
Study of the Reliability of Field Test Methods for Physical Fitness in Children Aged 2–3 Years

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Subjects
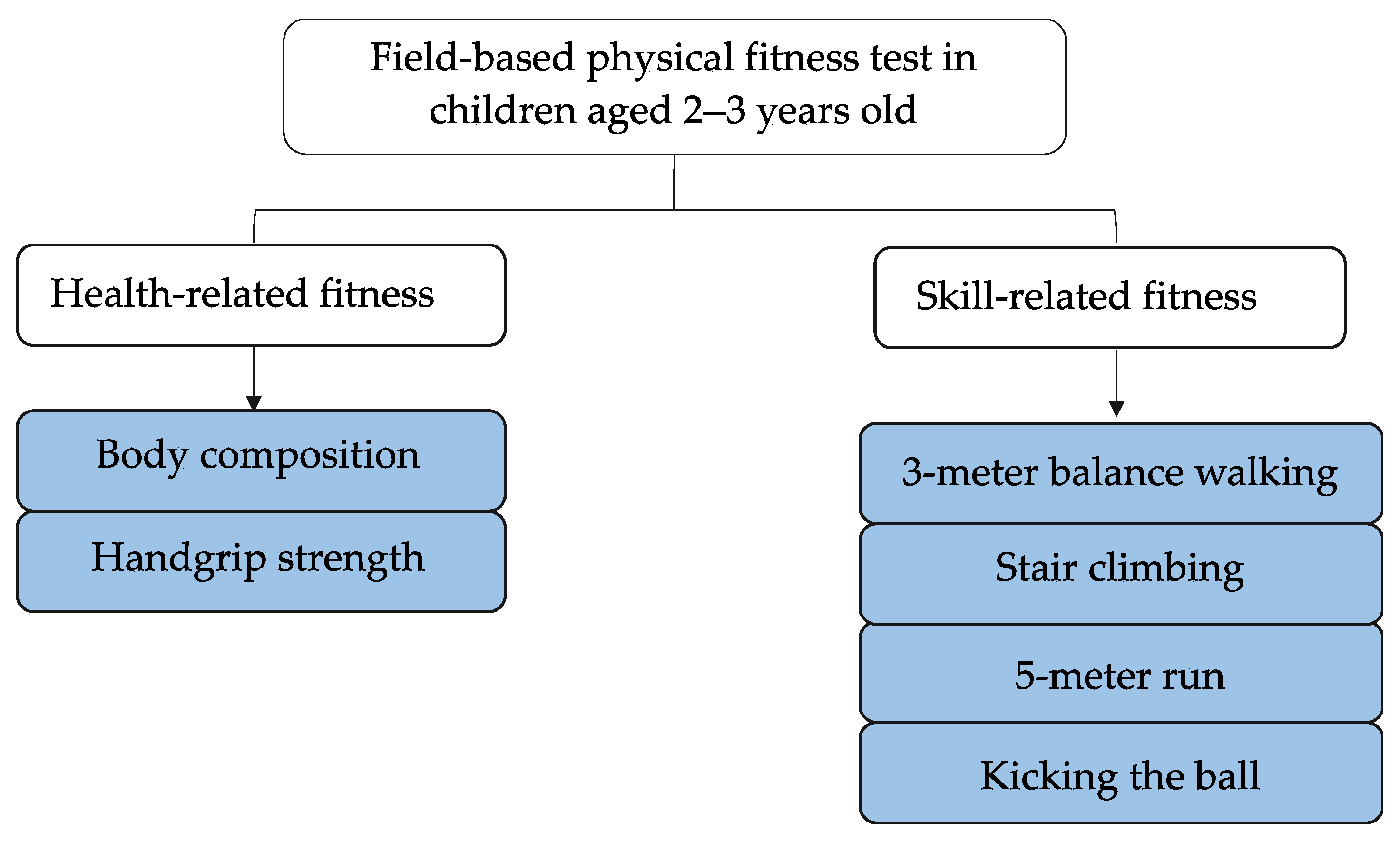
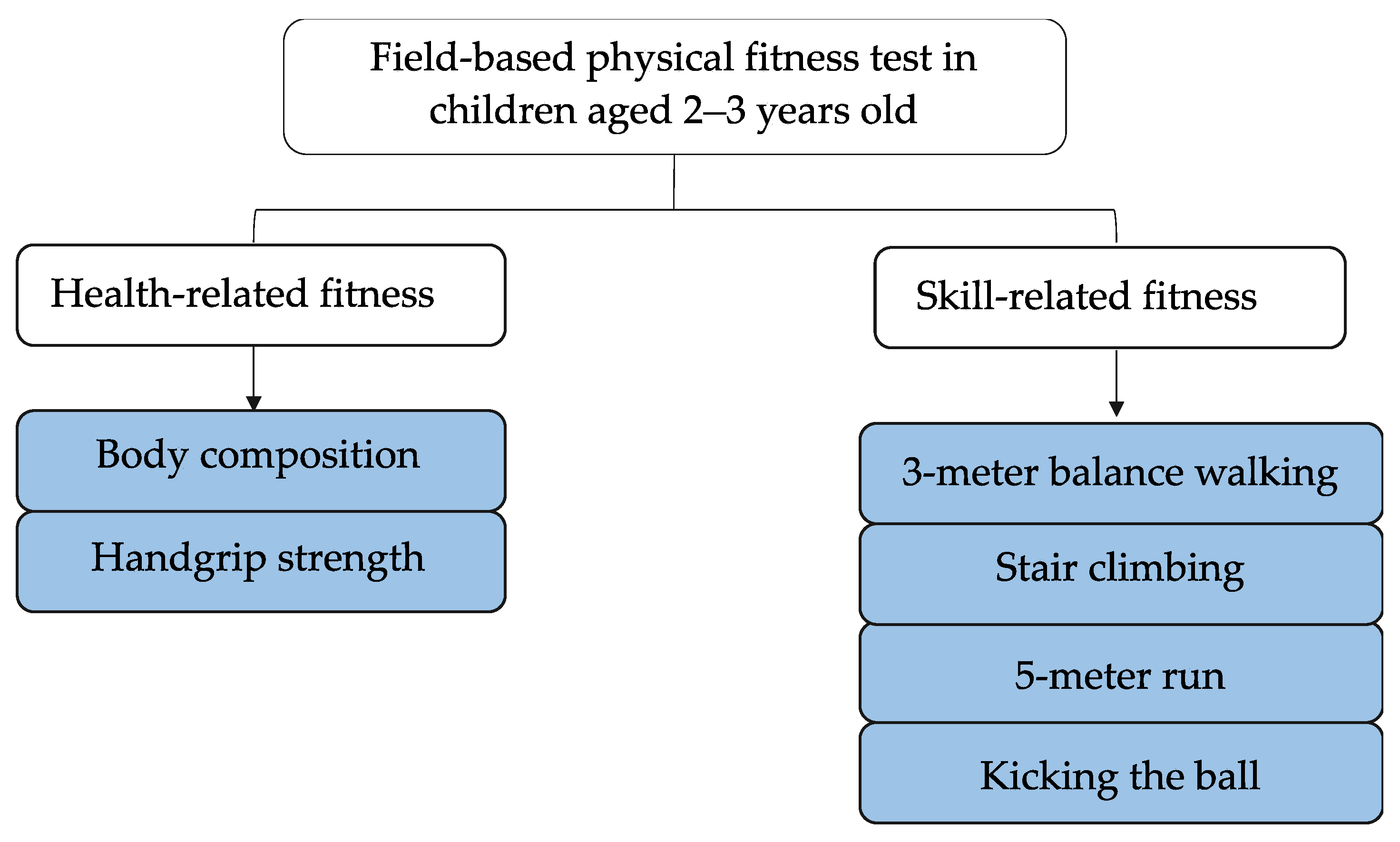
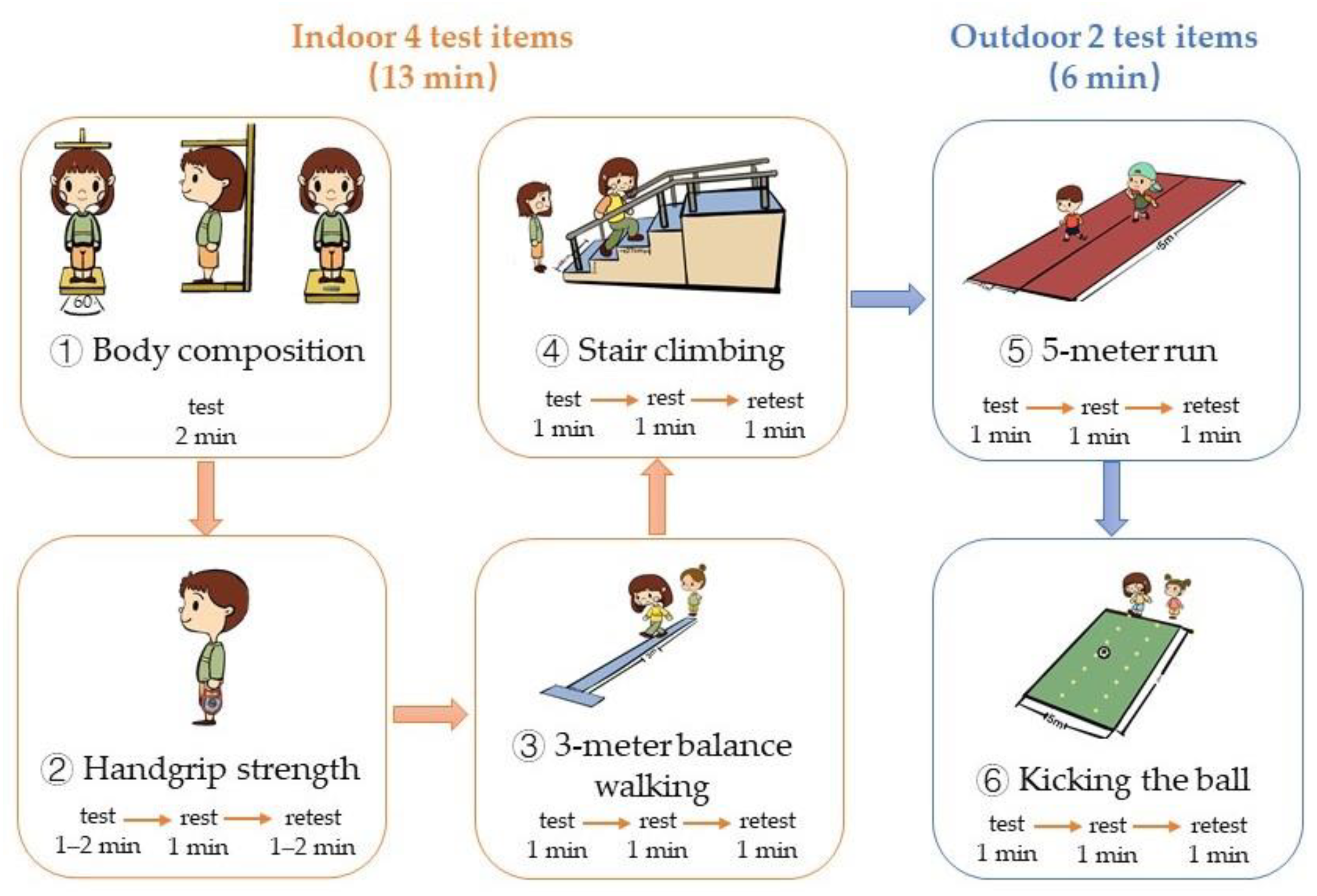
2.2. Materials and Tests
2.2.1. Body Composition
2.2.2. Handgrip Strength
2.2.3. 3-m Balance Walking
2.2.4. Stair Climbing
2.2.5. 5-Meter Run
2.2.6. Kicking the Ball
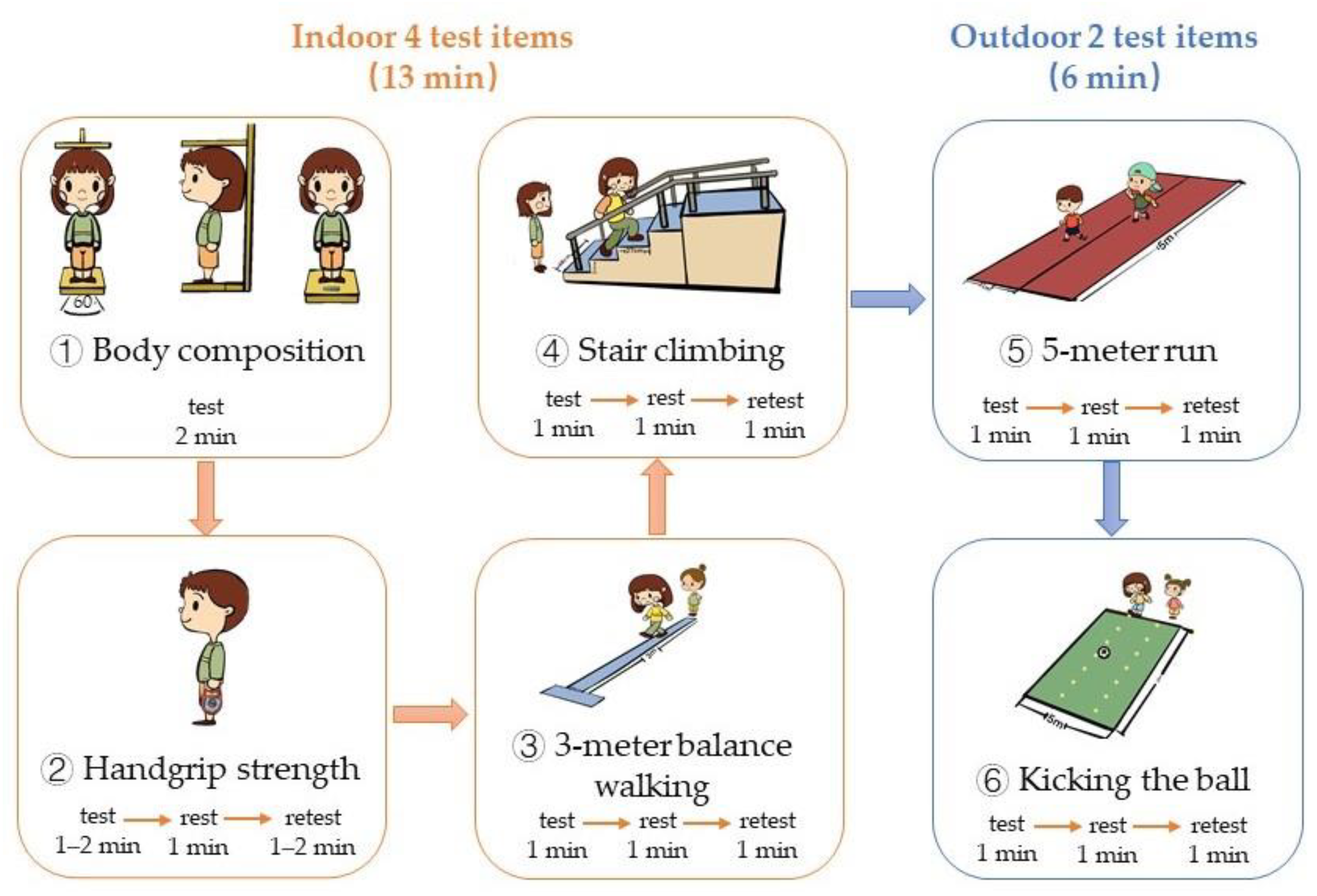
2.3. Procedure
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Participants
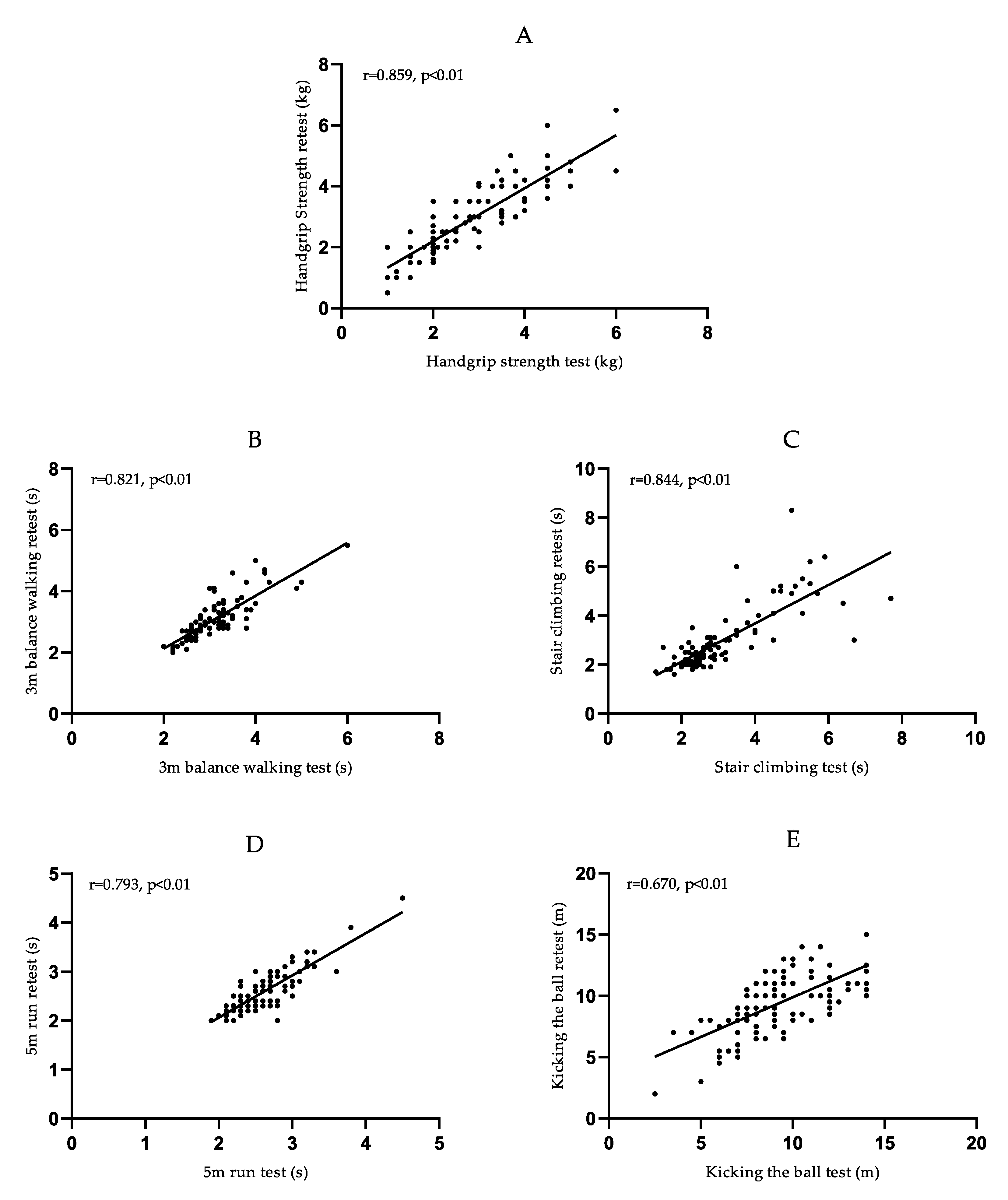
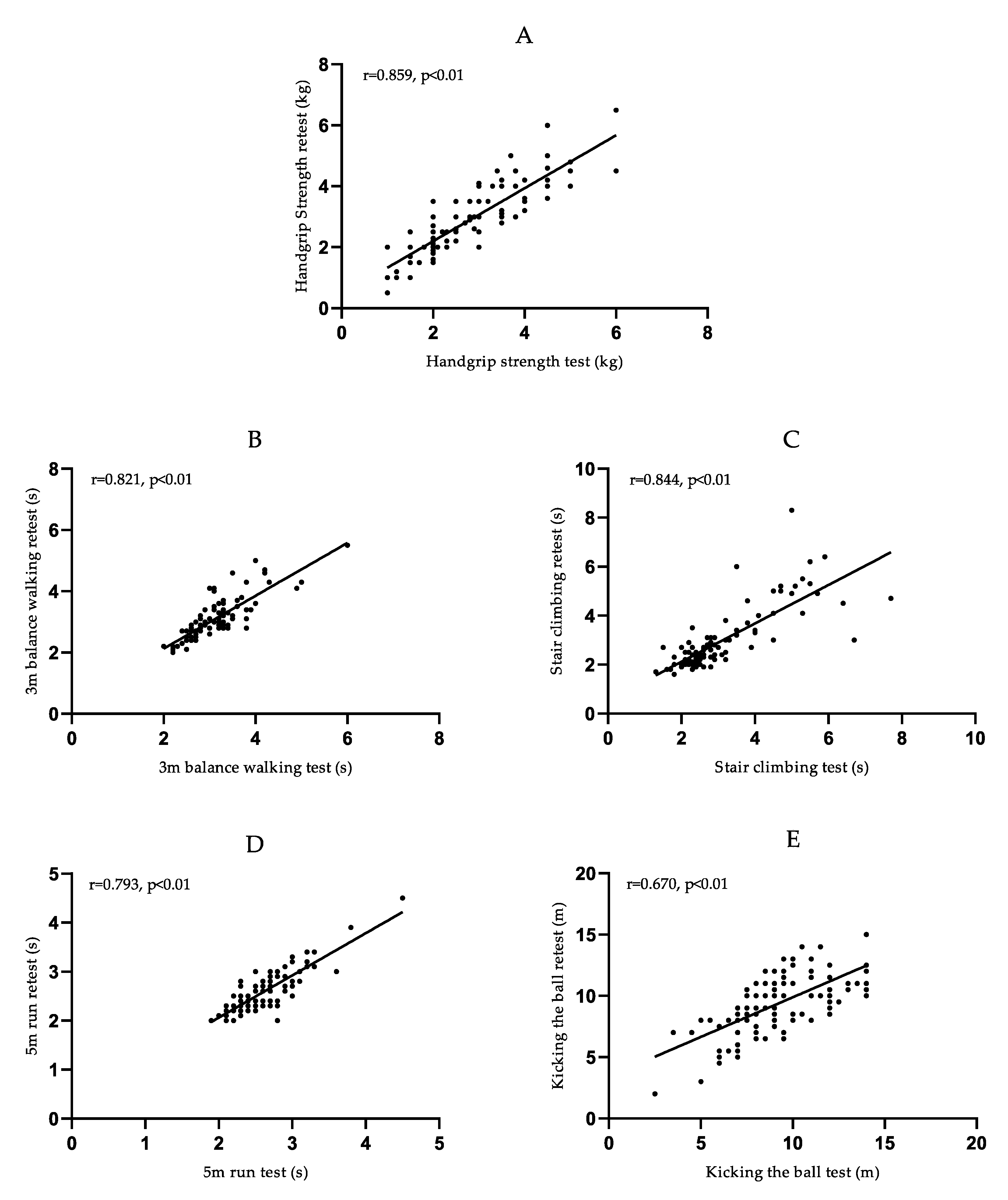
3.2. Reliability of Physical Fitness Test Items
3.3. Correlations between the Physical Fitness Test Items
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Corbin, C.B.; Welk, G.J.; Corbin, W.R.; Welk, K. Concepts of Physical Fitness: Active Lifestyles for Wellness; McGraw-Hill: New York, NY, USA, 2008. [Google Scholar]
- Wolters, K. ACSM’s Health-Related Physical Fitness Assessment Manual, 5th ed.; American College of Sports Medicine: Indianapolis, IN, USA, 2018; pp. 2–5. [Google Scholar]
- Donnelly, J.E.; Hillman, C.H.; Castelli, D.; Etnier, J.L.; Lee, S.; Tomporowski, P.; Lambourne, K.; Szabo-Reed, A.N. Physical Activity, Fitness, Cognitive Function, and Academic Achievement in Children: A Systematic Review. Med. Sci. Sports Exerc. 2016, 48, 1197–1222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raine, L.B.; Lee, H.K.; Saliba, B.J.; Chaddock-Heyman, L.; Hillman, C.; Kramer, A. The Influence of Childhood Aerobic Fitness on Learning and Memory. PLoS ONE 2013, 8, e72666. [Google Scholar] [CrossRef] [Green Version]
