


Social Frailty among Community-Dwelling Older Adults during the COVID-19 Pandemic in Korea: A Cross-Sectional Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection and Participants
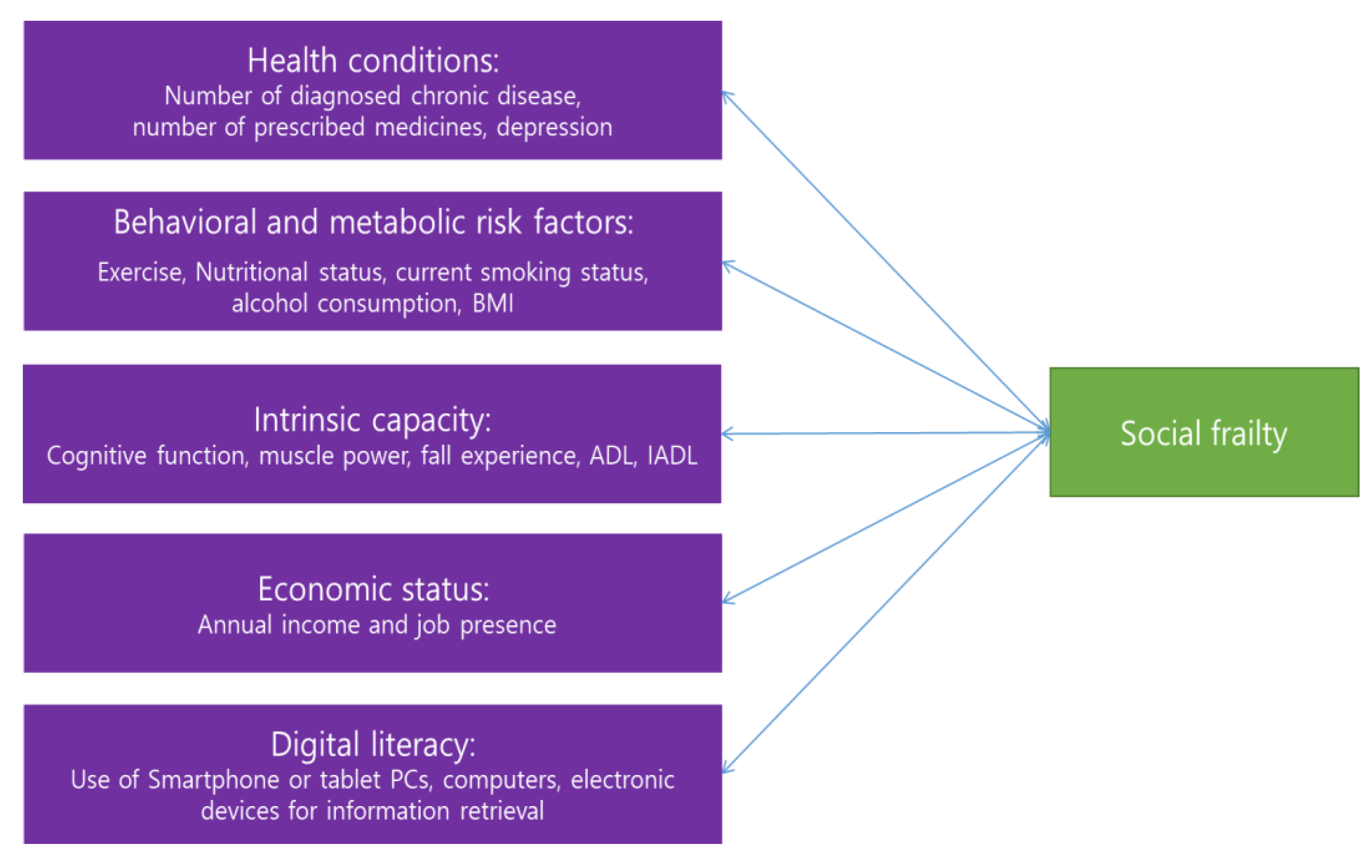
2.3. Measures
2.3.1. Social Frailty
2.3.2. Health Conditions
2.3.3. Behavioral and Metabolic Risk Factors
2.3.4. Intrinsic Capacity
2.3.5. Economic Status
2.3.6. Digital Literacy
2.4. Ethical Considerations
2.5. Data Analyses
3. Results
3.1. Prevalence Rate of Social Frailty
3.2. Differences in Health Conditions, Behavioral and Metabolic Risk Factors, and Intrinsic Capacity of Participants in the Robust, Social Prefrailty, and Social Frailty Groups
3.3. Differences in Economic Status and Digital Literacy of Participants in the Robust, Social Prefrailty, and Social Frailty Groups
3.4. Results of Multinomial Logistic Regression
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Social Isolation and Loneliness among Older People: Advocacy Brief. 2015. Available online: https://www.who.int/publications/i/item/9789240030749 (accessed on 1 February 2022).
