
Do Different Patterns of Employment Quality Contribute to Gender Health Inequities in the U.S.? A Cross-Sectional Mediation Analysis



Abstract
:1. Introduction
1.1. Employment Quality and Health
1.2. Gender, Employment Quality, and Health
1.3. The Current Study
2. Methods
2.1. Data
2.2. Health Measures
2.3. Construction of Employment Quality Measure
2.4. Gender and Other Covariates
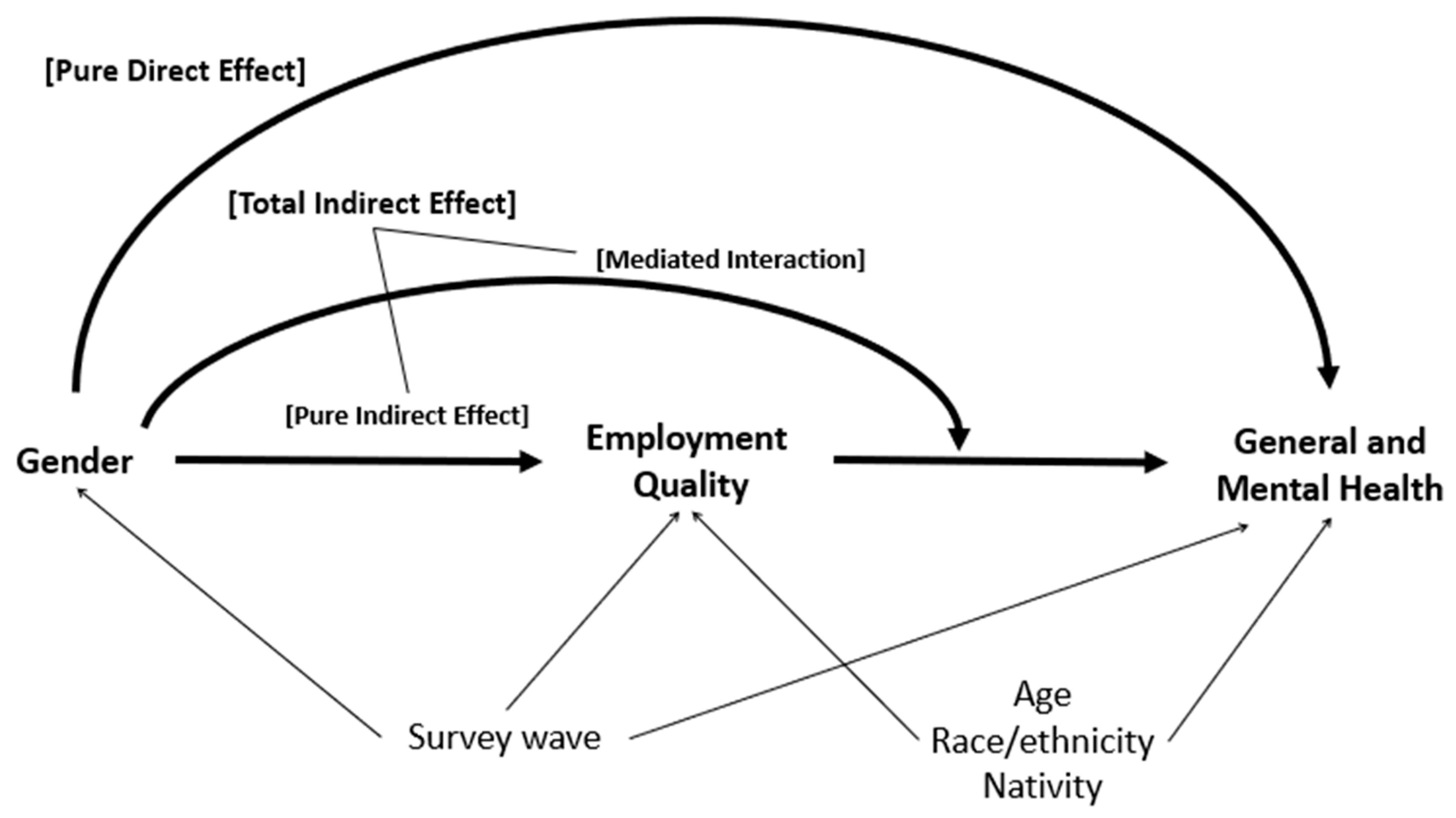
2.5. Analytic Approach
3. Results
4. Discussion
4.1. Application of Mediation Analysis Framework to Examine Potential Role of EQ in Gender Health Inequities
4.2. Accounting for Heterogeneity and Multidimensionality of Employment Relationships to Understand Gendered Labor Market Inequities
4.3. Limitations and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Benach, J.; Vives, A.; Amable, M.; Vanroelen, C.; Tarafa, G.; Muntaner, C. Precarious Employment: Understanding an Emerging Social Determinant of Health. Annu. Rev. Public Health 2014, 35, 229–253. [Google Scholar] [CrossRef] [PubMed]
- Bodin, T.; Çağlayan, Ç.; Garde, A.H.; Gnesi, M.; Jonsson, J.; Kiran, S.; Kreshpaj, B.; Leinonen, T.; Mehlum, I.S.; Nena, E.; et al. Precarious employment in occupational health-an OMEGA-NET working group position paper. Scand. J. Work. Environ. Health 2020, 46, 321–329. [Google Scholar] [CrossRef]
- Kreshpaj, B.; Orellana, C.; Burström, B.; Davis, L.; Hemmingsson, T.; Johansson, G.; Kjellberg, K.; Jonsson, J.; Wegman, D.H.; Bodin, T. What is precarious employment? A systematic review of definitions and operationalizations from quantitative and qualitative studies. Scand. J. Work. Environ. Health 2020, 46, 235–247. [Google Scholar] [CrossRef]
- Kalleberg, A.L. Good Jobs, Bad Jobs: The Rise of Polarized and Precarious Employment Systems in the United States, 1970s–2000s; Russell Sage Foundation: New York, NY, USA, 2011. [Google Scholar] [CrossRef]
- Oddo, V.M.; Zhuang, C.C.; Andrea, S.B.; Eisenberg-Guyot, J.; Peckham, T.; Jacoby, D.; Hajat, A. Changes in precarious employment in the United States: A longitudinal analysis. Scand. J. Work. Environ. Health 2020, 47, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Kim, I.-H.; Muntaner, C.; Shahidi, F.V.; Vives, A.; Vanroelen, C.; Benach, J. Welfare states, flexible employment, and health: A critical review. Health Policy 2011, 104, 99–127. [Google Scholar] [CrossRef]
- Fullerton, H.N.J. Labor Force Participation: 75 Years of Change, 1950–1998 and 1998–2025. Mon. Labor Rev. 1999, 122, 3. [Google Scholar]
- Bird, C.; Rieker, P. Gender and Health: The Effects of Constrained Choices and Social Policies; Cambridge University Press: Cambridge, UK, 2008. [Google Scholar] [CrossRef]
- Artazcoz, L.; Borrell, C.; Benach, J. Gender inequalities in health among workers: The relation with family demands. J. Epidemiol. Community Health 2001, 55, 639–647. [Google Scholar] [CrossRef]
- Campos-Serna, J.; Ronda-Pérez, E.; Artazcoz, L.; Moen, B.E.; Benavides, F.G. Gender inequalities in occupational health related to the unequal distribution of working and employment conditions: A systematic review. Int. J. Equity Health 2013, 12, 57. [Google Scholar] [CrossRef]
