
Effects of Regular Taekwondo Intervention on Health-Related Physical Fitness, Cardiovascular Disease Risk Factors and Epicardial Adipose Tissue in Elderly Women with Hypertension




Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Approval and Determination of Study Size
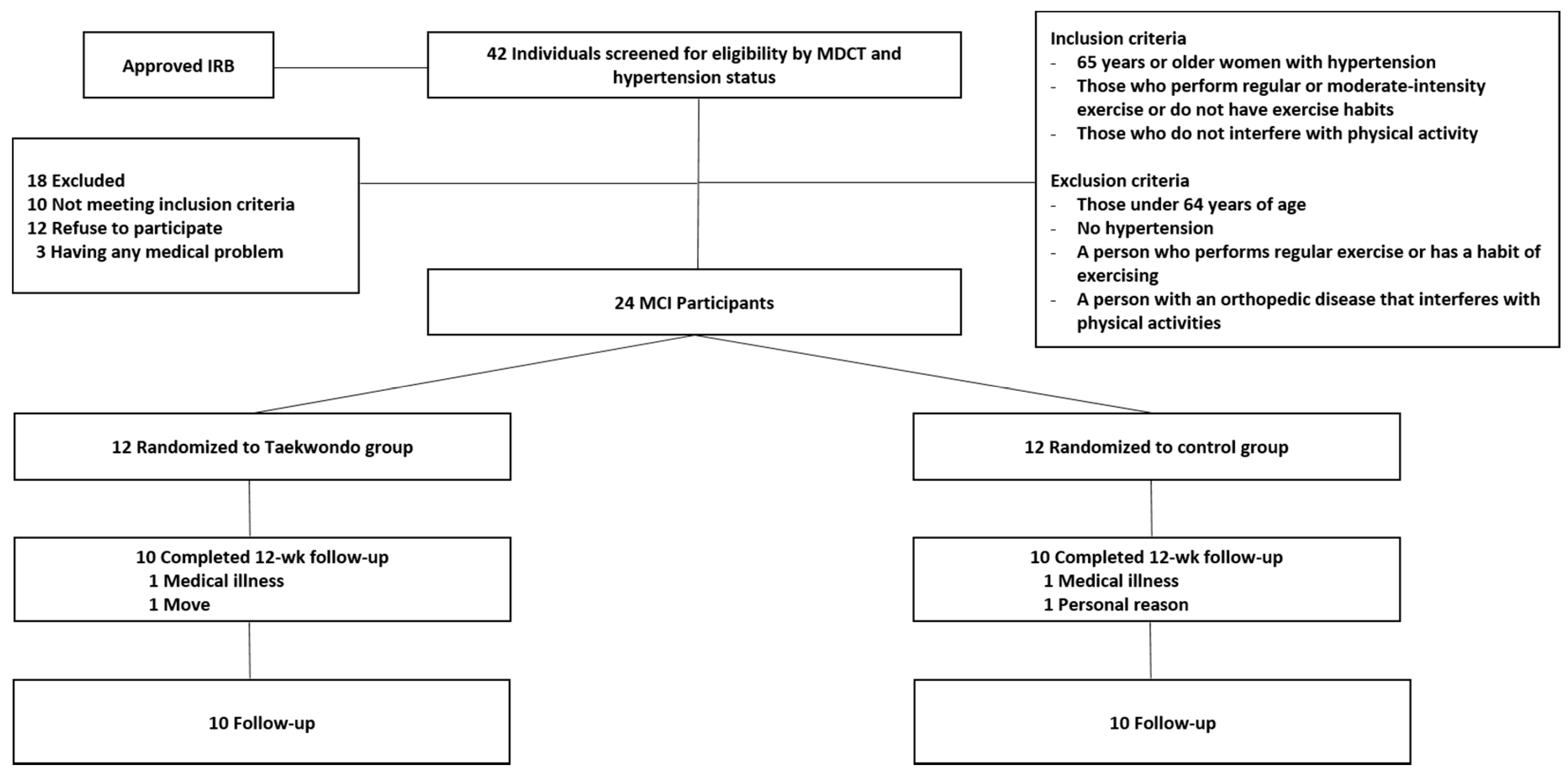
2.2. Participants
2.3. Measurement of Body Composition and BP
2.4. PA and Sedentary Behavior Measurement
2.5. HRPF Measurement
2.6. EAT Thickness Measurement
2.7. TKD Program
2.8. Blood Analysis
2.9. Statistical Analysis
3. Results
3.1. Body Composition and Daily PA and HRPF
3.2. CVD Risk Factor and EAT
3.3. Correlations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hardin, E.A.; Chin, K.M. Selexipag in the treatment of pulmonary arterial hypertension: Design, development, and therapy. Drug Des. Dev. Ther. 2016, 15, 3747–3754. [Google Scholar] [CrossRef]
- American Heart Association. Heart disease and stroke statistics–2015 update: A report from the American Heart Association. Circulation 2015, 131, 434–441. [Google Scholar]
- Statistics Korea. 2018 Elderly Person Statistics; Statistics Korea: Sejong City, Korea, 2018.
