
Healthcare Workers’ Emotions, Perceived Stressors, and Coping Strategies at Workplace during the COVID-19 Pandemic in Palestine

Abstract
:1. Introduction
2. Materials and Methods
2.1. Procedure
2.2. Subjects
2.3. Tool and Measures
2.4. Ethical Approval and Consent to Participate
2.5. Data Analysis
3. Results
3.1. Demographic Characteristics of the Participants
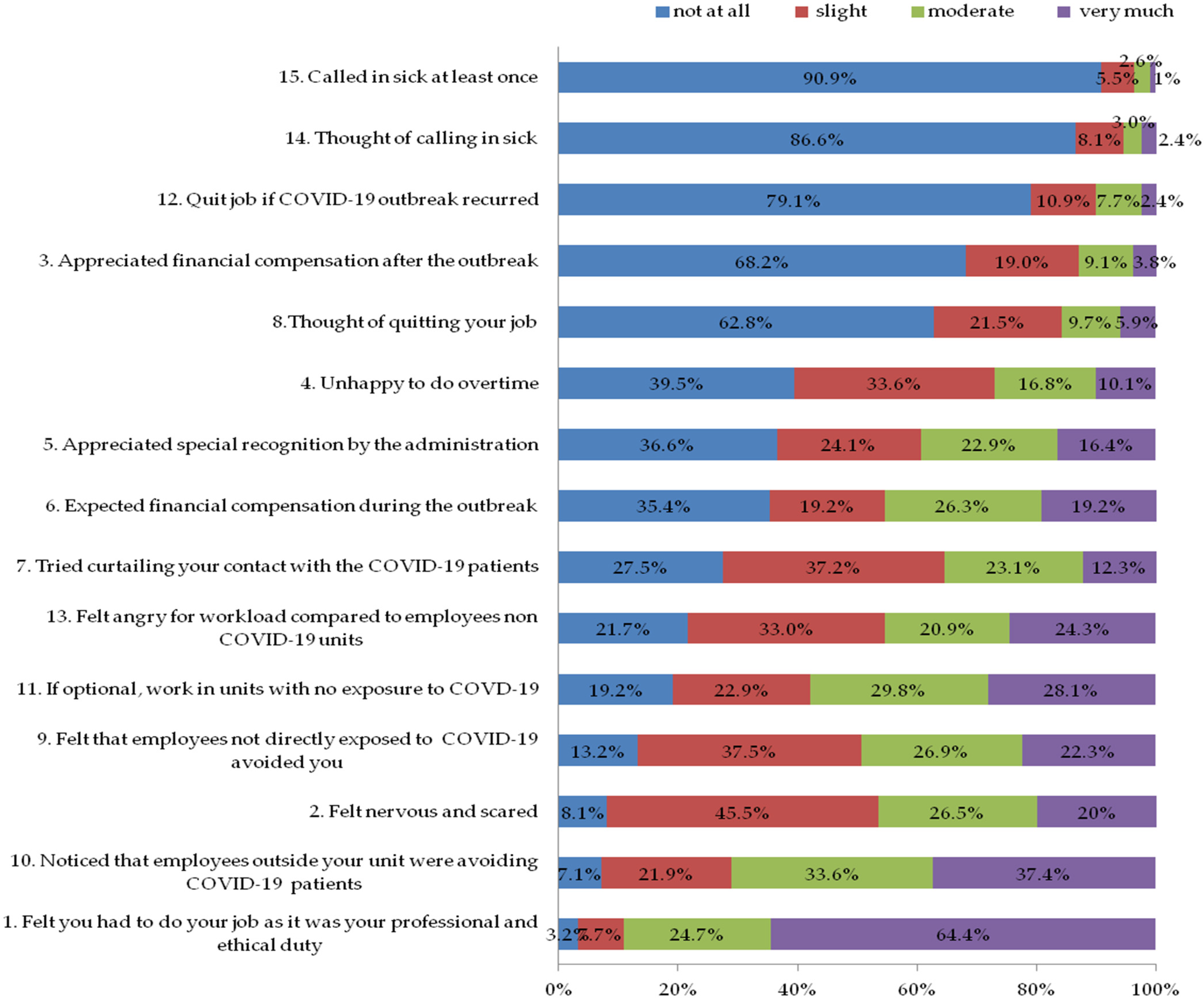
3.2. Section One: Staff’s Emotion
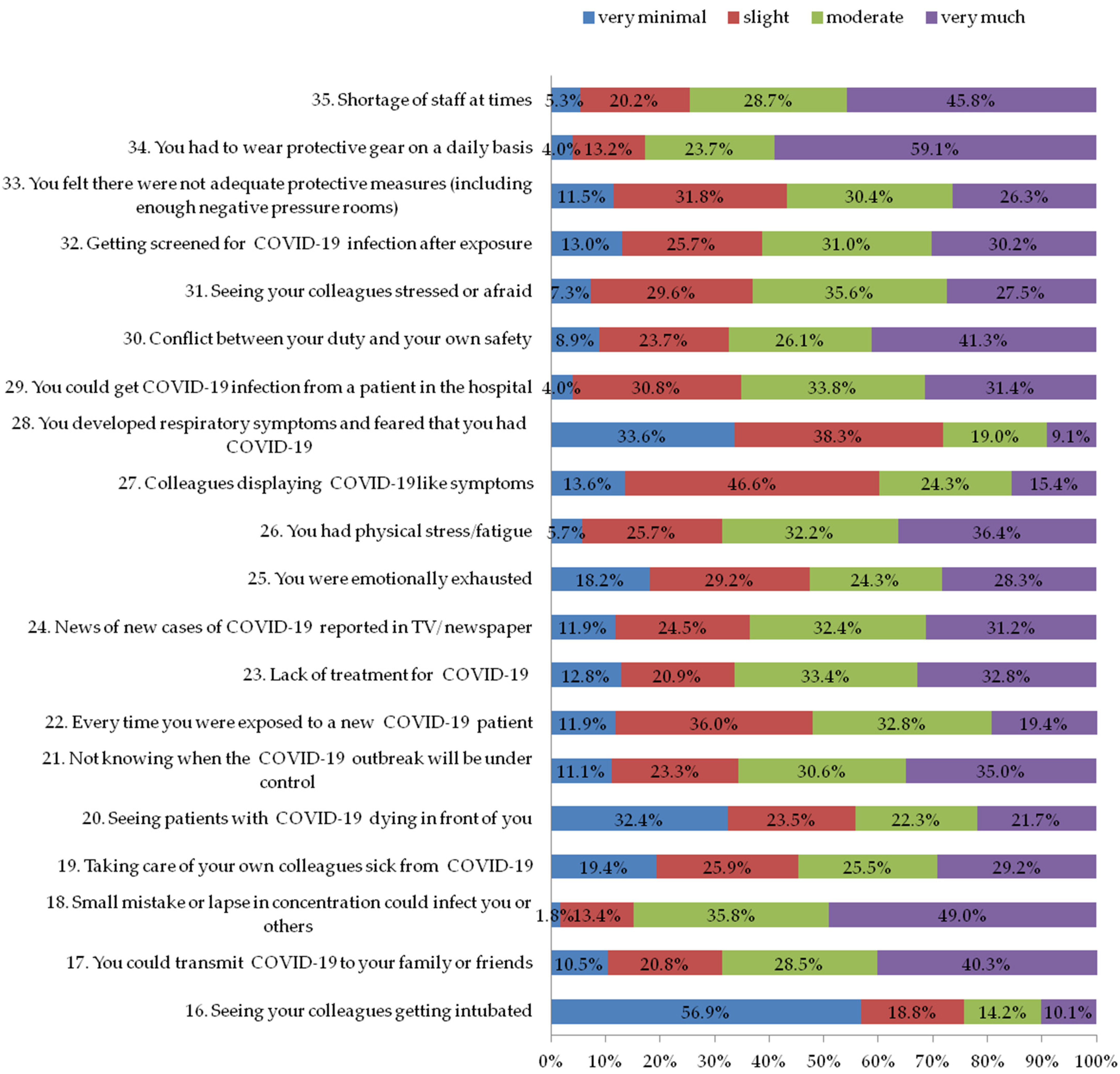
3.3. Section Two: Factors That Caused Stress among Staff during the COVID-19 Outbreak
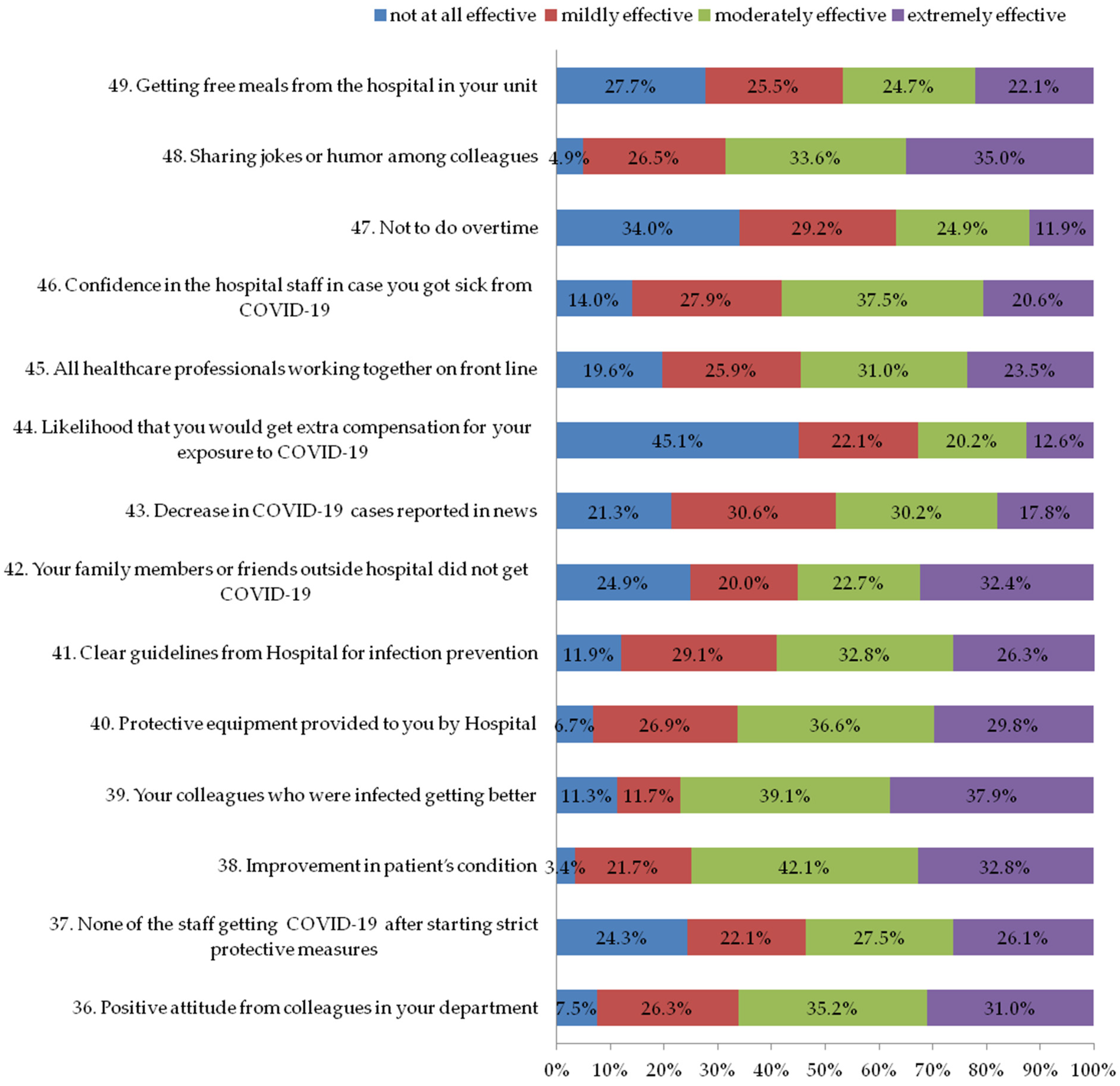
3.4. Section Three: Factors That Reduce Stress among Staff during the COVID-19 Outbreak
3.5. Section Four: Personal Coping Strategies Staff Could Have Used during the COVID-19 Outbreak
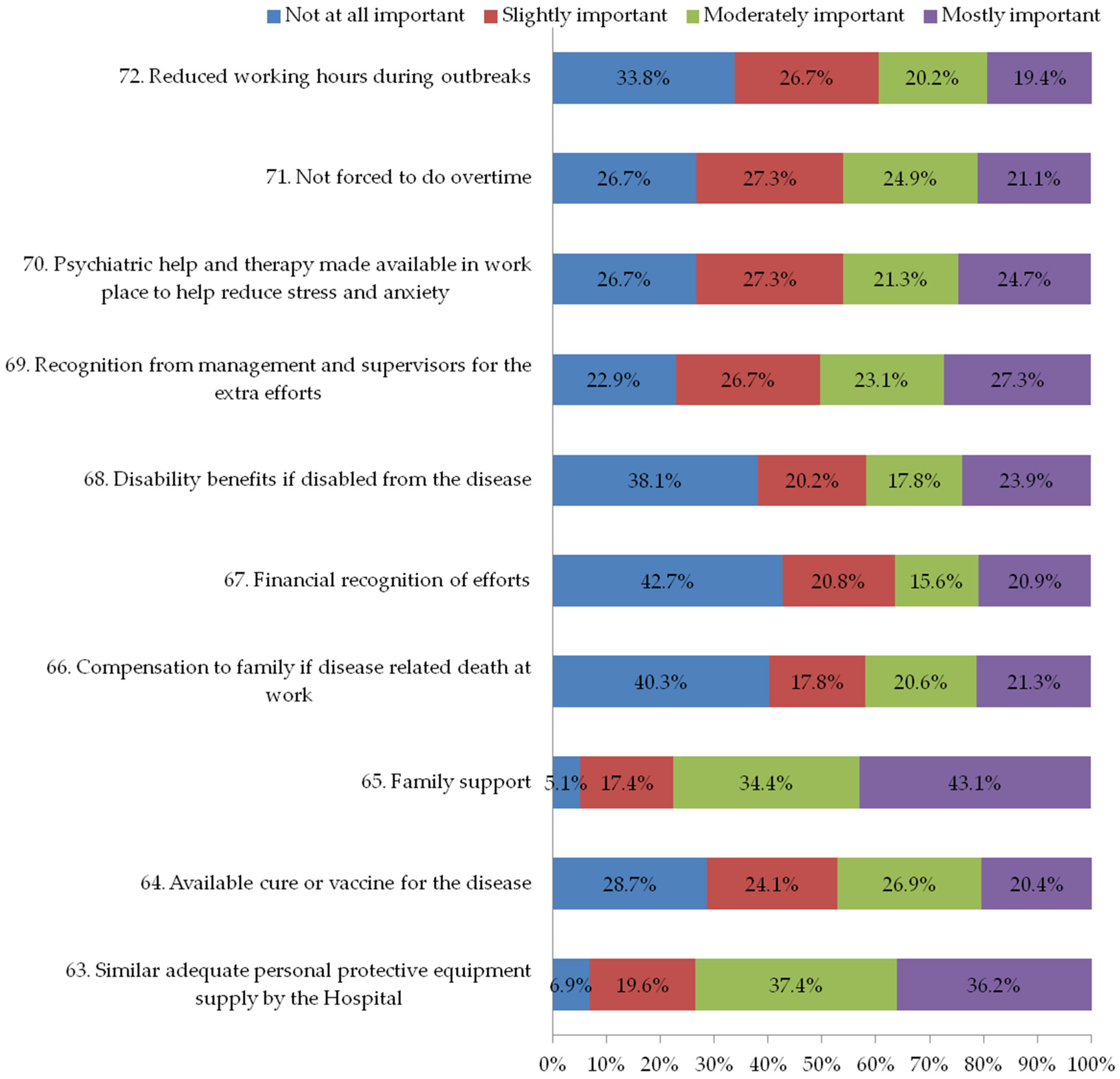
3.6. Section Five: Motivational Factors to Encourage the Continuation of Work in Future Outbreaks
3.7. Associations between Respondent Characteristics, Experience with COVID-19, Coping Strategies with Stress Score Index
3.8. Association between Coping Strategies, Motivation with Stress Scoring Index
3.9. Correlation between Stress Scoring, Coping, and Motivation Factors Scoring
4. Discussion
5. Study Limitations
6. Implications of the Study
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| COVID-19 | Coronavirus disease 2019 |
| HCWs | Healthcare workers |
| WHO | World Health Organization |
References
- Roy, A.; Singh, A.K.; Mishra, S.; Chinnadurai, A.; Mitra, A.; Bakshi, O. Mental health implications of COVID-19 pandemic and its response in India. Int. J. Soc. Psychiatry 2020, 67, 587–600. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Mental Health and COVID-19. World Health Organization: Geneva, Switzerland. 30 March 2020. Available online: http://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/novel-coronavirus-2019-ncov-technical-guidance/coronavirus-disease-covid-19-outbreak-technical-guidance-europe/mental-healthand-covid-19 (accessed on 1 February 2021).
- World Health Organization. Rolling Updates on Coronavirus Disease (COVID-19). World Health Organization: Geneva, Switzerland. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-as-they-happen (accessed on 1 February 2021).
- Khanal, P.; Devkota, N.; Dahal, M.; Paudel, K.; Joshi, D. Mental health impacts among health workers during COVID-19 in a low resource setting: A cross-sectional survey from Nepal. Global. Health 2020, 16, 89. [Google Scholar] [CrossRef] [PubMed]
- Xiang, Y.T.; Li, W.; Zhang, Q.; Jin, Y.; Rao, W.W.; Zeng, L.N.; Lok, G.K.; Chow, I.H.; Cheung, T.; Hall, B.J. Timely research papers about COVID-19 in China. Lancet 2020, 395, 684–685. [Google Scholar] [CrossRef]
- Huang, J.Z.; Han, M.F.; Luo, T.D.; Ren, A.K.; Zhou, X.P. Mental health survey of medical staff in a tertiary infectious disease hospital for COVID-19. Zhonghua Lao Dong Wei Sheng Zhi Ye Bing ZaZhi 2020, 38, 192–195. [Google Scholar] [CrossRef]
- Ran, L.; Chen, X.; Wang, Y.; Wu, W.; Zhang, L.; Tan, X. Risk Factors of Healthcare Workers With Coronavirus Disease 2019: A Retrospective Cohort Study in a Designated Hospital of Wuhan in China. Clin. Infect. Dis. 2020, 71, 2218–2221. [Google Scholar] [CrossRef]