- Menéndez, M.; Benach, J.; Muntaner, C.; Amable, M.; O’Campo, P. Is precarious employment more damaging to women’s health than men’s? Soc. Sci. Med. 2007, 64, 776–781. [Google Scholar] [CrossRef]
- Malmusi, D.; Artazcoz, L.; Benach, J.; Borrell, C. Perception or real illness? How chronic conditions contribute to gender inequalities in self-rated health. Eur. J. Public Health 2012, 22, 781–786. [Google Scholar] [CrossRef]
- Barford, A.; Dorling, D.; Smith, G.D.; Shaw, M. Life expectancy: Women now on top everywhere. BMJ 2006, 332, 808. [Google Scholar] [CrossRef] [PubMed]
- Puig-Barrachina, V.; Vanroelen, C.; Vives, A.; Martínez, J.M.; Muntaner, C.; Levecque, K.; Benach, J.; Louckx, F. Measuring employment precariousness in the European Working Conditions Survey: The social distribution in Europe. Work 2014, 49, 143–161. [Google Scholar] [CrossRef]
- Van Aerden, K.; Puig-Barrachina, V.; Bosmans, K.; Vanroelen, C. How does employment quality relate to health and job satisfaction in Europe? A typological approach. Soc. Sci. Med. 2016, 158, 132–140. [Google Scholar] [CrossRef]
- Van Aerden, K.; Moors, G.; Levecque, K.; Vanroelen, C. Measuring Employment Arrangements in the European Labour Force: A Typological Approach. Soc. Indic. Res. 2014, 116, 771–791. [Google Scholar] [CrossRef]
- Julià, M.; Vanroelen, C.; Bosmans, K.; Van Aerden, K.; Benach, J. Precarious Employment and Quality of Employment in Relation to Health and Well-being in Europe. Int. J. Health Serv. 2017, 47, 389–409. [Google Scholar] [CrossRef] [PubMed]
- Peckham, T.; Fujishiro, K.; Hajat, A.; Flaherty, B.; Seixas, N. Evaluating Employment Quality as a Determinant of Health in a Changing Labor Market. RSF Russell Sage Found. J. Soc. Sci. 2019, 5, 258–281. [Google Scholar] [CrossRef]
- Scott-Marshall, H.; Tompa, E. The health consequences of precarious employment experiences. Work 2011, 38, 369–382. [Google Scholar] [CrossRef]
- de Bustillo, R.M.; Fernández-Macías, E.; Antón, J.I.; Esteve, F. Indicators of Job Quality in the European Union; EU: Brussels, Belgium, 2009. [Google Scholar]
- Vives, A.; Amable, M.; Ferrer, M.; Moncada, S.; Llorens, C.; Muntaner, C.; Benavides, F.G.; Benach, J. The Employment Precariousness Scale (EPRES): Psychometric properties of a new tool for epidemiological studies among waged and salaried workers. Occup. Environ. Med. 2010, 67, 548–555. [Google Scholar] [CrossRef]
- Eisenberg-Guyot, J.; Peckham, T.; Andrea, S.B.; Oddo, V.; Seixas, N.; Hajat, A. Life-course trajectories of employment quality and health in the U.S.: A multichannel sequence analysis. Soc. Sci. Med. 2020, 264, 113327. [Google Scholar] [CrossRef] [PubMed]
- Vanroelen, C. Employment Quality: An Overlooked Determinant of Workers’ Health and Well-being? Ann. Work Expo. Health 2019, 63, 619–623. [Google Scholar] [CrossRef] [PubMed]
- Gevaert, J.; Van Aerden, K.; De Moortel, D.; Vanroelen, C. Employment Quality as a Health Determinant: Empirical Evidence for the Waged and Self-Employed. Work Occup. 2020, 48, 146–183. [Google Scholar] [CrossRef]
