Reliability and Validity of the Malay Mindful Eating Questionnaire (MEQ-M) among Overweight and Obese Adults

 ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. The Questionnaire
2.2. Translating the Questionnaire
2.3. Data Collection
2.4. Validation of MEQ-M
2.4.1. Construct Validity
2.4.2. Concurrent Validity
2.4.3. Reliability: Internal Consistency
2.4.4. Reliability: Test-Retest
3. Results
3.1. Participants
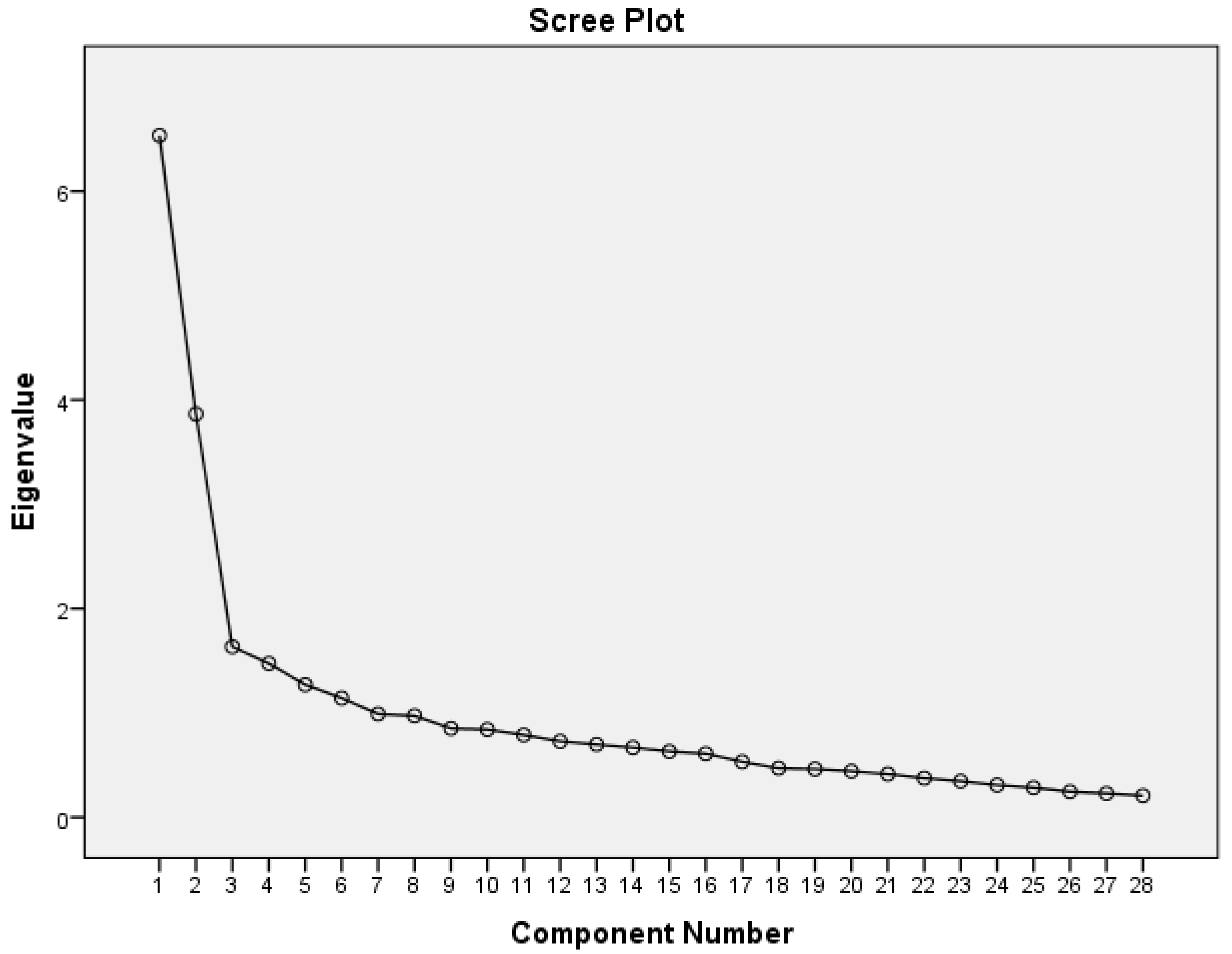
3.2. Construct Validity
3.3. Concurrent Validity
3.4. Reliability
3.5. Correlation between Sociodemographic Characteristics and the MEQ-M
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Item | Question |
|---|---|
| 1 | I eat so quickly that I don’t taste what I’m eating. |
| Saya makan dengan cepat sehingga saya tidak rasa apa yang saya makan. | |
| 2 | When I eat at “all you can eat” buffets, I tend to overeat. |
| Saya cenderung untuk terlebih makan apabila saya berada di jamuan buffet. | |
| 3 | At a party where there is a lot of good food, I notice when it makes me want to eat more food than I should. |
| Saya mempunyai keinginan untuk makan berlebihan sekiranya terdapat makanan yang lazat di sesebuah jamuan keramaian. | |
| 4 | I recognize when food advertisements make me want to eat. |
| Saya sedar iklan makanan akan membuatkan saya ingin makan. | |
| 5 | When a restaurant portion is too large, I stop eating when I’m full. |
| Apabila saiz porsi makanan di restoran/gerai terlalu besar, saya berhenti makan apabila sudah kenyang. | |
| 6 | My thoughts tend to wander while I am eating. |
| Fikiran saya cenderung melayang jauh/menerawang ketika sedang makan. | |
| 7 | When I’m eating one of my favorite foods, I don’t recognize when I’ve had enough. |
| Saya tidak sedar yang saya sudah kenyang apabila saya makan makanan yang saya gemari. | |
| 8 | I notice that just going into a movie theatre makes me want to eat candy or popcorn. |
| Saya ada keinginan untuk makan bertih jagung/makanan ringan apabila pergi menonton di pawagam. | |
| 9 | If it doesn’t cost much more, I get the larger size food or drink regardless of how hungry I feel. |
| Saya akan mengambil makanan/minuman bersaiz porsi besar tanpa mengira tahap kelaparan saya jika ia tidak melibatkan tambahan kos. | |
| 10 | I notice when there are subtle flavors in the foods I eat. |
| Saya dapat rasa/perasan jika terdapat sedikit perasa di dalam makanan saya. | |
| 11 | If there are leftovers that I like, I take a second helping even though I’m full. |
