
Ableism and Contours of the Attitudinal Environment as Identified by Adults with Long-Term Physical Disabilities: A Qualitative Study

 ,
,  , ,
, ,  and
and 
Abstract
:1. Introduction
A network of beliefs, processes and practices that produces a particular kind of self and body (the corporeal standard) that is projected as the perfect, species-typical and therefore essential and fully human. Disability then is cast as a diminished state of being human.[6] (p. 44)
2. Materials and Methods
2.1. Recruitment and Screening
2.2. Data Collection
2.3. Analysis
3. Results
3.1. Individual, Group, and Societal Attitudes
3.1.1. Understanding
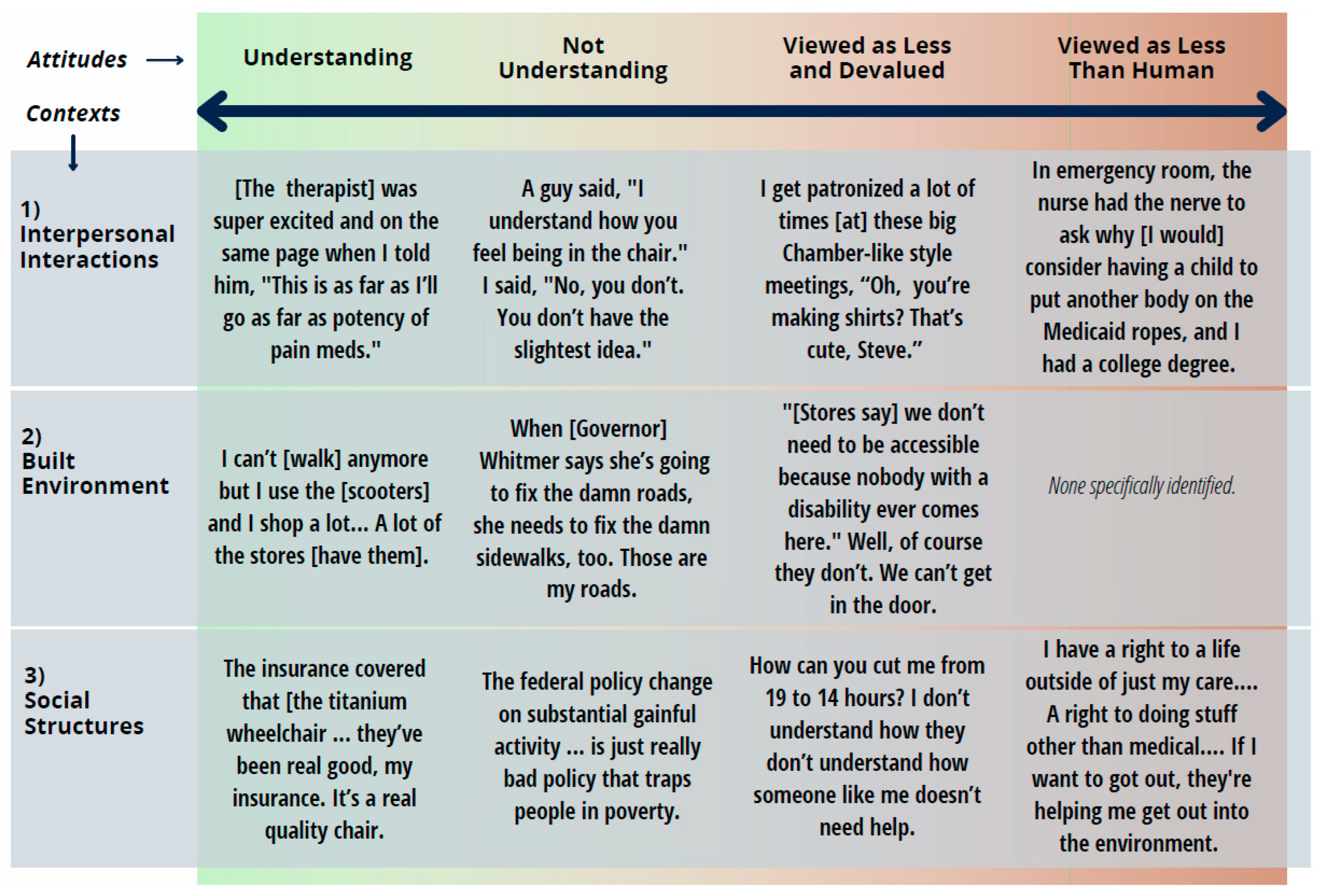
[The physical therapist] was like, “So you’ve never been on pain meds or muscle relaxers because of your CP [chronic pain]?” And I’m like, “Well, no, I’ve never really been on pain meds, and I’ve only been on one muscle relaxer, and it didn’t help”. And he’s like, “There’s so much we can do with you”. Like he was super excited, and he was on the same page when I told him you know, “This is as far as I’ll go as far as, um, potency of pain meds”.