- Van Aerden, K.; Gadeyne, S.; Vanroelen, C. Is any job better than no job at all? Studying the relations between employment types, unemployment and subjective health in Belgium. Arch. Public Health 2017, 75, 55. [Google Scholar] [CrossRef]
- Peckham, T.; Flaherty, B.; Hajat, A.; Fujishiro, K.; Jacoby, D.; Seixas, N. What Does Non-standard Employment Look Like in the United States? An Empirical Typology of Employment Quality. Soc. Indic. Res. 2022, 163, 555–583. [Google Scholar] [CrossRef]
- Andrea, S.B.; Eisenberg-Guyot, J.; Oddo, V.M.; Peckham, T.; Jacoby, D.; Hajat, A. Beyond Hours Worked and Dollars Earned: Multidimensional EQ, Retirement Trajectories and Health in Later Life. Work Aging Retire. 2021, 8, 51–73. [Google Scholar] [CrossRef] [PubMed]
- Artazcoz, L.; Borrell, C.; Cortàs, I.; Escribà-Agüir, V.; Cascant, L. Occupational epidemiology and work related inequalities in health: A gender perspective for two complementary approaches to work and health research. J. Epidemiol. Community Health 2007, 61, ii39–ii45. [Google Scholar] [CrossRef]
- Charles, M.; Bradley, K. Indulging Our Gendered Selves? Sex Segregation by Field of Study in 44 Countries. Am. J. Sociol. 2009, 114, 924–976. [Google Scholar] [CrossRef]
- Smith, M.; Piasna, A.; Burchell, B.; Rubery, J.; Rafferty, A.; Rose, J.; Carter, L. Women, Men and Working Conditions in Europe; Eurofound: Luxembourg, 2013. [Google Scholar]
- Blau, F.D.; DeVaro, J. New Evidence on Gender Differences in Promotion Rates: An Empirical Analysis of a Sample of New Hires. Ind. Relat. A J. Econ. Soc. 2007, 46, 511–550. [Google Scholar] [CrossRef]
- Artazcoz, L.; Artieda, L.; Borrell, C.; Cortès, I.; Benach, J.; García, V. Combining job and family demands and being healthy: What are the differences between men and women? Eur. J. Public Health 2004, 14, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Borrell, C.; Muntaner, C.; Benach, J.; Artazcoz, L. Social class and self-reported health status among men and women: What is the role of work organisation, household material standards and household labour? Soc. Sci. Med. 2004, 58, 1869–1887. [Google Scholar] [CrossRef]
- Moreno-Colom, S. The gendered division of housework time: Analysis of time use by type and daily frequency of household tasks. Time Soc. 2017, 26, 3–27. [Google Scholar] [CrossRef]
- Levanon, A.; England, P.; Allison, P. Occupational Feminization and Pay: Assessing Causal Dynamics Using 1950-2000 U.S. Census Data. Soc. Forces 2009, 88, 865–891. [Google Scholar] [CrossRef]
- Matthews, S.; Hertzman, C.; Ostry, A.; Power, C. Gender, work roles and psychosocial work characteristics as determinants of health. Soc. Sci. Med. 1998, 46, 1417–1424. [Google Scholar] [CrossRef]
- Franklin, P.; Zwysen, W.; Piasna, A. Temporal Dimensions of Job Quality and Gender: Exploring Differences in the Associations of Working Time and Health between Women and Men. Int. J. Environ. Res. Public Health 2022, 19, 4456. [Google Scholar] [CrossRef]