| Jika terdapat saki baki makanan yang saya gemari, saya akan makan lagi walaupun sudah kenyang. | |
| 12 | When eating a pleasant meal, I notice if it makes me feel relaxed. |
| Saya akan berasa tenang apabila saya makan makanan yang menyenangkan/menggembirakan. | |
| 13 | I snack without noticing that I am eating. |
| Saya mengudap tanpa saya sedari. | |
| 14 | When I eat a big meal, I notice if it makes me feel heavy or sluggish. |
| Saya akan merasa lesu selepas makan hidangan yang besar. | |
| 15 | I appreciate the way my food looks on my plate. |
| Saya menghargai rupa makanan yang dihidangkan di dalam pinggan saya. | |
| 16 | I stop eating when I’m full even when eating something I love. |
| Saya berhenti makan apabila sudah kenyang walaupun saya sedang makan makanan yang saya gemari. | |
| 17 | When I’m feeling stressed at work, I’ll go find something to eat. |
| Saya akan mencari makanan untuk dimakan sekiranya saya merasa tertekan di tempat kerja. | |
| 18 | If there’s good food at a party, I’ll continue eating even after I’m full. |
| Jika terdapat makanan yang lazat di jamuan keramaian, saya akan terus makan walaupun sudah kenyang. | |
| 19 | When I’m sad I eat to feel better. |
| Saya akan makan untuk menghilangkan kesedihan saya. | |
| 20 | I notice when foods and drinks are too sweet. |
| Saya dapat merasakan jika sesuatu makanan dan minuman itu terlalu manis. | |
| 21 | Before I eat, I take a moment to appreciate the colors and smells of my food. |
| Saya akan mengambil sedikit masa untuk menghargai warna dan bau makanan sebelum saya makan. | |
| 22 | I taste every bite of food that I eat. |
| Saya rasa setiap kunyahan makanan yang saya makan. | |
| 23 | I recognize when I’m eating and I’m not hungry. |
| Saya sedar apabila saya sedang makan dan tidak berasa lapar. | |
| 24 | I notice when I’m eating from a dish of candy just because it’s there. |
| Saya perasan saya makan sesuatu gula-gula/kerepek/makanan ringan hanya kerana ia berada berhampiran saya. | |
| 25 | When I’m at a restaurant, I can tell when the portion I’ve been served is too large for me. |
| Apabila saya berada di restoran/gerai makanan, saya dapat mengagak sekiranya saiz hidangannya terlalu besar bagi saya. | |
| 26 | I notice when the food I eat affects my emotional state. |
| Saya perasan jika sesuatu makanan itu memberi kesan kepada emosi saya. | |
| 27 | I have trouble not eating ice cream, cookies, or chips if they’re around the house. |
| Saya tidak dapat mengawal kemahuan untuk makan makanan ringan (spt. Aiskrim, biskut, kerepek) sekiranya makanan tersebut ada di rumah. | |