- Zhang, C.; Yang, L.; Liu, S.; Ma, S.; Wang, Y.; Cai, Z.; Du, H.; Li, R.; Kang, L.; Su, M.; et al. Survey of Insomnia and Related Social Psychological Factors Among Medical Staff Involved in the 2019 Novel Coronavirus Disease Outbreak. Front. Psychiatry 2020, 11, 306. [Google Scholar] [CrossRef]
- Ornell, F.; Schuch, J.B.; Sordi, A.O.; Kessler, F.H.P. "Pandemic fear" and COVID-19: Mental health burden and strategies. Braz. J. Psychiatry 2020, 42, 232–235. [Google Scholar] [CrossRef]
- Giusti, E.M.; Pedroli, E.; D’Aniello, G.E.; Stramba, B.C.; Pietrabissa, G.; Manna, C.; Stramba Badiale, M.; Riva, G.; Castelnuovo, G.; Molinari, E. The Psychological Impact of the COVID-19 Outbreak on Health Professionals: A Cross-Sectional Study. Front. Psychol. 2020, 11, 1684. [Google Scholar] [CrossRef]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors Associated With Mental Health Outcomes Among Health Care Workers Exposed to Coronavirus Disease 2019. JAMA Netw. Open 2020, 3, e203976. [Google Scholar] [CrossRef]
- Tan, R.; Yu, T.; Luo, K.; Teng, F.; Liu, Y.; Luo, J.; Hu, D. Experiences of clinical first-line nurses treating patients with COVID-19: A qualitative study. J. Nurs. Manag. 2020, 28, 1381–1390. [Google Scholar] [CrossRef]
- Chan, A.O.; Huak, C.Y. Psychological impact of the 2003 severe acute respiratory syndrome outbreak on health care workers in a medium size regional general hospital in Singapore. Occup. Med. 2004, 54, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Deng, J.F.; Olowokure, B.; Kaydos-Daniels, S.C.; Chang, H.J.; Barwick, R.S.; Lee, M.L.; Deng, C.Y.; Factor, S.H.; Chiang, C.E.; Maloney, S.A.; et al. Severe acute respiratory syndrome (SARS): Knowledge, attitudes, practices and sources of information among physicians answering a SARS fever hotline service. Public Health 2006, 120, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Chan, I.; Leung, M.Y.; Liang, Q. The Roles of Motivation and Coping Behaviours in Managing Stress: Qualitative Interview Study of Hong Kong Expatriate Construction Professionals in Mainland China. Int. J. Environ. Res. Public Health 2018, 15, 561. [Google Scholar] [CrossRef]
- Herzberg, F. One More Time: How Do You Motivate Employees? Harvard Business Review: Boston, MA, USA, 1968; pp. 53–62. [Google Scholar]
- Rose, S.; Hartnett, J.; Pillai, S. Healthcare worker’s emotions, perceived stressors and coping mechanisms during the COVID-19 pandemic. PLoS ONE 2021, 16, e0254252. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Yan, X.; Zhao, S.; Wang, J.; Ran, J.; Dong, D.; Wang, M.; Fung, H.; Yeoh, E.K.; Chung, R.Y.N. Association of time to diagnosis with socioeconomic position and geographical accessibility to healthcare among symptomatic COVID-19 patients: A retrospective study in Hong Kong. Health Place 2020, 66, 102465. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health. Corona Virus (COVID 19) in Palestine. 2021. Available online: http://corona.ps (accessed on 1 February 2021).
