
Cohort Profile: The Assessing Economic Transitions (ASSET) Study—A Community-Based Mixed-Methods Study of Economic Engagement among Inner-City Residents

 , ,
, ,
Abstract
1. Introduction
2. Cohort Description
2.1. Cohort Setting
2.2. Objectives and Study Design
2.3. Eligibility and Recruitment
2.4. Data Collection and Follow-Up
3. Study Measures
3.1. Survey Measures
3.2. Qualitative Concepts
3.3. Statistical Analyses
4. Findings to Date
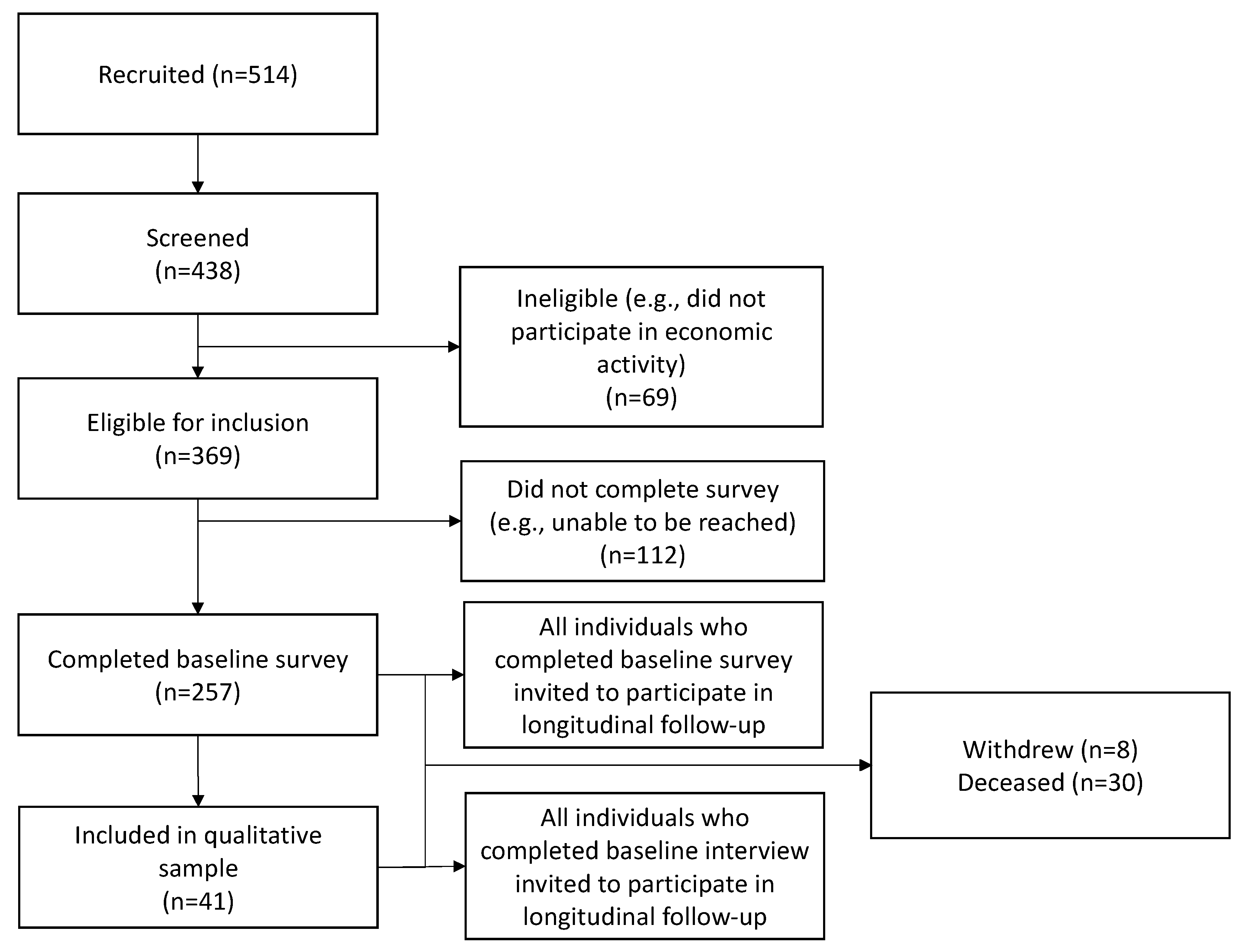
4.1. Recruitment and Retention
4.2. Cohort Characteristics
4.3. Substance Use, Health, and Well-Being
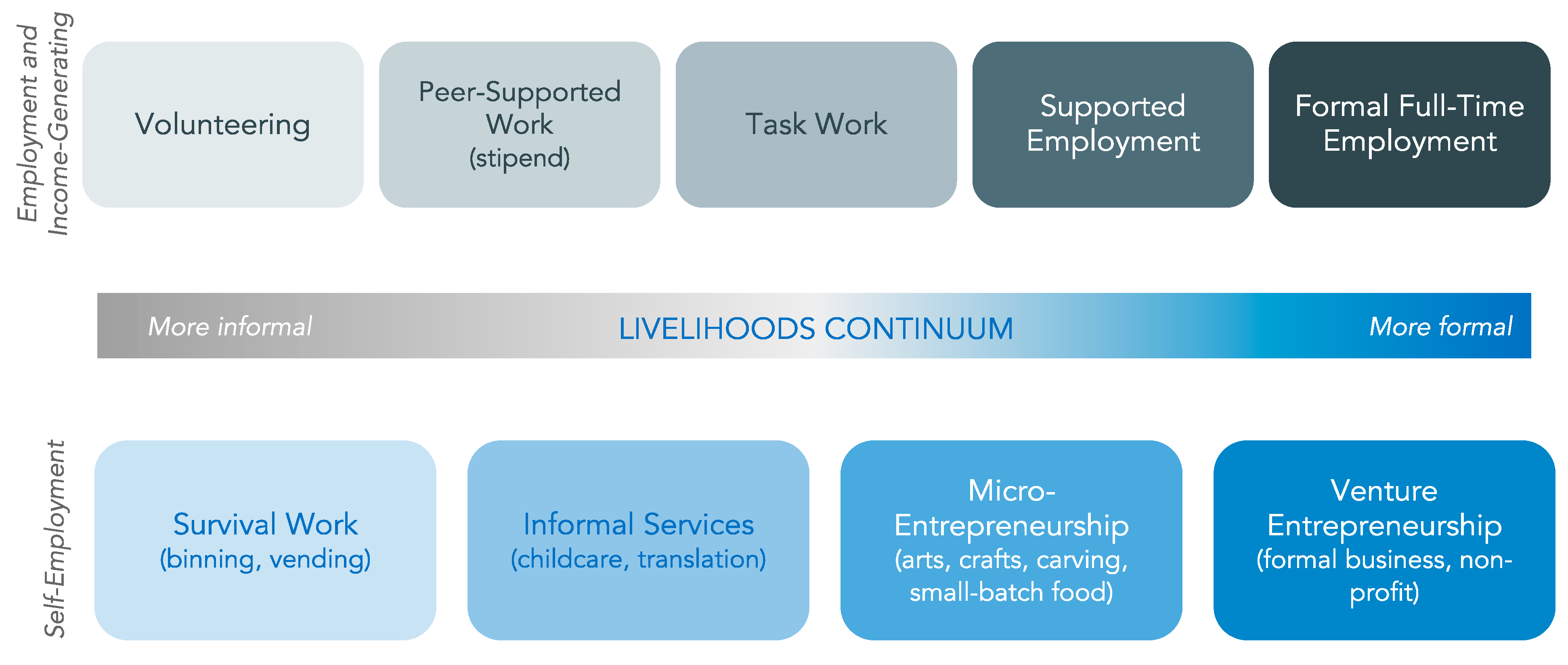
4.4. Economic Engagement
5. Discussion
Future Plans
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| BL | FUP | EXIT | ||
|---|---|---|---|---|
| Demographics & Background | ||||
| A1 | Age | x | ||
| A1 | Ethnicity | x | ||
| A2 | Gender identity | x | ||
| A3 | Relationship status | x | x | x |
| A4 | Immigration (place of birth) | x | ||
| A6 | Re-location | x | x | x |
| A6 | Neighbourhood | x | x | x |
| A7 | Co-habitation | x | x | x |
| A9 | Housing type and stability | x | x | x |
| Community Connectedness | ||||
| B1-2 | Community Involvement Measure | x | x | x |
| B3 | Social Inclusion Scale | x | x | x |
| B4 | Neighbourhood Cohesion | x | x | x |
| Economic Participation & Employment | ||||
| C2 | Employment Precarity | x | x | x |
| C11 | Unemployment/non-participation | x | ||
| C4 | Government assistance | x | x | x |
| C1 | Income Generation (across continuum) | x | x | x |
| C3 | Employment—formal & informal | x | x | x |
| C12 | Disruptive Events | x | x | x |
| C9 | Monthly Total Income, Allocation of monies | x | x | x |
| Work Intentions and Barriers | ||||
| D(1-6) | Perceptions of work: motivation to work, benefits of work (manifest and latent benefits) | x | x | x |
| D7 | Barriers to work | x | x | x |
| D8 | Perceived Employability Scale | x | x | x |
| D9 | Latent functions of employment (time structure, financial strain, | x | x | x |
| D10 | Resilience | x | x | x |
| Material Security | ||||
| E1 | Material Security | x | x | x |
| E2 | Food Security Scale | x | x | x |
| Education and Training | ||||
| F1-3 | Education & Training (partial, completed, current, planned, referrals | x | x | x |
| F4 | Training rigor | x | x | x |
| G1 | Employment service engagement (accessed, referrals, programs) | x | x | x |
| G2 | Barriers to accessing employment service | x | x | x |
| Substance Use and drug-related harm | ||||
| H1 | Substance past 12 months | x | ||
| H2 | Substance past 3 months: drug, route, frequency, dose, street value | x | x | x |
| H4 | Drug expenditure | x | x | x |
| H5 | Reduced risk Substance Use Practices | x | x | x |
| H6 | Riskier Substance Use Practices | x | x | x |
| H8 | Reasons for Substance Use | x | x | x |
| H9 | Substance use related to work | x | x | x |
| J1-5 | Binge drug use (length, frequency, harms) | x | x | x |
| K1-7 | Overdose (number, substance, route, help) | x | x | x |
| Debt | ||||
| L1 | Debt (who, reasons) | x | x | x |
| L2-7 | Drug debt and repercussions | x | x | x |
| Health measures | ||||
| M1 | Violence exposure (Childhood, adulthood, current) | x | x | x |
| M3 | Violence perpetration | x | x | x |
| N1 | Satisfaction scale/quality of life | x | x | x |
| N2 | Mental health | x | x | x |
| N3 | Physical Health | x | x | x |
| N4 | Current Health State | x | x | x |
| Service Utilization and Service access barriers | ||||
| O1-2 | Health Care (Hospital Admissions, emerg dept, drug use Tx EMS & paramedics, use and barriers) | x | x | x |
| O3-4 | Social Services (use and barriers) | x | x | x |
| O5 | Criminal Justice System (police interactions, circumstances) | x | x | x |
| COVID-19 | ||||
| CV1-2 | Awareness and Testing | x | ||
| CV12-14 | Social Distancing and precautions | x | x | x |
| CV15-16 | Housing precautions | x | x | x |
| C17 | Community connectedness | x | x | x |
| C18-21 | Education and training (enroll, barriers) | x | x | x |
| CV23-33 | Income generation safety and changes | x | x | x |
| CV34-36 | Social Assistance (changes, adequacy, barriers, clawbacks) | x | x | x |
| CV37-40 | Substance use changes | x | x | x |
| CV41-42 | Drug debt changes | x | x | x |
| CV43-44 | Violence (social distancing, self-isolation, police presence) | x | x | x |