What helps me is when the doctors and therapists talk to me and empower me to say, if you can make it work for you this way, we’re not going to worry about it that way. So that helped me to be able to combat my friends, my peers, my family members, that were saying, “No, you…” [And I am able to reply,] “No, I talked to this person who is a professional, who understands it, and she said it was fine if I do it this way, so you need to go there”.
3.1.2. Not Understanding
I don’t think there’s any sort of—sort of societal understanding that disability is not constant, that there’s ups and downs to how you experience disability…I think sometimes people think that person is faking when they’re less able”.
She doesn’t understand that, yeah, some days I can go in here and wipe down the counters and clean the kitchen, but today ain’t the day. Or, I could do this part, but I need you to come this week to mop the floors, she’s looking at me like, “You can do that. You can—you can go to all of these meetings and work all these jobs, but you can’t mop a floor?”
I had a guy one time; he said, “I understand how you feel being in the chair”. I said, “No, you don’t. You don’t have the slightest idea”. I said, “You think you that you understand”.
They’re not trying to not invite you. They’re thinking, “Well, she’s in a wheelchair, she can’t dance, why would we invite her?” And I’m telling them, “Invite me, it’s your birthday party!” So, I have to give people permission to be okay with me.
3.1.3. Viewed as Less and Devalued
It’s really frustrating and depressing when a doctor doesn’t listen to a patient and just talks over them or ignores what they say. That’s probably the one of the biggest pitfalls with being disabled that I found, is doctors already formulating their opinion of that—, they don’t wanna listen to the patient. They wanna tell a patient what to do, “Well, you shouldn’t transfer that way”. What do you mean? How do you know that? Have you ever transferred? You don’t know what you’re talking about? So, nope, doctors and people who are not, can’t conceive of what’s going on with a patient is very difficult for them to teach other people or communicate with or be able to take care of the patient.
I remember I had one doctor, I told him. He said, “Why do you use a wheelchair?” And I said, “I have ataxia”. And he proceeded to mansplain to me that ataxia is a symptom of MS. It is not a disease, and I chewed him a new one. Of course, I was on a lot of drugs at the time, but his resident students were with him. And I think they all got a very clear message that you don’t--don’t pretend you know more about this than I do because I’ve been dealing with it for years.
How to be looked upon as a businessperson, like, how other people look at other businesspeople, you know, that run corporations or run small businesses, they see them as a business, and they don’t see them as a hobby. I get patronized a lot of times when these big Chamber-like style meetings, where they go, “Oh, that’s—you know, you’re making [the product]? That’s cute, Steve”. I even get the pat on my shoulder, like, “That’s a good job. Good job that you—” you know, I feel like it brings me to where I am, like, in kindergarten, fingerpainting or something, like, “Okay, I’ll go out in my corner, and I make pictures all day, or something,” like, if they—some people treat it that way [...] that challenge is—is—to be able to be respected in that level [...] Man, I just need to—I want them to respect it”.
I had friends before my accident, and, you know, I would go and—and check on them, because they—I lived on the east side of Detroit, and they stayed on the west side. And I would go see them every once in a while, just to check on them or whatever. [...] And of course, since my accident, um, I—let’s just say I don’t get that back in return.