- Hillman, C.H.; Buck, S.M.; Themanson, J.R.; Pontifex, M.B.; Castelli, D.M. Aerobic fitness and cognitive development: Event-related brain potential and task performance indices of executive control in preadolescent children. Dev. Psychol. 2009, 45, 114–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warburton, D.E.R.; Nicol, C.W.; Bredin, S.S.D. Health benefits of physical activity: The evidence. Can. Med. Assoc. J. 2006, 174, 801–809. [Google Scholar] [CrossRef] [Green Version]
- Myers, J.; Kokkinos, P.; Nyelin, E. Physical Activity, Cardiorespiratory Fitness, and the Metabolic Syndrome. Nutrients 2019, 11, 1652. [Google Scholar] [CrossRef] [Green Version]
- Zhao, T.; Le, S.; Freitag, N.; Schumann, M.; Wang, X.; Cheng, S. Effect of Chronic Exercise Training on Blood Lactate Metabolism Among Patients with Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis. Front. Physiol. 2021, 12, 652023. [Google Scholar] [CrossRef]
- Ji, M.; Tang, A.; Zhang, Y.; Zou, J.; Zhou, G.; Deng, J.; Yang, L.; Li, M.; Chen, J.; Qin, H.; et al. The Relationship between Obesity, Sleep and Physical Activity in Chinese Preschool Children. Int. J. Environ. Res. Public Health 2018, 15, 527. [Google Scholar] [CrossRef] [Green Version]
- Tam, C.S.; Ravussin, E. Energy balance: An overview with emphasis on children. Pediatr. Blood Cancer 2012, 58, 154–158. [Google Scholar] [CrossRef] [Green Version]
- Bassett, D.R.; John, D.; Conger, S.A.; Fitzhugh, E.C.; Coe, D.P. Trends in Physical Activity and Sedentary Behaviors of United States Youth. J. Phys. Act. Health 2015, 12, 1102–1111. [Google Scholar] [CrossRef]
- Byrd-Bredbenner, C.; Martin-Biggers, J.; Povis, G.A.; Worobey, J.; Hongu, N.; Quick, V. Promoting healthy home environments and lifestyles in families with preschool children: HomeStyles, a randomized controlled trial. Contemp. Clin. Trials 2018, 64, 139–151. [Google Scholar] [CrossRef]