| 28 | I think about things I need to do while I am eating. |
| Saya memikirkan hal-hal lain yang saya perlu lakukan ketika sedang makan. |
References
- Framson, C.; Kristal, A.R.; Jeannette, S.; Littman, A.J.; Zeliadt, S.; Benitez, D. Development and validation of the Mindful Eating Questionnaire. J. Am. Diet Assoc. 2009, 109, 1439–1444. [Google Scholar] [CrossRef] [PubMed]
- Ruffault, A.; Czernichow, S.; Hagger, M.S.; Ferrand, M.; Erichot, N.; Carette, C.; Boujut, E.; Flahault, C. The effects of mindfulness training on weight-loss and health-related behaviours in adults with overweight and obesity: A systematic review and meta-analysis. Obes. Res. Clin. Pract. 2017, 11, 90–111. [Google Scholar] [CrossRef] [PubMed]
- Dunn, C.; Haubenreiser, M.; Johnson, M.; Nordby, K.; Aggarwal, S.; Myer, S.; Thomas, C.; Dunn, C.; Johnson, M.; Nordby, K. Mindfulness approaches and weight loss, weight maintenance, and weight regain. Curr. Obes. Rep. 2018, 7, 37–49. [Google Scholar] [CrossRef] [PubMed]
- Alberts, H.J.E.M.; Thewissen, R.; Raes, L. Dealing with problematic eating behaviour. The effects of a mindfulness-based intervention on eating behaviour, food cravings, dichotomous thinking and body image concern. Appetite 2012, 58, 847–851. [Google Scholar] [CrossRef]
- Beshara, M.; Hutchinson, A.D.; Wilson, C. Does mindfulness matter? Everyday mindfulness, mindful eating and self-reported serving size of energy dense foods among a sample of South Australian adults. Appetite 2013, 67, 25–29. [Google Scholar] [CrossRef]
- Mason, A.E.; Epel, E.S.; Kristeller, J.; Moran, P.J.; Dallman, M.; Lustig, R.H.; Acree, M.; Bacchetti, P.; Laraia, B.A.; Frederick, M. Effects of a mindfulness-based intervention on mindful eating, sweet consumption, and fasting glucose levels in obese adults: Data from the SHINE randomized controlled trial. J. Behav. Med. 2016, 39, 201–213. [Google Scholar] [CrossRef]
- Ganasegeran, K.; Al-dubai, S.A.R.; Qureshi, A.M.; Al-abed, A.A.A.; Am, R. Social and psychological factors affecting eating habits among university students in a Malaysian medical school: A cross-sectional study. Nutr. J. 2012, 11, 48–54. [Google Scholar] [CrossRef]
- Leung, S.L.; Barber, J.A.; Burger, A.; Barnes, R.D. Factors associated with healthy and unhealthy workplace eating behaviours in individuals with overweight / obesity with and without binge eating disorder. Obes. Sci. Pract. 2018, 4, 109–118. [Google Scholar] [CrossRef]