- World Health Organization. The Global Network for Age-Friendly Cities and Communities: Looking Back over the Last Decade, Looking forward to the Next. 2018. Available online: https://www.who.int/publications/i/item/WHO-FWC-ALC-18.4 (accessed on 14 January 2022).
- Bunt, S.; Steverink, N.; Olthof, J.; Van Der Schans, C.P.; Hobbelen, J. Social frailty in older adults: A scoping review. Eur. J. Ageing 2017, 14, 323–334. [Google Scholar] [CrossRef] [PubMed]
- Pek, K.; Chew, J.; Lim, J.P.; Yew, S.; Tan, C.N.; Yeo, A.; Ding, Y.Y.; Lim, W.S. Social Frailty Is Independently Associated with Mood, Nutrition, Physical Performance, and Physical Activity: Insights from a Theory-Guided Approach. Int. J. Environ. Res. Public Health 2020, 17, 4239. [Google Scholar] [CrossRef]
- Ko, H.; Jung, S. Association of Social Frailty with Physical Health, Cognitive Function, Psychological Health, and Life Satisfaction in Community-Dwelling Older Koreans. Int. J. Environ. Res. Public Health 2021, 18, 818. [Google Scholar] [CrossRef]
- Yamada, M.; Arai, H. Social Frailty Predicts Incident Disability and Mortality Among Community-Dwelling Japanese Older Adults. J. Am. Med Dir. Assoc. 2018, 19, 1099–1103. [Google Scholar] [CrossRef] [PubMed]
- Nagai, K.; Tamaki, K.; Kusunoki, H.; Wada, Y.; Tsuji, S.; Itoh, M.; Sano, K.; Amano, M.; Hayashitani, S.; Yokoyama, R.; et al. Physical frailty predicts the development of social frailty: A prospective cohort study. BMC Geriatr. 2020, 20, 403. [Google Scholar] [CrossRef] [PubMed]
- Wilder-Smith, A.; Freedman, D.O. Isolation, quarantine, social distancing and community containment: Pivotal role for old-style public health measures in the novel coronavirus (2019-nCoV) outbreak. J. Travel Med. 2020, 27. [Google Scholar] [CrossRef]
- Kim, H.; Shim, J. Digital literacy of elderly people and social activities. Korean J. Policy Anal. Eval. 2020, 30, 156–180. [Google Scholar]
- Lozupone, M.; La Montagna, M.; Di Gioia, I.; Sardone, R.; Resta, E.; Daniele, A.; Giannelli, G.; Bellomo, A.; Panza, F. Social Frailty in the COVID-19 Pandemic Era. Front. Psychiatry 2020, 11, 577113. [Google Scholar] [CrossRef]
- Chen, A.T.; Ge, S.; Cho, S.; Teng, A.K.; Chu, F.; Demiris, G.; Zaslavsky, O. Reactions to COVID-19, information and technology use, and social connectedness among older adults with pre-frailty and frailty. Geriatr. Nurs. 2021, 42, 188–195. [Google Scholar] [CrossRef]
- Korea Institute for Health and Social Affairs. Survey of Korea Older Adults. 2020. Available online: http://www.mohw.go.kr/react/jb/sjb030301vw.jsp?PAR_MENU_ID=03&MENU_ID=032901&CONT_SEQ=366496 (accessed on 17 July 2021).
