
NDIS Participants with Psychosocial Disabilities and Life-Limiting Diagnoses: A Scoping Review



Abstract
:1. Introduction
The interactions of people with disability with the NDIS and other service systems should be as seamless as possible, where integrated planning and coordinated supports, referrals and transitions are promoted, supported by a no wrong door approach.[2] (p1)
2. Methods
2.1. Development of Key Lines of Enquiry
- What information is available regarding the NDIS experiences of participants living with psychosocial disabilities?
- What information is available regarding the death, dying, and palliative care supports and experiences of NDIS participants?
- What information is available regarding the death, dying, and palliative care experiences of people living with psychosocial disabilities?
2.2. Publication Search Considerations
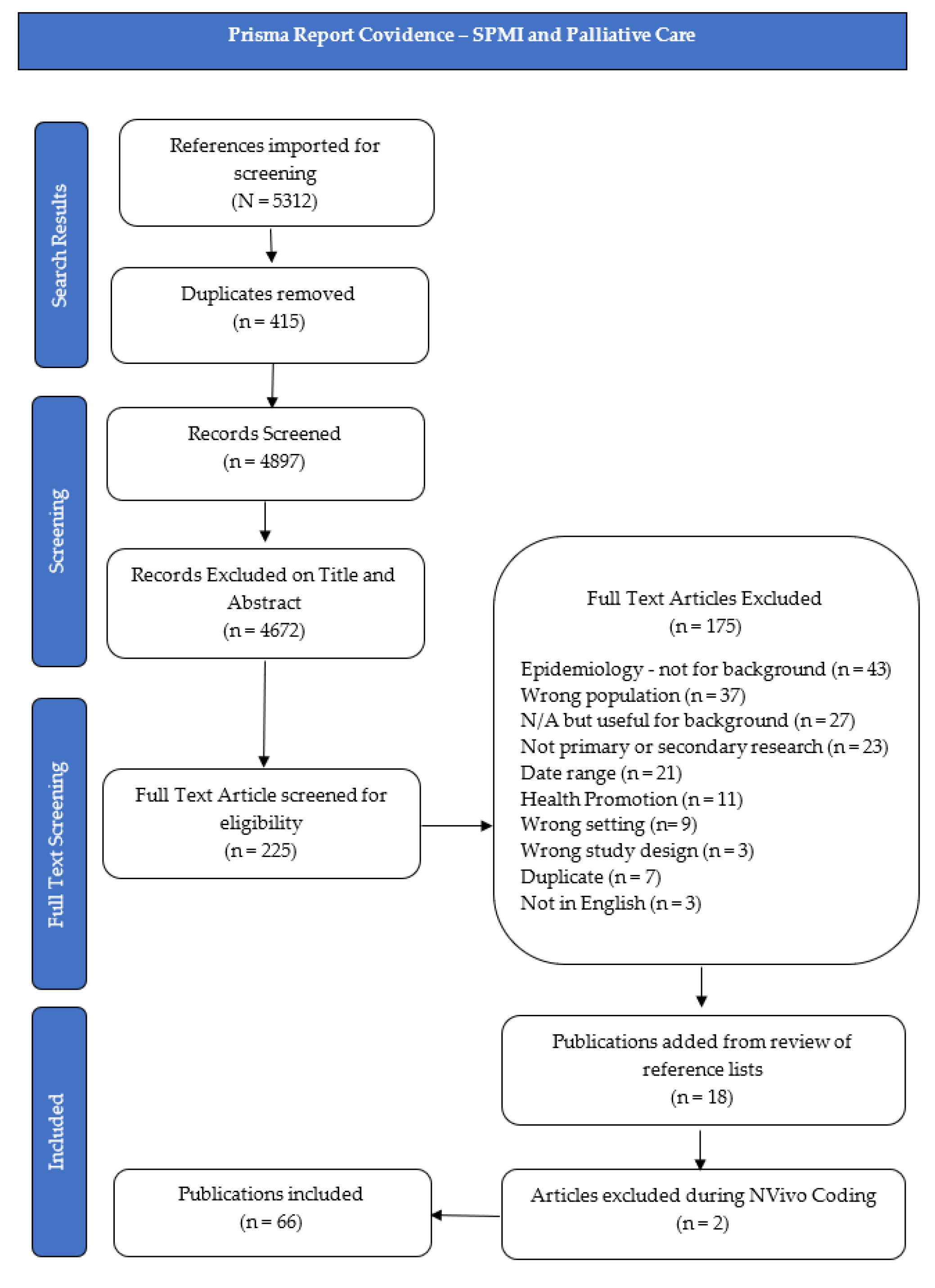
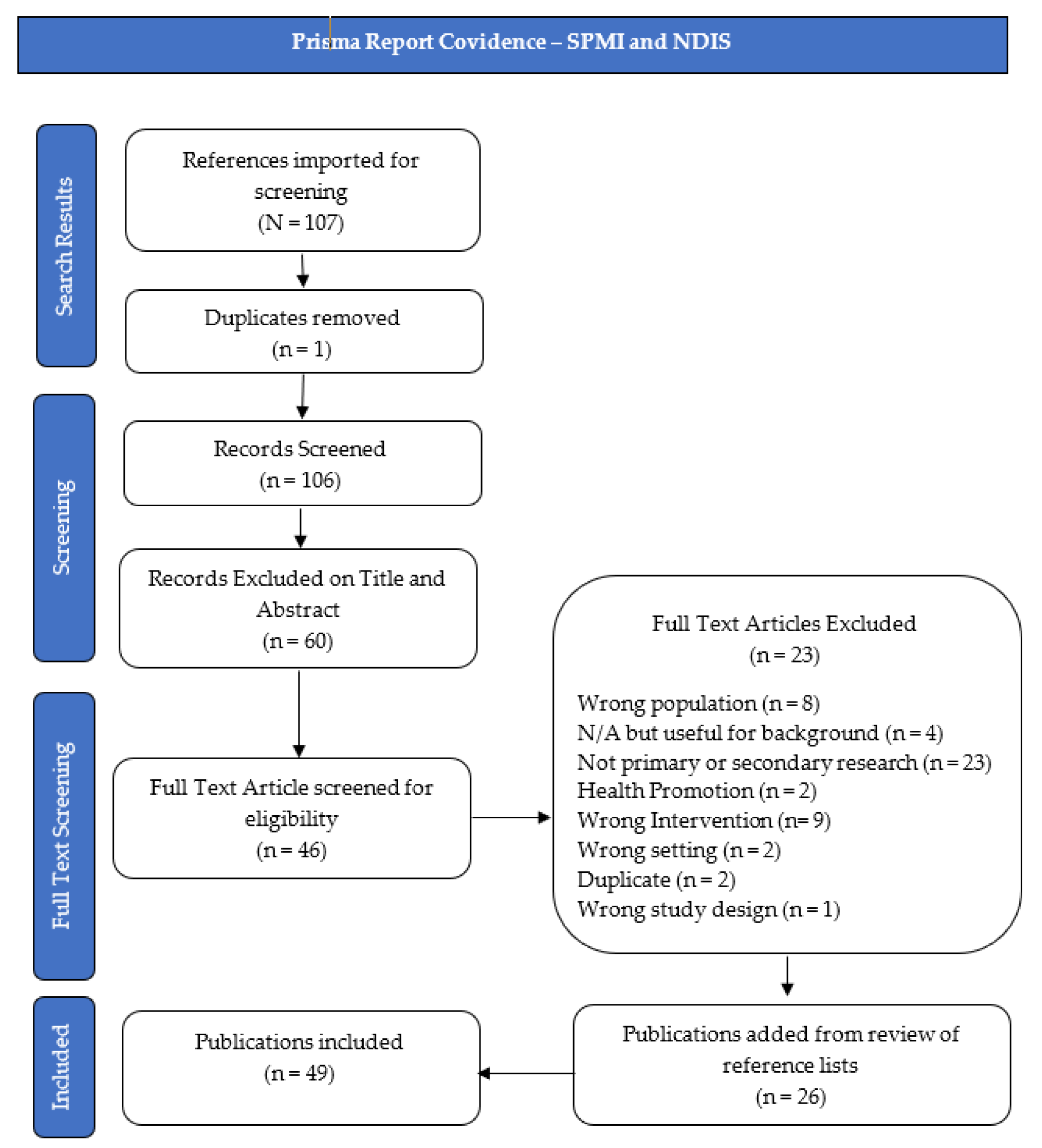
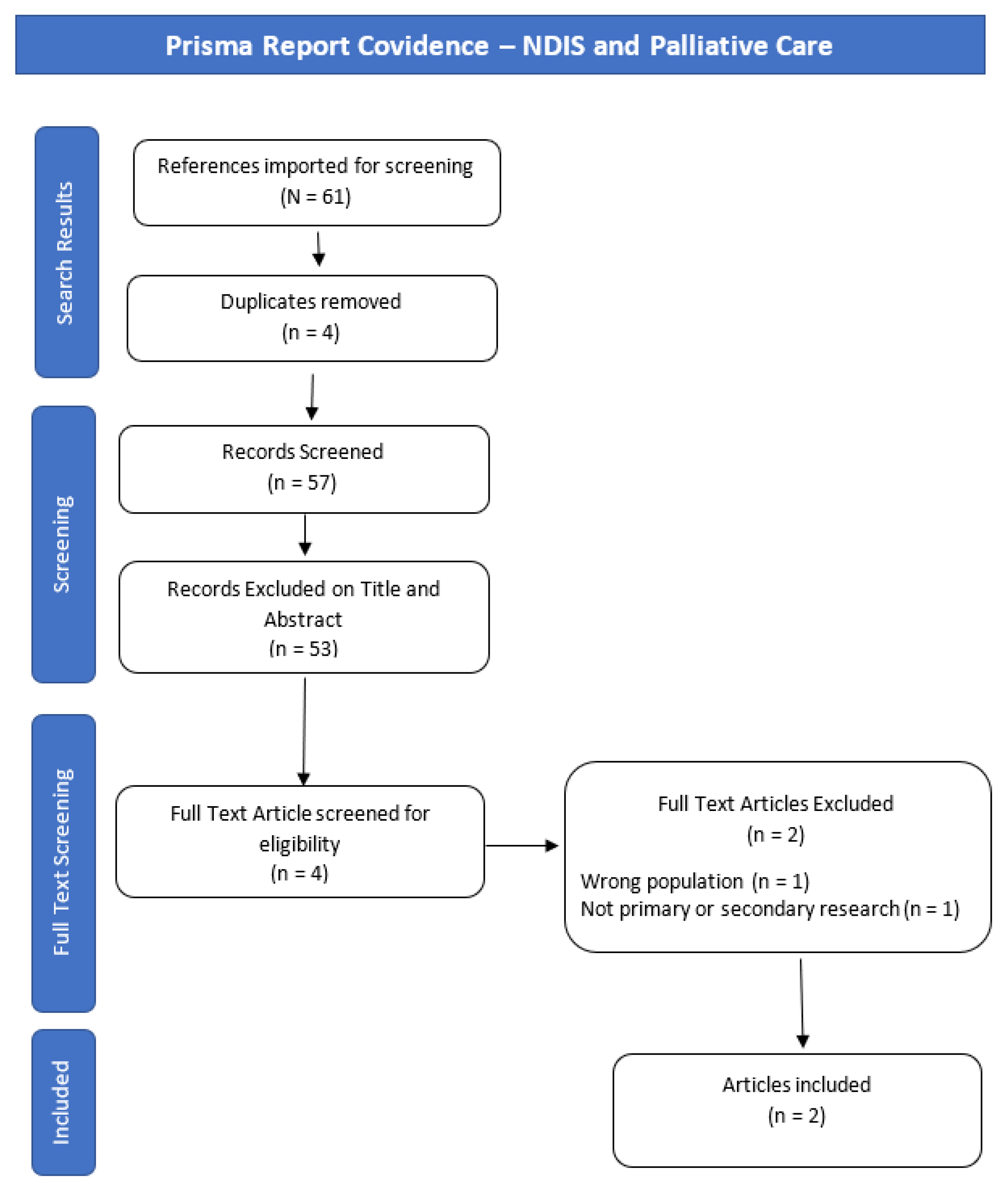
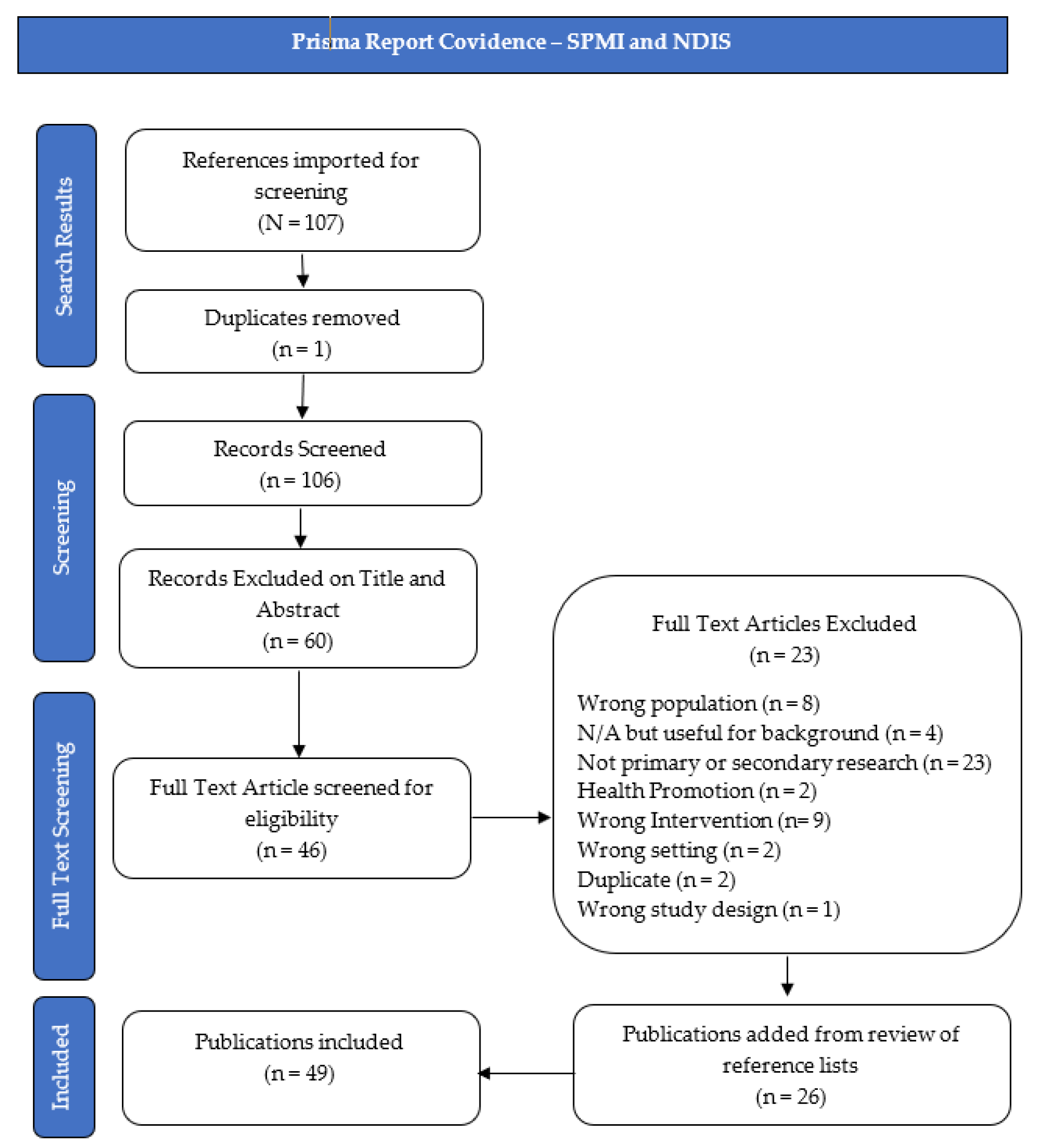
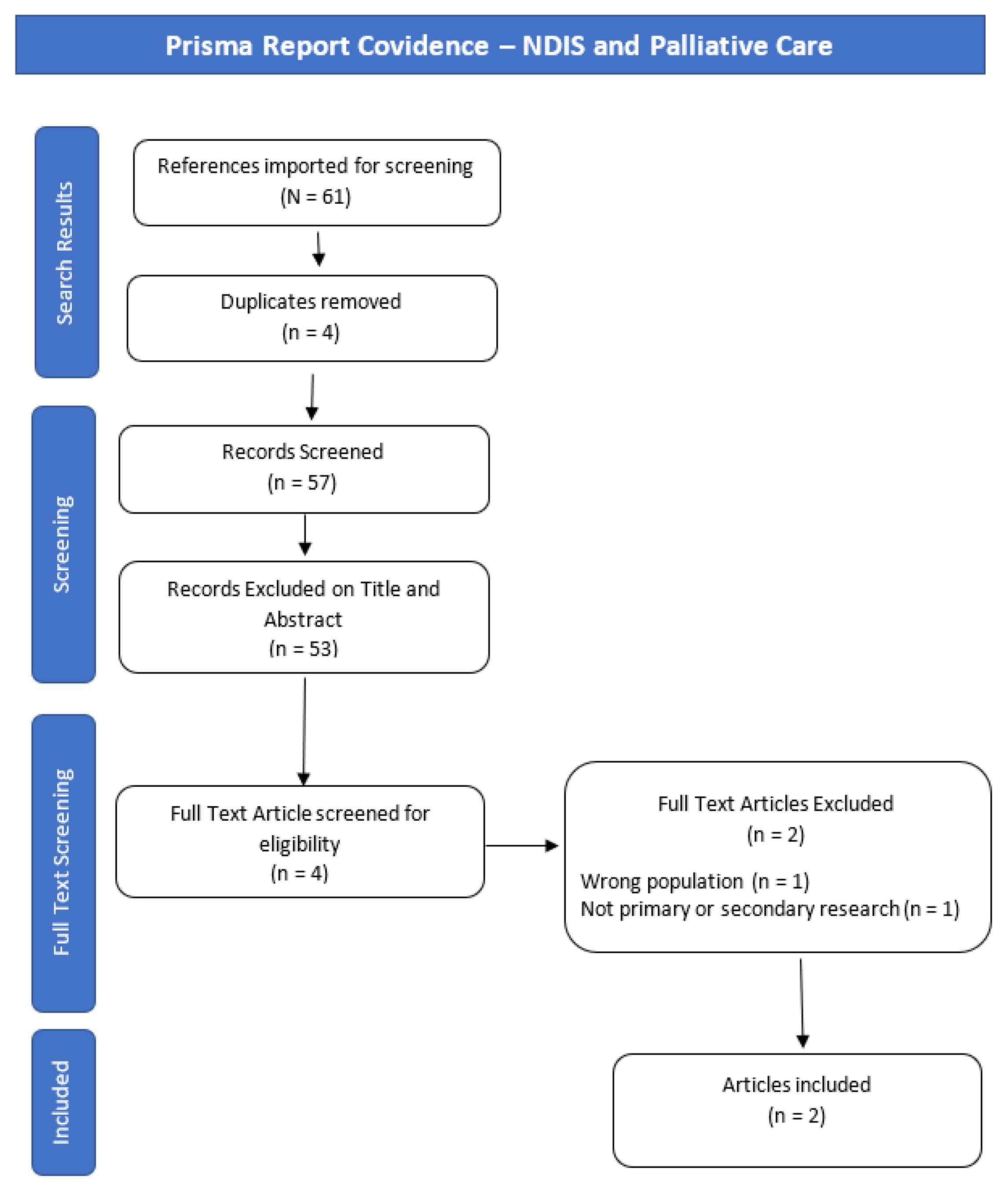
2.3. Publication Selection
3. Results
- What information is available regarding the NDIS experiences of participants living with psychosocial disabilities?