- Mazri, F.H.; Manaf, Z.A.; Shahar, S.; Fitri, A.; Ludin, M. The association between chronotype and dietary pattern among adults: A scoping review. Int J. Environ. Res. Public Health 2020, 17, 68. [Google Scholar] [CrossRef]
- Herbert, B.M.; Pollatos, O. Attenuated interoceptive sensitivity in overweight and obese individuals. Eat. Behav. 2014, 15, 445–448. [Google Scholar] [CrossRef]
- Kristeller, J.L.; Baer, R.A.; Quillian-Wolever, R. Mindfulness-based approaches to eating disorders. In Mindfulness-Based Treatment Approaches: Clinician’s Guide to Evidence Base and Applications; Baer, R.A., Ed.; Elsevier Academic Press: Cambridge, UK, 2006; pp. 75–91. [Google Scholar] [CrossRef]
- Kristeller, J.L.; Epel, E. Mindful eating and mindless eating: The science and the practice. In The Wiley Blackwell Handbook of Mindfulness; Ie, A., Ngnoumen, C.T., Langer, E.J., Eds.; John Wiley & Sons, Ltd.: West Sussex, UK, 2014; Volume 1 & 2, pp. 913–933. [Google Scholar] [CrossRef]
- Birch, L.L.; Fisher, J.O.; Davison, K.K. Learning to overeat: Maternal use of restrictive feeding practices promotes girls’ eating in the absence of hunger. Am. J. Clin. Nutr. 2003, 78, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Hawks, S.; Madanat, H.; Hawks, J.; Harris, A. The relationship between intuitive eating and health indicators among college women. Am. J. Health Educ. 2005, 36, 331–336. [Google Scholar] [CrossRef]
- Smith, T.S.; Hawks, S.R. Intuitive eating, diet composition, and the meaning of food in healthy weight promotion. Am. J. Health Educ. 2006, 37, 130–136. [Google Scholar] [CrossRef]
- Gianini, L.M.; White, M.A.; Masheb, R.M. Eating pathology, emotion regulation, and emotional overeating in obese adults with binge eating disorder. Eat. Behav. 2013, 14, 309–313. [Google Scholar] [CrossRef]
- Leehr, E.J.; Krohmer, K.; Schag, K.; Dresler, T.; Zipfel, S.; Giel, K.E. Emotion regulation model in binge eating disorder and obesity—A systematic review. Neurosci. Biobehav. Rev. 2015, 49, 125–134. [Google Scholar] [CrossRef]
- Micanti, F.; Iasevoli, F.; Cucciniello, C.; Costabile, R.; Loiarro, G.; Pecoraro, G.; Pasanisi, F.; Rossetti, G.L.; Galletta, D. The relationship between emotional regulation and eating behaviour: A multidimensional analysis of obesity psychopathology. Eat. Weight Disord. 2017, 22, 105–115. [Google Scholar] [CrossRef]
- Rosnah, I.; Idris, M.A.; Azmi, M.T.; Noor Hassim, I. Job stress on abdominal obesity: The moderating effects of anger and overeating behaviour. Malays. J. Nutr. 2017, 23, 437–448. [Google Scholar]