- Folkman, S. Stress, coping, and hope. Psycho-Oncology 2010, 19, 901–908. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Kar, N. Posttraumatic Stress, Depression, and Coping Following the 2015 Nepal Earthquake: A Study on Adolescents. Disaster Med. Public Health Prep. 2019, 13, 236–242. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.A.A.; Diab, S.S.E.M.; Elmahallawy, E.K. Exploring the Psychological Stress, Anxiety Factors, and Coping Mechanisms of Critical Care Unit Nurses During the COVID-19 Outbreak in Saudi Arabia. Front. Public Health 2021, 9, 767517. [Google Scholar] [CrossRef]
- Badawy, M.K. What We’ve Learned Managing Human Resources. Res. Technol. Manag. 1988, 31, 19–35. [Google Scholar] [CrossRef]
- Folkman, S. Positive psychological states and coping with severe stress. Soc. Sci. Med. 1997, 45, 1207–1221. [Google Scholar] [CrossRef]
- Tedlie Moskowitz, J.; Folkman, S.; Collette, L.; Vittinghoff, E. Coping and mood during aids-related caregiving and bereavement. Ann. Behav. Med. 1996, 18, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Park, C.L.; Folkman, S. Meaning in the context of stress and coping. Rev. Gen. Psychol. 1997, 2, 115–144. [Google Scholar] [CrossRef]
- Lazarus, R.S. Toward better research on stress and coping. Am. Psychol. 2000, 55, 665–673. [Google Scholar] [CrossRef] [PubMed]
- Fredrickson, B.L.; Tugade, M.M.; Waugh, C.E.; Larkin, G.R. What good are positive emotions in crises? A prospective study of resilience and emotions following the terrorist attacks on the United States on September 11th, 2001. J. Pers. Soc. Psychol. 2003, 84, 365–376. [Google Scholar] [CrossRef]
- Moskowitz, J.T.; Cheung, E.O.; Freedman, M.; Fernando, C.; Zhang, M.W.; Huffman, J.C.; Addington, E.L. Measuring positive emotion outcomes in positive psychology interventions: A literature review. Emot. Rev. 2020, 13, 60–73. [Google Scholar] [CrossRef]
- Khalid, I.; Khalid, T.J.; Qabajah, M.R.; Barnard, A.G.; Qushmaq, I.A. Healthcare Workers Emotions, Perceived Stressors and Coping Strategies During a MERS-CoVOutbreak. Clin. Med. Res. 2016, 14, 7–14. [Google Scholar] [CrossRef]
- Cai, H.; Tu, B.; Ma, J.; Chen, L.; Fu, L.; Jiang, Y.; Zhuang, Q. Psychological impact and coping strategies of frontline medical staff in hunan between January and March 2020 during the outbreak of coronavirus disease 2019 (COVID-19) in Hubei, China. Med. Sci. Monit. 2020, 26, e924171. [Google Scholar] [CrossRef]
- Asmar, I.T.; Naseef, H.; Al-Shami, N.; Jaghama, M.K.; Abukhalil, A.D.; Karsh, A.A.; AlFayyah, F.A.; Dagher, R.A.M. Impact ofCOVID-19 pandemic on the psychological status of Palestinian adults inthe West Bank, Palestine: A cross-sectional study. Open Psychol. J. 2021, 14, 227–237. [Google Scholar] [CrossRef]
- AlKhaldi, M.; Kaloti, R.; Shella, D.; Al Basuoni, A.; Meghari, H. Health system’s response to the COVID-19 pandemic in conflict settings: Policy reflections from Palestine. Glob. Public Health 2020, 15, 1244–1256. [Google Scholar] [CrossRef]
- El Sharif, N.; Ahmead M and Imam, A. COVID-19 infection prevention and control procedures and institutional trust: Perceptions of Palestinian healthcare workers. Front. Public Health 2022, 10, 947593. [Google Scholar] [CrossRef]