| CV46 | Social services utilization barriers | x | x | x |
| CV47 | Health services utilization barriers | x | x | x |
| CV48 | Treatment services utilization barriers | x | x | x |
| CV49-54 | Safe supply (use, adequacy, reasons barriers) | x | x | x |
Appendix B. Qualitative Enrolment and Follow-Up Schedule
| Baseline Visits | Cumulative Enrolment | Eligible for Follow-up | Follow-up Visits | Withdrew | Deceased | Follow-Up Rate (%) | |
|---|---|---|---|---|---|---|---|
| Round 07 (February–April 2021) | 26 | 26 | 0 | 0 | 0 | 0 | 0 |
| Round 08 (April–July 2021) | 11 | 37 | 0 | 0 | 0 | 1 | 0 |
| Round 09 (July–October 2021) | 3 | 40 | 25 | 21 | 0 | 0 | 84 |
| Round 10 (November 2021–January 2022) | 1 | 41 | 15 | 8 | 0 | 0 | 53.33 |
| Round 11 (February–April 2022) | 0 | 41 | 31 | 26 | 0 | 1 | 83.87 |
| Total | 41 | 41 | NA | 55 | 0 | 2 | 73.73 |
References
- Taha, S.; Maloney-Hall, B.; Buxton, J. Lessons learned from the opioid crisis across the pillars of the Canadian drugs and substances strategy. Subst. Abus. Treat. Prev. Policy 2019, 14, 32. [Google Scholar] [CrossRef] [PubMed]
- Ciccarone, D. The triple wave epidemic: Supply and demand drivers of the US opioid overdose crisis. Int. J. Drug Policy 2019, 71, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Nicola, M.; Chapman, J.; Crier, N.; Marsh, S.; McLeod, J.; Deane, L.A. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 2020, 78, 185. [Google Scholar] [CrossRef]
- Patel, J.A.; Nielsen, F.B.H.; Badiani, A.A.; Assi, S.; Unadkat, V.A.; Patel, B.; Ravindraen, R.; Wardle, H. Poverty, inequality and COVID-19: The forgotten vulnerable. Public Health 2020, 183, 110. [Google Scholar] [CrossRef] [PubMed]
- Canadian Substance Use Costs and Harms Scientific Working Group. Canadian Substance Use Costs and Harms (2007–2014) Preapared by the Canadian Institute for Substance Use Research and the Canadian Centre on Substance Use and Addiction; Canadian Centre on Substance Use and Addiction: Ottawa, ON, Canada, 2018. [Google Scholar]
- Degenhardt, L.; Whiteford, H.A.; Ferrari, A.J.; Baxter, A.J.; Charlson, F.J.; Hall, W.D.; Freedman, G.; Burstein, R.; Johns, N.; Engell, R.E.; et al. Global burden of disease attributable to illicit drug use and dependence: Findings from the Global Burden of Disease Study 2010. Lancet 2013, 382, 1564–1574. [Google Scholar] [CrossRef]
- van Draanen, J.; Tsang, C.; Mitra, S.; Karamouzian, M.; Richardson, L. Socioeconomic marginalization and opioid-related overdose: A systematic review. Drug Alcohol Depend. 2020, 214, 108127. [Google Scholar] [CrossRef]
- Richardson, L.; Long, C.; DeBeck, K.; Nguyen, P.; Milloy, M.J.S.; Wood, E.; Kerr, T.H. Socioeconomic marginalisation in the structural production of vulnerability to violence among people who use illicit drugs. J. Epidemiol. Community Health 2015, 69, 686–692. [Google Scholar] [CrossRef]
- Richardson, L.; Kerr, T.H.; Dobrer, S.; Puskas, C.M.; Guillemi, S.A.; Montaner, J.S.G.; Wood, E.; Milloy, M.J.S. Socioeconomic marginalization and plasma HIV-1 RNA nondetectability among individuals who use illicit drugs in a Canadian setting. AIDS 2015, 29, 2487–2495. [Google Scholar] [CrossRef]
- Salleh, N.A.M.; Van Draanen, J.; Nosova, E.; Barrios, R.; Richardson, L. Material security and adherence to antiretroviral therapy among HIV-positive people who use illicit drugs. AIDS 2020, 34, 1037–1045. [Google Scholar] [CrossRef]
- Henkel, D. Unemployment and substance use: A review of the literature (1990–2010). Curr. Drug Abus. Rev. 2011, 4, 4–27. [Google Scholar] [CrossRef]
- Richardson, L.; Sherman, S.G.; Kerr, T. Employment amongst people who use drugs: A new arena for research and intervention. Int. J. Drug Policy 2012, 23, 3–5. [Google Scholar] [CrossRef] [PubMed]
- Platt, J.J. Vocational Rehabilitation of Drug Abusers. Psychol. Bull. 1995, 117, 416–433. [Google Scholar] [CrossRef] [PubMed]
- Richardson, L.; Wood, E.; Montaner, J.; Kerr, T. Addiction treatment-related employment barriers: The impact of methadone maintenance. J. Subst. Abus. Treat. 2012, 43, 276–284. [Google Scholar] [CrossRef] [PubMed]
- Richardson, L.; Mammel, M.; Milloy, M.J.; Hayashi, K. Employment Cessation, Long Term Labour Market Engagement and HIV Infection Risk Among People Who Inject Drugs in an Urban Canadian Setting. AIDS Behav. 2019, 23, 3267–3276. [Google Scholar] [CrossRef] [PubMed]