- Harnois, C.E.; Bastos, J.L. Discrimination, Harassment, and Gendered Health Inequalities: Do Perceptions of Workplace Mistreatment Contribute to the Gender Gap in Self-reported Health? J. Health Soc. Behav. 2018, 59, 283–299. [Google Scholar] [CrossRef]
- Ahonen, E.Q.; Fujishiro, K.; Brown, S.; Wang, Y.; Palumbo, A.; Michael, Y. Gendered exposures: Exploring the role of paid and unpaid work throughout life in U.S. women’s cardiovascular health. Crit. Public Health 2020, 32, 357–367. [Google Scholar] [CrossRef]
- Wharton, C.S. Finding time for the ‘second shift’: The Impact of Flexible Work Schedules on Women’s Double Days. Gend. Soc. 1994, 8, 189–205. [Google Scholar] [CrossRef]
- Rieker, P.P.; Read, J.G. The Health Gender Gap: A Constrained Choice Explanation. A Constrained Choice Explanation. In The Psychology of Gender and Health: Conceptual and Applied Global Concerns; Elsevier Inc.: Oxford, UK, 2017; pp. 85–118. [Google Scholar]
- Winkler, M.R.; Telke, S.; Ahonen, E.Q.; Crane, M.M.; Mason, S.M.; Neumark-Sztainer, D. Constrained choices: Combined influences of work, social circumstances, and social location on time-dependent health behaviors. SSM Popul. Health 2020, 11, 100562. [Google Scholar] [CrossRef]
- Kim, I.-H.; Muntaner, C.; Khang, Y.-H.; Paek, D.; Cho, S.-I. The relationship between nonstandard working and mental health in a representative sample of the South Korean population. Soc. Sci. Med. 2006, 63, 566–574. [Google Scholar] [CrossRef]
- Pirani, E.; Salvini, S. Is temporary employment damaging to health? A longitudinal study on Italian workers. Soc. Sci. Med. 2015, 124, 121–131. [Google Scholar] [CrossRef] [Green Version]
- Vives, A.; Amable, M.; Ferrer, M.; Moncada, S.; Llorens, C.; Muntaner, C.; Benavides, F.G.; Benach, J. Employment Precariousness and Poor Mental Health: Evidence from Spain on a New Social Determinant of Health. J. Environ. Public Health 2013, 2013, 978656. [Google Scholar] [CrossRef]
- Williams, J.C.; Blair-Loy, M.; Berdahl, J.L. Cultural Schemas, Social Class, and the Flexibility Stigma. J. Soc. Issues 2013, 69, 209–234. [Google Scholar] [CrossRef]
- Vandello, J.A.; Hettinger, V.E.; Bosson, J.K.; Siddiqi, J. When Equal Isn’t Really Equal: The Masculine Dilemma of Seeking Work Flexibility. J. Soc. Issues 2013, 69, 303–321. [Google Scholar] [CrossRef]
- Smith, T.W.; Davern, M.; Freese, J.; Morgan, S.L. General Social Surveys, 1972–2018 [Machine-Readable Data File]. 2019. Available online: https://gss.norc.org/get-the-data (accessed on 14 December 2019).
- DeSalvo, K.B.; Bloser, N.; Reynolds, K.; He, J.; Muntner, P. Mortality prediction with a single general self-rated health question. A meta-analysis. J. Gen. Intern. Med. 2006, 21, 267–275. [Google Scholar] [CrossRef]
- Zajacova, A.; Dowd, J. Reliability of Self-rated Health in US Adults. Am. J. Epidemiol. 2011, 174, 977–983. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Self-reported frequent mental distress among adults—United States, 1993–1996. MMWR Morb. Mortal. Wkly. Rep. 1998, 47, 326. [Google Scholar]