- Maraqa, B.; Nazzal, Z.; Zink, T. Palestinian health care workers’ stress and stressors during COVID-19 pandemic: A cross-sectional study. J. Prim. Care Community Health 2020, 11, 2150132720955026. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Juang, Y.Y.; Su, Y.J.; Lee, H.L.; Lin, Y.H.; Chao, C.C. Facing SARS: Psychological impacts on SARS team nurses and psychiatric services in a Taiwan general hospital. Gen. Hosp. Psychiatry 2005, 27, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Aly, H.M.; Nemr, N.A.; Kishk, R.M.; Elsaid, N.M.A.B. Stress, anxiety and depression among healthcare workers facing COVID-19 pandemic in Egypt: A cross-sectional online-based study. BMJ Open 2021, 11, e045281. [Google Scholar] [CrossRef] [PubMed]
- .Akshaya, S.B.; Wafa, A.A.; Jamal, R.; Mohammadjavad, A.M.; Deepak, K.B. Knowledge and perceptions of COVID-19 among health care workers: Cross-sectional study. JMIR Public Health Surveill. 2020, 6, e19160. [Google Scholar]
- Spoorthy, M.S. Mental health problems faced by healthcare workers due to the COVID-19 pandemic—A review. Asian J. Psychiatr. 2020, 51, 102119. [Google Scholar] [CrossRef]
- Alnazly, E.; Khraisat, O.M.; Al-Bashaireh, A.M.; Bryant, C.L. Anxiety, Depression, Stress, Fear and Social Support during COVID-19 Pandemic among Jordanian Healthcare Workers. PLoS ONE 2021, 16, e0247679. [Google Scholar] [CrossRef]
- Koh, D.; Lim, M.K.; Chia, S.E.; Ko, S.M.; Qian, F.; Ng, V.; Tan, B.H.; Wong, K.S.; Chew, W.M.; Tang, H.K.; et al. Risk perception and impact of Severe Acute Respiratory Syndrome (SARS) on work and personal lives of healthcare workers in Singapore: What can we learn? Med. Care. 2005, 43, 676–682. [Google Scholar] [CrossRef]
- Mohsin, S.F.; Agwan, M.A.; Shaikh, S.; Alsuwaydani, Z.A.; AlSuwaydani, S.A. COVID-19: Fear and Anxiety among Healthcare Workers in Saudi Arabia. A Cross-Sectional Study. Inquiry 2021, 58, 469580211025225. [Google Scholar] [CrossRef]
- Ives, J.; Greenfield, S.; Parry, J.M.; Draper, H.; Gratus, C.; Petts, J.I.; Sorell, T.; Wilson, S. Healthcare workers’ attitudes to working during pandemic influenza: A qualitative study. BMC Public Health 2009, 9, 56. [Google Scholar] [CrossRef]
- Fernandez, R.; Lord, H.; Halcomb, E.; Moxham, L.; Middleton, R.; Alananzeh, I.; Ellwood, L. Implications for COVID-19: A systematic review of nurses’ experiences of working in acute care hospital settings during a respiratory pandemic. Int. J. Nurs. Stud. 2020, 111, 103637. [Google Scholar] [CrossRef]
- Aldarmasi, M.A.; Alghamdi, A.H. Factors Influencing Stress Perception among Healthcare Workers during the Coronavirus Pandemic: A Multi-centric Cross-sectional Study. Int. J. Med. Res. Health Sci. 2021, 10, 142–149. [Google Scholar]
- Ilczak, T.; Rak, M.; Ćwiertnia, M.; Mikulska, M.; Waksmańska, W.; Krakowiak, A.; Bobiński, R.; Kawecki, M. Predictors of stress among emergency medical personnel during the COVID-19 pandemic. Int. J. Occup. Med. Environ. Health 2021, 34, 139–149. [Google Scholar] [CrossRef] [PubMed]
- Supratman, S.; Mastuti, D.; Widodo, A.; Rosyid, F.N. Occupational Stress among Health Professional during COVID-19 Pandemic. In Proceedings of the International Conference on Health and Well Being, Tomsk, Russia, 29–30 July 2020; pp. 98–106. Available online: https://publikasiilmiah.ums.ac.id/xmlui/bitstream/handle/11617/12401/ichwb-13.pdf?sequence=3&isAllowed=y (accessed on 1 August 2022).