- Hadders-Algra, M. Early human motor development: From variation to the ability to vary and adapt. Neurosci. Biobehav. Rev. 2018, 90, 411–427. [Google Scholar] [CrossRef]
- Phillips, D.A.; Lowenstein, A.E. Early care, education, and child development. Annu. Rev. Psychol. 2011, 62, 483–500. [Google Scholar] [CrossRef]
- Pahkala, K.; Hernelahti, M.; Heinonen, O.J.; Raittinen, P.; Hakanen, M.; Lagström, H.; Viikari, J.S.; Rönnemaa, T.; Raitakari, O.T.; Simell, O. Body mass index, fitness and physical activity from childhood through adolescence. Br. J. Sports Med. 2013, 47, 71–77. [Google Scholar] [CrossRef] [Green Version]
- Jenni, O.G.; Chaouch, A.; Caflisch, J.; Rousson, V. Infant motor milestones: Poor predictive value for outcome of healthy children. Acta Paediatr. 2013, 102, e181-4. [Google Scholar] [CrossRef]
- Messerli-Bürgy, N.; Kakebeeke, T.H.; Meyer, A.H.; Arhab, A.; Zysset, A.E.; Stülb, K.; Leeger-Aschmann, C.S.; Schmutz, E.A.; Kriemler, S.; Puder, J.J.; et al. Walking onset: A poor predictor for motor and cognitive skills in healthy preschool children. BMC Pediatr. 2021, 21, 367. [Google Scholar] [CrossRef]
- Committee on Fitness Measures and Health Outcomes in Youth; Food and Nutrition Board; Institute of Medicine. Fitness Measures and Health Outcomes in Youth; Pillsbury, L., Oria, M., Pate, R., Eds.; National Academies Press: Washington, DC, USA, 2013. [Google Scholar]
- Ruiz, J.R.; Castro-Piñero, J.; España-Romero, V.; Artero, E.G.; Ortega, F.B.; Cuenca, M.M.; Jimenez-Pavón, D.; Chillón, P.; Girela-Rejón, M.J.; Mora, J.; et al. Field-based fitness assessment in young people: The ALPHA health-related fitness test battery for children and adolescents. Br. J. Sports Med. 2011, 45, 518–524. [Google Scholar] [CrossRef]