- Dam, R.M.T.; Spiegelman, D.; Franco, O.H.; Hu, F.B. Combined impact of lifestyle factors on mortality: Prospective cohort study in US women. BMJ 2008, 337, a1440. [Google Scholar] [CrossRef]
- Jia, G.; Jia, Y.; Sowers, J.R. Contribution of maladaptive adipose tissue expansion to development of cardiovascular disease. Compr. Physiol. 2011, 7, 253–262. [Google Scholar]
- Skarn, S.N.; Eggesbo, H.B.; Flaa, A.; Kjeldsen, S.E.; Rostrup, M.; Brunborg, C.; Reims, H.M.; Aksnes, T.A. Predictors of abdominal adipose tissue compartments: 18-years follow-up of young men with and without family history if diabetes. Eur. J. Intern. Med. 2016, 29, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.W.K.; Chair, S.Y.; Lee, D.T.F.; Leung, D.Y.P.; Sit, J.W.H.; Cheng, H.Y.; Taylor-Piliae, R.E. Tai Chi exercise is more effective than brisk walking in reducing cardiovascular disease risk factors among adults with hypertension: A randomised controlled trial. Int. J. Nurs. Stud. 2018, 88, 44–52. [Google Scholar] [CrossRef]
- Manson, J.E.; Willett, W.C.; Stampfer, M.J.; Colditz, G.A.; Hunter, D.J.; Hankinson, S.E.; Hennekens, C.H.; Speizer, F.E. Body weight and mortality among women. N. Engl. J. Med. 1995, 333, 677–685. [Google Scholar] [CrossRef]
- Albu, J.B.; Kovera, A.J.; Johnson, J.A. Fat distribution and health in obesity. Ann. N. Y. Acad. Sci. 2000, 904, 491–501. [Google Scholar] [CrossRef]
- Wilson, P.W.F.; D’Agostino, R.B.; Sullivan, L.; Parise, H.; Kannel, W.B. Overweight and obesity as determinants of cardiovascular risk: The Framinham experience. Arch. Intern. Med. 2002, 162, 1867–1872. [Google Scholar] [CrossRef]
- Taguchi, R.; Takasu, J.; Itani, Y.; Yamamoto, R.; Yokohama, K.; Watanabe, S.; Masuda, Y. Pericardial fat accumulation in men as a risk factor for coronary artery disease. Atherosclerosis 2001, 157, 203–209. [Google Scholar] [CrossRef]
- Iacobellis, G.; Pistilli, D.; Gucciardo, M.; Leonetti, F.; Miralfi, F.; Brancaccio, G.; Gallo, P.; Di Gioia, C.R.T. Adiponecting expression in human epicardail adipose tissue in vivo is lower in patients with coronary artery disease. Cytokine 2005, 29, 251–255. [Google Scholar]
- Iacobellis, G.; Barbaro, G. The double Role of Epicardial Adipose Tissue as pro-and Anti-inflammatory organ. Horm. Metab. Res. 2008, 40, 442–447. [Google Scholar] [CrossRef]
- Icobellis, G.; Ribaudo, M.C.; Assael, F.; Vecci, E.; Tiberti, C.; Zappaterreno, A.; Di Mario, U.; Leonetti, F. Echocardiographic epicardial adipose tissue is related to anteropometric and clinical parameters of metabolic syndrome: A new indicator of cardiovascular risk. JCEM 2003, 88, 5163–5168. [Google Scholar] [CrossRef]
- Ra, J.S.; Kim, H.S. Comined Influence of Obesity and Metabolic Syncrome on Ischemic Heart Disease in Korean middle aged and older adults. J. Korean Public Health Nurs. 2015, 29, 540–550. [Google Scholar] [CrossRef]
- Hikmet, Y.; Ugur, C.; Tuncay, H.; Ahmet, H.A.; Hamza, S.; Muhammet, D.; Levent, S.; Ergun, B.K.; Kudret, A.; Lale, T.; et al. Increased epicardial fat tissue is a marker of metabolic syndorme in adult patients. Int. J. Cardiol. 2011, 165, 308–313. [Google Scholar]
- Yang, C.; Li, L.; Zha, Y.; Peng, Z. Correlation between epicardial adipose tissue and severity of coronary artery stenosis evulated by 64-MDCT. Clin. Imaging 2016, 40, 477–480. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, N.; Moreno-Villegas, Z.; Gonzalez-Bris, A.; Egido, J.; Lorenzo, O. Regulation of visceral and epicardial adipose tissue for preventing cardiovascular injuries associated to obesity and diabetes. Cardiovasc. Diabetol. 2017, 16, 44. [Google Scholar] [CrossRef]
- Iozzo, P. Myocardial, perivascular, and epicardial fat. Diabetes Care Suppl. 2011, 34, 371–379. [Google Scholar] [CrossRef]
- Mazurek, T.; Zhang, L.; Zalewski, A. Human epicardial adipose tissue is a source of inflammatory mediator. Circulation 2003, 108, 2460–2466. [Google Scholar] [CrossRef] [PubMed]
