
Effects of HIIT and MIIT Suspension Training Programs on Sleep Quality and Fatigue in Older Adults: Randomized Controlled Clinical Trial

 ,
,  ,
, 
 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
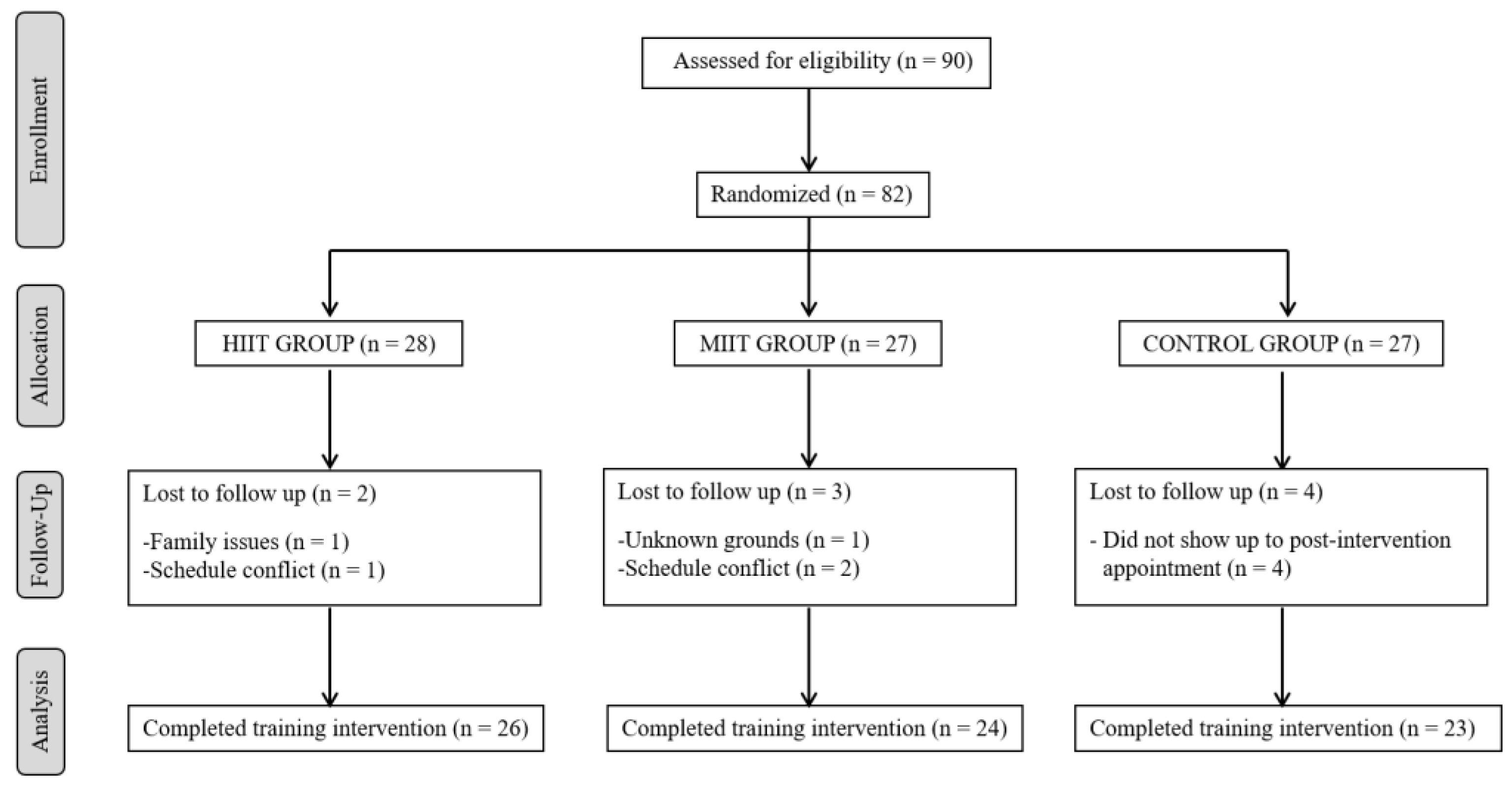
2.1. Study Design and Participants
2.2. Sample Size Calculation
2.3. Allocation to Intervention
2.4. Procedures
2.4.1. Sleep Quality
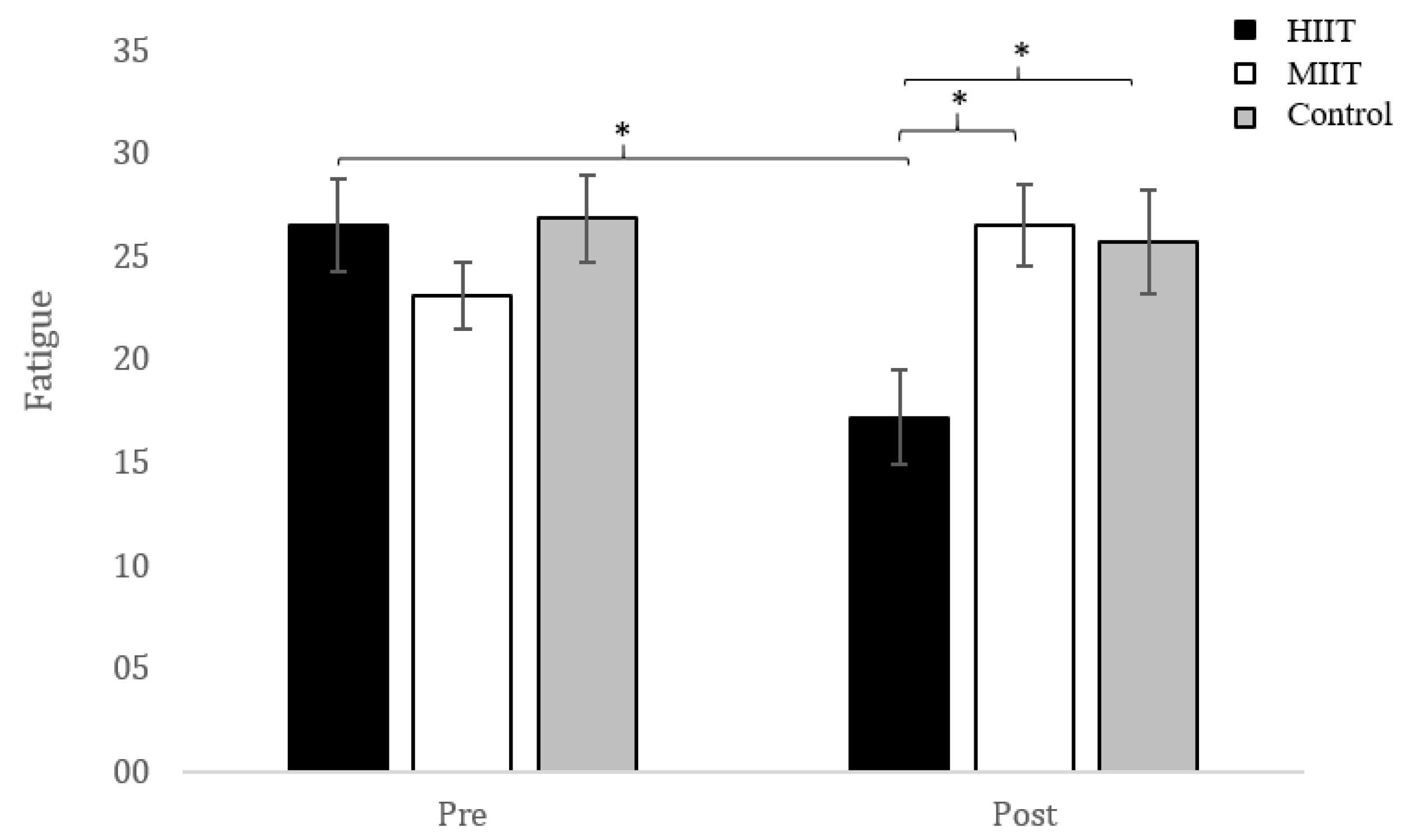
2.4.2. Fatigue
2.5. Training Programs
2.6. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Blake, A.J.; Morgan, K.; Bendall, M.J.; Dallosso, H.; Ebrahim, S.B.; Arie, T.H.; Fentem, P.H.; Bassey, E.J. Falls by elderly people at home: Prevalence and associated factors. Age Ageing 1988, 17, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Navarro-Flores, E.; Vallejo, R.B.; Losa-Iglesias, M.E.; Palomo-López, P.; Calvo-Lobo, C.; López-López, D.; Martínez-Jiménez, E.M.; Romero-Morales, C. Reliability, validity, and sensitivity of Edmonton Frail Scale (EFS) in older adults with foot disorders. Aging 2020, 10, 12. [Google Scholar] [CrossRef] [PubMed]
- Navarro-Flores, E.; Romero-Morales, C.; de Bengoa-Vallejo, R.B.; Rodríguez-Sanz, D.; Palomo-López, P.; López-López, D.; Losa-Iglesias, M.E.; Calvo-Lobo, C. Sex differences in frail older adults with foot pain in a spanish population: An observational study. Int. J. Environ. Res. Public Health 2020, 17, 6141. [Google Scholar] [CrossRef] [PubMed]
- Xiong, J.; Ma, T.; Lian, Z.; de Dear, R. Perceptual and physiological responses of elderly subjects to moderate temperatures. Build. Environ. 2019, 156, 117–122. [Google Scholar] [CrossRef]
- Foley, D.J.; Monjan, A.A.; Brown, S.L.; Simonsick, E.M.; Wallace, R.B.; Blazer, D.G. Sleep complaints among elderly persons: An epidemiologic study of three communities. Sleep 1995, 18, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Mazzotti, D.R.; Guindalini, C.; Moraes, W.A.; Andersen, M.L.; Cendoroglo, M.S.; Ramos, L.R.; Tufik, S. Human longevity is associated with regular sleep patterns, maintenance of slow wave sleep, and favorable lipid profile. Front. Aging Neurosci. 2014, 6, 134. [Google Scholar] [CrossRef]
- Sagayadevan, V.; Abdin, E.; Binte Shafie, S.; Jeyagurunathan, A.; Sambasivam, R.; Zhang, Y.; Picco, L.; Vaingankar, J.; Chong, S.A.; Subramaniam, M. Prevalence and correlates of sleep problems among elderly Singaporeans. Psychogeriatrics 2017, 17, 43–51. [Google Scholar] [CrossRef]