- Ozier, A.D.; Kendrick, O.W.; Leeper, J.D.; Knol, L.L.; Perko, M.; Burnham, J. Overweight and obesity are associated with emotion- and stress-related eating as measured by the Eating and Appraisal Due to Emotions and Stress Questionnaire. J. Am. Diet. Assoc. 2008, 108, 49–56. [Google Scholar] [CrossRef]
- Dallman, M.F. Stress-induced obesity and the emotional nervous system. Trends Endocrinol. Metab. 2010, 21, 159–165. [Google Scholar] [CrossRef]
- Sinha, R.; Jastreboff, A.M. Stress as a common risk factor for obesity and addiction. Biol. Psychiatry 2013, 73, 827–835. [Google Scholar] [CrossRef]
- Frayn, M.; Knäuper, B. Emotional eating and weight in adults: A review. Curr. Psychol. 2018, 37, 924–933. [Google Scholar] [CrossRef]
- Olson, K.L.; Emery, C.F. Mindfulness and weight loss: A systematic review. Psychosom. Med. 2015, 77, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Van Strien, T.; Peter Herman, C.; Verheijden, M.W. Eating style, overeating and weight gain. A prospective 2-year follow-up study in a representative Dutch sample. Appetite 2012, 59, 782–789. [Google Scholar] [CrossRef]
- Apolzan, J.W.; Myers, C.A.; Cowley, A.D.; Brady, H.; Hsia, D.S.; Stewart, T.M.; Redman, L.M.; Martin, C.K. Examination of the reliability and validity of the Mindful Eating Questionnaire in pregnant women. Appetite 2017, 100, 142–151. [Google Scholar] [CrossRef] [PubMed]
- Abbaspoor, Z.; Javadifar, N.; Miryan, M.; Abedi, P. Psychometric properties of the Iranian version of mindful eating questionnaire in women who seeking weight reduction. J. Eat. Disord. 2018, 6, 4–11. [Google Scholar] [CrossRef]
- Clementi, C.; Casu, G.; Gremigni, P. An Abbreviated Version of the Mindful Eating Questionnaire. J. Nutr. Educ. Behav. 2017, 49, 352–356. [Google Scholar] [CrossRef]
- Zainal, N.; Nor-Aziyan, Y.; Subramaniam, P. Psychometric properties of the Malay-translated Mindfulness, Attention and Awareness Scale (MAAS) in a Malaysian population. Malays. J. Psychiatry 2015, 24. [Google Scholar]
- World Health Organization (WHO). Fact Sheet on Obesity and Overweight. Available online: http://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight. (accessed on 15 September 2020).
- Institute for Public Health. National Health and Morbidity Survey 2015 (NHMS 2015). Vol. II: Non-Communicable Diseases, Risk Factors & Other Health Problems. Available online: http://www.iku.gov.my/nhms-2015 (accessed on 2 February 2020).
- Institute for Public Health. National Health and Morbidity Survey 2011 (NHMS 2011). Available online: http://www.iku.gov.my/nhms-2011 (accessed on 2 February 2020).