- Eszter, N.; Adam, L.J.; Bela, M.; Pal, M.H. Clinical importance of epicardial adipose tissue. Arch. Med. Sci. 2017, 13, 864–874. [Google Scholar]
- Ferrari, A.U.; Radaelli, A.; Centola, M. Physiology of aging. Invited review: Aging and the cardiovascular system. J. Appl. Physiol. 2003, 95, 2591–2597. [Google Scholar] [CrossRef] [PubMed]
- Larsen, B.A.; Allison, M.A.; Kang, E.; Saad, S.; Laughlin, G.A.; Araneta, M.R.G.; Barrett-Connor, E.; Wassel, C.L. Associations of Physical Activity and Sedentary Behavior with Regional Fat Deposition. Med. Sci. Sports Exerc. 2014, 46, 520–528. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.K.; Tanaka, K.; Kim, M.J.; Matsuo, T.; Tomita, T.; Ohkubo, H.; Maeda, S.; Ajisaka, R. Epicardial fat tissue: Relationship with cardiorespiratory fitness in men. Med. Sci. Sports Exerc. 2010, 42, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Eijsvogels, T.M.H.; Molossi, S.; Lee, D.J.; Emery, M.S.; Thompson, P.D. Exercise at the extremes: The amount of exercise to reduce cardiovascular events. J. Am. Coll. Cardiol. 2016, 67, 316–329. [Google Scholar] [CrossRef]
- American Heart Association. Cardiovascular Disease & Diabetes. Updated 2018. Available online: https://www.heart.org/en/health-topics/diabetes/why-diabetes-matters/cardiovascular-disease--diabetes (accessed on 12 April 2019).
- Palmefors, H.; DuttaRoy, S.; Rundqvist, B.; Borjesson, M. The effect of physical activity or exercise on key biomarkers in atherosclerosis—A systematic review. Atherosclerosis 2014, 235, 150–161. [Google Scholar] [CrossRef]
- Park, S.H.; So, Y.S.; Kim, M.J.; Kim, D.H.; Yoon, M.Y.; Kim, Y.J. Effect of Swimming Exercise on Epicardial Fat and Cardiovascular Risk Factor in Obese Adult Men. J. Coach. Dev. 2015, 17, 109–117. [Google Scholar]
- Kim, M.K.; Tomita, T.; Kim, M.J.; Sasai, H.; Maeda, S.; Tanaka, K. Aerobic exercise training reducese picardial fat in obese men. J. Appl. Physiol. 2009, 106, 5–11. [Google Scholar] [CrossRef]
- Roh, H.T.; Cho, S.Y.; So, W.Y. Taekwondo Training Improves Mood and Sociability in Children from Multicultural Families in South Korea: A Randomized Controlled Pilot Study. Int. J. Environ. Res. Public Health 2018, 15, 757. [Google Scholar] [CrossRef]
- Bridge, C.A.; Da Silva Santos, J.F.; Chaabène, H.; Franchini, E. Physical and physiological profiles of taekwondo athletes. Sports Med. 2014, 44, 713–733. [Google Scholar] [CrossRef]
- Lee, S.H.; Park, S.K.; Hong, G.R. The effect of taekwondo training on physical fitness and the allergic response factor of hypersensitive obese children. Arch. Budo 2018, 14, 113–121. [Google Scholar]
- Bridge, C.A.; Jones, M.A.; Hitchen, P.; Sanchez, X. Heart rate responses to Taekwondo training in experienced practitioners. J. Strength Cond. Res. 2007, 21, 718–723. [Google Scholar] [PubMed]
- Lee, Y.H.; Kim, K.T. Tai Chi as a Fall Prevention Intervention: An In-depth Literature Review of Randomized Controlled Trials and Suggestion to Taekwondo. Off. J. Korean Acad. Kinesiol. 2013, 15, 1–11. [Google Scholar]
- Jeong, M.K.; Jung, H.H. Effects of Silver Taekwondo Program on Self-reliance Physical Fitness, Depressive Symptoms and Diabetes Factors in Obese Elderly Women with Type 2 Diabetes. Korea J. Sports Sci. 2020, 29, 859–870. [Google Scholar] [CrossRef]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, 7th ed.; Lippincott Williams and Wilkins: Philadelphia, PA, USA, 2006. [Google Scholar]
- Gobel, F.L.; Norstrom, L.A.; Nelson, R.R.; Jorgensen, C.R.; Wang, Y. The rate-pressure product as an index of myocardial oxygen consumption during exercise in patients with angina pectoris. Circulation 1978, 57, 549–556. [Google Scholar] [CrossRef]
- Park, H.; Park, J.H.; Na, H.R.; Shimada, H.; Kim, G.M.; Jung, M.K.; Kim, W.K.; Park, K.W. Combined Intervention of Physical Activity, Aerobic Exercise, and Cognitive Exercise Intervention to Prevent Cognitive Decline for Patients with Mild Cognitive Impairment: A Randomized Controlled Clinical Study. J. Clin. Med. 2019, 8, 940. [Google Scholar] [CrossRef]