- Luo, J.; Zhu, G.; Zhao, Q.; Guo, Q.; Meng, H.; Hong, Z.; Ding, D. Prevalence and risk factors of poor sleep quality among Chinese elderly in an urban community: Results from the Shanghai aging study. PLoS ONE 2013, 8, e81261. [Google Scholar] [CrossRef]
- Chaput, J.P.; Dutil, C.; Sampasa-Kanyinga, H. Sleeping hours: What is the ideal number and how does age impact this? Nat. Sci. Sleep 2018, 10, 421–430. [Google Scholar] [CrossRef]
- Ohayon, M.M.; Carskadon, M.A.; Guilleminault, C.; Vitiello, M.V. Meta-analysis of quantitative sleep parameters from childhood to old age in healthy individuals: Developing normative sleep values across the human lifespan. Sleep 2004, 27, 1255–1273. [Google Scholar] [CrossRef]
- Kay, D.B.; Dzierzewski, J.M. Sleep in the Context of Healthy Aging and Psychiatric Syndromes. Sleep Med. Clin. 2015, 10, 11–15. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Vitiello, M.V.; Gooneratne, N.S. Sleep in Normal Aging. Sleep Med. Clin. 2018, 13, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Stone, K.L.; Xiao, Q. Impact of Poor Sleep on Physical and Mental Health in Older Women. Sleep Med. Clin. 2018, 13, 457–465. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Q.; Arem, H.; Moore, S.C.; Hollenbeck, A.R.; Matthews, C.E. A large prospective investigation of sleep duration, weight change, and obesity in the NIH-AARP Diet and Health Study cohort. Am. J. Epidemiol. 2013, 178, 1600–1610. [Google Scholar] [CrossRef] [PubMed]
- Schlesinger, A.; Redfern, M.S.; Dahl, R.E.; Jennings, J.R. Postural control, attention and sleep deprivation. Neuroreport 1998, 9, 49–52. [Google Scholar] [CrossRef]
- Thichumpa, W.; Howteerakul, N.; Suwannapong, N.; Tantrakul, V. Sleep quality and associated factors among the elderly living in rural Chiang Rai, northern Thailand. Epidemiol. Health 2018, 40, e2018018. [Google Scholar] [CrossRef]
- Stone, K.L.; Ancoli-Israel, S.; Blackwell, T.; Ensrud, K.E.; Cauley, J.A.; Redline, S.; Hillier, T.A.; Schneider, J.; Claman, D.; Cummings, S.R. Actigraphy-measured sleep characteristics and risk of falls in older women. Arch. Intern. Med. 2008, 168, 1768–1775. [Google Scholar]
- Gu, D.; Sautter, J.; Pipkin, R.; Zeng, Y. Sociodemographic and health correlates of sleep quality and duration among very old Chinese. Sleep 2010, 33, 601–610. [Google Scholar] [CrossRef]