- Afshin, A.; Forouzanfar, M.H.; Reitsma, M.B.; Sur, P.; Estep, K.; Lee, A.; Marczak, L.; Mokdad, A.H.; Moradi-Lakeh, M.; Naghavi, M.; et al. Health effects of overweight and obesity in 195 countries over 25 years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar] [CrossRef]
- Chrostowska, M.; Szyndler, A.; Hoffmann, M.; Narkiewicz, K. Impact of obesity on cardiovascular health. Best Pract. Res. Clin. Endocrinol. Metab. 2013, 27, 147–156. [Google Scholar] [CrossRef]
- Dobbins, M.; Decorby, K.; Choi, B.C.K. The association between obesity and cancer risk: A meta-analysis of observational studies from 1985 to 2011. ISRN Prev Med. 2013, 1–16. [Google Scholar] [CrossRef]
- Littleton, S.W. Impact of obesity on respiratory function. Respirology 2012, 17, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, S. Obesity and diabetes: Interrelationship. Adv. Obes. Weight Manag. Control. 2018, 8, 155–158. [Google Scholar] [CrossRef]
- Cao, J.J. Effect of obesity on bone metabolism. J. Orthop. Surg. Res. 2011, 6, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Pataky, Z.; Armand, S.; Müller-Pinget, S.; Golay, A.; Allet, L. Effects of obesity on functional capacity. Obesity 2014, 22, 56–62. [Google Scholar] [CrossRef]
- Tan, S.X.; Norhayati, I.; Nuruljannah, J.; Roszanadia, R.; Zahara, A.M. Obesity is associated with more sick leave and lower quality of life among malay male security officers. J. Sains Kesihatan Malays. 2016, 14, 31–37. [Google Scholar] [CrossRef]
- Kjellberg, J.; Tange Larsen, A.; Ibsen, R.; Højgaard, B. The socioeconomic burden of obesity. Obes. Facts 2017, 10, 493–502. [Google Scholar] [CrossRef]
- Lehnert, T.; Streltchenia, P.; Konnopka, A.; Riedel-Heller, S.G.; König, H.H. Health burden and costs of obesity and overweight in Germany: An update. Eur. J. Health Econ. 2015, 16, 957–967. [Google Scholar] [CrossRef]
- Seidell, J.C.; Halberstadt, J. The global burden of obesity and the challenges of prevention. Ann. Nutr. Metab. 2015, 66, 7–12. [Google Scholar] [CrossRef]
- Tambelli, R.; Cerniglia, L.; Cimino, S.; Ballarotto, G.; Paciello, M.; Lubrano, C.; Marchitelli, S.; Gnessi, L.; Lenzi, A. An exploratory study on the influence of psychopathological risk and impulsivity on BMI and perceived quality of life in obese patients. Nutrients 2017, 9, 431. [Google Scholar] [CrossRef]
- Moor, K.R.; Scott, A.J.; McIntosh, W.D. Mindful Eating and Its Relationship to Body Mass Index and Physical Activity Among University Students. Mindfulness 2013, 4, 269–274. [Google Scholar] [CrossRef]
- Pintado-Cucarella, S.; Rodríguez-Salgado, P. Mindful eating and its relationship with body mass index, binge eating, anxiety and negative affect. J. Behav. 2016, 8, 19–24. [Google Scholar] [CrossRef]
- Timmerman, G.M.; Brown, A. The effect of a mindful restaurant eating intervention on weight management in women. J. Nutr. Educ. Behav. 2012, 44, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Sperber, A.D. Translation and validation of study instruments for cross-cultural research. Gastroenterology 2004, 126, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Osborne, J.; Osborne, J.W.; Costello, A.B.; Kellow, J.T. Best practices in exploratory factor analysis. In Best Practices in Quantitative Methods; Osborne, J., Ed.; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2011; pp. 86–99. [Google Scholar] [CrossRef]