- Alexandre, P.K.; French, M.T. Further evidence on the labor market effects of addiction: Chronic drug use and employment in metropolitan Miami. Contemp. Econ. Policy 2004, 22, 382–393. [Google Scholar] [CrossRef]
- French, M.T.; Roebuck, M.C.; Alexandre, P.K. Illicit drug use, employment, and labor force participation. South. Econ. J. 2001, 68, 349–368. [Google Scholar]
- Bray, J.W.; Zarkin, G.A.; Dennis, M.L.; French, M.T. Symptoms of Dependence, Multiple Substance Use, and Labor Market Outcomes. Am. J. Drug Alcohol Abus. 2000, 26, 77–95. [Google Scholar] [CrossRef]
- Richardson, L.; Wood, E.; Li, K.; Kerr, T. Factors associated with employment among a cohort of injection drug users. Drug Alcohol Rev. 2010, 29, 293–300. [Google Scholar] [CrossRef]
- Perlmutter, A.S.; Conner, S.C.; Savone, M.; Kim, J.H.; Segura, L.E.; Martins, S.S. Is employment status in adults over 25 years old associated with nonmedical prescription opioid and stimulant use. Soc. Psychiatry Psychiatr. Epidemiol. 2017, 52, 291–298. [Google Scholar] [CrossRef]
- MacDonald, Z.; Pudney, S. The Wages of Sin? Illegal Drug Use and the Labour Market. Labour 2000, 14, 657–673. [Google Scholar] [CrossRef]
- DeSimone, J. Illegal drug use and employment. J. Labor Econ. 2002, 20, 952–977. [Google Scholar] [CrossRef]
- Atkinson, J.S.; Montoya, I.D.; Trevino, R.A.; Richard, A.J. Labor force participation in a sample of substance users. Am. J. Drug Alcohol Abus. 2000, 26, 355–367. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.E.; Reynolds, G.L.; Fisher, D.G. Employment status and psychological symptomatology among drug users not currently in treatment. Eval. Program Plan. 2001, 24, 215–220. [Google Scholar] [CrossRef]
- Koo, D.J.; Chitwood, D.D.; Sánchez, J. Factors for employment: A case-control study of fully employed and unemployed heroin users. Subst. Use Misuse 2007, 42, 1035–1054. [Google Scholar] [CrossRef] [PubMed]
- McCoy, C.B.; Comerford, M.; Metsch, L.R. Employment among chronic drug users at baseline and 6-month follow-up. Subst. Use Misuse 2007, 42, 1055–1067. [Google Scholar] [CrossRef]
- Richardson, L.; Wood, E.; Kerr, T. The impact of social, structural and physical environmental factors on transitions into employment among people who inject drugs. Soc. Sci. Med. 2013, 76, 126–133. [Google Scholar] [CrossRef]
- Jaffe, K.; Dong, H.; Godefroy, A.; Boutan, D.; Hayashi, K.; Milloy, M.S.; Kerr, T.; Richardson, L. Informal recycling, income generation and risk: Health and social harms among people who use drugs. Int. J. Drug Policy 2018, 60, 40–46. [Google Scholar] [CrossRef]
- Kerr, T.; Small, W.; Johnston, C.; Li, K.; Montaner, J.S.G.; Wood, E. Characteristics of injection drug users who participate in drug dealing: Implications for drug policy. J. Psychoact. Drugs 2008, 40, 147–152. [Google Scholar] [CrossRef]
- Shannon, K.; Kerr, T.; Allinott, S.; Chettiar, J.; Shoveller, J.; Tyndall, M.W. Social and structural violence and power relations in mitigating HIV risk of drug-using women in survival sex work. Soc. Sci. Med. 2008, 66, 911–921. [Google Scholar] [CrossRef]
- Richardson, L.; DeBeck, K.; Feng, C.; Kerr, T.; Wood, E. Employment and risk of injection drug use initiation among street involved youth in Canadian setting. Prev. Med. 2014, 66, 56–59. [Google Scholar] [CrossRef]
- DeBeck, K.; Shannon, K.; Wood, E.; Li, K.; Montaner, J.; Kerr, T. Income generating activities of people who inject drugs. Drug Alcohol Depend. 2007, 91, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Debeck, K.; Wood, E.; Qi, J.; Fu, E.; McArther, D.; Montaner, J.; Kerr, T. Interest in low-threshold employment among people who inject illicit drugs: Implications for street disorder. Int. J. Drug Policy 2011, 22, 376–384. [Google Scholar] [CrossRef] [PubMed]
- Long, C.; DeBeck, K.; Feng, C.; Montaner, J.; Wood, E.; Kerr, T. Income level and drug related harm among people who use injection drugs in a Canadian setting. Int. J. Drug Policy 2014, 25, 458–464. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Special Advisory Committee on the Epidemic of Opioid Overdoses. Opioid-Related Harms in Canada; Public Health Agency of Canada: Ottawa, ON, Canada, 2020.
- British Columbia Coroner’s Service. Illicit Drug Overdose Deaths in BC: Findings of Coroners’ Investigations; Ministry of Public Safety and Solicitor General: Victoria, BC, Canada, 2018.