- Neikrug, A.B.; Ancoli-Israel, S. Sleep disorders in the older adult—A mini-review. Gerontology 2010, 56, 181–189. [Google Scholar] [CrossRef]
- Fortier-Brochu, E.; Beaulieu-Bonneau, S.; Ivers, H.; Morin, C.M. Relations between sleep, fatigue, and health-related quality of life in individuals with insomnia. J. Psychosom. Res. 2010, 69, 475–483. [Google Scholar] [CrossRef]
- Alapin, I.; Fichten, C.S.; Libman, E.; Creti, L.; Bailes, S.; Wright, J. How is good and poor sleep in older adults and college students related to daytime sleepiness, fatigue, and ability to concentrate? J. Psychosom. Res. 2000, 49, 381–390. [Google Scholar] [CrossRef]
- Christie, A.D.; Seery, E.; Kent, J.A. Physical activity, sleep quality, and self-reported fatigue across the adult lifespan. Exp. Gerontol. 2016, 77, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Hita-Contreras, F.; Martínez-López, E.; Latorre-Román, P.A.; Garrido, F.; Santos, M.A.; Martínez-Amat, A. Reliability and validity of the Spanish version of the Pittsburgh Sleep Quality Index (PSQI) in patients with fibromyalgia. Rheumatol. Int. 2014, 34, 929–936. [Google Scholar] [CrossRef] [PubMed]
- McPhee, J.S.; French, D.P.; Jackson, D.; Nazroo, J.; Pendleton, N.; Degens, H. Physical activity in older age: Perspectives for healthy ageing and frailty. Biogerontology 2016, 17, 567–580. [Google Scholar] [CrossRef] [PubMed]
- Morelhão, P.K.; Tufik, S.; Andersen, M.L. What Are the Effects of Physical Activity on Sleep Quality and Low Back Pain in Older Adults? J. Clin. Sleep Med. 2019, 15, 1067–1068. [Google Scholar] [CrossRef] [PubMed]
- Yang, P.Y.; Ho, K.H.; Chen, H.C.; Chien, M.Y. Exercise training improves sleep quality in middle-aged and older adults with sleep problems: A systematic review. J. Physiother. 2012, 58, 157–163. [Google Scholar] [CrossRef]
- Stutts, W.C. Physical activity determinants in adults: Perceived benefits, barriers, and self-efficacy. Aaohn J. 2002, 50, 499–507. [Google Scholar] [CrossRef]
- Bartlett, J.D.; Close, G.L.; MacLaren, D.P.; Gregson, W.; Drust, B.; Morton, J.P. High-intensity interval running is perceived to be more enjoyable than moderate-intensity continuous exercise: Implications for exercise adherence. J. Sports Sci. 2011, 29, 547–553. [Google Scholar] [CrossRef]