- Tsutsumimoto, K.; Doi, T.; Makizako, H.; Hotta, R.; Nakakubo, S.; Makino, K.; Suzuki, T.; Shimada, H. Association of Social Frailty With Both Cognitive and Physical Deficits Among Older People. J. Am. Med Dir. Assoc. 2017, 18, 603–607. [Google Scholar] [CrossRef]
- Tsutsumimoto, K.; Doi, T.; Makizako, H.; Hotta, R.; Nakakubo, S.; Kim, M.; Kurita, S.; Suzuki, T.; Shimada, H. Social Frailty Has a Stronger Impact on the Onset of Depressive Symptoms than Physical Frailty or Cognitive Impairment: A 4-Year Follow-up Longitudinal Cohort Study. J. Am. Med Dir. Assoc. 2018, 19, 504–510. [Google Scholar] [CrossRef] [PubMed]
- Cho, M.J.; Bae, J.N.; Suh, G.H.; Hahm, B.J.; Kim, J.K.; Lee, D.W.; Kang, M.H. Validation of geriatric depression scale, Korean version (GDS) in the assessment of DSM-Ⅲ-R major depression. J. Korean Neuropsychiatr. Assoc. 1999, 38, 48–63. [Google Scholar]
- Kim, M.; Sohn, A.R.; Yang, J. Standard Drink, Guidelines for Low Risk Drinking, and Divided Discourses. Alcohol. Health Behav. Res. 2019, 20, 113–130. [Google Scholar] [CrossRef]
- Posner, B.M.; Jette, A.M.; Smith, K.W.; Miller, D.R. Nutrition and health risks in the elderly: The nutrition screening initiative. Am. J. Public Health 1993, 83, 972–978. [Google Scholar] [CrossRef] [PubMed]
- Han, J.W.; Kim, T.H.; Jhoo, J.H.; Park, J.H.; Kim, J.L.; Ryu, S.H.; Moon, S.W.; Choo, I.H.; Lee, D.W.; Yoon, J.C.; et al. A normative study of the mini mental state examination for dementia screening (MMSE-DS) and its short form (SMMSE-DS) in the Korean elderly. J. Korean Geriatr. Psythiatry 2010, 14, 7–37. [Google Scholar]
- Freer, K.; Wallington, S. Social frailty: The importance of social and environmental factors in predicting frailty in older adults. Br. J. Community Nurs. 2019, 24, 486–492. [Google Scholar] [CrossRef] [PubMed]
- Kojima, G.; Jivraj, S.; Iliffe, S.; Falcaro, M.; Liljas, A.; Walters, K. Alcohol Consumption and Risk of Incident Frailty: The English Longitudinal Study of Aging. J. Am. Med Dir. Assoc. 2019, 20, 725–729. [Google Scholar] [CrossRef]
- Kojima, G.; Liljas, A.; Iliffe, S.; Jivraj, S.; Walters, K. A systematic review and meta-analysis of prospective associations between alcohol consumption and incident frailty. Age Ageing 2018, 47, 26–34. [Google Scholar] [CrossRef]
- Sabia, S.; Elbaz, A.; Britton, A.; Bell, S.; Dugravot, A.; Shipley, M.; Kivimaki, M.; Singh-Manoux, A. Alcohol consumption and cognitive decline in early old age. Neurology 2014, 82, 332–339. [Google Scholar] [CrossRef]
- Ottenbacher, K.J.; Graham, J.E.; Al Snih, S.; Raji, M.; Samper-Ternent, R.; Ostir, G.V.; Markides, K.S. Mexican Americans and Frailty: Findings From the Hispanic Established Populations Epidemiologic Studies of the Elderly. Am. J. Public Health 2009, 99, 673–679. [Google Scholar] [CrossRef]