- Kline, P. A Psychometrics Primer; Free Association books: London, UK, 2000. [Google Scholar]
- Geisinger, K.F.; McCormick, C. Testing and assessment in cross-cultural psychology. In Handbook of Assessment Psychology; Graham, J.R., Naglieri, J.A., Eds.; Wiley: New York, NY, USA, 2003; Volume 10, pp. 109–110. [Google Scholar]
- Koo, T.K.; Li, M.Y. A Guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Brown, K.W.; Ryan, R.M. The Benefits of being present: Mindfulness and its role in psychological well-being. J. Pers. Soc. Psychol. 2003, 84, 822–848. [Google Scholar] [CrossRef]
- Cronbach, L.J. Coefficient alpha and the internal structure of tests. Psychometrika 1951, 16, 297–334. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 159–174. [Google Scholar] [CrossRef]
- Ji, L.J.; Zhang, Z.; Nisbett, R.E. Is it culture or is it language? Examination of language effects in cross-cultural research on categorization. J. Pers. Soc. Psychol. 2004, 87, 57–65. [Google Scholar] [CrossRef]
- Sousa, V.D.; Rojjanasrirat, W. Translation, adaptation and validation of instruments or scales for use in cross-cultural health care research: A clear and user-friendly guideline. J. Eval. Clin. Pract. 2011, 17, 268–274. [Google Scholar] [CrossRef]
- Ariffin, F.; Daud, S.; Ismail, Z.; Zainuddin, A.A.; Ramli, R. Language and cross-cultural influences in the psychometric evaluation of the Malaysian FertiQoL. Malays. J. Med. Health Sci. 2020, 16, 157–163. [Google Scholar]

| Age (years), mean ± SD | 40.3 ± 6.9 |
| BMI (kg/m2), mean ± SD (range) | 31.7 ± 6.1 (25.0–60.6) |
| Gender, n (%) | |
| Male | 41 (28.5) |
| Female | 103 (71.5) |
| Education level, n (%) | |
| Secondary school | 30 (20.8) |
| Tertiary | 113 (78.5) |
| Others | 1 (0.7) |
| Marital status, n (%) | |
| Single | 12 (8.3) |
| Married | 128 (88.9) |
| Divorced | 4 (2.8) |
| Monthly household income (RM), n (%) | |
| ≤RM 3000 (≤$718.99) | 21 (14.6) |
| RM 3001-RM 5000 ($719.23–$1198.32) | 50 (34.7) |
| RM 5001-RM 7000 ($1198.56–$1677.65) | 28 (19.4) |
| >RM 7000 (>$1677.65) | 45 (31.3) |
| MEQ Items | Factor 1 | Factor 2 | Factor 3 | Factor 4 | Factor 5 | Factor 6 | Factor 7 |
|---|---|---|---|---|---|---|---|
| Item 1 | 0.578 | ||||||
| Item 2 | 0.680 | ||||||
| Item 3 | −0.786 | ||||||
| Item 9 | 0.726 | ||||||
| Item 11 | 0.690 | ||||||
| Item 13 | 0.483 | ||||||
| Item 18 | 0.654 | ||||||
| Item 6 | 0.595 | ||||||
| Item 7 | 0.556 | ||||||
| Item 17 | 0.646 | ||||||
| Item 19 | 0.580 | ||||||
| Item 27 | 0.558 | ||||||
| Item 28 | 0.745 | ||||||
| Item 10 | 0.450 | ||||||
| Item 12 | 0.690 | ||||||
| Item 15 | 0.732 | ||||||
| Item 21 | 0.492 | ||||||
| Item 26 | 0.429 | ||||||
| Item 20 | 0.736 | ||||||
| Item 22 | 0.425 | ||||||
| Item 24 | 0.593 | ||||||
| Item 25 | 0.736 | ||||||
| Item 5 | 0.717 | ||||||
| Item 14 | 0.597 | ||||||
| Item 16 | 0.556 | ||||||
| Item 4 | 0.757 | ||||||
| Item 23 | 0.657 | ||||||
| Item 8 | 0.765 |
| MEQ-M Subscales | Factor 1 (Environmental Disinhibition) | Factor 2 (Emotional Response) | Factor 3 (Taste Awareness) | Factor 4 (Emotion Awareness) | Factor 5 (Portion Disinhibition) | Factor 6 (External Cues of Foods) | Factor 7 (External Cues of Place) |