- Kessler, H.S.; Sisson, S.B.; Short, K.R. The potential for high-intensity interval training to reduce cardiometabolic disease risk. Sports Med. 2012, 42, 489–509. [Google Scholar] [CrossRef]
- Rognmo, Ø.; Moholdt, T.; Bakken, H.; Hole, T.; Mølstad, P.; Myhr, N.E.; Grimsmo, J.; Wisløff, U. Cardiovascular risk of high-versus moderate-intensity aerobic exercise in coronary heart disease patients. Circulation 2012, 127, e638. [Google Scholar] [CrossRef]
- Wisloff, U.; Stoylen, A.; Loennechen, J.P.; Bruvold, M.; Rognmo, O.; Haram, P.M.; Tjonna, A.E.; Helgerud, J.; Slordahl, S.A.; Lee, S.J.; et al. Superior cardiovascular effect of aerobic interval training versus moderate continuous training in heart failure patients: A randomized study. Circulation 2007, 115, 3086–3094. [Google Scholar] [CrossRef] [PubMed]
- Meyer, P.; Gayda, M.; Juneau, M.; Nigam, A. High-intensity aerobic interval exercise in chronic heart failure. Curr. Heart Fail. Rep. 2013, 10, 130–138. [Google Scholar] [CrossRef]
- Phillips, B.E.; Kelly, B.M.; Lilja, M.; Ponce-González, J.G.; Brogan, R.J.; Morris, D.L.; Gustafsson, T.; Kraus, W.E.; Atherton, P.J.; Vollaard, N.; et al. A Practical and Time-efficient high-intensity interval Training Program Modifies cardio-Metabolic risk Factors in adults with risk Factors for Type ii Diabetes. Front. Endocrinol. 2017, 8, 229. [Google Scholar] [CrossRef] [PubMed]
- Gaedtke, A.; Morat, T. TRX Suspension Training: A New Functional Training Approach for Older Adults—Development, Training Control and Feasibility. Int. J. Exer. Sci. 2015, 8, 224–233. [Google Scholar]
- Campa, F.; Silva, A.M.; Toselli, S. Changes in Phase Angle and Handgrip Strength Induced by Suspension training in Older Women. Int. J. Sports Med. 2018, 39, 442–449. [Google Scholar] [CrossRef]
- Angleri, V.; Soligon, S.D.; da Silva, D.G.; Bergamasco, J.G.A.; Libardi, C.A. Suspension Training: A New Approach to improve Muscle Strength, Mass and Functional Performances in Older Adults? Front. Physiol. 2020, 10, 1576. [Google Scholar] [CrossRef] [PubMed]
- Jurado-Fasoli, L.; De-la-O, A.; Molina-Hidalgo, C.; Migueles, J.H.; Castillo, M.J.; Amaro-Gahete, F.J. Exercise training improves sleep quality: A randomized controlled trial. Eur. J. Clin. Investig. 2020, 50, e13202. [Google Scholar]