- What information is available regarding the death, dying, and palliative care supports and experiences of NDIS participants?
- What information is available regarding the death, dying, and palliative care experiences of people living with psychosocial disabilities?
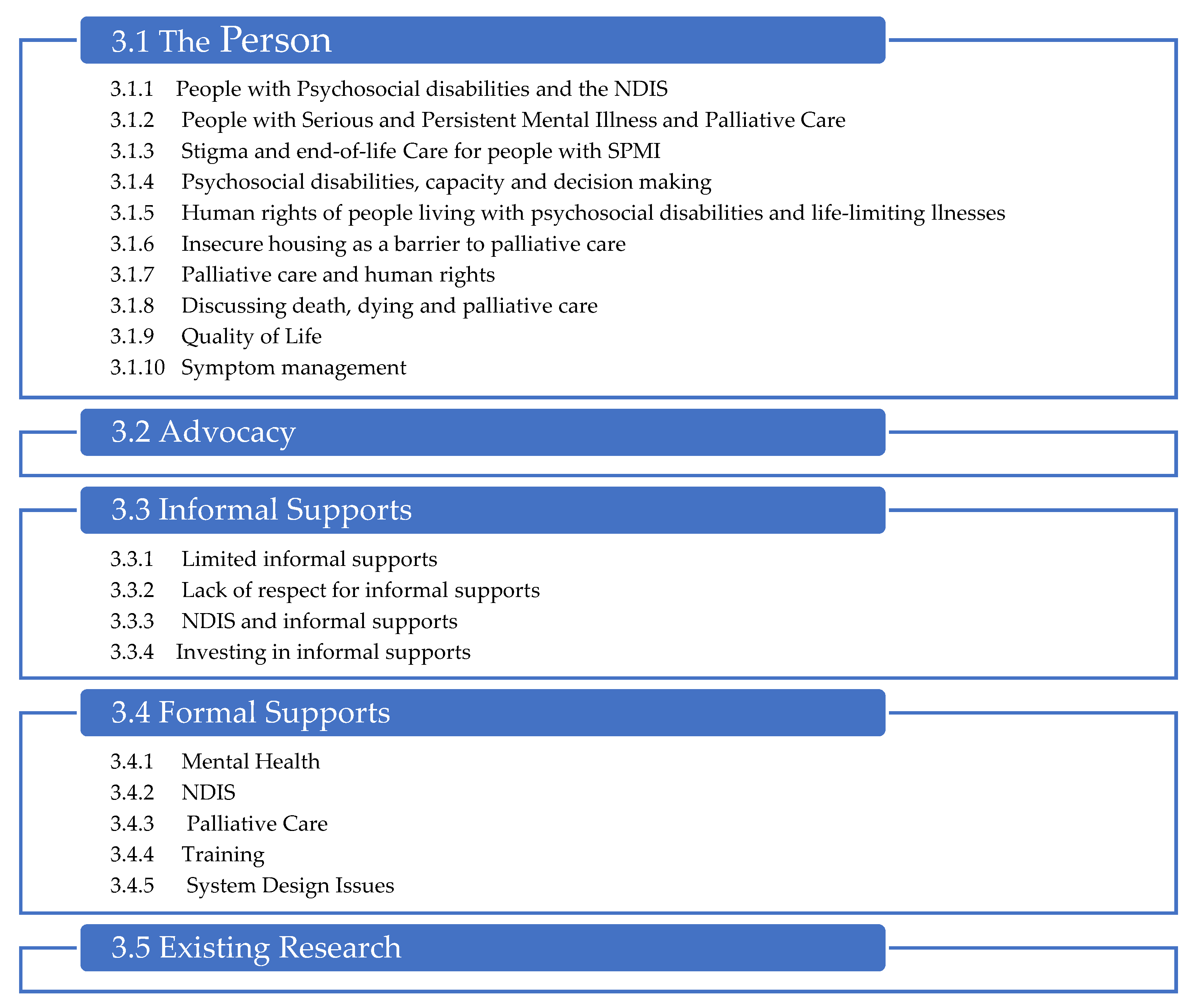
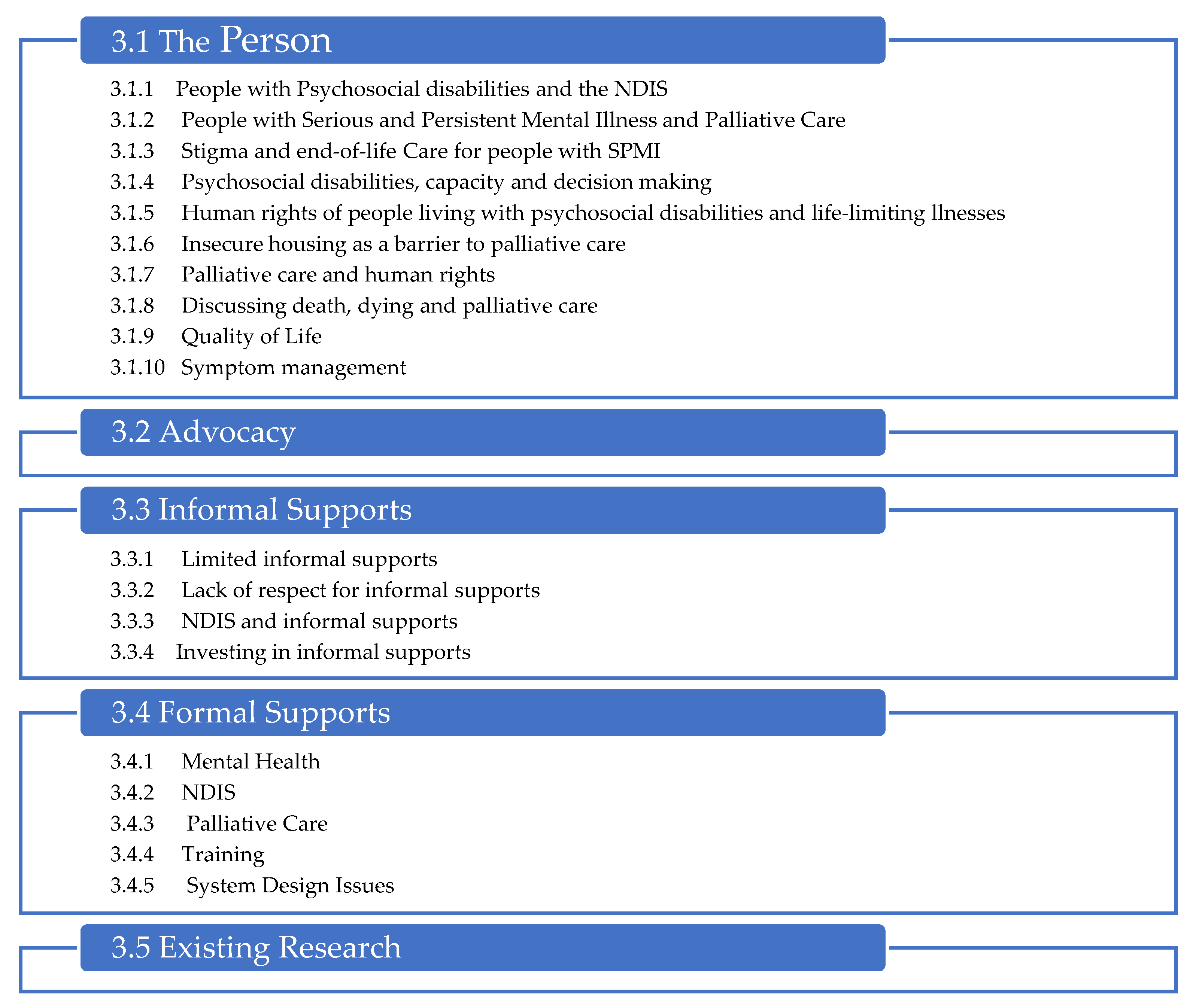
3.1. The Person
3.1.1. People with Psychosocial Disabilities and the NDIS
3.1.2. People with Serious and Persistent Mental Illness and Palliative Care
3.1.3. Stigma and End-of-Life Care for People with SPMI
3.1.4. Psychosocial Disabilities, Capacity and Decision-Making
3.1.5. Human Rights of People Living with Psychosocial Disabilities and Life-Limiting Illnesses
3.1.6. Insecure Housing as a Barrier to Palliative Care
3.1.7. Palliative Care and Human Rights
3.1.8. Discussing Death, Dying and Palliative Care
3.1.9. Quality of Life
3.1.10. Symptom Management
3.2. Advocacy
3.3. Informal Supports
3.3.1. Limited Informal Supports
3.3.2. Lack of Respect for Informal Supports
3.3.3. NDIS and Informal Supports
3.3.4. Investing in Informal Supports
3.4. Formal Supports
3.4.1. Mental Health
3.4.2. NDIS
3.4.3. Palliative Care
3.4.4. Training
3.4.5. System Design Issues
3.5. Existing Research
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Themes | Search Terms |
|---|---|
| NDIS String (National Disability Insurance) OR NDIS OR NDIA OR (disabilit* AND personal budget*) OR (user led organi*) OR (individuali* funding package*) NOT (neurodevelopmental impairments) NOT (national death information system) NOT (naphthalene diimides) NOT (neck disability indices) NOT (non-drug interventions) SPMI String (severe persistent mental adj2 illness) or SPMI or (psychosocial adj2 disability) or schizo* or (bipolar adj2 disorder) Palliative, Death, and Dying String Palliative or death or dying or (life adj1 limiting) or (end adj3 life) or (end adj1 stage) NOT (geriatric or euthanasia or COVID-19 or Alzheimer* or dementia or rat* or infant* or child* or adolescent or youth or dialysis or pharmac* or trauma or veteran or military or (cell adj3 death) or (death adj2 anxiety) or (death adj3 tumo*)) |
| Themes | Search Terms |
|---|---|
| Psychinfo Themes
| NDIS String (National Disability Insurance) OR NDIS OR NDIA OR (disabilit* AND personal budget*) OR (user led organi*) OR (individuali* funding package*) NOT (neurodevelopmental impairments) NOT (national death information system) NOT (naphthalene diimides) NOT (neck disability indices) NOT (non-drug interventions) SPMI String (severe persistent mental adj2 illness) or SPMI or (psychosocial adj2 disability) or schizo* or (Bipolar adj2 Disorder) Palliative, Death, and Dying String Palliative or death or dying or (life adj1 limiting) or (end adj3 life) or (end adj1 stage) NOT (geriatric or euthanasia or COVID-19 or Alzheimer* or dementia or rat* or infant* or child* or adolescent or youth or dialysis or pharmac* or trauma or veteran or military or (cell adj3 death) or (death adj2 anxiety) or (death adj3 tumo*)) |
| Themes | Search Terms |
|---|---|
| Theme 1-NDIS and SPMI “National Disability Insurance” OR ndis OR ndia OR “disabilit* AND personal budget*” OR “user led organi*” OR “individuali* funding package*” NOT “neurodevelopmental impairments” OR “national death information system” OR “naphthalene diimides” OR “neck disability indices” OR “non-drug interventions” AND “severe and persistent mental illness” OR SPMI OR “psychosocial disability” OR schizophrenia OR schizoaffective OR “bipolar disorder” Theme 2-Psychosocial Disability, Death, Dying, and Palliative Care (Limit to 2013+) TX(palliative OR death OR dying OR “life limiting” OR “end of life” OR “end stage”) NOT (geriatric OR euthanasia OR COVID-19 OR Alzheimer* OR dementia OR rat OR rats OR infant* OR child* OR adolescent OR youth OR dialysis OR pharmac* OR trauma OR veteran OR military OR “cell death” OR “death anxiety” OR “death tumo*”) AND “severe and persistent mental illness” OR SPMI OR “psychosocial disability” OR schizophrenia OR schizoaffective OR “bipolar disorder” Theme 3-NDIS and Death, Dying, and Palliative Care (Limit to 2013+) “National Disability Insurance” OR ndis OR ndia OR “disabilit* AND personal budget*” OR “user led organi*” OR “individuali* funding package*” NOT “neurodevelopmental impairments” OR “national death information system” OR “naphthalene diimides” OR “neck disability indices” OR “non-drug interventions” AND TX (palliative OR death OR dying OR “life limiting” OR “end of life” OR “end stage”) NOT TX (geriatric OR euthanasia OR COVID-19 OR Alzheimer* OR dementia OR rat OR rats OR infant* OR child* OR adolescent OR youth OR dialysis OR pharmac* OR trauma OR veteran OR military OR “cell death” OR “death anxiety” OR “death tumo*”) Theme 4-NDIS, SPMI and Psychosocial Disability, Death, Dying, and Palliative Care) “National Disability Insurance” OR ndis OR ndia OR “disabilit* AND personal budget*” OR “user led organi*” OR “individuali* funding package*” NOT “neurodevelopmental impairments” OR “national death information system” OR “naphthalene diimides” OR “neck disability indices” OR “non-drug interventions” AND TX (palliative OR death OR dying OR “life limiting” OR “end of life” OR “end stage”) NOT TX (geriatric OR euthanasia OR COVID-19 OR Alzheimer* OR dementia OR rat OR rats OR infant* OR child* OR adolescent OR youth OR dialysis OR pharmac* OR trauma OR veteran OR military OR “cell death” OR “death anxiety” OR “death tumo*”) AND TX “severe and persistent mental illness” OR SPMI OR “psychosocial disability” OR schizophrenia OR schizoaffective OR “bipolar disorder” |
| Themes | Search Terms |
|---|---|