I told him I was—you know, I’m still looking for somebody. So, he basically put it on his Facebook page, “Would anybody want to date a guy in a wheelchair?” And everybody who responded said no. I’m like, “Thanks, [name of person]. Way to make me feel better. Way to fill me with confidence and self-esteem”. [...] Yeah, it just—it just—you know, you think—you know, you try to put yourself out there as a nice guy, then something like this just go ahead, and just take your balloon and just [boof].
3.1.4. Viewed as Less Than Human
Some people won’t help you. They’ll see you struggling, and they will close the door on you, they’ll do—and so, that makes you think, “Wait a minute. Am I invisible? What just happened here?”
I quit trying to do it [get out of gravel] and I just was waving, and it took me—it took—took about an hour and a half before somebody came and helped me.
Where have you addressed the people with disabilities? Not once. Not once. […] Even in Michigan when—the State of the Address—I have made a design. It’s got the Michigan logo, and then it said ‘invisible’ and it was invisible because that’s how I felt. We feel invisible. I feel invisible. […] My car is like a smart car. Me and my chair is like as big as a smart car. People bump into me. Like how do you not see me? We’re very invisible because things are made—decisions are made in this country without the voice of people with the disabilities.
Normal [able-bodied] people, they don’t want you riding in the street. They would tell you to get the—out of the street. [...] They will—they do it all the time, and it makes you not even want to go nowhere, because of the fact that you got people telling you to get the—out of the street, and it’s like, what am I supposed to do if the sidewalks are not—are not good? […] They are going to tell me to get the fuck out of the street.
Oh yeah, there’s definitely a stigma in society you know. They see you in a wheelchair and they don’t they look away or they look at you like you have two heads. But some people just stare, they stare and they follow you and watch you and watch what you’re doing.
I know I went to, uh, looking for a prom dress, in my senior year, and the, um—and the owner of the store essentially threw me out of the store when I went with my mom, because he didn’t want me to try any dresses and stuff, uh, because he caught me when I came in and said, you know, “Well, who’s going to help you?” I said, “Well, I can do it myself, but I have my mom here”. He said, “Well, we’re about to close”.
I was 22 when I was pregnant, so, for the most part, my first—the first six months of my pregnancy was horrible. I was very, very sick, and I had to go to the emergency room more than once. This particular time, I was so sick, and I couldn’t even sit up in the car, and they called an ambulance to come and get me. When I got to the emergency room, the nurse had the nerve to ask me why [I would] consider having a child to put another body on the Medicaid ropes, and I had a college degree.
The other week, I was sick, and I had to go up to the emergency room, and I was laying on the dirt in the hall. And they said, “Ma’am, we need a urine sample”. I said, “Okay, you can have a urine sample. But I need help getting to the bathroom, and I need a cath”. The lady looked at me, she turned her head, and started talking to somebody else. And I called her, I said, “Ma’am, I have to use the restroom, you said you needed a urine sample”. She looked at me again and walked away. Somebody else came and they said, “Okay, I’m going to put the cath—” [To which I replied,] “No, I have to go to the bathroom, I need some help”.
3.2. Built Environment
3.2.1. Understanding
I can’t shop anymore but I use the Amigos [scooters provided by the store] and I shop a lot. At the stores, now I’ve noticed that a lot of the stores [provide scooters].
3.2.2. Not Understanding
I think primarily it’s cost, but it might be ignorance. Yeah, a lot of excuses running around on it, like uh maybe misunderstanding.
I don’t think it’s enforced, really, at all.
Really, if I can be so bold as to say, when [Michigan Governor] Gretchen Whitmer says she’s going to fix the damn roads, she needs to fix the damn sidewalks too. [laughter from others in focus group] Because those are my roads. [Athena]
3.2.3. Viewed as Less and Devalued
DHS [Michigan’s Department of Health and Human Services was] more concerned with my homeowner’s insurance than they were trying to pay for a ramp. They said if I didn’t show proof of my homeowner’s insurance, they didn’t want nothing to do with it.