- Jeong, M.K.; Lee, S.H.; Ryu, J.K.; Kim, Y.H.; Kim, E.H.; Hong, G.R.; Park, J.H.; Baek, S.H.; Park, S.K.; Jung, H.H. Effects of long-term multi-task exercise program on blood pressure, physical function and cognitive function in mild cognitive impairment elderly women with hypertension. Arch Budo 2019, 15, 93–102. [Google Scholar]
- Park, H.; Togo, F.; Watanabe, E.; Yasunaga, A.; Park, S.; Shephard, R.J.; Aoyagi, Y. Relationship of bone health to yearlong physical activity in older Japanese adults: Cross-sectional data from the Nakanojo Study. Osteoporos. Int. 2007, 18, 285–293. [Google Scholar] [CrossRef]
- Park, H.; Park, S.; Shephard, R.J.; Aoyagi, Y. Yearlong physical activity and sarcopenia in older adults: The Nakanojo Study. Eur. J. Appl. Physiol. 2010, 109, 953–961. [Google Scholar] [CrossRef]
- Park, J.H.; Park, S.K.; Lee, D.M.; Jeong, M.K.; Kim, D.H.; Lee, T.H.; Jeon, S.H.; Park, J.K.; Kim, E.H.; Min, S.K.; et al. The Relationship between Sedentary Behavior and Cystatin C, Blood Pressure in Obese Elderly Women. Korea J. Sports Sci. 2014, 23, 1191–1199. [Google Scholar]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; Lippincott Williams & Wilkins: Baltimore, MD, USA, 2018. [Google Scholar]
- Gaber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.M.; Nieman, D.C.; Swain, D.P.; ACSM. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef]
- Pescatello, L.S.; MacDonald, H.V.; Ash, G.I.; Lamberti, L.M.; Farquhar, W.B.; Arena, R.; Johnson, B.T. Assessing the Existing Professional Exercise Recommendations for Hypertension: A Review and Recommendations for Future Research Priorities. Mayo Clin. Proc. 2015, 90, 801–812. [Google Scholar] [CrossRef] [PubMed]
- Eckel, R.H.; Jakicic, J.M.; Ard, J.D.; De Sesus, J.M.; Miller, N.H.; Hubbard, V.S.; Lee, I.M.; Lichtenstein, A.H.; Loria, C.M.; Millen, B.E.; et al. 2013 AHA/ACC guideline on lifestyle management to reduce cardiovascular risk: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2014, 63, 2960–2984. [Google Scholar] [CrossRef] [PubMed]
- Jeong, M.K.; Ryu, J.K.; Jung, H.H.; Kim, H.W.; Park, S.K. Effects of Taekwondo aerobic and Combined Exercise Program on Health-related Physical Fitness and Physical Activity and Depression Scale in Menopausal Obesity Women. Korea J. Sports Sci. 2018, 27, 1199–1210. [Google Scholar] [CrossRef]
- Kim, E.H.; Park, S.K.; Hong, G.R. Effects of TTM and Longevity Exercise Program on Health-related Physical Fitness, Blood Pressure and IMT in Elderly Women with Hypertension. Korean Soc. Sports Leis. Stud. 2019, 75, 465–475. [Google Scholar]
- Jeong, M.K.; Park, H.T.; Park, S.K.; Kim, E.H.; Kwon, Y.C. Effects of Long-term Taekwondo Aerobic and Thera-band Training on Self-reliance Physcal Fitness, and hs-CRP concentration in Obese Elderly Women. Korea J. Sports Sci. 2015, 24, 1349–1358. [Google Scholar]
- Toskovic, N.N.; Blessing, D.; Williford, H.N. The effect of experience and gender on cardiovascular metabolic responses with dynamic Tae Kwon Do exercise. J. Strength. Cond. Res. 2002, 16, 278–285. [Google Scholar] [PubMed]
- Stewart, K.J.; Bacher, A.C.; Turner, K.L.; Fleg, J.L.; Hees, P.S.; Shapiro, E.P.; Tayback, M.; Ouyang, P. Effect of exercise on blood pressure in older persons: A randomized controlled trial. Archives Intern. Med. 2005, 165, 756–762. [Google Scholar] [CrossRef]
- Kim, E.H.; Park, S.K.; Kim, E.Y.; Hong, G.R. Effects of Combined Exercise Program on Glucose, Cardiovascular Disease Risk Factors and Health-Related Quality of Life in Elderly Women with Type II Diabetes. Korea J. Sports Sci. 2013, 22, 1133–1145. [Google Scholar]
- Ministry of Culture, Sports and Tourism. 2017 Korean National Health Status Survey; Ministry of Culture, Sports and Tourism: Sejong City, Korea, 2017.