| Theme 1 NDIS and SPMI (“severe AND persistent AND mental AND illness” OR spmi OR “psychosocial AND disability” OR schizophrenia OR schizoaffective OR “bipolar disorder”) AND (“National Disability Insurance” OR ndis OR ndia OR “disabilit* AND personal budget*” OR “user led organi*” OR “individuali* funding package*” AND NOT “neurodevelopmental impairments” AND NOT “national death information system” AND NOT “naphthalene diimides” AND NOT “neck disability indices” AND NOT “non-drug interventions”) Theme 2–Limit to 2013 (“severe AND persistent AND mental AND illness” OR spmi OR “psychosocial AND disability” OR schizophrenia OR schizoaffective OR “bipolar disorder”) AND (TITLE-ABS-KEY ((palliative OR death OR dying OR “life limiting” OR “end of life” OR “end stage”) AND NOT (geriatric OR euthanasia OR COVID-19 OR Alzheimer* OR dementia OR rat OR rats OR infant* OR child* OR adolescent OR youth OR dialysis OR pharmac* OR trauma OR veteran OR military OR “cell death” OR “death anxiety” OR “death tumo*”))) Theme 4–NDIS, Death, Dying, Palliative Care (“National Disability Insurance” OR ndis OR ndia OR “disabilit* AND personal budget*” OR “user led organi*” OR “individuali* funding package*” AND NOT “neurodevelopmental impairments” AND NOT “national death information system” AND NOT “naphthalene diimides” AND NOT “neck disability indices” AND NOT “non-drug interventions”) AND (TITLE-ABS-KEY ((palliative OR death OR dying OR “life limiting” OR “end of life” OR “end stage”) AND NOT (geriatric OR euthanasia OR COVID-19 OR Alzheimer* OR dementia OR rat OR rats OR infant* OR child* OR adolescent OR youth OR dialysis OR pharmac* OR trauma OR veteran OR military OR “cell death” OR “death anxiety” OR “death tumo*”))) Theme 5–SPMI, NDIS, and Palliative Care (“severe AND persistent AND mental AND illness” OR spmi OR “psychosocial AND disability” OR schizophrenia OR schizoaffective OR “bipolar disorder”) AND (TITLE-ABS-KEY ((palliative OR death OR dying OR “life limiting” OR “end of life” OR “end stage”) AND NOT (geriatric OR euthanasia OR COVID-19 OR Alzheimer* OR dementia OR rat OR rats OR infant* OR child* OR adolescent OR youth OR dialysis OR pharmac* OR trauma OR veteran OR military OR “cell death” OR “death anxiety” OR “death tumo*”))) AND (“National Disability Insurance” OR ndis OR ndia OR “disabilit* AND personal budget*” OR “user led organi*” OR “individuali* funding package*” AND NOT “neurodevelopmental impairments” AND NOT “national death information system” AND NOT “naphthalene diimides” AND NOT “neck disability indices” AND NOT “non-drug interventions”) |
Appendix B. Prisma-ScR Checklist
| Section | Item | Prisma-Scr Checklist Item | Reported on Page # |
| Title | |||
| Title | 1 | Identify the report as a scoping review. | 1 |
| Abstract | |||
| Structured summary | 2 | Provide a structured summary that includes (as applicable): background, objectives, eligibility criteria, sources of evidence, charting methods, results, and conclusions that relate to the review questions and objectives. | 1 |
| Introduction | |||
| Rationale | 3 | Describe the rationale for the review in the context of what is already known. Explain why the review questions/objectives lend themselves to a scoping review approach. | 2 & 3 |
| Objectives | 4 | Provide an explicit statement of the questions and objectives being addressed with reference to their key elements (e.g., population or participants, concepts, and context) or other relevant key elements used to conceptualise the review questions and/or objectives. | 2 & 3 |
| Methods | |||
| Protocol and registration | 5 | Indicate whether a review protocol exists; state if and where it can be accessed (e.g., a Web address); and if available, provide registration information, including the registration number. | N/A |
| Eligibility criteria | 6 | Specify characteristics of the sources of evidence used as eligibility criteria (e.g., years considered, language, and publication status), and provide a rationale. | 3 |
| Information sources | 7 | Describe all information sources in the search (e.g., databases with dates of coverage and contact with authors to identify additional sources), as well as the date the most recent search was executed. | 3 |
| Search | 8 | Present the full electronic search strategy for at least 1 database, including any limits used, such that it could be repeated. | 19–21 |
| Selection of sources of evidence | 9 | State the process for selecting sources of evidence (i.e., screening and eligibility) included in the scoping review. | 3–6 |
| Data charting process | 10 | Describe the methods of charting data from the included sources of evidence (e.g., calibrated forms or forms that have been tested by the team before their use, and whether data charting was done independently or in duplicate) and any processes for obtaining and confirming data from investigators. | 7 |
| Data items | 11 | List and define all variables for which data were sought and any assumptions and simplifications made. | 3 |
| Critical appraisal of individual sources of evidence | 12 | If done, provide a rationale for conducting a critical appraisal of included sources of evidence; describe the methods used and how this information was used in any data synthesis (if appropriate). | N/A |
| Synthesis of results | 13 | Describe the methods of handling and summarising the data that were charted. | 7 |
| Results | |||
| Selection of sources of evidence | 14 | Give numbers of sources of evidence screened, assessed for eligibility, and included in the review, with reasons for exclusions at each stage, ideally using a flow diagram. | 4–6 |
| Characteristics of sources of evidence | 15 | For each source of evidence, present characteristics for which data were charted and provide the citations. | 7–18 |
| Critical appraisal within sources of evidence | 16 | If done, present data on critical appraisal of included sources of evidence (see item 12). | N/A |
| Results of individual sources of evidence | 17 | For each included source of evidence, present the relevant data that were charted that relate to the review questions and objectives. | 7–18 |
| Synthesis of results | 18 | Summarise and/or present the charting results as they relate to the review questions and objectives. | 7 |
| Discussion | |||
| Summary of evidence | 19 | Summarise the main results (including an overview of concepts, themes, and types of evidence available), link to the review questions and objectives, and consider the relevance to key groups. | 7 |
| Limitations | 20 | Discuss the limitations of the scoping review process. | 2 |
| Conclusions | 21 | Provide a general interpretation of the results with respect to the review questions and objectives, as well as potential implications and/or next steps. | 17–18 |
| Funding | |||
| Funding | 22 | Describe sources of funding for the included sources of evidence, as well as sources of funding for the scoping review. Describe the role of the funders of the scoping review. | 18 (N/A) |
References
- Tune, D. Review of The National Disability Insurance Scheme Act 2013: Removing Red Tape and Implementing the NDIS Participant Service Guarantee; Department of Social Services: Canberra, Australia, 2019.