- Slavova, S.; Rock, P.; Bush, H.M.; Quesinberry, D.; Walsh, S.L. Signal of Increased Opioid Overdose during COVID-19 from Emergency Medical Services Data. Drug Alcohol Depend. 2020, 214, 108176. [Google Scholar] [CrossRef] [PubMed]
- Wakeman, S.E.; Green, T.C.; Rich, J. An overdose surge will compound the COVID-19 pandemic if urgent action is not taken. Nat. Med. 2020, 26, 819–820. [Google Scholar] [CrossRef]
- Barnay, T. Health, work and working conditions: A review of the European economic literature. Eur. J. Health Econ. 2016, 17, 693–709. [Google Scholar] [CrossRef]
- Van der Noordt, M.; IJzelenberg, H.; Droomers, M.; Proper, K.I. Health effects of employment: A systematic review of prospective studies. Occup. Environ. Med. 2014, 71, 730–736. [Google Scholar] [CrossRef]
- Burke, R.J.; Page, K.M. Research Handbook on Work and Well-Being; Edward Elgar Publishing: Northampton, MA, USA, 2017. [Google Scholar]
- Benach, J.; Muntaner, C. Precarious employment: Understanding an emerging social determinant of health. Annu. Rev. Public Health 2014, 35, 229–253. [Google Scholar] [CrossRef]
- Julià, M.; Vanroelen, C.; Bosmans, K.; Van Aerden, K.; Benach, J. Precarious Employment and Quality of Employment in Relation to Health and Well-being in Europe. Int. J. Health Serv. 2017, 47, 389–409. [Google Scholar] [CrossRef]
- Rivera, A.S.; Akanbi, M.; O’Dwyer, L.C.; McHugh, M. Shift work and long work hours and their association with chronic health conditions: A systematic review of systematic reviews with meta-analyses. PLoS ONE 2020, 15, e0231037. [Google Scholar] [CrossRef]
- Eisenberg-Guyot, J.; Peckham, T.; Andrea, S.B.; Oddo, V.; Seixas, N.; Hajat, A. Life-course trajectories of employment quality and health in the US: A multichannel sequence analysis. Soc. Sci. Med. 2020, 264, 113327. [Google Scholar] [CrossRef] [PubMed]
- Wagenaar, A.F.; Kompier, M.A.; Houtman, I.L.; van den Bossche, S.N.; Taris, T.W. Employment contracts and health selection: Unhealthy employees out and healthy employees in. J. Occup. Environ. Med. 2012, 54, 1192–1200. [Google Scholar] [CrossRef] [PubMed]
- McDonough, P.; Amick, B.C. The social context of health selection: A longitudinal study of health and employment. Soc. Sci. Med. 2001, 53, 135–145. [Google Scholar] [CrossRef]
- Netuveli, G. Understanding Population Trends and Processes: Social and Spatial Inequalities; Stillwell, J., Norman, P., Thomas, C., Surridge, P., Eds.; Springer: Dordrecht, The Netherlands, 2010; pp. 129–141. [Google Scholar]
- Ross, C.E.; Mirowsky, J. Does employment affect health? J. Health Soc. Behav. 1995, 36, 230–243. [Google Scholar] [CrossRef] [PubMed]
- Gavrielov-Yusim, N.; Friger, M. Use of administrative medical databases in population-based research. J. Epidemiol. Community Health 2014, 68, 283–287. [Google Scholar] [CrossRef] [PubMed]
- Kalsbeek, W.; Heiss, G. Building bridges between populations and samples in epidemiological studies. Annu. Rev. Public Health 2000, 21, 147–169. [Google Scholar] [CrossRef]
- Richardson, L.; Small, W.; Kerr, T. Pathways linking drug use and labour market trajectories: The role of catastrophic events. Sociol. Health Illn. 2016, 38, 137–152. [Google Scholar] [CrossRef]
- Conyers, L.M.; Richardson, L.A.; Datti, P.A.; Koch, L.C.; Misrok, M. A critical review of health, social, and prevention outcomes associated with employment for people living with HIV. AIDS Educ. Prev. 2017, 29, 475–490. [Google Scholar] [CrossRef]
- Richardson, L.; Richardson, L.; Milloy, M.-J.S.; Kerr, T.H.; Parashar, S.; Montaner, J.S.G.; Wood, E. Employment predicts decreased mortality among HIV-seropositive illicit drug users in a setting of universal HIV care. J. Epidemiol. Community Health 2014, 68, 93–96. [Google Scholar] [CrossRef]
- Jaffe, K.; Jaffe, K.; Nosova, E.; Maher, L.; Hayashi, K.; Milloy, M.J.; Richardson, L. Income generation and the patterning of substance use: A gender-based analysis. Drug Alcohol Depend. 2021, 226, 108862. [Google Scholar] [CrossRef]
- Hoffmann, R.; Kröger, H.; Geyer, S. Social causation versus health selection in the life course: Does their relative importance differ by dimension of SES. Soc. Indic. Res. 2019, 141, 1341–1367. [Google Scholar] [CrossRef]