- Elbqry, M.G.; Elmansy, F.M.; Elsayed, A.E.; Mansour, B.; Tantawy, A.; Eldin, M.B.; Sayed, H.H. Effect of COVID-19 stressors on healthcare workers’ performance and attitude at Suez Canal university hospitals. Middle East Curr. Psychiatry 2021, 28, 4. [Google Scholar] [CrossRef]
- Windarwati, H.D.; Ati, N.A.L.; Paraswati, M.D.; Ilmy, S.K.; Supianto, A.A.; Rizzal, A.F.; Sulaksono, A.D.; Lestari, R.; Supriati, L. Stressor, coping mechanisms, and motivation among health care workers in dealing with stress due to the COVID-19 pandemic in Indonesia. Asian J. Psychiatr. 2021, 56, 102470. [Google Scholar] [CrossRef]
- Chen, Q.; Liang, M.; Li, Y.; Guo, J.; Fei, D.; Wang, L.; He, L.I.; Sheng, C.; Cai, Y.; Li, X.; et al. Mental health care for medical staff in China during the COVID-19 outbreak. Lancet Psychiatry 2020, 7, e15–e16. [Google Scholar] [CrossRef]
- ANERA. Health Care System in Palestine. Available online: https://www.anera.org/blog/heathcare-in-palestine/September (accessed on 1 August 2022).
- Alser, O.; Alghoul, H.; Alkhateeb, Z.; Hamdan, A.; Albarqouni, L.; Saini, K. Healthcare workers preparedness for COVID-19 pandemic in the occupied Palestinian territory: A cross-sectional survey. BMC Health Serv. Res. 2021, 21, 766. [Google Scholar] [CrossRef]
- Hope, K.; Massey, P.D.; Osbourn, M.; Durrheim, D.N.; Kewley, C.D.; Turner, C. Senior clinical nurses effectively contribute to the pandemic influenza public health response. Aust. J. Adv. Nurs. 2021, 28, 47–53. [Google Scholar]
- Lam, K.K.; Hung, S.Y.M. Perceptions of emergency nurses during the human swine influenza outbreak: A qualitative study. Int. Emerg. Nurs. 2013, 21, 240–246. [Google Scholar] [CrossRef]
- Koh, Y.; Hegney, D.; Drury, V. Nurses’ perceptions of risk from emerging respiratory infectious diseases: A Singapore study. Int. J. Nurs. Pract. 2012, 18, 195–204. [Google Scholar] [CrossRef]
- Barth, A.; Egger, A.; Hladschik-Kermer, B.; Kropiunigg, U. Tränen im Krankenhaus-Eine Bestandsaufnahme unter Ärzten, Pflegepersonal und Medizinstudenten. Psychother. Psychosom. Med. Psychol. 2004, 54, 194–197. [Google Scholar] [CrossRef]
- Wagner, R.E.; Hexel, M.; Bauer, W.W.; Kropiunigg, U. Crying in hospitals: A survey of doctors’, nurses’ and medical students’ experience and attitudes. Z. Für Med. Ausbild. 1997, 6, 13–16. [Google Scholar] [CrossRef] [PubMed]
- Gračanin, A.; Bylsma, L.; Vingerhoets, A.J. Why only humans shed emotional tears: Evolutionary and cultural perspectives. Hum. Nat. 2018, 29, 104–133. [Google Scholar] [CrossRef]
- Angoff, N.R. Crying in the curriculum. JAMA 2001, 286, 1017–1018. [Google Scholar] [CrossRef] [PubMed]
- Kukulu, K.; Keser, I. Medical and nursing students crying in hospital settings. J. Nurs. Educ. 2006, 45, 426. [Google Scholar] [PubMed]
- Lerner, B.H. At Bedside, Stay Stoic or Display Emotions? [Online blog]. Retrieved 28 August 2017. 2008. Available online: http://www.nytimes.com/2008/04/22/health/views/22essa.html (accessed on 1 July 2022).