- Council of Australian Governments. Principles to Determine the Responsibilities of the NDIS and Other Service Systems; Council of Australian Governments: Canberra, Australia, 2015.
- NDIS Scheme Actuary. NDIS Annual Financial Sustainability Report 2020–2021; National Disability Insurance Agency, Australian Government: Geelong, Australia, 2021; p. 125. [Google Scholar]
- Wark, S.; Hussain, R.; Müller, A.; Ryan, P.; Parmenter, T. Challenges in providing end-of-life care for people with intellectual disability: Health services access. J. Appl. Res. Intellect. Disabil. 2017, 30, 1151–1159. [Google Scholar] [CrossRef] [PubMed]
- Morgan, B.D. “No Right Place to Die”: Nursing Attitudes and Needs in Caring for People With Serious Mental Illness at End-of-Life. J. Am. Psychiatr. Nurses Assoc. 2016, 22, 31–42. [Google Scholar] [CrossRef]
- Kugathasan, P.; Stubbs, B.; Aagaard, J.; Jensen, S.E.; Munk Laursen, T.; Nielsen, R.E. Increased mortality from somatic multimorbidity in patients with schizophrenia: A Danish nationwide cohort study. Acta Psychiatr. Scand. 2019, 140, 340–348. [Google Scholar] [CrossRef] [PubMed]
- Laursen, T.M. Causes of premature mortality in schizophrenia: A review of literature published in 2018. Curr. Opin. Psychiatry 2019, 32, 388–393. [Google Scholar] [CrossRef] [PubMed]
- Laursen, T.M.; Musliner, K.L.; Benros, M.E.; Vestergaard, M.; Munk-Olsen, T. Mortality and life expectancy in persons with severe unipolar depression. J. Affect. Disord. 2016, 193, 203–207. [Google Scholar] [CrossRef]
- Laursen, T.M.; Wahlbeck, K.; Hällgren, J.; Westman, J.; Ösby, U.; Alinaghizadeh, H.; Gissler, M.; Nordentoft, M. Life Expectancy and Death by Diseases of the Circulatory System in Patients with Bipolar Disorder or Schizophrenia in the Nordic Countries. PLoS ONE 2013, 8, e67133. [Google Scholar] [CrossRef]
- Meier, S.M.; Mattheisen, M.; Mors, O.; Mortensen, P.B.; Laursen, T.M.; Penninx, B.W. Increased mortality among people with anxiety disorders: Total population study. Br. J. Psychiatry 2016, 209, 216–221. [Google Scholar] [CrossRef]
- Momen, N.C.; Plana-Ripoll, O.; Agerbo, E.; Benros, M.E.; Børglum, A.D.; Christensen, M.K.; Dalsgaard, S.; Degenhardt, L.; de Jonge, P.; Debost, J.-C.P.; et al. Association between Mental Disorders and Subsequent Medical Conditions. N. Engl. J. Med. 2020, 382, 1721–1731. [Google Scholar] [CrossRef]
- Plana-Ripoll, O.; Weye, N.; Momen, N.; Christensen, M.; Iburg, K.; Laursen, T.M.; McGrath, J. Changes in differential mortality gap in those with mental disorders between 1995 and 2015 in Denmark. Aâ nationwide, register-based cohort study based on 7.4 million individual…Schizophrenia International Research Society (SIRS) 2020 Congress. Schizophr. Bull. 2020, 46, S17–S18. [Google Scholar] [CrossRef]
- Toender, A.; Munk-Olsen, T.; Vestergaard, M.; Larsen, J.; Suppli, N.; Dalton, S.; Vedsted, P.; Nordentoft, M.; Mortensen, P.; Laursen, T. impact of severe mental illness on cancer stage at diagnosis and subsequent mortality: A population-based register study. Schizophr. Res. 2018, 201, 62–69. [Google Scholar] [CrossRef]
- Stajduhar, K.I.; Mollison, A.; Giesbrecht, M.; McNeil, R.; Pauly, B.; Reimer-Kirkham, S.; Dosani, N.; Wallace, B.; Showler, G.; Meagher, C.; et al. “Just too busy living in the moment and surviving”: Barriers to accessing health care for structurally vulnerable populations at end-of-life. BMC Palliative Care 2019, 18, 11. [Google Scholar] [CrossRef] [PubMed]
- Donald, E.E.; Stajduhar, K.I. A scoping review of palliative care for persons with severe persistent mental illness. Palliat. Supportive Care 2019, 17, 479–487. [Google Scholar] [CrossRef] [PubMed]
- Shalev, D.; Brewster, K.; Arbuckle, M.R.; Levenson, J.A. A staggered edge: End-of-life care in patients with severe mental illness. Gen. Hosp. Psychiatry 2017, 44, 1–3. [Google Scholar] [CrossRef]
- Butler, H.; O’Brien, A.J. Access to specialist palliative care services by people with severe and persistent mental illness: A retrospective cohort study. Int. J. Ment. Health Nurs. 2018, 27, 737–746. [Google Scholar] [CrossRef] [PubMed]
- Jerwood, J.S.; Phimister, D.; Ward, G.; Holliday, N.; Coad, J. Barriers to palliative care for people with severe mental illness: Exploring the views of clinical staff. Eur. J. Palliat. Care 2018, 25, 20–25. [Google Scholar]
- Picot, S.A.; Glaetzer, K.M.; Myhill, K.J. Coordinating end of life care for individuals with a mental illness—A nurse practitioner collaboration. Coll. J. R. Coll. Nurs. Aust. 2015, 22, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.; Hepgul, N.; Higginson, I.J.; Gao, W. End-of-life care and place of death in adults with serious mental illness: A systematic review and narrative synthesis. Palliat. Med. 2020, 34, 49–68. [Google Scholar] [CrossRef]
- Brown, R.; Chambers, S.; Rosenberg, J. Exploring palliative care nursing of patients with pre-existing serious persistent mental illness. Prog. Palliat. Care 2019, 27, 117–121. [Google Scholar] [CrossRef]
- Jerwood, J.; Ward, G.; Phimister, D.; Holliday, N.; Coad, J. Lean in, don’t step back: The views and experiences of patients and carers with severe mental illness and incurable physical conditions on palliative and end of life care. Prog. Palliat. Care 2021, 29, 255–263. [Google Scholar] [CrossRef]
- Viprey, M.; Pauly, V.; Salas, S.; Baumstarck, K.; Orleans, V.; Llorca, P.-M.; Lancon, C.; Auquier, P.; Boyer, L.; Fond, G. Palliative and high-intensity end-of-life care in schizophrenia patients with lung cancer: Results from a French national population-based study. Eur. Arch. Psychiatry Clin. Neurosci. 2020, 271, 1571–1578. [Google Scholar] [CrossRef]
- Bloomer, M.J.; O’Brien, A.P. Palliative care for the person with a serious mental illness: The need for a partnership approach to care in Australia. Prog. Palliat. Care 2013, 21, 27–31. [Google Scholar] [CrossRef]
- Baruth, J.M.; Ho, J.B.; Mohammad, S.I.; Lapid, M.I. End-of-life care in schizophrenia: A systematic review. Int. Psychogeriatr. 2020, 33, 129–147. [Google Scholar] [CrossRef] [PubMed]
- Irwin, K.E.; Henderson, D.C.; Knight, H.P.; Pirl, W.F. Cancer care for individuals with schizophrenia. Cancer 2014, 120, 323–334. [Google Scholar] [CrossRef]
- Edwards, D.; Anstey, S.; Coffey, M.; Gill, P.; Mann, M.; Meudell, A.; Hannigan, B. End of life care for people with severe mental illness: Mixed methods systematic review and thematic synthesis (the MENLOC study). Palliat. Med. 2021, 35, 1747–1760. [Google Scholar] [CrossRef] [PubMed]
- Hinrichs, K.L.M.; Woolverton, C.B.; Meyerson, J.L. Help Me Understand: Providing Palliative Care to Individuals with Serious Mental Illness. Am. J. Hosp. Palliat. Med. 2022, 39, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Rentmeester, C. Regarding refusals of physically Ill people with mental illnesses at the end-of-life. Int. J. Ment. Health 2014, 43, 73–80. [Google Scholar] [CrossRef]
- National Disability Insurance Agency. Data and Insights Geelong: National Disability Insurance Agency. 2022 [updated 10 June 2022. NDIS Participant Data]. Available online: https://data.ndis.gov.au/explore-data (accessed on 12 July 2022).