- Local Economic Development Lab. DTES Information Hub Survey: Mapping the Continuum of Income-Generating Opportunities in Vancouver’s Downtown Eastside; Local Economic Development Lab: Vancouver, BC, Canada, 2015. [Google Scholar]
- Downtown Eastside Community Economic Development Strategic Action Committee. DTES Community Economic Development Strategy Phase II; City of Vancouver: Vancouver, BC, Canada, 2016. [Google Scholar]
- Vosko, L.F. Managing the Margins: Gender, Citizenship, and the International Regulation of Precarious Employment; Oxford University Press: New York, NY, USA, 2010. [Google Scholar]
- Kalleberg, A.L. Good Jobs, Bad Jobs; Russell Sage Foundation: New York, NY, USA, 2011. [Google Scholar]
- Greer, A.; Bungay, V.; Pauly, B.; Buxton, J. ‘Peer’ work as precarious: A qualitative study of work conditions and experiences of people who use drugs engaged in harm reduction work. Int. J. Drug Policy 2020, 85, 102922. [Google Scholar] [CrossRef] [PubMed]
- Olding, M.; Boyd, J.; Kerr, T.; McNeil, R. “And we just have to keep going”: Task shifting and the production of burnout among overdose response workers with lived experience. Soc. Sci. Med. 2021, 270, 113631. [Google Scholar] [CrossRef] [PubMed]
- Olding, M.; Barker, A.; McNeil, R.; Boyd, J. Essential work, precarious labour: The need for safer and equitable harm reduction work in the era of COVID-19. Int. J. Drug Policy 2021, 90, 103076. [Google Scholar] [CrossRef]
- Curnock, E.; Leyland, A.H.; Popham, F. The impact on health of employment and welfare transitions for those receiving out-of-work disability benefits in the UK. Soc. Sci. Med. 2016, 162, 1–10. [Google Scholar] [CrossRef]
- Polanyi, M.; Tompa, E. Rethinking work-health models for the new global economy: A qualitative analysis of emerging dimensions of work. Work 2004, 23, 3–18. [Google Scholar]
- Emslie, C.; Hunt, K. ‘Live to work’ or ‘work to live’? A qualitative study of gender and work–life balance among men and women in mid-life. Gender 2009, 16, 151–172. [Google Scholar]
- Brady, D. Theories of the Causes of Poverty. Annu. Rev. Sociol. 2019, 45, 155–175. [Google Scholar] [CrossRef]
- Malizia, E.; Feser, E.J.; Renski, H.; Drucker, J. Understanding Local Economic Development; Routledge: London, UK, 2020. [Google Scholar]
- Gagne, C.A.; Finch, W.L.; Myrick, K.J.; Davis, L.M. Peer Workers in the Behavioral and Integrated Health Workforce: Opportunities and Future Directions. Am. J. Prev. Med. 2018, 54, S258–S266. [Google Scholar] [CrossRef]
- Tookey, P.; Mason, K.; Broad, J.; Behm, M.; Bondy, L.; Powis, J. From client to co-worker: A case study of the transition to peer work within a multi-disciplinary hepatitis c treatment team in Toronto, Canada. Harm Reduct. J. 2018, 15, 41. [Google Scholar] [CrossRef]
- Hayre, K.M. Identifying Actions to Improve Low-Barrier Employment Initiatives in Vancouver; Exchange Inner City: Vancouver, BC, Canada, 2021. [Google Scholar]
- Ramsden, I. Cultural safety/Kawa Whakaruruhau ten years on: A personal overview. Nurs. Prax. N. Z. 2000, 15, 4–12. [Google Scholar] [CrossRef] [PubMed]
- Curtis, E.; Jones, R.; Tipene-Leach, D.; Walker, C.; Loring, B.; Paine, S.-J.; Reid, P. Why cultural safety rather than cultural competency is required to achieve health equity: A literature review and recommended definition. Int. J. Equity Health 2019, 18, 1–17. [Google Scholar] [CrossRef] [PubMed]
- First Nations Health Authority; First Nations Health Council; First Nations Director’s Association. Anti-Racism, Cultural Safety; Humility Framework: Vancouver, BC, Canada, 2021. [Google Scholar]
- Blustein, D.L.; Duffy, R.; Ferreira, J.A.; Cohen-Scali, V.; Cinamon, R.G.; Allan, B.A. Unemployment in the Time of COVID-19: A Research Agenda. J. Vocational Behav. 2020, 119, 103436. [Google Scholar] [CrossRef] [PubMed]
- Ivsins, A.; Benoit, C.; Kobayashi, K.; Boyd, S. From risky places to safe spaces: Re-assembling spaces and places in Vancouver’s Downtown Eastside. Health Place 2019, 59, 102164. [Google Scholar] [CrossRef]
- British Columbia Coroner’s Service. Illicit Drug Toxicity Deaths in BC: 1 January 2012–31 March 2022; British Columbia Coroner’s Service: Victoria, BC, Canada, 2022.
- British Columbia Coroner’s Service. Illicit Drug Toxicity Deaths in BC: 1 January 2009–31 October 2019; British Columbia Coroner’s Service: Victoria, BC, Canada, 2019.