- Gobbens, R.J.; van Assen, M.A. Associations between multidimensional frailty and quality of life among Dutch older people. Arch. Gerontol. Geriatr. 2017, 73, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Sun, F.; Tang, Z. Social Frailty is Associated with Physical Functioning, Cognition, and Depression, and Predicts Mortality. J. Nutr. Health Aging 2018, 22, 989–995. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Arai, H.; Kim, S. Social activities are associated with cognitive decline in older Koreans. Geriatr. Gerontol. Int. 2017, 17, 1191–1196. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, L.C.; Steptoe, A. Social Isolation, Loneliness, and Health Behaviors at Older Ages: Longitudinal Cohort Study. Ann. Behav. Med. 2018, 52, 582–593. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.Y.; Chiou, A.F. Social media usage, social support, intergenerational relationships, and depressive symptoms among older adults. Geriatr. Nurs. 2020, 41, 615–621. [Google Scholar] [CrossRef]
- Hayashi, T.; Noguchi, T.; Kubo, Y.; Tomiyama, N.; Ochi, A.; Hayashi, H. Social frailty and depressive symptoms during the COVID-19 pandemic among older adults in Japan: Role of home exercise habits. Arch. Gerontol. Geriatr. 2022, 98, 104555. [Google Scholar] [CrossRef]
- Lee, K.; Jeong, G.-C.; Yim, J. Consideration of the Psychological and Mental Health of the Elderly during COVID-19: A Theoretical Review. Int. J. Environ. Res. Public Health 2020, 17, 8098. [Google Scholar] [CrossRef]
- Xie, B.; Charness, N.; Fingerman, K.; Kaye, J.; Kim, M.T.; Khurshid, A. When Going Digital Becomes a Necessity: Ensuring Older Adults’ Needs for Information, Services, and Social Inclusion During COVID-19. J. Aging Soc. Policy 2020, 32, 460–470. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Category | Total (n = 9920, 100%) Mean (SD) | Robust a (n = 1218, 12.3%) Mean (SD) or n (%) | Social Prefrailty b (n = 3612, 36.4%) Mean (SD) or n (%) | Social Frailty c (n = 5090, 51.3%) Mean (SD) or n (%) | χ2/F | p | Scheffé Test |
|---|---|---|---|---|---|---|---|---|
| Demographic characteristics | ||||||||
| Age (years) | 73.4 (6.5) | 72.1 (5.8) | 73.2 (6.2) | 73.93 (6.9) | 41.89 | <0.001 | a < b, a < c | |
| Male | 3971 (40.0) | 604 (49.6) | 1467 (40.6) | 1900 (37.3) | 62.36 | <0.001 | ||
| Education (years) | 8.2 (4.0) | 9.11 (3.6) | 8.38 (3.9) | 7.84 (4.1) | 55.67 | <0.001 | a > b, a > c | |
| Health conditions | ||||||||
| Number of diagnosed chronic diseases | 1.8 (1.5) | 1.5 (1.3) | 1.7 (1.4) | 2.01 (1.6) | 87.17 | <0.001 | a < b, a < c | |
| Number of prescribed medicines | 1.8 (1.5) | 1.4 (1.2) | 1.6 (1.4) | 1.95 (1.7) | 80.67 | <0.001 | a < b, a < c | |
| Depression | 3.4 (3.4) | 2.2 (2.3) | 2.7 (2.7) | 4.17 (3.8) | 317.51 | <0.001 | a < b, a < c | |
| Behavioral and metabolic risk factors | ||||||||