- Centers for Disease Control and Prevention. Self-reported frequent mental distress among adults—United States, 1993–2001. MMWR. Morb. Mortal. Wkly. Rep. 2004, 53, 963. [Google Scholar]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide; Eighth Edition; Muthén & Muthén: Los Angeles, CA, USA, 2017. [Google Scholar]
- Krieger, N. Genders, sexes, and health: What are the connections—and why does it matter? Int. J. Epidemiol. 2003, 32, 652–657. [Google Scholar] [CrossRef]
- Vander Weele, T.J. A Three-way Decomposition of a Total Effect into Direct, Indirect, and Interactive Effects. Source Epidemiol. 2013, 24, 224–232. [Google Scholar] [CrossRef] [PubMed]
- Glymour, M.M.; Spiegelman, D. Evaluating Public Health Interventions: 5. Causal Inference in Public Health Research—Do Sex, Race, and Biological Factors Cause Health Outcomes? Am. J. Public Health 2017, 107, 81–85. [Google Scholar] [CrossRef]
- VanderWeele, T.J.; Robinson, W. On the Causal Interpretation of Race in Regressions Adjusting for Confounding and Mediating Variables. Epidemiology 2014, 25, 473–484. [Google Scholar] [CrossRef] [PubMed]
- McLarnon, M.J.W.; O’Neill, T. Extensions of Auxiliary Variable Approaches for the Investigation of Mediation, Moderation, and Conditional Effects in Mixture Models. Organ. Res. Methods 2018, 21, 955–982. [Google Scholar] [CrossRef]
- Muthén, B. Applications of Causally Defined Direct and Indirect Effects in Mediation Analysis Using SEM in Mplus; University of California: Los Angeles, CA, USA, 2011. [Google Scholar]
- Vermunt, J.K. Latent Class Modeling with Covariates: Two Improved Three-Step Approaches. Politi Anal. 2010, 18, 450–469. [Google Scholar] [CrossRef]
- Nylund-Gibson, K.; Grimm, R.P.; Masyn, K.E. Prediction from Latent Classes: A Demonstration of Different Approaches to Include Distal Outcomes in Mixture Models. Struct. Equ. Model. A Multidiscip. J. 2019, 26, 967–985. [Google Scholar] [CrossRef]
- Bauer, G.R.; Scheim, A.I. Methods for analytic intercategorical intersectionality in quantitative research: Discrimination as a mediator of health inequalities. Soc. Sci. Med. 2019, 226, 236–245. [Google Scholar] [CrossRef]
- Preacher, K.J.; Selig, J. Advantages of Monte Carlo Confidence Intervals for Indirect Effects. Commun. Methods Meas. 2012, 6, 77–98. [Google Scholar] [CrossRef]
- MacKinnon, D.P.; Krull, J.L.; Lockwood, C.M. Equivalence of the Mediation, Confounding and Suppression Effect. Prev. Sci. 2000, 1, 173–181. [Google Scholar] [CrossRef]
- Chun, H.; Khang, Y.-H.; Kim, I.-H.; Cho, S.-I. Explaining gender differences in ill-health in South Korea: The roles of socio-structural, psychosocial, and behavioral factors. Soc. Sci. Med. 2008, 67, 988–1001. [Google Scholar] [CrossRef] [PubMed]
- Hosseinpoor, A.R.; Williams, J.S.; Amin, A.; De Carvalho, I.A.; Beard, J.; Boerma, T.; Kowal, P.; Naidoo, N.; Chatterji, S. Social Determinants of Self-Reported Health in Women and Men: Understanding the Role of Gender in Population Health. PLoS ONE 2012, 7, e34799. [Google Scholar] [CrossRef]