- Dasgupta, N.; Beletsky, L.; Ciccarone, D. Opioid Crisis: No Easy Fix to Its Social and Economic Determinants. Am. J. Public Health 2018, 108, 182–186. [Google Scholar] [CrossRef]
- Gringeri, C.E. The Poverty of Hard Work: Multiple Jobs and Low Wages in Family Economies of Rural Utah Households. J. Sociol. Soc. Welf. 2001, 28, 3–22. [Google Scholar]
- Creswell, J.W. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches; Sage Publications, Inc.: Thousand Oaks, CA, USA, 2009. [Google Scholar]
- Creswell, J.W.; Clark, V.L.P. Designing and Conducting Mixed Methods Research; Sage Publications, Inc.: Thousand Oaks, CA, USA, 2017. [Google Scholar]
- Magnani, R.; Sabin, K.; Saidel, T.; Heckathorn, D. Review of sampling hard-to-reach and hidden populations for HIV surveillance. AIDS 2005, 19, S67–S72. [Google Scholar] [CrossRef]
- Van Draanen, J.; Hayashi, K.; Milloy, M.J.; Nosova, E.; Shulha, H.; Grant, C.; Richardson, L. Material security as a measure of poverty: A validation study with people who use drugs. Soc. Indic. Res. 2021, 157, 501–521. [Google Scholar] [CrossRef]
- Ivankova, N.V.; Creswell, J.W.; Stick, S.L. Using mixed-methods sequential explanatory design: From theory to practice. Field Methods 2006, 18, 3–20. [Google Scholar] [CrossRef]
- Suri, H. Purposeful sampling in qualitative research synthesis. Qual. Res. J. 2011, 11, 63–75. [Google Scholar] [CrossRef]
- Euser, A.M.; Zoccali, C.; Jager, K.J.; Dekker, F.W. Cohort studies: Prospective versus retrospective. Nephron Clin. Pract. 2009, 113, c214–c217. [Google Scholar] [CrossRef] [PubMed]
- Boyd, J.; Richardson, L.; Anderson, S.; Kerr, T.; Small, W.; McNeil, R. Transitions in income generation among marginalized people who use drugs: A qualitative study on recycling and vulnerability to violence. Int. J. Drug Policy 2018, 59, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Stull, D.E.; Leidy, N.K.; Parasuraman, B. Optimal recall periods for patient-reported outcomes: Challenges and potential solutions. Curr. Med. Res. Opin. 2009, 25, 929–942. [Google Scholar] [CrossRef]
- Richardson, L.; Laing, A.; Choi, J.; Nosova, E.; Milloy, M.-J.; Marshall, B.; Singer, J.; Wood, E.; Kerr, T. Effect of alternative income assistance schedules on drug use and drug-related harm: A randomised controlled trial. Lancet Public Health 2021, 6, e324–e334. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Lewchuck, W.; Procyk, S.; Lafleche, M.; Rosen, D.; Dyson, D.; Shields, J.; Goldring, L.; Viducis, P.; Meisner, A.; Vrankulj, S. Is precarious employment low income employment? the changing labour market in southern Ontario. Just Labour 2014, 22, 51–73. [Google Scholar] [CrossRef]
- Ompad, D.C.; Nandi, V.; Cerdá, M.; Crawford, N.; Galea, S.; Vlahov, D. Beyond income: Material resources among drug users in economically-disadvantaged New York City neighborhoods. Drug Alcohol Depend. 2012, 120, 127–134. [Google Scholar] [CrossRef]
- Richardson, L.; Laing, A.; Milloy, M.-J.; Maynard, R.; Nosyk, B.; Marshall, B.; Grafstein, E.; Daly, P.; Wood, E.; Montaner, J.; et al. Protocol of the impact of alternative social assistance disbursement on drug-related harm (TASA) study: A randomized controlled trial to evaluate changes to payment timing and frequency among people who use illicit drugs. BMC Public Health 2016, 16, 668. [Google Scholar] [CrossRef]
- British Columbia Centre on Substance Use; BC Ministry of Health; Ministry of Mental Health and Addictions. Risk Mitigation in the Context of Dual Health Emergencies—Interim Clinical Guidance: Update. Available online: https://www.bccsu.ca/COVID-19 (accessed on 5 April 2022).
- Dupuis, M.; Baggio, S.; Gmel, G. Validation of a brief form of the Perceived Neighborhood Social Cohesion questionnaire. J. Health Psychol. 2017, 22, 218–227. [Google Scholar] [CrossRef]
- Jahoda, M. Employment and Unemployment: A Social-Psychological Analysis; Cambridge University Press: New York, NY, USA, 1982. [Google Scholar]
- Creed, P.A.; Macintyre, S.R. The relative effects of deprivation of the latent and manifest benefits of employment on the well-being of unemployed people. J. Occup. Health Psychol. 2001, 6, 324. [Google Scholar] [CrossRef] [PubMed]
- Lundberg, O.; Manderbacka, K. Assessing reliability of a measure of self-rated health. Scand. J. Soc. Med. 1996, 24, 218–224. [Google Scholar] [CrossRef] [PubMed]
- DeSalvo, K.B.; Fisher, W.P.; Tran, K.; Bloser, N. Assessing measurement properties of two single-item general health measures. Qual. Life Res. 2006, 15, 191–201. [Google Scholar] [CrossRef] [PubMed]
- Üstün, T.B.; Chatterji, S.; Kostanjsek, N.; Rehm, J.; Kennedy, C.; Epping-Jordan, J.; Saxena, S.; Korff, M.V.; Pull, C. Developing the World Health Organization disability assessment schedule 2.0. Bull. World Health Organ. 2010, 88, 815–823. [Google Scholar] [CrossRef] [PubMed]
- Conrad, K.J.; Yagelka, J.R.; Matters, M.D.; Rich, A.R.; Williams, V.; Buchanan, M. Reliability and validity of a modified Colorado Symptom Index in a national homeless sample. Ment. Health Serv. Res. 2001, 3, 141–153. [Google Scholar] [CrossRef]
- Cummins, R.A.; Eckersley, R.; Pallant, J.; Van Vugt, J.; Misajon, R. Developing a national index of subjective wellbeing: The Australian Unity Wellbeing Index. Soc. Indic. Res. 2003, 64, 159–190. [Google Scholar] [CrossRef]
- Marshall, B.D.L.; Fairbairn, N.; Li, K.; Wood, E.; Kerr, T. Physical violence among a prospective cohort of injection drug users: A gender-focused approach. Drug Alcohol Depend. 2008, 97, 237–246. [Google Scholar] [CrossRef]
