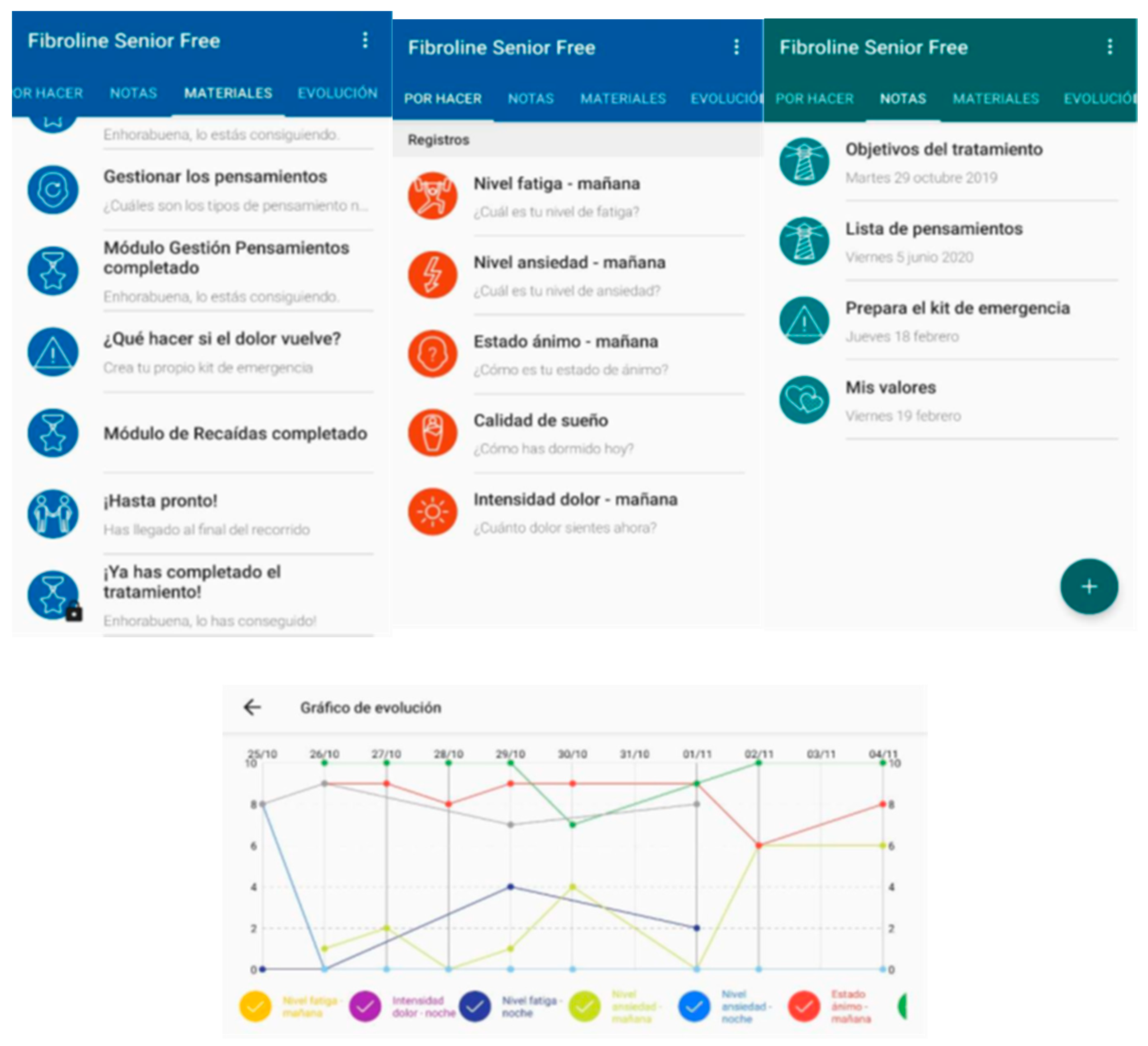
2.4. The Mobile Application
2.5. Data Analysis
3. Results
3.1. Description of the Study Sample
3.2. Satisfaction with the App
3.3. Comparisons between Pre-Treatment, Post-Treatment, and 3-Month Follow-Up Measures of the Outcome Variables
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Sarzi-Puttini, P.; Giorgi, V.; Marotto, D.; Atzeni, F. Fibromyalgia: An update on clinical characteristics, aetiopathogenesis and treatment. Nat. Rev. Rheumatol. 2020, 16, 645–660. [Google Scholar] [CrossRef] [PubMed]
- Walitt, B.; Nahin, R.L.; Katz, R.S.; Bergman, M.J.; Wolfe, F. The Prevalence and Characteristics of Fibromyalgia in the 2012 National Health Interview Survey. PLoS ONE 2015, 10, e0138024. [Google Scholar] [CrossRef]
- Celepkolu, T.; Gamze Erten Bucaktepe, P.; Yilmaz, A.; Pervane, V.D.; Batmaz, I.; Sariyildiz, M.A. Assessment of quality of life, anxiety, depression, and sleep quality in women with fibromyalgia and their spouses. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 4506–4513. [Google Scholar] [PubMed]
- Horta-Baas, G.; Romero-Figueroa, M.D.S. Self-reported disability in women with fibromyalgia from a tertiary care center. Adv. Rheumatol. 2019, 59, 45. [Google Scholar] [CrossRef] [PubMed]
- Bair, M.J.; Krebs, E.E. Fibromyalgia. Ann. Intern. Med. 2020, 172, ITC33–ITC48. [Google Scholar] [CrossRef] [PubMed]
- Tangen, S.F.; Helvik, A.-S.; Eide, H.; Fors, E.A. Pain acceptance and its impact on function and symptoms in fibromyalgia. Scand. J. Pain 2020, 20, 727–736. [Google Scholar] [CrossRef]
- Bernardy, K.; Klose, P.; Welsch, P.; Häuser, W. Efficacy, acceptability and safety of cognitive behavioural therapies in fibromyalgia syndrome—A systematic review and meta-analysis of randomized controlled trials. Eur. J. Pain 2018, 22, 242–260. [Google Scholar] [CrossRef]
- Perrot, S.; Russell, I.J. More ubiquitous effects from non-pharmacologic than from pharmacologic treatments for fibromyalgia syndrome: A meta-analysis examining six core symptoms. Eur. J. Pain 2014, 18, 1067–1080. [Google Scholar] [CrossRef]
- de la Vega, R.; Miró, J. mHealth: A strategic field without a solid scientific soul. a systematic review of pain-related apps. PLoS ONE 2014, 9, e101312. [Google Scholar] [CrossRef]
- Llorens-Vernet, P.; Miró, J. Standards for Mobile Health-Related Apps: Systematic Review and Development of a Guide. JMIR mHealth uHealth 2020, 8, e13057. [Google Scholar] [CrossRef]
- Pfeifer, A.-C.; Uddin, R.; Schröder-Pfeifer, P.; Holl, F.; Swoboda, W.; Schiltenwolf, M. Mobile Application-Based Interventions for Chronic Pain Patients: A Systematic Review and Meta-Analysis of Effectiveness. J. Clin. Med. 2020, 9, 3557. [Google Scholar] [CrossRef] [PubMed]