- Bohannon, R.W.; Bear-Lehman, J.; Derosiers, J.; Massy-westropp, N.; Mathiowets, V. Average grip strength: A meta-analysis of data obtained with a Jamar Dynamometer from individuals 75 years or more of age. J. Geriatr. Phys. Ther. 2015, 30, 28–31. [Google Scholar] [CrossRef]
- Rijk, J.M.; Roos, P.R.; Deckx, L.; Van den Akker, M.; Buntinx, F. Prognostic value of handgrip strength in people aged 60 years and older: A systematic review and meta-analysis. Med. Index. 2016, 16, 5–20. [Google Scholar] [CrossRef]
- Rogers, M.A.; Evans, W.J. Changes on skeletal muscle with aging. effects of exercise training. Exerc. Sports Sci. Rev. 1993, 21, 65–102. [Google Scholar] [CrossRef]
- Pescatello, L.S.; Vanheest, J.L. Physical activity mediates a healthier body weight in the presence of obesity. Br. J. Sports Med. 2000, 34, 86–93. [Google Scholar] [CrossRef]
- Keith, M.D.; Daichi, S. Physical Activity and the Prevention of Hypertension. Curr. Hypertens. Rep. 2013, 15, 659–668. [Google Scholar]
- Cheng, H.M.; Chiang, C.E.; Chen, C.H. The Novelty of the 2015 Guidelines of the Taiwan Society of Cardiology and the Taiwan Hypertension Society for the Management of Hypertension. Pulse 2015, 3, 29–34. [Google Scholar] [CrossRef]
- Sironi, A.M.; Gastaldelli, A.; Mari, A.; Ciociaro, D.; Postano, V.; Buzziggoli, E.; Ghione, S.; Turchi, S.; Lombardi, M.; Ferrannini, E. Visceral fat in hypertension: Influence on insulin resistance and beta-cell function. Hypertension 2004, 44, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Adriana, L.S.; Luciana, M.L.; Eliane, A.C.; Renato, P.V.; Wellongton, S.; Thaos, C.Z.; Leon, A.D. Blood pressure in hypertensive women after aerobics and hydrogymnastics sessions. Nutr. Hosp. 2015, 32, 823–828. [Google Scholar]
- Stanley, S.F.; Nathan, D.W. Hypertension and Cardiovascular Disease: Contributions of the Framingham Heart Study. Glob. Heart 2013, 8, 49–57. [Google Scholar]
- Korea Centers for Disease Control and Prevention. The Seventh Korea National Health and Nutrition Examination Survey (KNHANES VII-2); Korea Centers for Disease Control and Prevention: Cheongwon-gun, Korea, 2017.
- Manuel, M.; Paolo, D.R.; Maria, R.P.; Francesco, B.; Giovanni, M.V. New evidences about the strict relationship between the epicardial fat and the aerobic exercise. IJC Metab. Endocr. 2015, 6, 55–58. [Google Scholar]
- Kalyana, C.B.; Arun, G.M.; Padma, K.; Krishnananda, N.; Vasudeva, G.; Vidya, N. Effect of aerobic exercise on echocardiographic epicardial adipose tissue thickness in overweight individuals. Diabetes Metab. Syndr. Obes. 2018, 11, 303–312. [Google Scholar]
- Talman, A.H.; Psaltis, P.J.; Cameron, J.D.; Meredith, I.T.; Senevirantne, S.K.; Wong, D.T.L. Epicardial adipose tissue: Far more than a fat depot. Cardiovasc. Diagn. Ther. 2014, 4, 416–429. [Google Scholar]
- Iacobellis, G. Local and systemic effects of the multifaceted epicardial adipose tissue depot. Nat. Rev. Endocrinol. 2015, 11, 363–371. [Google Scholar] [CrossRef] [PubMed]
- Gunasekar, P.; Swier, V.J.; Fleegel, J.P.; Boosani, C.S.; Radwan, M.M.; Agrawal, D.K. Vitamin D and Macrophage Polarization in Epicardial Adipose Tissue of Atherosclerotic Swine. PLoS ONE 2018, 13, e0199411. [Google Scholar] [CrossRef] [PubMed]
- Libby, P.; Ridker, P.M.; Maseri, A. Inflammation and atherosclerosis. Circulation 2002, 105, 1135–1143. [Google Scholar] [CrossRef]