- Neale, J.; Kemp, P.A. Substance Misuse: The Implications of Research, Policy and Practice; Barlow, J., Ed.; Jessica Kingsley Publishers: London, UK, 2009; pp. 94–101. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Core Team: Vienna, Austria, 2022. [Google Scholar]
- Carten, R. Better at Home Final Report on Community Consultations in the Downtown Eastside; Better at Home: Vancouver, BC, Canada, 2014. [Google Scholar]
- BC Non-Profit Housing Association. 2020 Homeless Count in Metro Vancouver; BC Non-Profit Housing Association: Vancouver, BC, Canada, 2020. [Google Scholar]
- Altonji, J.G.; Blank, R.M. Race and gender in the labor market. Handb. Labor Econ. 1999, 3, 3143–3259. [Google Scholar]
- Sjonnesen, K.; Bulloch, A.G.M.; Williams, J.; Lavorato, D.; Patten, B.S. Characterization of disability in Canadians with mental disorders using an abbreviated version of a DSM-5 emerging measure: The 12-Item WHO Disability Assessment Schedule (WHODAS) 2.0. Can. J. Psychiatry 2016, 61, 227–235. [Google Scholar] [CrossRef]
- Andrews, G.; Kemp, A.; Sunderland, M.; Von Korff, M.; Ustun, T.B. Normative data for the 12 item WHO Disability Assessment Schedule 2.0. PLoS ONE 2009, 4, e8343. [Google Scholar] [CrossRef]
- Palepu, A.; Patterson, M.; Strehlau, V.; Moniruzzamen, A.; de Bibiana, J.T.; Frankish, J.; Krausz, M.; Somers, J. Daily substance use and mental health symptoms among a cohort of homeless adults in Vancouver, British Columbia. J. Urban Health 2013, 90, 740–746. [Google Scholar] [CrossRef] [PubMed]
- Colledge, S.; Peacock, A.; Leung, J.; Larney, S.; Grebely, J.; Hickman, M.; Cunningham, E.; Trickey, A.; Stone, J.; Vickerman, P. The prevalence of non-fatal overdose among people who inject drugs: A multi-stage systematic review and meta-analysis. Int. J. Drug Policy 2019, 73, 172–184. [Google Scholar] [CrossRef] [PubMed]
- Ku, L.; Brantley, E. Widening social and health inequalities during the COVID-19 pandemic. JAMA Health Forum 2020, 1, e200721. [Google Scholar] [CrossRef]
- Perry, B.L.; Aronson, B. Pandemic precarity: COVID-19 is exposing and exacerbating inequalities in the American heartland. Proc. Natl. Acad. Sci. USA 2021, 118, e2020685118. [Google Scholar] [CrossRef]
- Hill, R.; Narayan, A. ‘COVID-19 and Inequality: A Review of the Evidence on Likely Impact and Policy Options’; Working Paper; Centre for Disaster Protection: London, UK, 2020. [Google Scholar]
- Stowe, M.J.; Calvey, T.; Scheibein, F.; Arya, S. Access to healthcare and harm reduction services during the COVID-19 pandemic for people who use drugs. J. Addict. Med. 2020, 14, e287–e289. [Google Scholar] [CrossRef]
- Brener, L.; Rance, J.; Caruana, T.; Horwitz, R.; Bryant, J. Assessing the Impact of COVID on Harm Reduction Services; UNSW Centre for Social Reseach in Health: Sydney, Australia, 2021. [Google Scholar]
- Gur-Arie, R.; Jamrozik, E.; Kingori, P. No jab, no job? Ethical issues in mandatory COVID-19 vaccination of healthcare personnel. BMJ Glob. Health 2021, 6, e004877. [Google Scholar] [CrossRef]
- Biemer, P.P.; Groves, R.M.; Lyberg, L.E.; Mathiowetz, N.A.; Sudman, S. Measurement Errors in Surveys; Wiley: New York, NY, USA, 2011. [Google Scholar]
- McElrath, K.; Chitwood, D.D.; Griffin, D.K.; Comerford, M. The consistency of self-reported HIV risk behavior among injection drug users. Am. J. Public Health 1994, 84, 1965–1970. [Google Scholar] [CrossRef]
- Neale, J.; Allen, D.; Coombes, L. Qualitative research methods within the addictions. Addiction 2005, 100, 1584–1593. [Google Scholar] [CrossRef]
- Darke, S. Self-report among injecting drug users: A review. Drug Alcohol Depend. 1998, 51, 253–263. [Google Scholar] [CrossRef]
- Fendrich, M.; Johnson, T.P.; Sudman, S.; Wislar, J.S.; Spiehler, V. Validity of drug use reporting in a high-risk community sample: A comparison of cocaine and heroin survey reports with hair tests. Am. J. Epidemiol. 1999, 149, 955. [Google Scholar] [CrossRef]
- Weatherby, N.L.; Needle, R.; Cesari, H.; Booth, R.; McCoy, C.B.; Watters, J.K.; Williams, M.; Chitwood, D. Validity of self-reported drug use among injection drug users and crack cocaine users recruited through street outreach. Eval. Program Plan. 1994, 17, 347–355. [Google Scholar] [CrossRef]
- Shen, Q. Location characteristics of inner-city neighborhoods and employment accessibility of low-wage workers. Environ. Plan. B Plan. Des. 1998, 25, 345–365. [Google Scholar] [CrossRef]


| Baseline Visits | Cumulative Enrolment | Eligible for Follow-Up | Follow-Up Visits | Withdrew | Deceased | Follow-Up Rate (%) | |
|---|---|---|---|---|---|---|---|
| Round 00 (Apr–Jul 2019) | 95 | 95 | 0 | 0 | 2 | 0 | NA |
| Round 01 (Jul–Oct 2019) | 87 | 182 | 93 | 84 | 1 | 2 | 90.32 |
| Round 02 (Nov 2019–Jan 2020) | 24 | 206 | 177 | 155 | 0 | 4 | 87.57 |
| Round 03 (Feb–Apr 2020) | 20 * | 226 | 197 | 80 * | 0 | 0 | 40.61 * |
| Round 04 (Apr–Jul 2020) | 0 * | 0 * | 0 * | 0 * | 0 * | 0 * | 0 * |
| Round 05 (Jul–Oct 2020) | 0 | 226 | 217 | 153 | 0 | 4 | 70.51 |
| Round 06 (Nov 2020–Jan 2021) | 11 | 237 | 214 | 144 | 2 | 2 | 67.29 |
| Round 07 (Feb–Apr 2021) | 4 | 241 | 221 | 149 | 1 | 3 | 67.42 |
| Round 08 (Apr–Jul 2021) | 4 | 245 | 221 | 147 | 2 | 5 | 66.52 |
| Round 09 (Jul–Oct 2021) | 5 | 250 | 218 | 136 | 0 | 3 | 62.39 |
| Round 10 (Nov 2021–Jan 2022) | 1 | 251 | 221 | 157 | 0 | 5 | 71.04 |