- Veronese, G.; Mahamid, F.A.; Bdier, D. Subjective well-being, sense of coherence, and posttraumatic growth mediate the association between COVID-19 stress, trauma, and burnout among Palestinian health-care providers. Am. J. Orthopsychiatry 2022, 92, 291–301. [Google Scholar] [CrossRef]
- Liu, Y.; Chen, H.; Zhang, N.; Wang, X.; Fan, Q.; Zhang, Y.; Huang, L.; Hu, B.; Li, M. Anxiety and depression symptoms of medical staff under COVID-19 epidemic in China. J. Affect. Disord. 2021, 278, 144–148. [Google Scholar] [CrossRef]
- Vicente, V.; Jansson, J.; Wikström, M.; Danehorn, E.; Wahlin, R.R. Prehospital Emergency Nurses’ coping strategies associated to traumatic experiences. Int. Emerg. Nurs. 2021, 59, 101083. [Google Scholar] [CrossRef]
- Liu, Q.; Luo, D.; Haase, J.E.; Guo, Q.; Wang, X.Q.; Liu, S.; Xia, L.; Liu, Z.; Yang, J.; Yang, B.X. The experiences of health-care providers during the COVID-19 crisis in China: A qualitative study. Lancet Glob. Health 2020, 8, e790–e798. [Google Scholar] [CrossRef]
- Nzaji, M.K.; Ngombe, L.K.; Mwamba, G.N.; Ndala, D.B.B.; Miema, J.M.; Lungoyo, C.L.; Mwimba, B.L.; Bene, A.C.M.; Musenga, E.M. Acceptability of Vaccination against COVID-19 among Healthcare Workers in the Democratic Republic of the Congo. Pragmat. Obs. Res. 2020, 11, 103–109. [Google Scholar] [CrossRef]
- Shekhar, R.; Sheikh, A.B.; Upadhyay, S.; Singh, M.; Kottewar, S.; Mir, H.; Barrett, E.; Pal, S. COVID-19 Vaccine Acceptance among Health Care Workers in the United States. Vaccines 2021, 9, 119. [Google Scholar] [CrossRef]
- Rajkumar, R.P. COVID-19 and mental health: A review of the existing literature. Asian J. Psychiatr. 2020, 52, 102066. [Google Scholar] [CrossRef] [PubMed]
- Kang, L.; Li, Y.; Hu, S.; Chen, M.; Yang, C.; Yang, B.X.; Wang, Y.; Hu, J.; Lai, J.; Ma, X.; et al. The mental health of medical workers in Wuhan, China dealing with the 2019 novel coronavirus. Lancet Psychiatry 2020, 7, e14. [Google Scholar] [CrossRef]
- Phua, D.H.; Tang, H.K.; Tham, K.Y. Coping responses of emergency physicians and nurses to the 2003 severe acute respiratory syndrome outbreak. Acad. Emerg. Med. 2005, 12, 322–328. [Google Scholar] [CrossRef] [PubMed]
- Yin, H.; Huang, S.; Lv, L. A multilevel analysis of job characteristics, emotion regulation, and teacher well-being: A job demands-resources model. Front. Psychol. 2018, 9, 2395. [Google Scholar] [CrossRef] [PubMed]
- Martínez, J.P.; Méndez, I.; Ruiz-Esteban, C.; Fernández-Sogorb, A.; García-Fernández, J.M. Profiles of Burnout, Coping Strategies and Depressive Symptomatology. Front. Psychol. 2020, 11, 591. [Google Scholar] [CrossRef]
- Babore, A.; Lombardi, L.; Viceconti, M.L.; Pignataro, S.; Marino, V.; Crudele, M.; Candelori, C.; Bramanti, S.M.; Trumello, C. Psychological effects of the COVID-2019 pandemic: Perceived stress and coping strategies among healthcare professionals. Psychiatry Res. 2020, 293, 113366. [Google Scholar] [CrossRef]
- Healy, S.; Tyrrell, M. Stress in emergency departments: Experiences of nurses and doctors. Emerg. Nurse 2011, 19, 31–37. [Google Scholar] [CrossRef]
- Xu, H.G.; Johnston, A.N.; Greenslade, J.H.; Wallis, M.; Elder, E.; Abraham, L.; Thom, O.; Carlstrom, E.; Crilly, J. Stressors and coping strategies of emergency department nurses and doctors: A cross-sectional study. Australas. Emerg. Care 2019, 22, 180–186. [Google Scholar] [CrossRef]
- Wong, T.W.; Yau, J.K.; Chan, C.L.; Kwong, R.S.; Ho, S.M.; Lau, C.C.; Lit, C.H. The psychological impact of severe acute respiratory syndrome outbreak on healthcare workers in emergency departments and how they cope. Eur. J. Emerg. Med. 2005, 12, 13–18. [Google Scholar] [CrossRef]
- Smith, G.P. Motivation. In Human Resources Management and Development Handbook, 2nd ed.; Tracey, W., Ed.; Free Press: New York, NY, USA, 2014. [Google Scholar]
- Kakkos, N.; Trivellas, P. Investigating the link between motivation, work stress and job performance. Evidence from the banking industry. In Proceedings of the 8th International Conference on Enterprise Systems, Accounting and Logistics (8th ICESAL ’11), Thassos, Greece, 10–12 July 2011; pp. 408–428. [Google Scholar]
- Park, J.; Chung, S.; An, H.; Park, S.; Lee, C.; Kim, S.Y.; Lee, J.D.; Kim, K.S. A structural model of stress, motivation, and academic performance in medical students. Psychiatry Investig. 2012, 9, 143–149. [Google Scholar] [CrossRef]
- Chen, T.L.; Huang, M.Y.; Su, T.H. Work motivation, work stress, and job satisfaction in between Taiwan and China–An empirical study. World Acad. Sci. Eng. Tech. 2012, 68, 1446–1450. [Google Scholar]