I have to fight just to get a handicap accessible button on the door. It took me a year and a half to get that at my school. Something that was already on there, back in the ’80s, but for some reason, they took it off. [Because there was no button for accessing the school’s restroom,] I used to have to walk to Burger King just to use the bathroom. I used to have to walk to Coney Island to use the bathroom. And then, go all the way back to school, then go all the way—then press the button on the elevator, and go all the way back upstairs and go to class.
A lot of the restaurants and social areas and new development housing has more to do with people’s attitudes toward individuals. […] I’ve been at a lot of housing conferences, so when they talk about new development, and you ask a question, “Why is everything a second-floor walk-up development, what about individuals in wheelchairs?” “Well, they’re going to have to produce minimum visitability,” that means that one entrance is at ground level. The entrance doesn’t have to have a bathroom.
I think [restaurants] hope nobody asks and that we’ll get away with it because of the idea of—of people saying, well, we don’t need to be accessible because nobody with a disability ever comes here. Well, of course they don’t because we can’t get in the door!
3.2.4. Viewed as Less Than Human
3.3. Social Institutions, Programs, Systems, and Structures
3.3.1. Understanding
The insurance covered that [the titanium wheelchair he had custom made]; the insurance covered the parts after two years. [inaudible] I replaced the seat, matter of fact I placed a seat about I think within that year, I replaced [inaudible] and insurance paid for it, they’ve been real good, my insurance. It’s a real quality chair, it’s a Dixie chair. It’s a good name brand, I had no problem with it, just working it out.
[I think the system works and is fair] because even me—like, in a handicapped vehicle, I went to Michigan—Michigan Rehabilitation Services, which is MRS, and they get funding to help, um, people’s—whatever, to help them be able to stay working, so I was like, “I need a vehicle to get to work. I need a handicapped vehicle to get to work”. They brought me two in the past.
3.3.2. Not Understanding
If you make more than $1100 in the Social Security disability check, you don’t qualify for Medicaid, which means that you don’t qualify for services that you need to help you with your daily living supports.
“It’s the limits on the insurance [that makes my health care only adequate]. It’s really not the health care workers. I see them go out of their way to try and do as much as they can with the limits that’re put on them. They give me information, they give me what resources they can, they motivate me, they answer my questions, but they’re limited in what they’re able to do”.
I would love it if they [PCAs] could be paid more; things would be so much better for me. You know they-they’re making $9.65 an hour right now. And anyone can go to McDonald’s and make, I don’t know, $12 or $15 or whatever. [...] I think that that right there would probably weed a lot of people they would--they wouldn’t be forced to hire certain people that were unqualified or whatever. And [hire] more and more-more caring people if they were making a certain amount of money.
3.3.3. Viewed as Less and Devalued
How you can cut me from 19 to 14 h, when I’m actually somebody who—who really needs the care. [...] when it comes to somebody like me, I consider myself almost like a 24-h care [....] But when it comes to somebody like me, you know, who actually needs the care, you know. I didn’t ask to, um, have this disease or be born with it. [… They] dictate your life, and then kind of like how many hours you should get or—or shouldn’t get…like how can you tell me how many hours I should or shouldn’t qualify for…I don’t understand how they don’t understand how someone like me doesn’t need the help, you know.
If we really meant something in this country, when they have these coronavirus briefings every day, instead of addressing the seniors and the people in the nursing homes, where have you addressed the people with disabilities? Not once. Not once. [...] I have made a design. It’s got the Michigan logo, and then it said ‘invisible’ and it was invisible because that’s how I felt. [...] We’re very invisible because things are made—decisions are made in this country without the voice of people with the disabilities.
3.3.4. Viewed as Less Than Human
So yeah, attitude—I mean thinking of disability as a 100% negative thing is, um, pervasive. […] If we have a mindset of disability as bad or negative, it makes us want to get rid of it […] by shoving them in nursing homes or killing them or um, you know, ignoring them. [Olivia]
It’s like I have right to a life, you know, outside of just my care, you know. [...] Doing stuff outside of medical, you know. It’s whatever. If it’s they take me outside, and we’re sitting outside and we’re playing cards outside, you know. That’s a right to just do something other than medical.