| Round 11 (Feb–Apr 2022) | 6 | 257 | 214 | 143 | 0 | 1 | 66.82 |
| Total: | 257 | 257 | NA | 1347 | 8 | 29 | 62.77 |
| n (%) | |
|---|---|
| Total | 256 (100%) |
| Gender (n = 256) | |
| Cisgender man | 145 (57%) |
| Cisgender woman | 101 (39%) |
| Transgender, gender diverse, or two-spirit | 10 (3.9%) |
| Race/Ethnicity (n = 250) | |
| Indigenous (Aboriginal, First Nations, Inuit, Metis) | 99 (40%) |
| Asian (Indian, Pakistani, Chinese, Vietnamese, Japanese, Filipino) | 11 (4.4%) |
| Black (African, Caribbean) | 7 (2.8%) |
| White (European or European descent) | 122 (49%) |
| Not captured by above categories | 11 (4.4%) |
| Born outside of Canada (n-255) | 23 (9.0%) |
| Age (n = 256) | |
| Less than 45 years old | 80 (31%) |
| 45–60 years old | 156 (61%) |
| 60+ years old | 20 (7.8%) |
| Relationship status (n = 255) | |
| Single/Dating | 177 (69%) |
| Partnered/Married/Common law | 63 (25%) |
| Separated/Divorced/Widowed | 15 (5.9%) |
| Housing situation (n = 256) | |
| Homeless past 30 days | 27 (11%) |
| Stably housed | 229 (89%) |
| Educational attainment (n = 256) | |
| Less than high school | 132 (52%) |
| High school or more | 124 (48%) |
| Lifetime | Current a | |
|---|---|---|
| Substance use b | 254 (99%) | 218 (86%) |
| Binge use | 195 (78%) | 72 (32%) |
| Daily opioid use c | 251 (98%) | 69 (27%) |
| Daily stimulant use d | 245 (96%) | 51 (20%) |
| Accidental overdose | 140 (56%) | 29 (12%) |
| Enrolled in substance use disorder treatment e | -- | 127 (50%) |
| Satisfaction with health, range 0–10 (higher = higher satisfaction) | -- | 7.00 (6.00, 9.00) |
| WHO Disability Assessment Schedule, range: 0–48 (higher = greater functional impairment) | -- | 14 (6, 22) |
| Modified Colorado Symptom Index score, range: 0–50 (higher = higher symptom frequency) | -- | 12 (5, 19) |
| Lifetime | Current a | |
|---|---|---|
| Average monthly income ($ CAD) d | -- | 1955 (1521, 2489) |
| Attended school/training program b | 202 (79%) | 50 (20%) |
| Used employment services | 141 (55%) | 80 (31%) |
| Received income assistance | ||
| Employable/hardship income assistance | 200 (78%) | 27 (11%) |
| Disability assistance | 216 (84%) | 202 (83%) |
| Employment insurance | 97 (38%) | 2 (0.8%) |
| Old age security/Public pension | 22 (8.6%) | 20 (7.8%) |
| Income generation | ||
| Informal/prohibited/illegal activities | 245 (96%) | 191 (75%) |
| Recycling (binning, buy/sell) c | 153 (60%) | 80 (31%) |
| Squeegeeing | 18 (7.0%) | 0 (0%) |
| Panhandling | 73 (29%) | 14 (5.5%) |
| Theft, stealing (shoplifting, breaking into cars/houses) | 120 (47%) | 17 (6.6%) |
| Selling needles | 18 (7.0%) | 1 (0.4%) |
| Selling cigarettes/tobacco | 81 (32%) | 28 (11%) |
| Selling drugs/enforcing | 150 (59%) | 43 (17%) |
| Sex work | 21 (8.2%) | 2 (0.8%) |
| Other criminal(ized) activity | 90 (35%) | 24 (9.4%) |
| Stipend | 192 (75%) | 152 (59%) |
| Formal employment | 246 (96%) | 129 (50%) |
| Self-employed | 136 (53%) | 50 (20%) |
| Primary employment-income source | ||
| Casual (on-call, day labour) | -- | 105 (42%) |
| Temporary/fixed term contract | -- | 22 (8.8%) |
| Self-employed | -- | 20 (8.0%) |
| Permanent part-time (<30 h/week)/varied hours | -- | 88 (35%) |
| Permanent full-time (30 h or more/week) | -- | 14 (5.6%) |
| Labour force participation | ||
| Always had formal job or was looking for work | 16 (6.2%) | -- |
| Usually have a job or looking for one | 82 (32%) | -- |
| Vary between working/looking for work and not working/not looking | 78 (30%) | -- |
| Rarely working or looking for work | 66 (26%) | -- |
| Have never had or looked for formal job | 14 (5.5%) | -- |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Richardson, L.; Minh, A.; McCormack, D.; Laing, A.; Barbic, S.; Hayashi, K.; Milloy, M.-J.; Huyser, K.R.; Leahy, K.; Li, J., on behalf of the ASSET Study Team. Cohort Profile: The Assessing Economic Transitions (ASSET) Study—A Community-Based Mixed-Methods Study of Economic Engagement among Inner-City Residents. Int. J. Environ. Res. Public Health 2022, 19, 10456. https://doi.org/10.3390/ijerph191610456
Richardson L, Minh A, McCormack D, Laing A, Barbic S, Hayashi K, Milloy M-J, Huyser KR, Leahy K, Li J on behalf of the ASSET Study Team. Cohort Profile: The Assessing Economic Transitions (ASSET) Study—A Community-Based Mixed-Methods Study of Economic Engagement among Inner-City Residents. International Journal of Environmental Research and Public Health. 2022; 19(16):10456. https://doi.org/10.3390/ijerph191610456
Chicago/Turabian StyleRichardson, Lindsey, Anita Minh, Deb McCormack, Allison Laing, Skye Barbic, Kanna Hayashi, M.-J. Milloy, Kimberly R. Huyser, Kathleen Leahy, and Johanna Li on behalf of the ASSET Study Team. 2022. "Cohort Profile: The Assessing Economic Transitions (ASSET) Study—A Community-Based Mixed-Methods Study of Economic Engagement among Inner-City Residents" International Journal of Environmental Research and Public Health 19, no. 16: 10456. https://doi.org/10.3390/ijerph191610456
APA StyleRichardson, L., Minh, A., McCormack, D., Laing, A., Barbic, S., Hayashi, K., Milloy, M.-J., Huyser, K. R., Leahy, K., & Li, J., on behalf of the ASSET Study Team. (2022). Cohort Profile: The Assessing Economic Transitions (ASSET) Study—A Community-Based Mixed-Methods Study of Economic Engagement among Inner-City Residents. International Journal of Environmental Research and Public Health, 19(16), 10456. https://doi.org/10.3390/ijerph191610456