- Turk, D.C.; Dworkin, R.H.; Allen, R.R.; Bellamy, N.; Brandenburg, N.; Carr, D.B.; Cleeland, C.; Dionne, R.; Farrar, J.T.; Galer, B.S.; et al. Core outcome domains for chronic pain clinical trials: IMMPACT recommendations. Pain 2003, 106, 337–345. [Google Scholar] [CrossRef] [PubMed]
- Dworkin, R.H.; Turk, D.C.; Farrar, J.T.; Haythornthwaite, J.A.; Jensen, M.P.; Katz, N.P.; Kerns, R.D.; Stucki, G.; Allen, R.R.; Bellamy, N.; et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain 2005, 113, 9–19. [Google Scholar] [CrossRef] [PubMed]
- Häuser, W.; Fisher, E.; Perrot, S.; Moore, R.A.; Makri, S.; Bidonde, J. Non-pharmacological interventions for fibromyalgia (fibromyalgia syndrome) in adults: An overview of Cochrane Reviews. Cochrane Database Syst. Rev. 2022, 2022. [Google Scholar]
- Jensen, M.P.; Castarlenas, E.; Tomé-Pires, C.; de la Vega, R.; Sánchez-Rodríguez, E.; Miró, J. The Number of Ratings Needed for Valid Pain Assessment in Clinical Trials: Replication and Extension. Pain Med. 2015, 16, 1764–1772. [Google Scholar] [CrossRef]
- Castarlenas, E.; Sánchez-Rodríguez, E.; de la Vega, R.; Roset, R.; Miró, J. Agreement between verbal and electronic versions of the Numerical Rating Scale (NRS-11) when used to assess pain intensity in adolescents. Clin. J. Pain 2015, 31, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Rico, A.; Fernández, J.A. Propiedades clinimétricas de la versión castellana del cuestionario de Pittsburgh. Vigilia-Sueño 1997, 9, 81–94. [Google Scholar]
- Pilkonis, P.A.; Choi, S.W.; Reise, S.P.; Stover, A.M.; Riley, W.T.; Cella, D. Item banks for measuring emotional distress from the patient-reported outcomes measurement information system (PROMIS®): Depression, anxiety, and anger. Assessment 2011, 18, 263–283. [Google Scholar] [CrossRef]
- Miró, J.; Sánchez-Rodríguez, E.; Brijaldo, S.; Jensen, M.P. The Silhouettes Fatigue Scale: Comprehensibility and validity in older individuals. Disabil. Rehabil. 2020, 42, 1906–1911. [Google Scholar] [CrossRef]
- Expósito-Vizcaíno, S.; Sánchez-Rodríguez, E.; Miró, J. The role of physical, cognitive and social factors in pain interference with activities of daily living among individuals with chronic cancer pain. Eur. J. Cancer Care 2020, 29, e13203. [Google Scholar] [CrossRef]
- Miró, J.; Jensen, M.P.; Ramírez-Maestre, C.; Esteve, R.; López-Martínez, A.E.; de la Vega, R. The Silhouettes Fatigue Scale: A validity study with individuals with physical disabilities and chronic pain. Disabil. Rehabil. 2021, 1–6. [Google Scholar] [CrossRef] [PubMed]
- de la Vega, R.; Roset, R.; Galán, S.; Miró, J. Fibroline: A mobile app for improving the quality of life of young people with fibromyalgia. J. Health Psychol. 2018, 23, 67–78. [Google Scholar] [CrossRef] [Green Version]