It’s not just physical that we require. […] I feel like anything that—that has something where it can help make our lives better or a little more normal than before, that they should be, like, okay with it, but since it’s not, like a medical thing, they feel like that’s something they shouldn’t have to pay for.
4. Discussion
4.1. Recommendations for Future Research
4.2. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- Background: If you can introduce yourself—that would be great. Just say your first name and a little bit about yourself. What type of physical disability do you have? How long have you had it? What are the key activities and identities that are important to you?
- Health: Please provide information about your health and the issues that have come up with aging with a physical disability.
- Personal support: What personal support, including family and friends, have allowed you to maintain your health?
- Community supports and programs: What community supports and programs, including faith-based initiatives, transportation, and other services, have supported your physical and emotional health as well as ability to participate in employment and other important life activities?
- Supports related to healthcare access and quality: What factors related to your access to healthcare, including health insurance, have been most important in helping you to maintain your health?
- Role of equipment and assistive technology in aging with a disability: What assistive technology, including access to durable medical equipment, wheelchairs, and the internet?
- Role of the built/physical environment: What components of the built environment (home, community, other) have supported your physical and emotional health as well as ability to participate in employment and other important life activities?
- Role of attitudinal environment: How has the knowledge and attitudes of people whom you encounter in your community and healthcare environments impacted your ability to maintain your health?
- Role of policy: Are there local, regional, and national policies that you feel are particularly helpful or have supported your physical and emotional health as well as ability to participate in your community and other important life activities?
- Other important issues or advice: Discrimination related to race, gender and age pose serious problems in our society. In what ways did this impact your health? So, what have we missed? Are there other things that we have not yet talked about which you think were relevant to aging with a physical disability?
References
- Disability Inclusion Overview; World Bank: Washington, DC, USA, 2021.
- Centers for Disease Control and Prevention. Disability Impacts All of Us Infographic; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2019; Volume 8. [Google Scholar]
- Nario-Redmond, M.R. Ableism: The Causes and Consequences of Disability Prejudice, 1st ed.; Wiley-Blackwell: Oxford, UK, 2019; p. 400. [Google Scholar]
- World Health Organization. International Classification of Functioning, Disability and Health; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- World Health Organization. Towards a Common Language for Functioning, Disabilit and Health: ICF; World Health Organization: Geneva, Switzerland, 2002; p. 1021. [Google Scholar]
- Campbell, F. Inciting legal fictions: ‘disability’s’ date with ontology and the ableist body of the law. Griffith Law Rev. 2001, 10, 42. [Google Scholar]
- Wolbring, G. Ability Privilege: A Needed Addition to Privilege Studies; ID 2487616; Social Science Research Network: Rochester, NY, USA, 2014. [Google Scholar]
- Namkung, E.H.; Carr, D. The Psychological Consequences of Disability over the Life Course: Assessing the Mediating Role of Perceived Interpersonal Discrimination. J. Health Soc. Behav. 2020, 61, 190–207. [Google Scholar] [CrossRef]
- Emerson, E.; Milner, A.; Aitken, Z.; Krnjacki, L.; Vaughan, C.; Llewellyn, G.; Kavanagh, A. Overt acts of perceived discrimination reported by British working-age adults with and without disability. J. Public Health 2019, 43, e16–e23. [Google Scholar] [CrossRef] [PubMed]