|---|---|---|---|---|---|---|---|
| MAAS | 0.295 b | 0.329 b | −0.039 | 0.047 | 0.031 | −0.147 | −0.179 a |
| Factor 1 | 0.592 b | −0.161 | 0.105 | 0.092 | −0.414 b | −0.336 b | |
| Factor 2 | −0.322 b | −0.013 | −0.06 | −0.520 b | −0.414 b | ||
| Factor 3 | 0.447 b | 0.398 b | 0.396 b | 0.307 b | |||
| Factor 4 | 0.449 b | 0.262 b | 0.078 | ||||
| Factor 5 | 0.114 | 0.000 | |||||
| Factor 6 | 0.359 b |
| Subscales | Cronbach’s Alpha | McDonald’s Omega | Mean ± SD | ICC (95% CI) |
|---|---|---|---|---|
| MEQ-M | ||||
| Environmental disinhibition | 0.52 | 0.67 | 2.9 ± 0.39 | 0.320 |
| Emotional response | 0.62 | 0.80 | 3.1 ± 0.51 | 0.468 |
| Taste awareness | 0.70 | 0.71 | 2.4 ±0.52 | 0.256 |
| Emotion awareness | 0.62 | 0.64 | 2.7 ± 0.50 | 0.083 |
| Portion disinhibition | 0.54 | 0.58 | 2.5 ± 0.53 | −0.173 |
| External cues of food | 0.27 | NA | 2.3 ± 0.59 | −0.213 |
| External cues of place | NA | NA | 2.2 ± 0.85 | −0.065 |
| Summary score | 0.64 | 0.44 | 2.6 ± 0.25 | 0.104 |
| MAAS | 0.88 | 0.89 | 4.57 ± 0.59 | 0.295 |
| MEQ-M Subscales | Age | BMI | Gender | Education Level | Marital Status | Household Monthly Income |
|---|---|---|---|---|---|---|
| Environmental disinhibition | 0.255 ** | −0.207 * | 0.169 * | −0.026 | −0.015 | 0.082 |
| Emotional response | 0.266 ** | −0.072 | −0.017 | 0.048 | 0.018 | 0.127 |
| Taste awareness | −0.077 | 0.115 | 0.125 | 0.017 | 0.053 | −0.009 |
| Emotion awareness | 0.036 | 0.000 | 0.060 | −0.060 | 0.006 | −0.025 |
| Portion disinhibition | −0.015 | 0.052 | −0.007 | 0.048 | 0.038 | −0.077 |
| External cues of food | −0.071 | 0.066 | 0.137 | 0.149 | −0.048 | −0.043 |
| External cues of place | −0.074 | 0.022 | −0.009 | 0.000 | −0.027 | −0.104 |
| Summary score | 0.104 | 0.002 | 0.127 | −0.017 | 0.007 | −0.010 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdul Basir, S.M.; Abdul Manaf, Z.; Ahmad, M.; Abdul Kadir, N.B.; Ismail, W.N.K.; Mat Ludin, A.F.; Shahar, S. Reliability and Validity of the Malay Mindful Eating Questionnaire (MEQ-M) among Overweight and Obese Adults. Int. J. Environ. Res. Public Health 2021, 18, 1021. https://doi.org/10.3390/ijerph18031021
Abdul Basir SM, Abdul Manaf Z, Ahmad M, Abdul Kadir NB, Ismail WNK, Mat Ludin AF, Shahar S. Reliability and Validity of the Malay Mindful Eating Questionnaire (MEQ-M) among Overweight and Obese Adults. International Journal of Environmental Research and Public Health. 2021; 18(3):1021. https://doi.org/10.3390/ijerph18031021
Chicago/Turabian StyleAbdul Basir, Siti Munirah, Zahara Abdul Manaf, Mahadir Ahmad, Nor Ba’yah Abdul Kadir, Wan Nur Khairunnisa Ismail, Arimi Fitri Mat Ludin, and Suzana Shahar. 2021. "Reliability and Validity of the Malay Mindful Eating Questionnaire (MEQ-M) among Overweight and Obese Adults" International Journal of Environmental Research and Public Health 18, no. 3: 1021. https://doi.org/10.3390/ijerph18031021
APA StyleAbdul Basir, S. M., Abdul Manaf, Z., Ahmad, M., Abdul Kadir, N. B., Ismail, W. N. K., Mat Ludin, A. F., & Shahar, S. (2021). Reliability and Validity of the Malay Mindful Eating Questionnaire (MEQ-M) among Overweight and Obese Adults. International Journal of Environmental Research and Public Health, 18(3), 1021. https://doi.org/10.3390/ijerph18031021