- Ross, C.E.; Bird, C.E. Sex Stratification and Health Lifestyle: Consequences for Men’s and Women’s Perceived Health. J. Health Soc. Behav. 1994, 35, 161–178. [Google Scholar] [CrossRef] [PubMed]
- Gray, B.J.; Grey, C.; Hookway, A.; Homolova, L.; Davies, A.R. Differences in the impact of precarious employment on health across population subgroups: A scoping review. Perspect. Public Health 2021, 141, 37–49. [Google Scholar] [CrossRef]
- Goldin, C. A Grand Gender Convergence: Its Last Chapter. Am. Econ. Rev. 2014, 104, 1091–1119. [Google Scholar] [CrossRef] [Green Version]
- Cotter, D.A.; Hermsen, J.M.; Ovadia, S.; Vanneman, R. The glass ceiling. Soc. Forces 2001, 80, 655–681. [Google Scholar] [CrossRef]
- Quesnel-Vallée, A.; DeHaney, S.; Ciampi, A. Temporary work and depressive symptoms: A propensity score analysis. Soc. Sci. Med. 2010, 70, 1982–1987. [Google Scholar] [CrossRef]
- Valero, E.; Martin, U.; Bacigalupe, A.; Utzet, M. The impact of precarious jobs on mental health: A gender-sensitive literature review. In International Archives of Occupational and Environmental Health; Springer Science and Business Media Deutschland GmbH: Berlin, Germany, 2020; pp. 1–13. [Google Scholar] [CrossRef]
- Andrea, S.B.; Eisenberg-Guyot, J.; Peckham, T.; Oddo, V.M.; Hajat, A. Intersectional trends in employment quality in older adults in the United States. SSM Popul. Health 2021, 15, 100868. [Google Scholar] [CrossRef] [PubMed]
- Fujishiro, K.; Ahonen, E.Q.; Winkler, M. Poor-quality employment and health: How a welfare regime typology with a gender lens Illuminates a different work-health relationship for men and women. Soc. Sci. Med. 2021, 291, 114484. [Google Scholar] [CrossRef] [PubMed]
- Padrosa, E.; Vanroelen, C.; Muntaner, C.; Benach, J.; Julià, M. Precarious employment and mental health across European welfare states: A gender perspective. Int. Arch. Occup. Environ. Health 2022, 95, 1463–1480. [Google Scholar] [CrossRef]
- De Moortel, D.; Vandenheede, H.; Vanroelen, C. Contemporary employment arrangements and mental well-being in men and women across Europe: A cross-sectional study. Int. J. Equity Health 2014, 13, 90. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Label | % of Wage Earners | Character of EQ Type |
|---|---|---|
| SER-like | 28 | These jobs have generally favorable EQ features, including a permanent arrangement, full-time hours, adequate wages, working during the day shift, and with adequate information/equipment to complete work. They also have moderate levels of schedule control and development opportunities and are unlikely to experience excessive work hours or workplace harassment. |
| Portfolio | 17 | These jobs have permanent arrangements, standard day shifts, and low levels of harassment; however, they are distinguished by having the highest income, employee involvement, development opportunity, and degree of schedule control of all of the EQ types. On the other hand, they work long hours. |