- Hammel, J.; Magasi, S.; Heinemann, A.; Gray, D.B.; Stark, S.; Kisala, P.; Carlozzi, N.E.; Tulsky, D.; Garcia, S.F.; Hahn, E.A. Environmental Barriers and Supports to Everyday Participation: A Qualitative Insider Perspective From People With Disabilities. Arch. Phys. Med. Rehabil. 2015, 96, 578–588. [Google Scholar] [CrossRef] [PubMed]
- Snyder, L.A.; Carmichael, J.S.; Blackwell, L.V.; Cleveland, J.N.; Thornton, G.C. Perceptions of discrimination and justice among employees with disabilities. Empl. Responsib. Rights J. 2010, 22, 5–19. [Google Scholar] [CrossRef]
- Carr, D.; Namkung, E.H. Physical Disability at Work: How Functional Limitation Affects Perceived Discrimination and Interpersonal Relationships in the Workplace. J. Health Soc. Behav. 2021, 62, 545–561. [Google Scholar] [CrossRef] [PubMed]
- Moscoso-Porras, M.G.; Alvarado, G.F. Association between perceived discrimination and healthcare–seeking behavior in people with a disability. Disabil. Health J. 2018, 11, 93–98. [Google Scholar] [CrossRef]
- Link, B.G.; Phelan, J.C. Conceptualizing Stigma. Annu. Rev. Sociol. 2001, 27, 363–385. [Google Scholar] [CrossRef]
- Hatzenbuehler, M.L.; Link, B.G. Introduction to the special issue on structural stigma and health. Soc. Sci. Med. 2014, 103, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Hatzenbuehler, M.L. Structural Stigma: Research Evidence and Implications for Psychological Science. Am. Psychol. 2016, 71, 742–751. [Google Scholar] [CrossRef] [PubMed]
- Bos, A.E.R.; Pryor, J.B.; Reeder, G.D.; Stutterheim, S.E. Stigma: Advances in Theory and Research. Basic Appl. Soc. Psychol. 2013, 35, 1–9. [Google Scholar] [CrossRef]
- Corrigan, P.W.; Lam, C. Challenging the structural discrimination of psychiatric disabilities: Lessons learned from the American disability community. Rehabil. Educ. 2007, 21, 53–58. [Google Scholar] [CrossRef]
- Auterman, B.L. Structural Ableism: Disability, Institutionalized Discrimination, and Denied Citizenship; Sarah Lawrence College: Yonkers, NY, USA, 2011. [Google Scholar]
- Hansen, H.; Bourgois, P.; Drucker, E. Pathologizing poverty: New forms of diagnosis, disability, and structural stigma under welfare reform. Soc. Sci. Med. 2014, 103, 76–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stark, S.; Hollingsworth, H.H.; Morgan, K.A.; Gray, D.B. Development of a measure of receptivity of the physical environment. Disabil. Rehabil. 2007, 29, 123–137. [Google Scholar] [CrossRef] [PubMed]
- Hamraie, A.a. Building access: Universal Design and the Politics of Disability; University of Minnesota Press: Minneapolis, MN, USA, 2017. [Google Scholar]
- Livingston, K. When architecture disables: Teaching undergraduates to perceive ableism in the built environment. Teach. Sociol. 2000, 28, 182–191. [Google Scholar] [CrossRef]
- Clarke, P.; Twardzik, E.; Meade, M.A.; Peterson, M.D.; Tate, D. Social participation among adults aging with long-term physical disability: The role of socioenvironmental factors. J. Aging Health 2019, 31, 145S–168S. [Google Scholar] [CrossRef]
- Imrie, R. Barriered and Bounded Places and the Spatialities of Disability. Urban Stud. 2001, 38, 231–237. [Google Scholar] [CrossRef]
- Shakespeare, T. Disability Rights and Wrongs; Routledge: New York, NY, USA, 2006. [Google Scholar]
- Mertens, D.M. Transformative Research and Evaluation, 1st ed.; The Guilford Press: New York, NY, USA, 2008; p. 402. [Google Scholar]
- Mertens, D.M. Transformative Paradigm: Mixed Methods and Social Justice. J. Mix. Methods Res. 2007, 1, 212–225. [Google Scholar] [CrossRef]
- Fassinger, R.; Morrow, S.L. Toward best practices in quantitative, qualitative, and mixed-method research: A social justice perspective. J. Soc. Action Couns. Psychol. 2013, 5, 69–83. [Google Scholar] [CrossRef]
- Lyons, H.Z.; Bike, D.H.; Ojeda, L.; Johnson, A.; Rosales, R.; Flores, L.Y. Qualitative research as social justice practice with culturally diverse populations. J. Soc. Action Couns. Psychol. 2013, 5, 10–25. [Google Scholar] [CrossRef]
- U.S. Census Bureau QuickFacts. Available online: https://www.census.gov/quickfacts/S010219 (accessed on 21 February 2022).