- Saleem, M.; Tufail, M.W.; Atta, A.; Asghar, S. Innovative workplace behavior, motivation level, and perceived stress among healthcare employees. Pak. J. Commer. Soc. Sci. 2015, 9, 438–446. [Google Scholar]
- Chew, B.H.; Ramli, A.S.; Omar, M.; Ismail, I.Z. A preliminary study of job satisfaction and motivation among the Malaysian primary healthcare professionals. Malays. Fam. Physician Off. J. Acad. Fam. Physicians Malays. 2013, 8, 15–25. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| F | % | ||
|---|---|---|---|
| Gender | Female | 77 | 15.2% |
| Male | 429 | 84.8% | |
| Age | 20–30 years | 276 | 54.5% |
| 31–40 years | 158 | 31.2% | |
| 41–50 years | 60 | 11.9% | |
| >50 years | 12 | 2.4% | |
| Marital Status | Single | 190 | 37.5% |
| Married | 309 | 61.1% | |
| Divorced | 7 | 1.4% | |
| Place of Residence | Village | 212 | 41.9 |
| City | 232 | 45.8 | |
| Camp | 62 | 12.3 | |
| Occupation | Physician | 158 | 31.3% |
| Nurse | 348 | 68.7% | |
| Area | West Bank | 303 | 59.9% |
| Jerusalem | 59 | 11.7% | |
| Gaza Strip | 144 | 28.5% | |
| Monthly Income | <1000$ | 164 | 32.4% |
| 1000–1500$ | 262 | 51.8% | |
| 1500–2100$ | 67 | 13.2% | |
| >2100 $ | 13 | 2.6% | |
| Place of COVID-19 work | Special treatment centers | 139 | 27.5% |
| Hospitals | 309 | 61.1% | |
| Quarantine hotels | 8 | 1.6% | |
| Work in more than one treatment place | 50 | 9.9% | |
| Was this your first time working with COVID-19 patients? | No | 117 | 23.1% |
| Yes | 389 | 76.9% | |
| Did you receive training to deal with COVID-19 patients? | No | 310 | 61.3 |
| Yes | 196 | 38.7 | |
| Did you receive training to treat COVID-19 patients? | No | 286 | 56.5% |
| Yes | 196 | 38.7% | |
| Can not remember | 24 | 4.7% | |
| Your work with COVID-19 patients in treatment centers is | Compulsory | 370 | 73.1% |
| Voluntary | 96 | 19.0% | |
| Other | 40 | 7.9% | |
| Stress Index | Adjusted Analysis * | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ≤27 Low n= 130 | 28–43 Moderate n = 254 | >43 High n = 122 | p Value | 95% Wald Confidence Interval for Exp (B) | ||||||||
| n | % | n | % | n | % | Sig. | Sig. | Exp (B) | Lower | Upper | ||
| Age | 20–30 years | 50 | 38.5 | 149 | 58.7 | 77 | 63.1 | 0.02 | 0.034 | 0.25 | 0.07 | 0.90 |
| 31–40 years | 54 | 41.5 | 72 | 28.3 | 32 | 26.2 | 0.073 | 0.54 | 0.27 | 1.05 | ||
| 41–50 years | 20 | 15.4 | 29 | 11.4 | 11 | 9.0 | 0.002 | 0.46 | 0.29 | 0.75 | ||
| >50 years | 6 | 4.6 | 4 | 1.6 | 2 | 1.6 | Ref. | |||||
| Occupation †† | Physician | 55 | 42.3 | 76 | 30.0 | 27 | 22.1 | 0.007 | 0.00 | 2.38 | 1.14 | 4.97 |
| Nurse | 65 | 50.0 | 160 | 63.2 | 81 | 66.4 | 0.01 | 2.14 | 1.34 | 3.41 | ||
| Other | 10 | 7.7 | 17 | 6.7 | 14 | 11.5 | Ref. | |||||
| Place of COVID-19 work | COVID-19 treatment centers | 45 | 34.6 | 72 | 28.3 | 22 | 18.0 | 0.19 | 1.66 | 0.86 | 3.20 | |
| COVID-19 hospitals | 67 | 51.5 | 154 | 60.6 | 88 | 72.1 | 0.057 | 0.81 | 0.84 | 0.21 | 3.26 | |
| COVID-19 quarantine hotels | 3 | 2.3 | 4 | 1.6 | 1 | 0.8 | 0.03 | 1.58 | 1.03 | 2.43 | ||
| More than one treatment place | 15 | 11.5 | 24 | 9.4 | 11 | 9.0 | Ref. | |||||
| Did you receive training to treat COVID-19 patients? | No | 53 | 40.8 | 148 | 58.3 | 85 | 69.7 | 000 | 0.74 | 0.84 | 0.30 | 2.35 |
| Yes | 69 | 53.1 | 99 | 39.0 | 28 | 23.0 | 0.001 | 0.41 | 0.25 | 0.68 | ||
| Can’t remember | 8 | 6.2 | 7 | 2.8 | 9 | 7.4 | Ref. | |||||
| Stress Index | Adjusted Analysis * | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ≤27 Low n = 130 | 28–43 Moderate n = 254 | >43 High n = 122 | p Value | 95% Wald Confidence Interval for AOR | ||||||||
| n | % | n | % | n | % | Sig. | Sig. | AOR | Lower | Upper | ||
| Model 1: Coping strategies * | ||||||||||||
| 52. Considered every patient admitted to the hospital as having COVID-19 infection and using full protective gear even if patient was COVID-19 negative | Never | 8 | 6.2 | 10 | 3.9 | 8 | 6.6 | 0.09 | 0.91 | 0.99 | 0.72 | 1.35 |
| Sometimes | 21 | 16.2 | 32 | 12.6 | 10 | 8.2 | 0.04 | 0.79 | 0.63 | 0.99 | ||
| Often | 51 | 39.2 | 85 | 33.5 | 30 | 24.6 | 0.01 | 0.84 | 0.72 | 0.97 | ||
| Always | 50 | 38.5 | 127 | 50.0 | 74 | 60.7 | Ref. | |||||
| 54. Avoided going out in public places to minimize exposure from COVID-19 | Never | 13 | 10.0 | 7 | 2.8 | 3 | 2.5 | 0.002 | 0.04 | 0.67 | 0.48 | 0.94 |
| Sometimes | 34 | 26.2 | 49 | 19.3 | 18 | 14.8 | 0.29 | 0.87 | 0.71 | 1.07 | ||
| Often | 47 | 36.2 | 99 | 39.0 | 47 | 38.5 | 0.92 | 0.99 | 0.85 | 1.17 | ||