- Council of Europe Publishing and Documentation Service Eurofit. Handbook for the EUROFIT Tests of Physical Fitness: Sports Division 299 Strasbourg; Council of Europe Publishing and Documentation Service: Strasbourg, France, 1993. [Google Scholar]
- Meredith, M.D.; Welk, G.; The Cooper Institute. Fitnessgram and Activitygram Test Administration Manual-Updated, 4th ed.; Human Kinetics: Champaign, IL, USA, 2010. [Google Scholar]
- Cadenas-Sanchez, C.; Tellez, B.M.; Sanchez-Delgado, G.; Mora-Gonzalez, J.; Castro-Piñero, J.; Löf, M.; Ruiz, J.R.; Ortega, F.B. Assessing physical fitness in preschool children: Feasibility, reliability and practical recommendations for the PREFIT battery. J. Sci. Med. Sport 2016, 19, 910–915. [Google Scholar] [CrossRef]
- Cadenas-Sanchez, C.; Intemann, T.; Labayen, I.; Peinado, A.B.; Vidal-Conti, J.; Sanchis-Moysi, J.; Moliner-Urdiales, D.; Perez, M.A.R.; Garcia-Prieto, J.C.; Santos, J.D.R.F.; et al. Physical fitness reference standards for preschool children: The PREFIT project. J. Sci. Med. Sport 2019, 22, 430–437. [Google Scholar] [CrossRef] [Green Version]
- Latorre Román, P.; Mora López, D.; Fernández Sánchez, M.; Salas Sánchez, J.; Moriana Coronas, F.; García-Pinillos, F. Test-retest reliability of a field-based physical fitness assessment for children aged 3–6 years. Nutr. Hosp. 2015, 32, 1683–1688. [Google Scholar]
- Latorre-Román, P.A.; Mora-López, D.; García-Pinillos, F. Effects of a physical activity programme in the school setting on physical fitness in preschool children. Child Care Health Dev. 2018, 44, 427–432. [Google Scholar] [CrossRef]