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Peters, M.D.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Evid. Synth. 2020, 18, 2119–2126. [Google Scholar] [CrossRef]
- Pollock, D.; Davies, E.L.; Peters, M.D.J.; Tricco, A.C.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H.; Munn, Z. Undertaking a scoping review: A practical guide for nursing and midwifery students, clinicians, researchers, and academics. J. Adv. Nurs. 2021, 77, 2102–2113. [Google Scholar] [CrossRef]
- Smith-Merry, J.; Hancock, N.; Gilroy, J.; Llewellyn, G.; Yen, I. Mind the Gap: The National Disability Insurance Scheme and psychosocial disability. In Final Report: Stakeholder Identified Gaps and Solutions; University of Sydney: Camperdown, Australia, 2018. [Google Scholar]
- Federal Register of Legislation. National Disability Insurance Scheme Act 2013 (Cth); Federal Register of Legislation: Canberra, Australia, 2013.
- Sweers, K.; de Casterle, B.D.; Detraux, J.; De Hert, M. End-of-life (care) perspectives and expectations of patients with schizophrenia. Arch. Psychiatr. Nurs. 2013, 27, 246–252. [Google Scholar] [CrossRef]
- Hamilton, D.; Hancock, N.; Scanlan, J.N.; Banfield, M. The National Disability Insurance Scheme and people with severe and persistent mental illness/psychosocial disability: A review, analysis and synthesis of published literature. Aust. N. Zeal. J. Psychiatry 2020, 54, 1162–1172. [Google Scholar] [CrossRef] [PubMed]
- Den Boer, K.; De Veer, A.J.E.; Schoonmade, L.J.; Verhaegh, K.J.; Van Meijel, B.; Francke, A.L. A systematic review of palliative care tools and interventions for people with severe mental illness. BMC Psychiatry 2019, 19, 106. [Google Scholar] [CrossRef] [PubMed]
- Grassi, L.; Riba, M. Cancer and severe mental illness: Bi-directional problems and potential solutions. Psycho-Oncology 2020, 29, 1445–1451. [Google Scholar] [CrossRef] [PubMed]
- Woods, A.; Willison, K.; Kington, C.; Gavin, A. Palliative care for people with severe persistent mental illness: A review of the literature. Can. J. Psychiatry—Rev. Can. Psychiatry 2008, 53, 725–736. [Google Scholar] [CrossRef]
- Zumstein, N.; Riese, F. Defining Severe and Persistent Mental Illness—A Pragmatic Utility Concept Analysis. Front. Psychiatry 2020, 11, 648. [Google Scholar] [CrossRef] [PubMed]
- González-Rodríguez, A.; Labad, J.; Seeman, M.V. Schizophrenia and cancer. Curr. Opin. Supportive Palliat. Care 2020, 14, 232–238. [Google Scholar] [CrossRef]
- Jørgensen, M.; Mainz, J.; Lange, P.; Johnsen, S.P. Quality of care and clinical outcomes of chronic obstructive pulmonary disease in patients with schizophrenia. A Dan. Nationwide Study. Int. J. Qual. Health Care 2018, 30, 351–357. [Google Scholar] [CrossRef]
- Lawn, S.; Zabeen, S.; Rowlands, N.; Picot, S. Hidden care: Revelations of a case-note audit of physical health care in a community mental health service. Int. J. Ment. Health Nurs. 2018, 27, 1742–1755. [Google Scholar] [CrossRef]
- Spilsbury, K.; Rosenwax, L.; Brameld, K.; Kelly, B.; Arendts, G. Morbidity burden and community-based palliative care are associated with rates of hospital use by people with schizophrenia in the last year of life: A population-based matched cohort study. PLoS ONE 2018, 13, e0208220. [Google Scholar] [CrossRef]
- Gondek, T.M.; Krolicka, A.; Piotrowski, P.; Kiejna, A. The European studies on mortality in schizophrenia. Psychiatr. Pol. 2015, 49, 1139–1148. [Google Scholar] [CrossRef]
- Huang, H.K.; Wang, Y.W.; Hsieh, J.G.; Hsieh, C.J. Disparity of end-of-life care in cancer patients with and without schizophrenia: A nationwide population-based cohort study. Schizophr. Res. 2018, 195, 434–440. [Google Scholar] [CrossRef] [PubMed]
- McKillip, K.M.; Lott, A.D.; Swetz, K.M. Respecting autonomy and promoting the patient’s good in the setting of serious terminal and concurrent mental illness. Yale J. Biol. Med. 2019, 92, 597–602. [Google Scholar] [PubMed]
- McNamara, B.; Same, A.; Rosenwax, L.; Kelly, B. Palliative care for people with schizophrenia: A qualitative study of an under-serviced group in need. BMC Palliat. Care 2018, 17, 53. [Google Scholar] [CrossRef] [PubMed]
- Cortis, N.; Van Toorn, G. Safeguarding in Australia’s new disability markets: Frontline workers’ perspectives. Crit. Soc. Policy 2021, 42, 197–219. [Google Scholar] [CrossRef]
- De Veer, A.J.E.; Stringer, B.; Van Meijel, B.; Verkaik, R.; Francke, A.L. Access to palliative care for homeless people: Complex lives, complex care. BMC Palliat. Care 2018, 17, 119. [Google Scholar] [CrossRef] [PubMed]
- Carey, G.; Malbon, E.; Blackwell, J. Administering inequality? The National Disability Insurance Scheme and administrative burdens on individuals. Aust. J. Public Adm. 2021, 80, 854–872. [Google Scholar]
- Shalev, D.; Fields, L.; Shapiro, P.A. End-of-Life Care in Individuals with Serious Mental Illness. Psychosomatics 2020, 61, 428–435. [Google Scholar] [CrossRef]
- Gillieatt, S.; Martin, R.; Dorozenko, K.P.; Munro, A. Evaluation of a West Australian residential mental health respite service. Health Soc. Care Community 2018, 26, e442–e450. [Google Scholar] [CrossRef]
- Mazanec, P.; Verga, S.; Foley, H.; Mehta, A.K. The Need for Cultural Inclusivity in Global Palliative Nursing: Caring for Selected Underserved Populations in the United States. J. Hosp. Palliat. Nurs. 2019, 21, E1–E8. [Google Scholar] [CrossRef]
- Shalev, D.; Brewster, K.K.; Levenson, J.A. End-of-life care for patients with schizophrenia #332. J. Palliat. Med. 2017, 20, 787–788. [Google Scholar]
- Lawrence, D.; Kisely, S. Inequalities in healthcare provision for people with severe mental illness. J. Psychopharmacol. 2010, 24, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Terpstra, T.L.; Williamson, S. Palliative care for terminally ill individuals with borderline personality disorder. J. Psychosoc. Nurs. Ment. Health Serv. 2019, 57, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Dawson, S.; Muir-Cochrane, E.; Simpson, A.; Lawn, S. Community treatment orders and care planning: How is engagement and decision-making enacted? Health Expect. Int. J. Public Particip. Health Care Health Policy 2021, 24, 1859–1867. [Google Scholar] [CrossRef] [PubMed]
- Carney, T.; Then, S.-N.; Bigby, C.; Wiesel, I.; Douglas, J. National Disability Insurance Scheme plan decision-making: Or when tailor-made case planning met Taylorism & the algorithms? Melb. Univ. Law Rev. 2019, 42, 780. [Google Scholar]
- Carney, T. Supported Decision-Making for People with Cognitive Impairments: An Australian Perspective? Laws 2015, 4, 37–59. [Google Scholar] [CrossRef]
- Swanson, J.W.; Swartz, M.S.; Elbogen, E.B.; Van Dorn, R.A.; Ferron, J.; Wagner, H.R.; McCauley, B.J.; Mimi Kim, M.A. Facilitated psychiatric advance directives: A randomised trial of an intervention to foster advance treatment planning among persons with severe mental illness. Am. J. Psychiatry 2006, 163, 1943–1951. [Google Scholar] [CrossRef]
- Trachsel, M. The Ethical Importance of Assessing End-of-Life Care Preferences in Patients with Severe and Persistent Mental Illness. Am. J. Geriatr. Psychiatry 2018, 26, 98–99. [Google Scholar] [CrossRef]
- Australian Government. NDIS Practice Standards and Quality Indicators; NDIS Quality and Safeguards Commission, Ed.; Commonwealth Government of Australia: Canberra, Australia, 2018; pp. 1–45.