| Always | 36 | 27.7 | 99 | 39.0 | 54 | 44.3 | Ref. | |||||
| 61. Avoided media news about COVID-19 and related fatalities | Never | 33 | 25.4 | 56 | 22.0 | 23 | 18.9 | 0.000 | 0.50 | 0.93 | 0.74 | 1.18 |
| Sometimes | 65 | 50.0 | 94 | 37.0 | 36 | 29.5 | 0.01 | 0.80 | 0.65 | 0.99 | ||
| Often | 19 | 14.6 | 72 | 28.3 | 35 | 28.7 | 0.57 | 0.94 | 0.75 | 1.16 | ||
| Always | 13 | 10.0 | 32 | 12.6 | 28 | 23.0 | Ref. | |||||
| 62. Vented emotions by crying, screaming etc. | Never | 87 | 66.9 | 157 | 61.8 | 63 | 51.6 | 0.002 | 0.03 | 0.76 | 0.59 | 0.99 |
| Sometimes | 29 | 22.3 | 56 | 22.0 | 25 | 20.5 | 0.33 | 0.87 | 0.66 | 1.15 | ||
| Often | 8 | 6.2 | 30 | 11.8 | 17 | 13.9 | 0.93 | 0.99 | 0.73 | 1.33 | ||
| Always | 6 | 4.6 | 11 | 4.3 | 17 | 13.9 | Ref. | |||||
| Model 2: Motivation ** | ||||||||||||
| 64. Available cure or vaccine for the disease | Never | 24 | 18.5 | 74 | 29.1 | 47 | 38.5 | 000 | 0.07 | 1.22 | 0.981 | 1.51 |
| Sometimes | 41 | 31.5 | 62 | 24.4 | 19 | 15.6 | 0.80 | 0.97 | 0.77 | 1.21 | ||
| Often | 48 | 36.9 | 65 | 25.6 | 23 | 18.9 | 0.19 | 0.86 | 0.70 | 1.07 | ||
| Always | 17 | 13.1 | 53 | 20.9 | 33 | 27.0 | Ref. | |||||
| 65. Family support | Never | 8 | 6.2 | 9 | 3.5 | 9 | 7.4 | 0.001 | 0.73 | 0.95 | 0.71 | 1.26 |
| Sometimes | 28 | 21.5 | 49 | 19.3 | 11 | 9.0 | 0.003 | 0.76 | 0.63 | 0.91 | ||
| Often | 55 | 42.3 | 85 | 33.5 | 34 | 27.9 | 0.05 | 0.86 | 0.74 | 1.00 | ||
| Always | 39 | 30.0 | 111 | 43.7 | 68 | 55.7 | Ref. | |||||
| 66. Compensation to family if disease-related death at work | Never | 52 | 40.0 | 101 | 39.8 | 51 | 41.8 | 0.000 | 0.22 | 0.85 | 0.66 | 1.08 |
| Sometimes | 29 | 22.3 | 49 | 19.3 | 12 | 9.8 | 0.34 | 0.88 | 0.68 | 1.19 | ||
| Often | 29 | 22.3 | 58 | 22.8 | 17 | 13.9 | 0.42 | 0.90 | 0.71 | 1.15 | ||
| Always | 20 | 15.4 | 46 | 18.1 | 42 | 34.4 | Ref. | |||||
| 67. Financial recognition of efforts | Never | 49 | 37.7 | 117 | 46.1 | 50 | 41.0 | 000 | 0.020 | 0.75 | 0.58 | 0.97 |
| Sometimes | 42 | 32.3 | 52 | 20.5 | 11 | 9.0 | 0.004 | 0.70 | 0.55 | 0.89 | ||
| Often | 24 | 18.5 | 38 | 15.0 | 17 | 13.9 | 0.080 | 0.81 | 0.64 | 1.03 | ||
| Always | 15 | 11.5 | 47 | 18.5 | 44 | 36.1 | Ref. | |||||
| 69. Recognition from management and supervisors for the extra efforts | Never | 22 | 16.9 | 57 | 22.4 | 37 | 30.3 | 0.023 | 0.01 | 1.40 | 1.07 | 1.81 |
| Sometimes | 39 | 30.0 | 65 | 25.6 | 31 | 25.4 | 0.03 | 1.26 | 1.01 | 1.58 | ||
| Often | 38 | 29.2 | 63 | 24.8 | 16 | 13.1 | 0.25 | 1.12 | 0.91 | 1.38 | ||
| Always | 31 | 23.8 | 69 | 27.2 | 38 | 31.1 | Ref. | |||||
| 72. Reduced working hours during outbreaks | Never | 38 | 29.2 | 88 | 34.6 | 45 | 36.9 | 0000 | 0.21 | 0.85 | 0.66 | 1.09 |
| Sometimes | 48 | 36.9 | 73 | 28.7 | 14 | 11.5 | 0.01 | 0.72 | 0.57 | 0.93 | ||
| Often | 30 | 23.1 | 48 | 18.9 | 24 | 19.7 | 0.28 | 0.87 | 0.68 | 1.11 | ||
| Always | 14 | 10.8 | 45 | 17.7 | 39 | 32.0 | Ref. | |||||
| Mean | Std. Deviation | Correlation Coefficient with Stress Scoring | Adjusted Analysis * with Stress Index | |||||
|---|---|---|---|---|---|---|---|---|
| Spearman’s rho | Significance | Sig. | ||||||
| Coping scoring | 23.3 | 6.86 | 0.25 | 0.000 | 0.000 | 1.06 | 1.03 | 1.09 † |
| Motivation scoring | 14.8 | 8.19 | 0.067 | 0.14 | 0.078 | 1.02 | 0.99 | 1.04 ‡ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmead, M.; El Sharif, N.; Asad, S. Healthcare Workers’ Emotions, Perceived Stressors, and Coping Strategies at Workplace during the COVID-19 Pandemic in Palestine. Int. J. Environ. Res. Public Health 2022, 19, 11966. https://doi.org/10.3390/ijerph191911966
Ahmead M, El Sharif N, Asad S. Healthcare Workers’ Emotions, Perceived Stressors, and Coping Strategies at Workplace during the COVID-19 Pandemic in Palestine. International Journal of Environmental Research and Public Health. 2022; 19(19):11966. https://doi.org/10.3390/ijerph191911966
Chicago/Turabian StyleAhmead, Muna, Nuha El Sharif, and Samer Asad. 2022. "Healthcare Workers’ Emotions, Perceived Stressors, and Coping Strategies at Workplace during the COVID-19 Pandemic in Palestine" International Journal of Environmental Research and Public Health 19, no. 19: 11966. https://doi.org/10.3390/ijerph191911966
APA StyleAhmead, M., El Sharif, N., & Asad, S. (2022). Healthcare Workers’ Emotions, Perceived Stressors, and Coping Strategies at Workplace during the COVID-19 Pandemic in Palestine. International Journal of Environmental Research and Public Health, 19(19), 11966. https://doi.org/10.3390/ijerph191911966