- Fang, H.; Ho, I.M.K. Intraday reliability, sensitivity, and minimum detectable change of national physical fitness measurement for preschool children in China. PLoS ONE 2020, 15, e0242369. [Google Scholar] [CrossRef]
- Fang, H.; Quan, M.; Zhou, T.; Sun, S.; Zhang, J.; Zhang, H.; Cao, Z.; Zhao, G.; Wang, R.; Chen, P. Relationship between Physical Activity and Physical Fitness in Preschool Children: A Cross-Sectional Study. BioMed Res. Int. 2017, 2017, 9314026. [Google Scholar] [CrossRef]
- Amado-Pacheco, J.C.; Prieto-Benavides, D.H.; Correa-Bautista, J.E.; García-Hermoso, A.; Agostinis-Sobrinho, C.; Alonso-Martínez, A.M.; Izquierdo, M.; Ramírez-Vélez, R. Feasibility and Reliability of Physical Fitness Tests among Colombian Preschool Children. Int. J. Environ. Res. Public Health 2019, 16, 3069. [Google Scholar] [CrossRef] [Green Version]
- Radecki, L.; Sand-Loud, N.; O’Connor, K.G.; Sharp, S.; Olson, L.M. Trends in the Use of Standardized Tools for Developmental Screening in Early Childhood: 2002–2009. Pediatrics 2011, 128, 14–19. [Google Scholar] [CrossRef]
- Council on Children with Disabilities; Section on Developmental Behavioral Pediatrics; Bright Futures Steering Committee; Medical Home Initiatives for Children with Special Needs Project Advisory Committee. Identifying infants and young children with developmental disorders in the medical home: An algorithm for developmental surveillance and screening. Pediatrics 2006, 118, 405–420. [Google Scholar] [CrossRef] [Green Version]
- Sheldrick, R.C.; Marakovitz, S.; Garfinkel, D.; Carter, A.S.; Perrin, E.C. Comparative Accuracy of Developmental Screening Questionnaires. JAMA Pediatr. 2020, 174, 366–374. [Google Scholar] [CrossRef]