- Tylec, A.; Dubas-Slemp, H.; Wojcicka, A.; Drop, B.; Kucharska, K. The difficulties of secondary prophylaxis of cervical cancer in women suffering from paranoid schizophrenia—A case study. Psychiatr. Pol. 2018, 52, 251–259. [Google Scholar] [CrossRef]
- Fond, G.; Baumstarck, K.; Auquier, P.; Pauly, V.; Bernard, C.; Orleans, V.; Llorca, P.-M.; Lancon, C.; Salas, S.; Boyer, L. End-of-Life Care Among Patients with Bipolar Disorder and Cancer: A Nationwide Cohort Study. Psychosom. Med. 2020, 82, 722–732. [Google Scholar] [CrossRef]
- Fond, G.; Pauly, V.; Duba, A.; Salas, S.; Viprey, M.; Baumstarck, K.; Orleans, V.; Llorca, P.-M.; Lancon, C.; Auquier, P.; et al. End of life breast cancer care in women with severe mental illnesses. Sci. Rep. 2021, 11, 10167. [Google Scholar] [CrossRef]
- Hanan, D.M.; Lyons, K.S. Hospice Use Among Individuals with Severe Persistent Mental Illness. J. Am. Psychiatr. Nurses Assoc. 2021, 27, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.; Gaughran, F.; Whitburn, T.; Higginson, I.J.; Gao, W. Acute care utilisation towards the end of life and the place of death for patients with serious mental disorders: A register-based cohort study in South London. Public Health 2021, 194, 79–85. [Google Scholar] [CrossRef] [PubMed]
- UN General Assembly, Convention on the Rights of Persons with Disabilities, 13 December 2006, A/RES/61/106, Annex I. Available online: https://www.refworld.org/docid/4680cd212.html (accessed on 24 July 2022).
- David, C.; West, R. NDIS Self-Management Approaches: Opportunities for choice and control or an Uber-style wild west? Aust. J. Soc. Issues 2017, 52, 331–346. [Google Scholar] [CrossRef]
- Edmunds, M. Inequitable physical illness and premature mortality for people with severe mental illness in Australia: A social analysis. Health Hum. Rights 2018, 20, 273–281. [Google Scholar] [PubMed]
- Terpstra, T.L.; Williamson, S.; Terpstra, T. Palliative care for terminally ill individuals with schizophrenia. J. Psychosoc. Nurs. Ment. Health Serv. 2014, 52, 32–38. [Google Scholar] [CrossRef]
- Hurley, J.H.M. Carers’ experiences of the National Disability Insurance Scheme workforce: A qualitative study informing workforce development. Aust. J. Soc. Issues 2021, 57, 458–471. [Google Scholar] [CrossRef]
- World Health Organisation. Palliative Care. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/palliative-care (accessed on 1 November 2021).
- Duckett, S. Aligning policy objectives and payment design in palliative care. BMC Palliat. Care 2018, 17, 42. [Google Scholar] [CrossRef]
- Park, T.; Hegadoren, K.; Workun, B. Working at the Intersection of Palliative End-of-Life and Mental Health Care: Provider Perspectives. J. Palliat. Care 2020, 37, 183–189. [Google Scholar] [CrossRef]
- Australian Government. The National Palliative Care Strategy; Department of Health: Canberra, Australia, 2018.
- Carpiniello, B.; Wasserman, D. European Psychiatric Association policy paper on ethical aspects in communication with patients and their families. Eur. Psychiatry 2020, 63, e36. [Google Scholar] [CrossRef]
- Foti, M.E.; Bartels, S.J.; Van Citters, A.D.; Merriman, M.P.; Fletcher, K.E. End-of-Life Treatment Preferences of Persons with Serious Mental Illness. Psychiatr. Serv. 2005, 56, 585–591. [Google Scholar] [CrossRef]
- Souza, F.; Duff, G.; Swait, J. “Whose plan is it?” Understanding how the goal pursuit of Consumers and Carers influence choices in the Australian Disability Sector. J. Choice Model. 2021, 40, 100300. [Google Scholar]
- Wilson, E.; Campain, R.; Pollock, S.; Brophy, L.; Stratford, A. Exploring the personal, programmatic and market barriers to choice in the NDIS for people with psychosocial disability. Aust. J. Soc. Issues 2021, 57, 164–184. [Google Scholar] [CrossRef]
- Joint Standing Committee on the National Disability Insurance Scheme. NDIS Planning Final Report; Parliament of Australia: Canberra, Australia, 2020; pp. 65–67.
- Ganzini, L.; Socherman, R.; Duckart, J.; Shores, M. End-of-life care for veterans with schizophrenia and cancer. Psychiatr. Serv. 2010, 61, 725–728. [Google Scholar] [CrossRef] [PubMed]
- Baker, A. Palliative and End-of-Life Care in the Serious and Persistently Mentally Ill Population. J. Am. Psychiatr. Nurses Assoc. 2005, 11, 298–303. [Google Scholar] [CrossRef]
- Knippenberg, I.; Zaghouli, N.; Engels, Y.; Vissers, K.C.P.; Groot, M.M. Severe mental illness and palliative care: Patient semistructured interviews. BMJ Supportive Palliat. Care 2020. [Google Scholar] [CrossRef]
- Harman, S.M.M.D. Psychiatric and Palliative Care in the Intensive Care Unit. Crit. Care Clin. 2017, 33, 735–743. [Google Scholar] [CrossRef]
- Graneheim, U.H.; Åström, S. Until Death Do Us Part: Adult Relatives’ Experiences of Everyday Life Close to Persons with Mental Ill-Health. Issues Ment. Health Nurs. 2016, 37, 602–608. [Google Scholar] [CrossRef]
- Happell, B.; Wilson, K.; Platania-Phung, C.; Stanton, R. Filling the gaps and finding our way: Family carers navigating the healthcare system to access physical health services for the people they care for. J. Clin. Nurs. 2017, 26, 1917–1926. [Google Scholar] [CrossRef]
- Diminic, S.; Lee, Y.Y.; Hielscher, E.; Harris, M.G.; Kealton, J.; Whiteford, H.A. Quantifying the size of the informal care sector for Australian adults with mental illness: Caring hours and replacement cost. Soc. Psychiatry Psychiatr. Epidemiol. 2021, 56, 387–400. [Google Scholar] [CrossRef]
- National Disability Insurance Agency. NDIS Pricing Arrangements and Price Limits; National Disability Insurance Agency: Geelong, Australia, 2021; pp. 1–110. [Google Scholar]
- Hussain, R.; Parmenter, T.; Wark, S.; Janicki, M.; Knox, M.; Hayhoe, N. Mitigating the impact of the ‘silos’ between the disability and aged-care sectors in Australia: Development of a Best Practice Framework. J. Appl. Res. Intellect. Disabil. 2021, 34, 1477–1488. [Google Scholar] [CrossRef]
- Waters, R.A.; Buchanan, A. An exploration of person-centred concepts in human services: A thematic analysis of the literature. Health Policy 2017, 121, 1031–1039. [Google Scholar] [CrossRef] [PubMed]
- Hummell, E.; Venning, A.; Foster, M.; Fisher, K.R.; Kuipers, P. A rapid review of barriers and enablers of organisational collaboration: Identifying challenges in disability reform in Australia. Aust. J. Soc. Issues 2022, 57, 441–457. [Google Scholar] [CrossRef]
- Foster, M.; Hummell, E.; Fisher, K.; Borg, S.J.; Needham, C.; Venning, A. Organisations adapting to dual aspirations of individualisation and collaboration in the National Disability Insurance Scheme (NDIS) market. Aust. J. Public Adm. 2022, 81, 127–144. [Google Scholar] [CrossRef]
- Isaacs, A.N.; Firdous, F. A care coordination model can facilitate interagency collaboration when designing recovery-oriented services. J. Psychosoc. Nurs. Ment. Health Serv. 2019, 57, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Isaacs, A.N.; Dalziel, K.; Sutton, K.; Maybery, D. Referral patterns and implementation costs of the partners in recovery initiative in Gippsland: Learnings for the National Disability Insurance Scheme. Australas. Psychiatry 2018, 26, 586–589. [Google Scholar] [CrossRef] [PubMed]
- Lewis, S.B.; Florio, T.; Srasuebkul, P.; Trollor, J.N. Impact of disability services on mental health service utilisation in adults with intellectual disability. J. Appl. Res. Intellect. Disabil. 2020, 33, 1357–1367. [Google Scholar] [CrossRef] [PubMed]
- Bloomer, M. The challenges of end of life care in acute hospitals. Coll. J. R. Coll. Nurs. Aust. 2015, 22, 241–242. [Google Scholar] [CrossRef]
- Isaacs, A.N.; Sutton, K.; Beauchamp, A. Recovery oriented services for persons with severe mental illness can focus on meeting needs through care coordination. J. Ment. Health Policy Econ. 2020, 23, 55–60. [Google Scholar]
- Hancock, N.; Smith-Merry, J.; Gillespie, J.A.; Yen, I. Is the Partners in Recovery program connecting with the intended population of people living with severe and persistent mental illness? What are their prioritised needs? Aust. Health Rev. 2017, 41, 566–572. [Google Scholar] [CrossRef]