| Exercise (yes) | 692 (56.8) | 2041 (56.5) | 2454 (48.2) | 69.66 | <0.001 | |||
| Exercise (weekly frequency) | 4.8 (1.8) | 5.2 (1.6) | 4.8 (1.8) | 4.6 (1.8) | 29.81 | <0.001 | a > b, a > c | |
| Nutritional status | Mean score | 2.0 (3.0) | 0.9 (1.77) | 1.5 (2.3) | 2.6 (3.5) | 251.30 | <0.001 | a < b, a < c, b < c |
| Good | 7058 (71.1) | 1068 (87.7) | 2807 (77.7) | 3183 (62.5) | 486.07 | <0.001 | ||
| Moderate nutritional risk | 1943 (19.6) | 123 (10.1) | 625 (17.3) | 1195 (23.5) | ||||
| High nutritional risk | 919 (9.3) | 27 (2.2) | 180 (5.0) | 712 (14.0) | ||||
| Current smoking (yes) | 1089 (11.0) | 206 (16.9) | 375 (10.4) | 508 (10.0) | 50.40 | <0.001 | ||
| Drinking frequency over the past year | 1.2 (1.8) | 1.5 (1.90) | 1.1 (1.7) | 1.1 (1.7) | 27.79 | <0.001 | a > b, a > c | |
| Risk drinkers | 1943 (52.8) | 248 (45.4) | 672 (51.1) | 1023 (56.3) | 22.32 | <0.001 | ||
| Alcohol consumption | 3.9 (2.3) | 3.8 (2.31) | 3.7 (2.1) | 4.0 (2.3) | 4.22 | 0.015 | b < c | |
| BMI | Mean score | 23.6 (2.6) | 23.6 (2.36) | 23.7 (2.5) | 23.5 (2.7) | 4.03 | 0.018 | b > c |
| Underweight | 213 (2.2) | 14 (1.2) | 67 (1.9) | 132 (2.6) | 15.71 | 0.003 | ||
| Normal | 7208 (72.9) | 917 (75.6) | 2605 (72.3) | 3686 (72.6) | ||||
| Obesity | 2468 (25.0) | 282 (23.2) | 929 (25.8) | 1257 (24.8) | ||||
| Intrinsic capacity | ||||||||
| Cognitive scale | 24.3 (5.3) | 25.8 (4.04) | 24.7 (4.9) | 23.7 (5.7) | 90.42 | <0.001 | a > b, a > c, b > c | |
| Muscle power | Performed | 7285 (73.4) | 1009 (82.8) | 2754 (76.2) | 3522 (69.2) | 159.64 | <0.001 | |
| Fall experiences | Yes | 633 (6.4) | 49 (4.0) | 195 (5.4) | 389 (7.6) | 30.73 | <0.001 | |
| ADL | 7.2 (1.1) | 7.0 (0.3) | 7.1 (0.7) | 7.3 (1.4) | 45.58 | <0.001 | a < c, b < c | |
| IADL | 10.6 (2.6) | 10.1 (0.9) | 10.3 (1.8) | 10.9 (3.2) | 78.52 | <0.001 | a < c, b < c | |
| Characteristic | Total (n = 9920, 100%) Mean (SD) or n (%) | Robust a (n = 1218, 12.3%) Mean (SD) or n (%) | Social Prefrailty b (n = 3612, 36.4%) Mean (SD) or n (%) | Social Frailty c (n = 5090, 51.3%) Mean (SD) or n (%) | χ2/F | p | Scheffé Test | |
|---|---|---|---|---|---|---|---|---|
| Economic status | ||||||||
| Job | Yes | 516 (42.4) | 1320 (36.5) | 1778 (34.9) | 23.48 | <0.001 | ||
| Annual income (10,000 Won) | 2700.6 (3976.7) | 3256.5 (2777.8) | 2698.8 (2500.4) | 2568.8 (4944.8) | 14.74 | <0.001 | a > b, a > c | |
| Digital literacy | ||||||||
| Use of smartphones or tablet PCs | Yes | 5083 (51.2) | 766 (62.9) | 1939 (53.7) | 2378 (46.7) | 116.43 | <0.001 | |
| Use of computers | Yes | 543 (5.5) | 97 (8.0) | 239 (6.6) | 207 (4.1) | 43.19 | <0.001 | |
| Utilization of electronic devices (information retrieval) | 3955 (45.6) | 599 (52.8) | 1509 (47.0) | 1847 (42.8) | 39.96 | <0.001 | ||
| Robust versus Social Frailty | Social Prefrailty versus Social Frailty | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| B | p | Exp (B) | 95% CI | B | p | Exp (B) | 95% CI | |||