- WHO Multicentre Growth Reference Study Group; de Onis, M. WHO Child Growth Standards based on length/height, weight and age. Acta Paediatr. 2006, 95, 76–85. [Google Scholar]
- Latorre Román, P.; Moreno Del Castillo, R.; Lucena Zurita, M.; Salas Sánchez, J.; García-Pinillos, F.; Mora López, D. Physical fitness in preschool children: Association with sex, age and weight status. Child Care Health Dev. 2017, 43, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Henriksson, P.; Cadenas-Sanchez, C.; Leppänen, M.H.; Nyström, C.D.; Ortega, F.B.; Pomeroy, J.; Ruiz, J.R.; Löf, M. Associations of Fat Mass and Fat-Free Mass with Physical Fitness in 4-Year-Old Children: Results from the MINISTOP Trial. Nutrients 2016, 8, 473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lubans, D.R.; Morgan, P.J.; Cliff, D.P.; Barnett, L.M.; Okely, A.D. Fundamental movement skills in children and adolescents: Review of associated health benefits. Sports Med. 2010, 40, 1019–1035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marrus, N.; Eggebrecht, A.T.; Todorov, A.; Elison, J.T.; Wolff, J.J.; Cole, L.; Gao, W.; Pandey, J.; Shen, M.D.; Swanson, M.; et al. Walking, Gross Motor Development, and Brain Functional Connectivity in Infants and Toddlers. Cereb. Cortex 2018, 28, 750–763. [Google Scholar] [CrossRef]
- Sanchez-Delgado, G.; Cadenas-Sanchez, C.; Mora-Gonzalez, J.; Martinez-Tellez, B.; Chillón, P.; Löf, M.; Ortega, F.B.; Ruiz, J.R. Assessment of handgrip strength in preschool children aged 3 to 5 years. J. Hand Surg. Eur. Vol. 2015, 40, 966–972. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Boys (n = 44) Mean ± SD | Girls (n = 59) Mean ± SD | Sig. | 2 Years (n = 41) Mean ± SD | 3 Years (n = 62) Mean ± SD | Sig. | Total (n = 103) Mean ± SD | |