- Bullock, A.; Kovacevic, A.; Kuhn, T.; Heisz, J.J. Optimizing Sleep in Older Adults: Where Does High-Intensity Interval Training Fit? Front. Psychol. 2020, 21, 576316. [Google Scholar] [CrossRef]
- Adams, S.C.; DeLorey, D.S.; Davenport, M.H.; Fairey, A.S.; North, S.; Courneya, K.S. Effects of high-intensity interval training on fatigue and quality of life in testicular cancer survivors. Br. J. Cancer 2018, 118, 1313–1321. [Google Scholar] [CrossRef]
- Balsalobre-Fernández, C.; Cordón, Á.; Unquiles, N.; Muñoz-García, D. Movement velocity in the chair squat is associated with measures of functional capacity and cognition in elderly people at low risk of fall. PeerJ 2018, 6, e4712. [Google Scholar] [CrossRef]
- Harriss, D.J.; Macsween, A.; Atkinson, G. Standards for Ethics in Sport and Exercise Science Research: 2018 Update. Int. J. Sports Med. 2017, 38, 1126–1131. [Google Scholar] [CrossRef] [PubMed]
- Akbari Kamrani, A.A.; Shams, A.; Shamsipour Dehkordi, P.; Mohajeri, R. The effect of low and moderate intensity aerobic exercises on sleep quality in men older adults. Pak. J. Med. Sci. 2014, 30, 417–421. [Google Scholar] [CrossRef] [PubMed]
- Boutron, I.; Moher, D.; Altman, D.G.; Schulz, K.F.; Ravaud, P.; CONSORT Group. Extending the CONSORT statement to randomized trials of nonpharmacologic treatment: Explanation and elaboration. Ann. Intern. Med. 2008, 148, 295–309. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Obesity: Preventing and Management of the Global Epidemic. Report of the WHO Consultation. Technical Report Series, No. 894; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Krupp, L.B.; LaRocca, N.G.; Muir-Nash, J.; Steinberg, A.D. The fatigue severity scale. Application to patients with multiple sclerosis and systemic lupus erythematosus. Arch. Neurol. 1989, 46, 1121–1123. [Google Scholar] [CrossRef]
- Hjollund, N.H.; Andersen, J.H.; Bech, P. Assessment of fatigue in chronic disease: A bibliographic study of fatigue measurement scales. Health Qual. Life Outcomes 2007, 5, 12. [Google Scholar] [CrossRef] [PubMed]
- Ellingsen, Ø.; Halle, M.; Conraads, V.; Støylen, A.; Dalen, H.; Delagardelle, C.; Larsen, A.I.; Hole, T.; Mezzani, A.; Van Craenenbroeck, E.M.; et al. High-Intensity Interval Training in Patients with Heart Failure with Reduced Ejection Fraction. Circulation 2017, 135, 839–849. [Google Scholar] [CrossRef]