- Zhang, H.; Zhang, C. Vasoprotection by dietary supplements and exercise: Role of TNFalpha signaling. Exp. Diabetes. Res. 2012, 2012, 972679. [Google Scholar]
- Sacks, H.S.; Fain, J.N. Human epicardial adipose tissue: A review. Am. Heart J. 2007, 153, 907–917. [Google Scholar] [CrossRef]
- Osborn, L.; Hession, C.; Tizard, R.; Vassallo, C.; Luhowskyj, S.; Chi-Rosso, G.; Lobb, R. Direct expression cloning of vascular cell adhesion molecule 1, a cytokine-induced endothelial protein that binds to lymphocytes. Cell 1989, 59, 1203–1211. [Google Scholar] [CrossRef]
- Gearing, A.J.H.; Hemingway, I.; Pigoit, R.; Hughes, J.; Rees, A.J.; Cashman, S.J. Soluble forms of vascular adhesion molecules, E-selectin, ICAM-1, and VCAM-1: Pathological significance. Ann. N. Y. Acad. Sci. 1992, 667, 324–331. [Google Scholar] [CrossRef] [PubMed]
- Dimitriadis, G.K.; Kaur, J.; Adya, R.; Miras, A.D.; Mattu, H.S.; Hattersley, J.G.; Kaltsas, G.; Tan, B.K.; Randeva, H.S. Chemerin induces endothelial cell inflammation: Activation of nuclear factor-kappa beta and monocyte-endothelial adhesion. Oncotarget 2018, 9, 16678–16690. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Taekwondo (n = 10) | Control (n = 10) | p-Value |
|---|---|---|---|
| Socio-demographic | |||
| Age (years) | 72.90 ± 5.84 | 71.90 ± 3.11 | 0.057 |
| Hypertension duration (years) | 11.90 ± 4.33 | 11.30 ± 4.62 | 0.676 |
| Hypertension drug duration (years) | 10.80 ± 3.79 | 10.40 ± 4.55 | 0.396 |
| Job, n (%) | 0 (0%) | 0 (0%) | 1.000 |
| Smoking (yes), n (%) | 0 (0%) | 0 (0%) | 1.000 |
| Alcohol consumption (yes), n (%) | 0 (0%) | 0 (0%) | 1.000 |
| Physical Characteristics and Blood pressure | |||
| Body height (m) | 1.51 ± 0.03 | 1.50 ± 0.05 | 0.491 |
| Body weight (kg) | 57.48 ± 5.69 | 56.91 ± 2.97 | 0.063 |
| Body mass index (kg/m2) | 25.32 ± 2.54 | 25.30 ± 1.68 | 0.176 |
| Lean body mass (kg) | 32.81 ± 3.13 | 34.71 ± 4.34 | 0.591 |
| Percent body fat (%) | 42.82 ± 3.81 | 42.57 ± 3.66 | 0.886 |
| Waist circumference (cm) | 92.28 ± 6.61 | 91.96 ± 4.29 | 0.231 |
| Hip circumference (cm) | 100.72 ± 5.42 | 99.57 ± 3.40 | 0.283 |
| Waist hip ratio | 0.92 ± 0.03 | 0.92 ± 0.05 | 0.204 |
| Systolic blood pressure (mmHg) | 150.90 ± 7.99 | 148.20 ± 7.10 | 0.815 |
| Diastolic blood pressure (mmHg) | 92.20 ± 6.32 | 91.20 ± 6.51 | 0.982 |
| Items | Contents | Time (min) | ||
|---|---|---|---|---|
| Warm-Up | Shuttle Walking, Sitting Stretching | 10 | ||
| The content of Taekwondo training intervention | 1~4 week | Stance—Close, Parallel, Riding, Forward, Forward inflection (5 times) Fist punching—Trunk, Face opposite, Underneath (Both 15 times) Blocking—Underneath, Trunk, Face opposite (Both 15 times) Kick—Front, Roundhouse, Downward, Side (Both 15 times) Taekwonrobic (Seperated action 2 times, With rhythm 2 times) (20 min) Step box—Basic step, Knee up, Kick, Leg curl, Tap (20 min) | HRR; 40~59% | 70 |
| 5~12 week | Stance—Close, Parallel, Riding, Forward, Forward inflection (5 times) Fist punching—Trunk, Face opposite, Underneath, Side (Both 15 times) Blocking—Underneath, Trunk, Face opposite (Both 15 times) Kick—Front, Roundhouse, Downward, Side (Both 15 times) Taekwonrobic (Seperated action 2 times, With rhythm 2 time) (20 min) Step box—Basic step, Knee up, Kick, Leg curl, Tap (20 min) | HRR; 60~75% | ||
| Cool-down | Shuttle walking, Standing stretching | 10 | ||