|---|---|---|---|---|---|---|---|
| Age (years) | 2.96 ± 0.27 | 3.04 ± 0.26 | ns | 2.74 ± 0.14 | 3.18 ± 0.15 | ** | 3.01 ± 0.26 |
| Weight (kg) | 14.88 ± 1.80 | 14.71 ± 1.67 | ns | 14.21 ± 1.54 | 15.15 ± 1.74 | ** | 14.78 ± 1.72 |
| Height (cm) | 96.67 ± 5.00 | 96.82 ± 4.15 | ns | 94.07 ± 3.89 | 98.53 ± 4.00 | ** | 96.75 ± 4.51 |
| Body mass index (kg/m2) | 15.89 ± 1.02 | 15.66 ± 1.04 | ns | 16.03 ± 1.10 | 15.57 ± 0.95 | * | 15.76 ± 1.03 |
| Handgrip strength (kg) | 3.25 ± 1.30 | 2.94 ± 1.04 | ns | 2.84 ± 1.24 | 3.22 ± 1.09 | ns | 3.07 ± 1.16 |
| 3 m balance walking (s) | 3.03 ± 0.66 | 2.93 ± 0.44 | ns | 3.24 ± 0.62 | 2.80 ± 0.41 | ** | 2.98 ± 0.54 |
| Stair climbing (s) | 2.87 ± 1.19 | 2.68 ± 0.88 | ns | 3.20 ± 1.21 | 2.47 ± 0.76 | ** | 2.76 ± 1.02 |
| 5 m run (s) | 2.51 ± 0.49 | 2.46 ± 0.28 | ns | 2.60 ± 0.41 | 2.40 ± 0.35 | ** | 2.48 ± 0.39 |
| Kicking the ball (m) | 10.55 ± 2.60 | 10.25 ± 2.49 | ns | 9.26 ± 2.36 | 11.11 ± 2.37 | ** | 10.37 ± 2.53 |
| Test (n = 103) Mean ± SD | Retest (n = 103) Mean ± SD | Pearson Correlation | ICC | 95% Confidence Interval | |
|---|---|---|---|---|---|
| Handgrip strength (kg) | 2.80 ± 1.10 | 2.89 ± 1.12 | 0.859 | 0.857 | 0.795~0.901 |
| 3 m balance walking (s) | 3.13 ± 0.61 | 3.10 ± 0.64 | 0.821 | 0.821 | 0.746~0.875 |
| Stair climbing (s) | 3.05 ± 1.23 | 2.94 ± 1.22 | 0.844 | 0.791 | 0.706~0.854 |
| 5 m run (s) | 2.58 ± 0.40 | 2.56 ± 0.41 | 0.793 | 0.844 | 0.779~0.892 |
| Kicking the ball (m) | 9.40 ± 2.62 | 9.50 ± 2.53 | 0.670 | 0.672 | 0.550~0.765 |
| Weight | Height | Body Mass Index | Handgrip Strength | 3 m Balance Walking | Stair Climbing | 5 m Run | Kicking the Ball | |
|---|---|---|---|---|---|---|---|---|
| Weight | 1 | 0.804 ** | 0.576 ** | 0.190 | −0.194 * | −0.041 | −0.078 | 0.138 |