- Williams, A.; Fisher, E.; Hearn, L.; Eccleston, C. Psychological therapies for the management of chronic pain (excluding headache) in adults. Cochrane Database Syst. Rev. 2020, 2020. [Google Scholar] [CrossRef] [PubMed]
- Mecklenburg, G.; Smittenaar, P.; Erhart-Hledik, J.C.; Perez, D.A.; Hunter, S. Effects of a 12-week digital care program for chronic knee pain on pain, mobility, and surgery risk: Randomized controlled trial. J. Med. Internet Res. 2018, 20, e156. [Google Scholar] [CrossRef]
- Theadom, A.; Cropley, M.; Smith, H.E.; Feigin, V.L.; Mcpherson, K. Mind and body therapy for fibromyalgia. Cochrane Database Syst. Rev. 2015, 2015, CD001980. [Google Scholar] [CrossRef] [PubMed]
- Estévez-López, F.; Maestre-Cascales, C.; Russell, D.; Álvarez-Gallardo, I.C.; Rodriguez-Ayllon, M.; Hughes, C.M.; Davison, G.W.; Sañudo, B.; McVeigh, J.G. Effectiveness of Exercise on Fatigue and Sleep Quality in Fibromyalgia: A Systematic Review and Meta-analysis of Randomized Trials. Arch. Phys. Med. Rehabil. 2021, 102, 752–761. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.-Y.; Lee, J.-S.; Park, S.-Y.; Kim, S.-J.; Son, C.-G. Systematic review of randomized controlled trials for chronic fatigue syndrome/myalgic encephalomyelitis (CFS/ME). J. Transl. Med. 2020, 18, 7. [Google Scholar] [CrossRef]
- Prins, J.B.; Bleijenberg, G.; Bazelmans, E.; Elving, L.D.; de Boo, T.M.; Severens, J.L.; van der Wilt, G.J.; Spinhoven, P.; van der Meer, J.W. Cognitive behaviour therapy for chronic fatigue syndrome: A multicentre randomised controlled trial. Lancet 2001, 357, 841–847. [Google Scholar] [CrossRef]
- Hayran, Y.; İncel Uysal, P.; Öktem, A.; Aksoy, G.G.; Akdoğan, N.; Yalçın, B. Factors affecting adherence and patient satisfaction with treatment: A cross-sectional study of 500 patients with acne vulgaris. J. Dermatol. Treat. 2021, 32, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Jamison, R.N.; Mei, A.; Ross, E.L. Longitudinal trial of a smartphone pain application for chronic pain patients: Predictors of compliance and satisfaction. J. Telemed. Telecare 2018, 24, 93–100. [Google Scholar] [CrossRef]
- Carson, J.W.; Carson, K.M.; Jones, K.D.; Mist, S.D.; Bennett, R.M. Follow-up of yoga of awareness for fibromyalgia: Results at 3 months and replication in the wait-list group. Clin. J. Pain 2012, 28, 804–813. [Google Scholar] [CrossRef] [PubMed]
- Serrat, M.; Sanabria-Mazo, J.P.; Almirall, M.; Musté, M.; Feliu-Soler, A.; Méndez-Ulrich, J.L.; Sanz, A.; Luciano, J.V. Effectiveness of a Multicomponent Treatment Based on Pain Neuroscience Education, Therapeutic Exercise, Cognitive Behavioral Therapy, and Mindfulness in Patients With Fibromyalgia (FIBROWALK Study): A Randomized Controlled Trial. Phys. Ther. 2021, 101, pzab200. [Google Scholar] [CrossRef] [PubMed]