- Charmaz, K. Constructing Grounded Theory, 2nd ed.; SAGE Publications Ltd.: London, UK; Thousand Oaks, CA, USA, 2014; p. 416. [Google Scholar]
- Braun, V.; Clarke, V. Reflecting on reflexive thematic analysis. Qual. Res. Sport Exerc. Health 2019, 11, 589–597. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Andrews, E. Disability as Diversity. Webinar for the Academy of Rehabilitation Psychology Oxford Series; Oxford University Press: New York, NY, USA, 2022. [Google Scholar]
- Vilchinsky, N.; Findler, L.; Werner, S. Attitudes toward people with disabilities: The perspective of attachment theory. Rehabil. Psychol. 2010, 55, 298–306. [Google Scholar] [CrossRef] [PubMed]
- Dunn, D.S. Outsider Privileges Can Lead to Insider Disadvantages: Some Psychosocial Aspects of Ableism. J. Soc. Issues 2019, 75, 665–682. [Google Scholar] [CrossRef] [Green Version]
- Namkung, E.H.; Carr, D. Perceived interpersonal and institutional discrimination among persons with disability in the U.S.: Do patterns differ by age? Soc. Sci. Med. 2019, 239, 112521. [Google Scholar] [CrossRef]
- Ostrove, J.M.; Kornfeld, M.; Ibrahim, M. Actors against Ableism? Qualities of Nondisabled Allies from the Perspective of People with Physical Disabilities. J. Soc. Issues 2019, 75, 924–942. [Google Scholar] [CrossRef] [Green Version]
- Droogendyk, L.; Wright, S.C.; Lubensky, M.; Louis, W.R. Acting in Solidarity: Cross-Group Contact between Disadvantaged Group Members and Advantaged Group Allies. J. Soc. Issues 2016, 72, 315–334. [Google Scholar] [CrossRef] [Green Version]
- Reeve, D. Part of the problem or part of the solution? How far do ‘reasonable adjustments’ guarantee ‘inclusive access for disabled customers’. In Disability, Spaces and Places of Policy Exclusion; Soldatic, K., Morgan, H., Roulstone, A., Eds.; Routledge Advances in Disability Studies; Routledge, Taylor & Francis Group: London, UK, 2014. [Google Scholar]
- Sibley, D. Geographies of Exclusion: Society and Difference in the West, 1st ed.; Routledge: London, UK; Routledge, UK, 1995; p. 224. [Google Scholar]
- Imrie, R. Space, place and policy regimes: The changing contours of disability and citizenship. In Disability, Spaces and Places of Policy Exclusion; Soldatic, K., Morgan, H., Roulstone, A., Eds.; Routledge advances in disability studies; Routledge, Taylor & Francis Group: London, UK, 2014. [Google Scholar]
- Campbell, F. Contours of Ableism: The Production of Disability and Abledness, 1st ed.; Palgrave Macmillan: London, UK, 2009. [Google Scholar]
- Massey, D. Space, Place, and Gender; University of Minnesota Press: Minneapolis, MN, USA, 1994; p. 288. [Google Scholar]
- Reber, L. The cramped and crowded room: The search for a sense of belonging and emotional well-being among temporary low-wage migrant workers. Emot. Space Soc. 2021, 40, 100808. [Google Scholar] [CrossRef]
- Gorman, R. The feminist standpoint and the trouble with “informal learning”: A way forward for Marxist-feminist educational research. In Renewing Dialogues in Marxism and Education; Springer: Berlin/Heidelberg, Germany, 2007; pp. 183–199. [Google Scholar]
- Nario-Redmond, M.R.; Kemerling, A.A.; Silverman, A. Hostile, Benevolent, and Ambivalent Ableism: Contemporary Manifestations. J. Soc. Issues 2019, 75, 726–756. [Google Scholar] [CrossRef] [Green Version]