- Lukersmith, S.; Taylor, J.; Salvador-Carulla, L. Vagueness and ambiguity in communication of case management: A content analysis in the Australian national disability insurance scheme. Int. J. Integr. Care 2021, 21, 17. [Google Scholar] [CrossRef]
- Faulkner, A. Survivor research and Mad Studies: The role and value of experiential knowledge in mental health research. Disabil. Soc. 2017, 32, 500–520. [Google Scholar] [CrossRef]
- Isaacs, A.N.; Beauchamp, A.; Sutton, K.; Maybery, D. Unmet needs of persons with a severe and persistent mental illness and their relationship to unmet accommodation needs. Health Soc. Care Community 2019, 27, e246–e256. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, S.; Redmond, C.; Boyer, P.; Gleeson, P.; Russell, P. Culture clash? Recovery in mental health under Australia’s National Disability Insurance Scheme—A case study. Public Health Res. Pract. 2019, 29, 29011902. [Google Scholar] [PubMed]
- Wiesel, I.; Whitzman, C.; Gleeson, B.; Bigby, C. The National Disability Insurance Scheme in an Urban Context: Opportunities and Challenges for Australian Cities. Urban Policy Res. 2019, 37, 1–12. [Google Scholar] [CrossRef]
- Nagington, M.; Walshe, C.; Luker, K.A. A poststructural rethinking of the ethics of technology in relation to the provision of palliative home care by district nurses. Nurs. Philos. 2016, 17, 59–70. [Google Scholar] [CrossRef] [PubMed]
- Kotzé, C.; Roos, J.L.; Ehlers, R. End-of-Life Decision-Making Capacity in Older People with Serious Mental Illness. Front. Psychiatry 2021, 12, 752897. [Google Scholar] [CrossRef]
- Gamaluddin, S.A.; Keating, S.S.; McKenzie, R.R.; Kim, K.Y. Palliative care for persons with severe mental illness. Palliat. Care Perspect. Pract. Impact Qual. Life Glob. View 2017, 1, 3–22. [Google Scholar]
- Ganzini, L.; Gross, A.F. Cancer care for patients with schizophrenia. In Psycho-Oncology, 3rd ed.; Oxford University Press: Oxford, UK, 2015; pp. 345–355. [Google Scholar]
- Taylor, J.; Swetenham, K.; Myhill, K.; Picot, S.; Glaetzer, K.; Loon, A. IMhPaCT: An education strategy for cross-training palliative care and mental health clinicians. Int. J. Palliat. Nurs. 2012, 18, 290–294. [Google Scholar] [CrossRef]
- Evenblij, K.; Widdershoven, G.A.M.; Onwuteaka-Philipsen, B.D.; de Kam, H.; Pasman, H.R.W. Palliative care in mental health facilities from the perspective of nurses: A mixed-methods study. J. Psychiatr. Ment. Health Nurs. 2016, 23, 409–418. [Google Scholar] [CrossRef]
- Carey, G.; Dickinson, H. A longitudinal study of the implementation experiences of the Australian National Disability Insurance Scheme: Investigating transformative policy change. BMC Health Serv. Res. 2017, 17, 570. [Google Scholar] [CrossRef]
- Fleming, P.; McGilloway, S.; Hernon, M.; Furlong, M.; O’Doherty, S.; Keogh, F.; Stainton, T. Individualised funding interventions to improve health and social care outcomes for people with a disability: A mixed-methods systematic review. Campbell Syst. Rev. 2019, 15. [Google Scholar] [CrossRef]
- Cortis, N.; Van Toorn, G. Commentary on “Regulating disability services: The case of Australia’s National Disability Insurance Scheme quality and safeguarding system” (Hough, 2021). Res. Pract. Intellect. Dev. Disabil. 2021, 8, 119–125. [Google Scholar] [CrossRef]
- Mills, J.; Rosenberg, J.P.; McInerney, F. Building community capacity for end of life: An investigation of community capacity and its implications for health-promoting palliative care in the Australian Capital Territory. Crit. Public Health 2015, 25, 218–230. [Google Scholar] [CrossRef]
- David, R.; Elizabeth, M. Risk and Opportunity—The Leadership Challenge in a World of Uncertainty—Learnings from Research into the Implementation of the Australian National Disability Insurance Scheme. J. Risk Financ. Manag. 2021, 14, 383. [Google Scholar]
- Judd, M.J.; Dorozenko, K.P.; Breen, L.J. Workplace stress, burnout and coping: A qualitative study of the experiences of Australian disability support workers. Health Soc. Care Community 2017, 25, 1109–1117. [Google Scholar] [CrossRef]
- Dickinson, H.; Carey, G. Managing care integration during the implementation of large-scale reforms. J. Integr. Care 2017, 25, 6–16. [Google Scholar] [CrossRef]
- National Disability Insurance Agency. List A—Conditions Which Are Likely to Meet the Disability Requirements in Section 24 of the NDIS Act Geelong. 2019. Available online: https://www.ndis.gov.au/about-us/operational-guidelines/access-ndis-operational-guideline/list-conditions-which-are-likely-meet-disability-requirements-section-24-ndis-act (accessed on 3 December 2021).
- Australian Government. Australia’s Disability Strategy 2021–2031; Department of Social Services, Commonwealth of Australia: Canberra, Australia, 2021.
- Westermair, A.L.; Schreiber, W.; Dümchen, J.; Perrar, K.M. Psychiatrists in palliative care of people with severe psychiatric illnesses and an oncological comorbidity. Nervenarzt 2020, 91, 404–410. [Google Scholar] [CrossRef]
- Chochinov, H.M.; Martens, P.J.; Prior, H.J.; Kredentser, M.S. Comparative health care use patterns of people with schizophrenia near the end of life: A population-based study in Manitoba, Canada. Schizophr. Res. 2012, 141, 241–246. [Google Scholar] [CrossRef]
- Elie, D.; Marino, A.; Torres-Platas, S.G.; Noohi, S.; Semeniuk, T.; Segal, M.; Looper, K.J.; Rej, S. End-of-Life Care Preferences in Patients with Severe and Persistent Mental Illness and Chronic Medical Conditions: A Comparative Cross-Sectional Study. Am. J. Geriatr. Psychiatry 2018, 26, 89–97. [Google Scholar] [CrossRef]
- Griffith, L.J. Good palliative care for a patient with schizophrenia dying of emphysema and heart failure. Psychiatry 2007, 4, 61–65. [Google Scholar]
- Brown, M.; Drummond, C. Advance care directives are an important part of good healthcare. Intern. Med. J. 2017, 47, 975–976. [Google Scholar] [CrossRef] [PubMed]
- National Disability Insurance Agency. Intergovernmental Agreements: Australian Government. 2021. (Updated 1 September 2021). Available online: https://www.ndis.gov.au/about-us/governance/intergovernmental-agreements (accessed on 2 January 2022).
- Productivity Commission. Disability Care and Support Productivity Commission Inquiry Report; Australian Government: Canberra, Australia, 2011.
- Stewart, V.; Slattery, M.; Roennfeldt, H.; Wheeler, A.J. Partners in Recovery: Paving the way for the National Disability Insurance Scheme. Aust. J. Prim. Health 2018, 24, 208–215. [Google Scholar] [CrossRef] [PubMed]
- Visser, K.; Stewart, V.; Slattery, M. Supporting choice, recovery, and participation: Clear and easy to understand information is the key to ndis access for those with psychosocial disability. J. Soc. Incl. 2020, 11, 33–46. [Google Scholar]
- Rutherford, J.; Willmott, L.; White, B.P. Physician attitudes to voluntary assisted dying: A scoping review. BMJ Supportive Palliat. Care 2020, 20, 20. [Google Scholar] [CrossRef]
- Daya, I.; Hamilton, B.; Roper, C. Authentic engagement: A conceptual model for welcoming diverse and challenging consumer and survivor views in mental health research, policy, and practice. Int. J. Ment. Health Nurs. 2020, 29, 299–311. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boschen, K.; Phelan, C.; Lawn, S. NDIS Participants with Psychosocial Disabilities and Life-Limiting Diagnoses: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 10144. https://doi.org/10.3390/ijerph191610144
Boschen K, Phelan C, Lawn S. NDIS Participants with Psychosocial Disabilities and Life-Limiting Diagnoses: A Scoping Review. International Journal of Environmental Research and Public Health. 2022; 19(16):10144. https://doi.org/10.3390/ijerph191610144
Chicago/Turabian StyleBoschen, Kathy, Caroline Phelan, and Sharon Lawn. 2022. "NDIS Participants with Psychosocial Disabilities and Life-Limiting Diagnoses: A Scoping Review" International Journal of Environmental Research and Public Health 19, no. 16: 10144. https://doi.org/10.3390/ijerph191610144
APA StyleBoschen, K., Phelan, C., & Lawn, S. (2022). NDIS Participants with Psychosocial Disabilities and Life-Limiting Diagnoses: A Scoping Review. International Journal of Environmental Research and Public Health, 19(16), 10144. https://doi.org/10.3390/ijerph191610144