- Udina-Cortés, C.; Fernández-Carnero, J.; Romano, A.A.; Cuenca-Zaldívar, J.N.; Villafañe, J.H.; Castro-Marrero, J.; Alguacil-Diego, I.M. Effects of neuro-adaptive electrostimulation therapy on pain and disability in fibromyalgia: A prospective, randomized, double-blind study. Medicine 2020, 99, e23785. [Google Scholar] [CrossRef] [PubMed]
- Llorens-Vernet, P.; Miró, J. The Mobile App Development and Assessment Guide (MAG): Delphi-Based Validity Study. JMIR mHealth uHealth 2020, 8, e17760. [Google Scholar] [CrossRef]


{kind=link}
| Mean Pre-Treatment (SD) | Post-Treatment | Mean 3-Month Follow-Up (SD) | p Value Pre-Treatment- Post-Treatment | p Value Pre-Treatment- 3-Month Follow-Up | p Value Post-Treatment- 3-Month Follow-Up | |||
|---|---|---|---|---|---|---|---|---|
| n | Mean (SD) | n | Mean (SD) | |||||
| Pain Severity (NRS-11) | 7.93 (4.16) | 53 | 7.41 (1.49) | 29 | 7.61 (1.31) | 0.007 | 0.546 | 0.753 |
| Sleep Quality (PSQI) | 13.74 (3.83) | 52 | 14.71 (3.65) | 26 | 13.50 (5.16) | 0.874 | 0.105 | 0.073 |
| Anxiety (PROMIS) | 25.89 (6.81) | 52 | 23.79 (7.61) | 23 | 25.13 (8.122) | 0.007 | 0.081 | 0.779 |
| Depression (PROMIS) | 24.88 (8.09) | 48 | 22.42 (8.39) | 19 | 22.95 (9.02) | 0.004 | 0.868 | 0.019 |
| Fatigue (SFS) | 4.30 (1.19) | 48 | 4.27 (1.25) | 19 | 4.21 (1.36) | 0.718 | 0.856 | 0.190 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miró, J.; Lleixà-Daga, M.; de la Vega, R.; Llorens-Vernet, P.; Jensen, M.P. A Mobile Application to Help Self-Manage Pain Severity, Anxiety, and Depressive Symptoms in Patients with Fibromyalgia Syndrome: A Pilot Study. Int. J. Environ. Res. Public Health 2022, 19, 12026. https://doi.org/10.3390/ijerph191912026
Miró J, Lleixà-Daga M, de la Vega R, Llorens-Vernet P, Jensen MP. A Mobile Application to Help Self-Manage Pain Severity, Anxiety, and Depressive Symptoms in Patients with Fibromyalgia Syndrome: A Pilot Study. International Journal of Environmental Research and Public Health. 2022; 19(19):12026. https://doi.org/10.3390/ijerph191912026
Chicago/Turabian StyleMiró, Jordi, Meritxell Lleixà-Daga, Rocío de la Vega, Pere Llorens-Vernet, and Mark P. Jensen. 2022. "A Mobile Application to Help Self-Manage Pain Severity, Anxiety, and Depressive Symptoms in Patients with Fibromyalgia Syndrome: A Pilot Study" International Journal of Environmental Research and Public Health 19, no. 19: 12026. https://doi.org/10.3390/ijerph191912026
APA StyleMiró, J., Lleixà-Daga, M., de la Vega, R., Llorens-Vernet, P., & Jensen, M. P. (2022). A Mobile Application to Help Self-Manage Pain Severity, Anxiety, and Depressive Symptoms in Patients with Fibromyalgia Syndrome: A Pilot Study. International Journal of Environmental Research and Public Health, 19(19), 12026. https://doi.org/10.3390/ijerph191912026