| Inflexible skilled | 15 | The jobs have high wages, opportunities to develop abilities, union representation, and involvement in decision-making; however, these jobs are also characterized by a high probability of irregular shifts, low schedule control, workplace harassment, long hours, and mandatory extra work. |
| Dead-end | 14 | These jobs have permanent arrangements with adequate wages and high union representation; however, workers in these jobs generally experience poor worker–employer relations. This EQ type has the lowest levels of opportunity to develop and is most likely to report inadequate information, equipment, and training to perform their work. They also lack control over their schedule or involvement in decision-making, and experience high workplace harassment. |
| Precarious | 13 | These jobs have generally poor EQ features. From a contractual perspective, these jobs have a high probability of non-permanent working arrangements, low wages, non-full-time hours, and irregular shifts. From a relational perspective, this group has very low development opportunity, schedule control, union representation, and employee involvement, as well as experiencing high workplace harassment. |
| Optimistic precarious | 13 | This type is like the Precarious EQ type in terms of contractual features; however, they experience high levels of development opportunity, schedule control, and employee involvement, as well as having a lower probability of encountering harassment at work. |
| Measure | Level | Total | Women | Men | p-Value b |
|---|---|---|---|---|---|
| n = 6367 a | n = 3405 | n = 2962 | |||
| Survey wave | 2002 | 1542 (24) | 803 (24) | 739 (25) | 0.536 |
| 2006 | 1489 (23) | 801 (24) | 688 (23) | ||
| 2010 | 1011 (16) | 562 (17) | 449 (15) | ||
| 2014 | 1068 (17) | 568 (17) | 500 (17) | ||
| 2018 | 1257 (20) | 671 (20) | 586 (20) | ||
| Age | 30 and under | 1521 (24) | 796 (23) | 725 (24) | 0.167 |
| 31–50 | 3077 (48) | 1630 (48) | 1447 (49) | ||
| Over 50 | 1769 (28) | 979 (29) | 790 (27) | ||
| Race/ethnicity | White | 4339 (68) | 2255 (66) | 2084 (70) | <0.001 |
| Black | 1004 (16) | 624 (18) | 380 (13) | ||
| Hispanic | 747 (12) | 380 (11) | 367 (12) | ||
| Asian/Pacific Is. | 202 (3) | 103 (3) | 99 (3) | ||
| AI/AN c | 75 (1) | 43 (1) | 32 (1) | ||
| Nativity | Born in U.S. | 5629 (88) | 3050 (90) | 2579 (87) | 0.002 |
| Foreign born | 738 (12) | 355 (10) | 383 (13) | ||
| Employment quality type d | SER-like | 2086 (33) | 1231 (36) | 855 (29) | <0.001 |
| Portfolio | 1041 (16) | 378 (11) | 663 (22) | ||
| Inflexible Skilled | 847 (13) | 349 (10) | 498 (17) | ||
| Dead-end | 832 (13) | 406 (12) | 426 (14) | ||
| Precarious | 768 (12) | 515 (15) | 253 (9) | ||
| Optimistic Precarious | 793 (12) | 526 (15) | 267 (9) | ||
| Self-rated Health | Good | 5438 (85) | 2896 (85) | 2542 (86) | 0.597 |
| Poor | 897 (14) | 490 (14) | 407 (14) | ||
| Missing e | 32 (1) | 19 (1) | 13 (0) | ||
| Frequent mental distress | Absent | 5646 (89) | 2974 (87) | 2672 (90) | 0.002 |
| Present | 650 (10) | 388 (11) | 262 (9) | ||
| Missing e | 71 (1) | 43 (1) | 28 (1) |
| Self-Rated Health n = 6335 | Frequent Mental Distress n = 6296 | |||||||
|---|---|---|---|---|---|---|---|---|