- Whittle, H.J.; Palar, K.; Ranadive, N.A.; Turan, J.M.; Kushel, M.; Weiser, S.D. “The land of the sick and the land of the healthy”: Disability, bureaucracy, and stigma among people living with poverty and chronic illness in the United States. Soc. Sci. Med. 2017, 190, 181–189. [Google Scholar] [CrossRef] [Green Version]
- Meade, M.A.; Mahmoudi, E.; Lee, S.-Y.D. The intersection of disability and healthcare disparities: A conceptual framework. Disabil. Rehabil. 2015, 37, 632–641. [Google Scholar] [CrossRef] [PubMed]
- Lincoln, Y.S.; Guba, E. Naturalistic Inquiry, 1st ed.; SAGE Publications: Newbury Park, CA, USA, 1985; p. 416. [Google Scholar]
- Fassinger, R.E. Fassinger, Ruth E-Paradigms, praxis, problems, and promise: Grounded theory in counseling psychology research—Sowiport. J. Couns. Psychol. 2005, 52, 156–166. [Google Scholar] [CrossRef]
- Doyle, S. Member Checking With Older Women: A Framework for Negotiating Meaning. Health Care Women Int. 2007, 28, 888–908. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Number of Participants | |
| Participant Characteristics (n = 50) | |
| City of residence | |
| Flint | 23 |
| Detroit | 27 |
| Demographic characteristic | |
| Female/Male | 24/26 |
| Race/Ethnicity | |
| Black | 31 (60%) |
| Hispanic or biracial | 3 (5%) |
| White | 16 (35%) |
| Age range | 23–75 |
| Household income * | |
| <$20,000 | 17 |
| $20,000–29,000 | 13 |
| $30,000–39,000 | 2 |
| $40,000–49,000 | 2 |
| Preferred not to say (not including 7 key informants) | 9 |
| Estimate < $29,000 | 5 |
| Estimate > $30,000 | 4 |
| Data Collection Characteristics | |
| Focus group, in-person (3 conducted) | 18 |
| Interview, in-person | 3 |
| Interview, remote | 29 |
| Follow-up focus group, remote (2 conducted) ** | 9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reber, L.; Kreschmer, J.M.; James, T.G.; Junior, J.D.; DeShong, G.L.; Parker, S.; Meade, M.A. Ableism and Contours of the Attitudinal Environment as Identified by Adults with Long-Term Physical Disabilities: A Qualitative Study. Int. J. Environ. Res. Public Health 2022, 19, 7469. https://doi.org/10.3390/ijerph19127469
Reber L, Kreschmer JM, James TG, Junior JD, DeShong GL, Parker S, Meade MA. Ableism and Contours of the Attitudinal Environment as Identified by Adults with Long-Term Physical Disabilities: A Qualitative Study. International Journal of Environmental Research and Public Health. 2022; 19(12):7469. https://doi.org/10.3390/ijerph19127469
Chicago/Turabian StyleReber, Lisa, Jodi M. Kreschmer, Tyler G. James, Jaime D. Junior, Gina L. DeShong, Shan Parker, and Michelle A. Meade. 2022. "Ableism and Contours of the Attitudinal Environment as Identified by Adults with Long-Term Physical Disabilities: A Qualitative Study" International Journal of Environmental Research and Public Health 19, no. 12: 7469. https://doi.org/10.3390/ijerph19127469
APA StyleReber, L., Kreschmer, J. M., James, T. G., Junior, J. D., DeShong, G. L., Parker, S., & Meade, M. A. (2022). Ableism and Contours of the Attitudinal Environment as Identified by Adults with Long-Term Physical Disabilities: A Qualitative Study. International Journal of Environmental Research and Public Health, 19(12), 7469. https://doi.org/10.3390/ijerph19127469