| Lower | Upper | Lower | Upper | |||||||
| (Constant) | −2.913 | 0.001 | −1.364 | 0.005 | ||||||
| Age | 0.004 | 0.548 | 1.004 | 0.991 | 1.017 | 0.006 | 0.148 | 1.006 | 0.998 | 1.015 |
| Gender (male) | 0.116 | 0.135 | 1.123 | 0.965 | 1.307 | 0.019 | 0.721 | 1.019 | 0.919 | 1.130 |
| Number of diagnosed chronic diseases | −0.036 | 0.209 | 0.965 | 0.912 | 1.020 | −0.015 | 0.413 | 0.985 | 0.951 | 1.021 |
| Depression | −0.128 | 0.000 | 0.880 | 0.856 | 0.903 | −0.098 | 0.000 | 0.906 | 0.892 | 0.921 |
| Exercise (yes) | 0.165 | 0.016 | 1.179 | 1.032 | 1.348 | 0.236 | 0.000 | 1.266 | 1.156 | 1.386 |
| Nutritional status (Good) | 1.432 | 0.000 | 4.185 | 2.783 | 6.293 | 0.780 | 0.000 | 2.181 | 1.809 | 2.630 |
| Nutritional status (Moderate) | 0.611 | 0.006 | 1.842 | 1.193 | 2.846 | 0.483 | 0.000 | 1.620 | 1.332 | 1.971 |
| Current smoking (yes) | 0.385 | 0.000 | 1.470 | 1.198 | 1.804 | 0.039 | 0.633 | 1.040 | 0.887 | 1.219 |
| Drinking frequency during the last one year | 0.053 | 0.011 | 1.054 | 1.012 | 1.098 | −0.003 | 0.866 | 0.997 | 0.968 | 1.027 |
| BMI | 0.008 | 0.561 | 1.008 | 0.981 | 1.036 | 0.017 | 0.060 | 1.017 | 0.999 | 1.035 |
| Cognitive scale | 0.040 | 0.000 | 1.041 | 1.025 | 1.057 | 0.011 | 0.020 | 1.011 | 1.002 | 1.020 |
| Fall experiences during the last one year (yes) | −0.166 | 0.310 | 0.847 | 0.615 | 1.167 | −0.042 | 0.665 | 0.959 | 0.794 | 1.159 |
| ADL | −0.158 | 0.041 | 0.854 | 0.734 | 0.994 | −0.073 | 0.008 | 0.930 | 0.881 | 0.982 |
| Annual income | 0.000 | 0.570 | 1.000 | 1.000 | 1.000 | 0.000 | 0.046 | 1.000 | 1.000 | 1.000 |
| Use of smartphones or tablet PCs (yes) | 0.212 | 0.008 | 1.236 | 1.056 | 1.448 | 0.085 | 0.111 | 1.089 | 0.981 | 1.210 |
| Likelihood ratio test chi2 | 1017.889 | |||||||||
| p | <0.001 | |||||||||
| Pseudo R2 (Nagelkerke) | 0.115 | |||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, S.; Ko, H. Social Frailty among Community-Dwelling Older Adults during the COVID-19 Pandemic in Korea: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 11963. https://doi.org/10.3390/ijerph191911963
Choi S, Ko H. Social Frailty among Community-Dwelling Older Adults during the COVID-19 Pandemic in Korea: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(19):11963. https://doi.org/10.3390/ijerph191911963
Chicago/Turabian StyleChoi, Seunghye, and Hana Ko. 2022. "Social Frailty among Community-Dwelling Older Adults during the COVID-19 Pandemic in Korea: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 19: 11963. https://doi.org/10.3390/ijerph191911963
APA StyleChoi, S., & Ko, H. (2022). Social Frailty among Community-Dwelling Older Adults during the COVID-19 Pandemic in Korea: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 19(19), 11963. https://doi.org/10.3390/ijerph191911963