| Probability Difference | (95% CI) | Odd Ratio | (95% CI) | Probability Difference | (95% CI) | Odd Ratio | (95% CI) | |
| Total Effect | −0.003 | (−0.021, 0.015) | 0.97 | (0.78, 1.19) | 0.039 | (0.009, 0.069) | 1.34 | (1.07, 1.67) |
| Pure Direct Effect | −0.018 | (−0.036, −0.001) | 0.79 | (0.63, 1.00) | 0.013 | (−0.016, 0.044) | 1.11 | (0.88, 1.41) |
| Total Indirect Effect | 0.015 | (0.005, 0.028) | 1.22 | (1.06, 1.41) | 0.026 | (0.006, 0.046) | 1.21 | (1.05, 1.39) |
| Pure Indirect Effect | 0.023 | (0.010, 0.038) | −0.003 | (−0.024, 0.019) | ||||
| Mediated interaction | −0.008 | (−0.024, 0.008) | 0.029 | (0.004, 0.055) | ||||
| EQ Type | Predicted EQ Distribution a | Predicted Poor SRH | Predicted FMD | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Women | Men | Women | Men | Women | Men | |||||||
| SER-like | 0.285 | (0.22, 0.35) | 0.201 | (0.15, 0.26) | 0.073 | (0.05, 0.11) | 0.076 | (0.04, 0.12) | 0.107 | (0.06, 0.16) | 0.044 | (0.00, 0.11) |
| Portfolio | 0.046 | (0.03, 0.08) | 0.175 | (0.11, 0.25) | 0.014 | (0.00, 0.05) | 0.030 | (0.01, 0.05) | 0.081 | (0.01, 0.17) | 0.094 | (0.05, 0.16) |
| Inflexible skilled | 0.116 | (0.08, 0.16) | 0.233 | (0.17, 0.30) | 0.073 | (0.03, 0.14) | 0.055 | (0.03, 0.09) | 0.126 | (0.05, 0.23) | 0.167 | (0.11, 0.24) |
| Dead-end | 0.080 | (0.05, 0.12) | 0.136 | (0.09, 0.19) | 0.111 | (0.07, 0.18) | 0.153 | (0.11, 0.22) | 0.206 | (0.12, 0.31) | 0.240 | (0.15, 0.34) |
| Precarious | 0.215 | (0.15, 0.30) | 0.106 | (0.07, 0.16) | 0.160 | (0.11, 0.22) | 0.149 | (0.08, 0.24) | 0.329 | (0.24, 0.42) | 0.219 | (0.11, 0.35) |
| Optimistic precarious | 0.258 | (0.19, 0.33) | 0.149 | (0.11, 0.20) | 0.078 | (0.05, 0.12) | 0.176 | (0.11, 0.27) | 0.170 | (0.10, 0.25) | 0.136 | (0.05, 0.24) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peckham, T.; Seixas, N.; de Castro, A.B.; Hajat, A. Do Different Patterns of Employment Quality Contribute to Gender Health Inequities in the U.S.? A Cross-Sectional Mediation Analysis. Int. J. Environ. Res. Public Health 2022, 19, 11237. https://doi.org/10.3390/ijerph191811237
Peckham T, Seixas N, de Castro AB, Hajat A. Do Different Patterns of Employment Quality Contribute to Gender Health Inequities in the U.S.? A Cross-Sectional Mediation Analysis. International Journal of Environmental Research and Public Health. 2022; 19(18):11237. https://doi.org/10.3390/ijerph191811237
Chicago/Turabian StylePeckham, Trevor, Noah Seixas, A. B. de Castro, and Anjum Hajat. 2022. "Do Different Patterns of Employment Quality Contribute to Gender Health Inequities in the U.S.? A Cross-Sectional Mediation Analysis" International Journal of Environmental Research and Public Health 19, no. 18: 11237. https://doi.org/10.3390/ijerph191811237
APA StylePeckham, T., Seixas, N., de Castro, A. B., & Hajat, A. (2022). Do Different Patterns of Employment Quality Contribute to Gender Health Inequities in the U.S.? A Cross-Sectional Mediation Analysis. International Journal of Environmental Research and Public Health, 19(18), 11237. https://doi.org/10.3390/ijerph191811237