- Tanaka, H.; Monahan, K.D.; Seals, D.R. Age-predicted maximal heart rate revisited. J. Am. Coll. Cardiol. 2001, 37, 153–156. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Hillsdale, N.J., Ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988. [Google Scholar]
- Stepnowsky, C.J.; Ancoli-Israel, S. Sleep and Its Disorders in Seniors. Sleep Med. Clin. 2008, 3, 281–293. [Google Scholar]
- Schutte-Rodin, S.; Broch, L.; Buysse, D.; Dorsey, C.; Sateia, M. Clinical guideline for the evaluation and management of chronic insomnia in adults. J. Clin. Sleep Med. 2008, 4, 487–504. [Google Scholar] [CrossRef]
- Ibáñez, V.; Silva, J.; Cauli, O. A survey on sleep questionnaires and diaries. Sleep Med. 2018, 42, 90–96. [Google Scholar] [CrossRef]
- Karimi, S.; Soroush, A.; Towhidi, F.; Makhsosi, B.R.; Karimi, M.; Jamehshorani, S.; Akhgar, A.; Fakhri, M.; Abdi, A. Surveying the effects of an exercise program on the sleep quality of elderly males. Clin. Interv. Aging 2016, 11, 997–1002. [Google Scholar] [PubMed]
- Halpern, J.; Cohen, M.; Kennedy, G. Yoga for improving sleep quality and quality of life for older adults. Altern. Ther. Health Med. 2014, 20, 37–46. [Google Scholar]
- Aibar-Almazán, A.; Hita-Contreras, F.; Cruz-Díaz, D.; de la Torre-Cruz, M.; Jiménez-García, J.D.; Martínez-Amat, A. Effects of Pilates training on sleep quality, anxiety, depression and fatigue in postmenopausal women: A randomized controlled trial. Maturitas 2019, 124, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Meng, M.; Hale, L.; Friedberg, F. Prevalence and predictors of fatigue in middleaged and older adults: Evidence from the health and retirement study. J. Am. Geriatr. Soc. 2010, 58, 2033–2034. [Google Scholar] [CrossRef] [PubMed]
- Puetz, T.W.; O’Connor, P.J.; Dishman, R.K. Effects of chronic exercise on feelings of energy and fatigue: A quantitative synthesis. Psychol. Bull. 2006, 132, 866–876. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.H.; Kim, K.H. Effects of self-foot reflexology on stress, fatigue and blood circulation in premenopausal middle-aged women. J. Korean Acad. Nurs. 2009, 39, 662–672. [Google Scholar]



{kind=link}
{kind=link}
| Total | HIIT | MIIT | Control | p Value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| (n = 73) | (n = 26) | (n = 24) | (n = 23) | |||||||
| Age, years | 68.49 | (5.18) | 68.23 | (2.97) | 68.75 | (5.98) | 68.52 | (6.33) | 0.940 | |