| Jeong et al. (2018, modified program) | ||||
| Variable | Group | Baseline | 12 Weeks | % Diff | p-Value (Interaction) |
|---|---|---|---|---|---|
| Body weight (kg) | Taekwondo | 57.48 ± 5.69 | 56.53 ± 5.58 | −1.65 *** | 0.001 |
| Control | 56.91 ± 2.97 | 57.21 ± 2.95 | 0.53 | ||
| Body mass index (kg/m2) | Taekwondo | 25.32 ± 2.54 | 24.91 ± 2.57 | −1.63 *** | 0.001 |
| Control | 25.30 ± 1.68 | 25.44 ± 1.67 | 0.53 | ||
| Lean body mass (kg) | Taekwondo | 32.81 ± 3.13 | 34.60 ± 2.94 | 5.46 *** | 0.023 |
| Control | 34.71 ± 4.34 | 34.21 ± 4.05 | −1.44 | ||
| Percent body fat (%) | Taekwondo | 42.82 ± 3.81 | 39.97 ± 4.15 | −6.66 *** | 0.000 |
| Control | 42.57 ± 3.66 | 43.91 ± 3.44 | 3.14 | ||
| Waist circumference (cm) | Taekwondo | 92.28 ± 6.61 | 88.36 ± 6.36 | −4.25 *** | 0.000 |
| Control | 91.96 ± 4.29 | 93.38 ± 4.68 | 1.54 * | ||
| Hip circumference (cm) | Taekwondo | 100.72 ± 5.42 | 97.19 ± 5.31 | −3.50 *** | 0.000 |
| Control | 99.57 ± 3.40 | 100.26 ± 2.98 | 0.69* | ||
| Waist hip ratio | Taekwondo | 0.92 ± 0.03 | 0.91 ± 0.02 | −0.78 | 0.080 |
| Control | 0.92 ± 0.05 | 0.93 ± 0.05 | 0.82 | ||
| Moderate to vigorous physical activity (min/day) | Taekwondo | 11.20 ± 8.39 | 39.90 ± 10.21 | 256.25 *** | 0.000 |
| Control | 12.90 ± 9.84 | 12.60 ± 8.37 | −2.33 | ||
| Step count (steps/day) | Taekwondo | 3739.90 ± 1220.41 | 9125.30 ± 2367.07 | 144.00 *** | 0.000 |
| Control | 3361.60 ± 1460.99 | 3277.00 ± 1418.76 | −2.52 | ||
| Sedentary behavior (min/day) | Taekwondo | 1428.80 ± 8.39 | 1100.10 ± 10.21 | −23.01 *** | 0.000 |
| Control | 1427.10 ± 9.84 | 1427.40 ± 8.37 | 0.02 | ||
| Hand grip strength (kg) (dominant) | Taekwondo | 20.93 ± 3.67 | 23.72 ± 3.94 | 13.33 * | 0.014 |
| Control | 21.68 ± 3.37 | 20.25 ± 3.99 | −6.60 | ||
| Repeated chair stand (frequency) | Taekwondo | 8.80 ± 1.97 | 7.34 ± 1.02 | −16.57 ** | 0.003 |
| Control | 8.89 ± 1.43 | 9.23 ± 1.46 | 3.85 | ||
| Trunk flexion in sitting position (cm) | Taekwondo | 14.45 ± 6.02 | 17.65 ± 5.69 | 22.15 *** | 0.003 |
| Control | 12.78 ± 6.76 | 13.55 ± 6.63 | 6.03 | ||
| 2 min walking (frequency) | Taekwondo | 108.40 ± 10.62 | 118.60 ± 11.60 | 10.20 *** | 0.003 |
| Control | 110.10 ± 19.99 | 101.90 ± 24.70 | −7.45 |
| Variable | Group | Baseline | 12 Weeks | % Diff | p-Value (Interaction) |
|---|---|---|---|---|---|
| Total cholesterol (mg/dL) | Taekwondo | 232.10 ± 37.45 | 203.20 ± 25.44 | −12.45 *** | 0.002 |
| Control | 231.60 ± 29.28 | 232.30 ± 27.85 | 0.30 | ||
| Triglyceride (mg/dL) | Taekwondo | 171.10 ± 16.50 | 154.90 ± 15.72 | −9.47 ** | 0.008 |
| Control | 170.20 ± 18.19 | 169.50 ± 20.45 | −0.41 | ||
| Low density lipoprotein cholesterol (mg/dL) | Taekwondo | 119.30 ± 22.93 | 100.50 ± 18.04 | −15.76 ** | 0.000 |
| Control | 118.50 ± 13.11 | 121.50 ± 12.39 | 8.01 | ||
| High density lipoprotein cholesterol (mg/dL) | Taekwondo | 49.40 ± 7.66 | 59.50 ± 9.00 | 20.45 *** | 0.001 |
| Control | 50.50 ± 8.89 | 49.50 ± 9.07 | −1.98 | ||
| Monocyte chemotactic protein-1 (pg/mL) | Taekwondo | 447.59 ± 52.64 | 407.30 ± 67.12 | −9.00 * | 0.009 |
| Control | 454.87 ± 69.89 | 474.79 ± 82.54 | 4.38 | ||
| Soluble vascular cell adhesion molecule-1 (ng/mL) | Taekwondo | 802.61 ± 62.44 | 739.02 ± 85.16 | −7.90 *** | 0.009 |
| Control | 837.37 ± 105.90 | 855.72 ± 111.33 | 2.19 | ||