| Height | 1 | −0.018 | 0.236 * | −0.293 ** | −0.220 * | −0.217 * | 0.161 | |
| Body mass index | 1 | 0.008 | 0.085 | 0.230* | 0.170 | 0.013 | ||
| Handgrip strength | 1 | −0.341 ** | −0.484 ** | −0.404 ** | 0.211 * | |||
| 3 m balance walking | 1 | 0.551 ** | 0.576 ** | −0.270 ** | ||||
| Stair climbing | 1 | 0.586 ** | −0.299 ** | |||||
| 5 m run | 1 | −0.164 | ||||||
| Kicking the ball | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ke, D.; Wang, D.; Huang, H.; Hu, X.; Sasaki, J.; Liu, H.; Wang, X.; Lu, D.; Wang, J.; He, G. Study of the Reliability of Field Test Methods for Physical Fitness in Children Aged 2–3 Years. Int. J. Environ. Res. Public Health 2022, 19, 7522. https://doi.org/10.3390/ijerph19127522
Ke D, Wang D, Huang H, Hu X, Sasaki J, Liu H, Wang X, Lu D, Wang J, He G. Study of the Reliability of Field Test Methods for Physical Fitness in Children Aged 2–3 Years. International Journal of Environmental Research and Public Health. 2022; 19(12):7522. https://doi.org/10.3390/ijerph19127522
Chicago/Turabian StyleKe, Dandan, Duona Wang, Hui Huang, Xiangying Hu, Jun Sasaki, Hezhong Liu, Xiaofei Wang, Dajiang Lu, Jian Wang, and Gengsheng He. 2022. "Study of the Reliability of Field Test Methods for Physical Fitness in Children Aged 2–3 Years" International Journal of Environmental Research and Public Health 19, no. 12: 7522. https://doi.org/10.3390/ijerph19127522
APA StyleKe, D., Wang, D., Huang, H., Hu, X., Sasaki, J., Liu, H., Wang, X., Lu, D., Wang, J., & He, G. (2022). Study of the Reliability of Field Test Methods for Physical Fitness in Children Aged 2–3 Years. International Journal of Environmental Research and Public Health, 19(12), 7522. https://doi.org/10.3390/ijerph19127522