| Sex, % | Men | 17 | (100) | 2 | (11.8) | 7 | (41.2) | 8 | (47.1) | 0.058 |
| Women | 56 | (100) | 24 | (42.9) | 17 | (30.4) | 15 | (26.8) | ||
| Smoker, % | Yes | 6 | (100) | 2 | (33.33) | 4 | (66.67) | 0 | (0) | 0.114 |
| Weight, kg | 76.51 | 12.15 | 73.75 | 14.20 | 76.48 | 12.09 | 79.65 | 9.03 | 0.240 | |
| Height, cm | 157.00 | 7.89 | 155.65 | 7.60 | 159.13 | 8.12 | 15.637 | 7.85 | 0.266 | |
| BMI, kg/m2 | 30.593 | 3.25 | 2948 | 3.69 | 30.33 | 3.07 | 32.13 | 2.30 | 0.019 | |
| No | 67 | (100) | 2 | (33.3) | 4 | (66.7) | 0 | (0) | ||
| FSS | 2.83 | 1.12 | 2.94 | 1.28 | 2.56 | 0.90 | 2.98 | 1.12 | 0.365 | |
| PSQI, score | Subjective sleep quality | 1.18 | (0.84) | 1.23 | (0.86) | 1.38 | (0.71) | 0.91 | (0.90) | 0.156 |
| Sleep latency | 1.30 | (1.01) | 1.46 | (1.07) | 1.13 | (0.95) | 1.30 | (1.02) | 0.506 | |
| Sleep duration | 1.18 | (0.90) | 1.15 | (0.97) | 1.21 | (0.83) | 1.17 | (0.94) | 0.978 | |
| Sleep efficiency | 1.08 | (1.21) | 0.92 | (1.16) | 1.25 | (1.29) | 1.09 | (1.20) | 0.640 | |
| Sleep disturbances | 1.55 | (0.62) | 1.69 | (0.74) | 1.58 | (0.58) | 1.35 | (0.49) | 0.148 | |
| Use of sleeping medication | 0.95 | (1.32) | 0.73 | (1.19) | 0.92 | (1.35) | 1.22 | (1.44) | 0.440 | |
| Daytime dysfunction | 0.51 | (0.56) | 0.50 | (0.51) | 0.38 | (0.49) | 0.65 | (0.65) | 0.234 | |
| Total score | 7.74 | (4.31) | 7.69 | (3.93) | 7.83 | (4.45) | 7.70 | (4.75) | 0.992 | |
| Poor sleep quality, % | Yes | 46 | (63.01) | 17 | (36.96) | 15 | (32.61) | 14 | (30.43) | 0.946 |
| No | 27 | (36.99) | 9 | (33.33) | 9 | (33.33) | 9 | (33.33) | ||
| Post-Intervention Values | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HIIT | MIIT | CONTROL (n = 23) | Group | Time | Group × Time | |||||||||||
| (n = 26) | (n = 24) | |||||||||||||||
| Mean | SD | Mean | SD | Mean | SD | F (2, 70) | p | η2 | F (1, 70) | p | η2 | F (2, 70) | p | η2 | ||
| FSS | 1.91 | 1.30 | 2.95 | 1.07 | 2.85 | 1.34 | 1.66 | 0.198 | 2.70 | 0.103 | 7.01 | 0.002 | 0.17 | |||
| PSQI | Subjective sleep quality † | 0.81 | 0.69 | 0.91 | 0.79 | 0.91 | 0.61 | 0.87 | 0.423 | 11.29 | 0.001 | 0.14 | 5.01 | 0.009 | 0.13 | |
| Sleep latency | 1.04 | 1.04 | 1.79 | 1.10 | 1.30 | 1.06 | 0.32 | 0.729 | 0.68 | 0.414 | 10.55 | <0.001 | 0.23 | |||
| Sleep duration | 0.81 | 0.80 | 0.71 | 0.81 | 1.35 | 0.98 | 1.11 | 0.335 | 4.81 | 0.032 | 0.06 | 3.85 | 0.026 | 0.10 | ||