| Soluble intercelluar cell adhesion molecule-1 (ng/mL) | Taekwondo | 210.02 ± 73.96 | 189.16 ± 62.39 | −9.93 | 0.181 |
| Control | 211.71 ± 68.96 | 254.99 ± 62.26 | 20.44 | ||
| Soluble E-selectin (ng/mL) | Taekwondo | 49.76 ± 18.71 | 40.79 ± 15.90 | −18.02 ** | 0.018 |
| Control | 48.24 ± 14.10 | 48.50 ± 15.23 | 0.56 | ||
| Interukin-1β (pg/mL) | Taekwondo | 0.16 ± 0.04 | 0.12 ± 0.04 | −21.02 ** | 0.001 |
| Control | 0.14 ± 0.02 | 0.16 ± 0.02 | 11.35 | ||
| Tumor necrosis factor-α (pg/mL) | Taekwondo | 2.30 ± 1.08 | 1.34 ± 0.58 | −48.64 * | 0.042 |
| Control | 2.25 ± 1.60 | 2.66 ± 1.71 | 18.12 | ||
| High-sensitivity C-reactive protein (mg/L) | Taekwondo | 0.81 ± 0.69 | 0.63 ± 0.32 | −21.05 | 0.069 |
| Control | 0.79 ± 0.72 | 1.41 ± 0.73 | 43.92 ** | ||
| Pulse pressure (mmHg) | Taekwondo | 58.70 ± 3.77 | 61.00 ± 12.42 | 3.92 | 0.664 |
| Control | 57.00 ± 3.50 | 57.50 ± 4.70 | 0.88 | ||
| Mean arterial pressure (mmHg) | Taekwondo | 111.77 ± 6.69 | 96.23 ± 10.96 | −13.90 ** | 0.000 |
| Control | 110.20 ± 6.51 | 112.47 ± 4.44 | 2.06 | ||
| MVO2 rest (mmHg × beats/min × 10−3) | Taekwondo | 11.52 ± 0.83 | 10.45 ± 1.10 | −9.28 * | 0.002 |
| Control | 11.31 ± 0.66 | 11.52 ± 0.73 | 1.82 | ||
| Systolic blood pressure (mmHg) | Taekwondo | 150.90 ± 7.99 | 136.90 ± 12.46 | −9.28 ** | 0.002 |
| Control | 148.20 ± 7.10 | 150.80 ± 5.80 | 1.75 ** | ||
| Diastolic blood pressure (mmHg) | Taekwondo | 92.20 ± 6.32 | 75.90 ± 12.40 | −17.68 ** | 0.000 |
| Control | 91.20 ± 6.51 | 93.30 ± 4.50 | 2.30 | ||
| Epicardial adipose tissue (mm2) | Taekwondo | 1995.20 ± 911.79 | 1890.50 ± 893.16 | −5.25 ** | 0.041 |
| Control | 1541.80 ± 367.67 | 1609.30 ± 438.39 | 4.38 |
| Variable | Epicardial Adipose Tissue (mm2) |
|---|---|
| Lean body mass (kg) | −0.453 * |
| Sedentary time (min/day) | 0.459 * |
| Triglyceride (mg/dL) | 0.493 * |
| Monocyte chemotactic protein-1 (pg/mL) | 0.524 * |
| Interukin-1β (pg/mL) | 0.530 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.H.; Jeong, M.K.; Park, H.; Park, S.K. Effects of Regular Taekwondo Intervention on Health-Related Physical Fitness, Cardiovascular Disease Risk Factors and Epicardial Adipose Tissue in Elderly Women with Hypertension. Int. J. Environ. Res. Public Health 2021, 18, 2935. https://doi.org/10.3390/ijerph18062935
Kim YH, Jeong MK, Park H, Park SK. Effects of Regular Taekwondo Intervention on Health-Related Physical Fitness, Cardiovascular Disease Risk Factors and Epicardial Adipose Tissue in Elderly Women with Hypertension. International Journal of Environmental Research and Public Health. 2021; 18(6):2935. https://doi.org/10.3390/ijerph18062935
Chicago/Turabian StyleKim, Yun Hwan, Min Ki Jeong, Hyuntae Park, and Sang Kab Park. 2021. "Effects of Regular Taekwondo Intervention on Health-Related Physical Fitness, Cardiovascular Disease Risk Factors and Epicardial Adipose Tissue in Elderly Women with Hypertension" International Journal of Environmental Research and Public Health 18, no. 6: 2935. https://doi.org/10.3390/ijerph18062935
APA StyleKim, Y. H., Jeong, M. K., Park, H., & Park, S. K. (2021). Effects of Regular Taekwondo Intervention on Health-Related Physical Fitness, Cardiovascular Disease Risk Factors and Epicardial Adipose Tissue in Elderly Women with Hypertension. International Journal of Environmental Research and Public Health, 18(6), 2935. https://doi.org/10.3390/ijerph18062935