| Sleep efficiency | 0.69 | 0.93 | 1.13 | 1.30 | 1.35 | 1.30 | 1.15 | 0.322 | 0.06 | 0.808 | 1.31 | 0.277 | ||||
| Sleep disturbances | 1.19 | 0.75 | 1.79 | 0.66 | 1.61 | 0.66 | 1.41 | 0.252 | 0.02 | 0.902 | 9.08 | <0.001 | 0.21 | |||
| Sleep medication | 0.92 | 1.29 | 1.17 | 1.43 | 1.35 | 1.30 | 0.88 | 0.421 | 1.99 | 0.162 | 0.06 | 0.421 | ||||
| Daytime dysfunction †† | 0.62 | 0.75 | 0.67 | 0.58 | 0.96 | 0.71 | 2.28 | 0.111 | 6.16 | 0.016 | 0.08 | 0.43 | 0.654 | |||
| Total score ††† | 6.08 | 3.29 | 7.95 | 4.15 | 8.55 | 4.43 | 0.98 | 0.381 | 0.16 | 0.901 | 5.50 | 0.006 | 0.15 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiménez-García, J.D.; Hita-Contreras, F.; de la Torre-Cruz, M.J.; Aibar-Almazán, A.; Achalandabaso-Ochoa, A.; Fábrega-Cuadros, R.; Martínez-Amat, A. Effects of HIIT and MIIT Suspension Training Programs on Sleep Quality and Fatigue in Older Adults: Randomized Controlled Clinical Trial. Int. J. Environ. Res. Public Health 2021, 18, 1211. https://doi.org/10.3390/ijerph18031211
Jiménez-García JD, Hita-Contreras F, de la Torre-Cruz MJ, Aibar-Almazán A, Achalandabaso-Ochoa A, Fábrega-Cuadros R, Martínez-Amat A. Effects of HIIT and MIIT Suspension Training Programs on Sleep Quality and Fatigue in Older Adults: Randomized Controlled Clinical Trial. International Journal of Environmental Research and Public Health. 2021; 18(3):1211. https://doi.org/10.3390/ijerph18031211
Chicago/Turabian StyleJiménez-García, José Daniel, Fidel Hita-Contreras, Manuel Jesús de la Torre-Cruz, Agustín Aibar-Almazán, Alexander Achalandabaso-Ochoa, Raquel Fábrega-Cuadros, and Antonio Martínez-Amat. 2021. "Effects of HIIT and MIIT Suspension Training Programs on Sleep Quality and Fatigue in Older Adults: Randomized Controlled Clinical Trial" International Journal of Environmental Research and Public Health 18, no. 3: 1211. https://doi.org/10.3390/ijerph18031211
APA StyleJiménez-García, J. D., Hita-Contreras, F., de la Torre-Cruz, M. J., Aibar-Almazán, A., Achalandabaso-Ochoa, A., Fábrega-Cuadros, R., & Martínez-Amat, A. (2021). Effects of HIIT and MIIT Suspension Training Programs on Sleep Quality and Fatigue in Older Adults: Randomized Controlled Clinical Trial. International Journal of Environmental Research and Public Health, 18(3), 1211. https://doi.org/10.3390/ijerph18031211