
A Novel Predictor for Micro-Scale COVID-19 Risk Modeling: An Empirical Study from a Spatiotemporal Perspective


Abstract
:1. Introduction
2. Data and Methodology
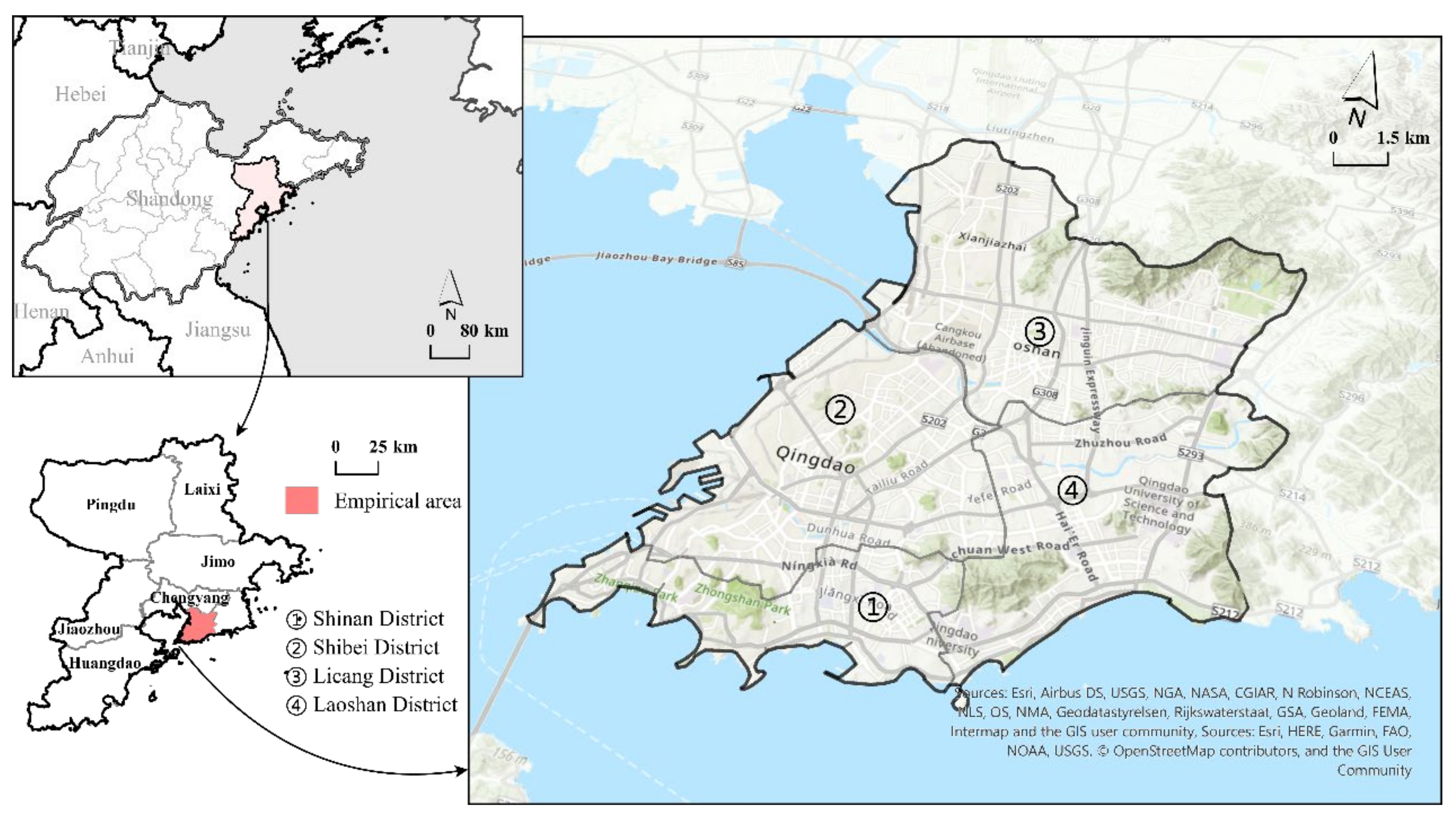
2.1. Empirical Area
2.2. Data Sources and Measures
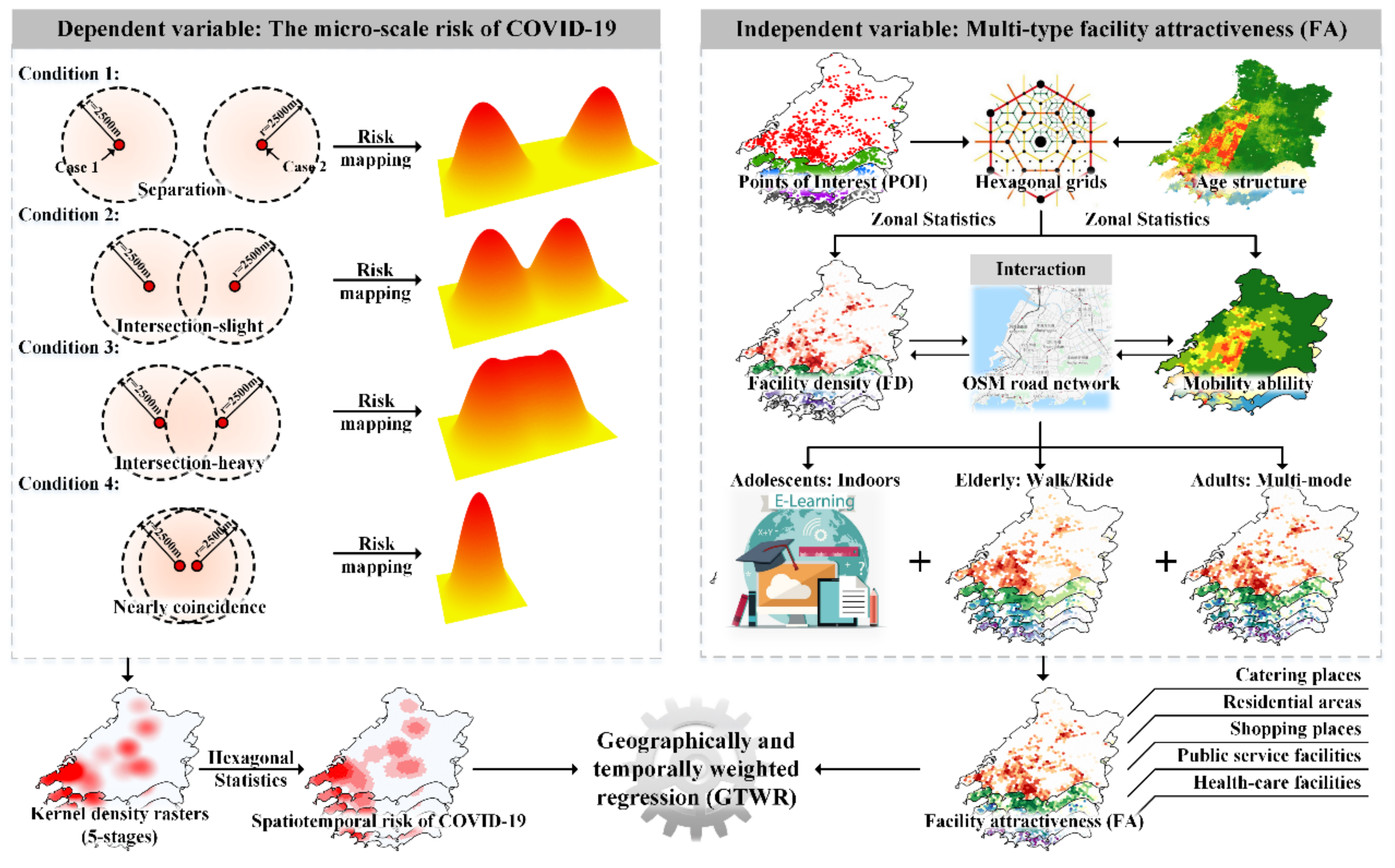
2.3. Methodology
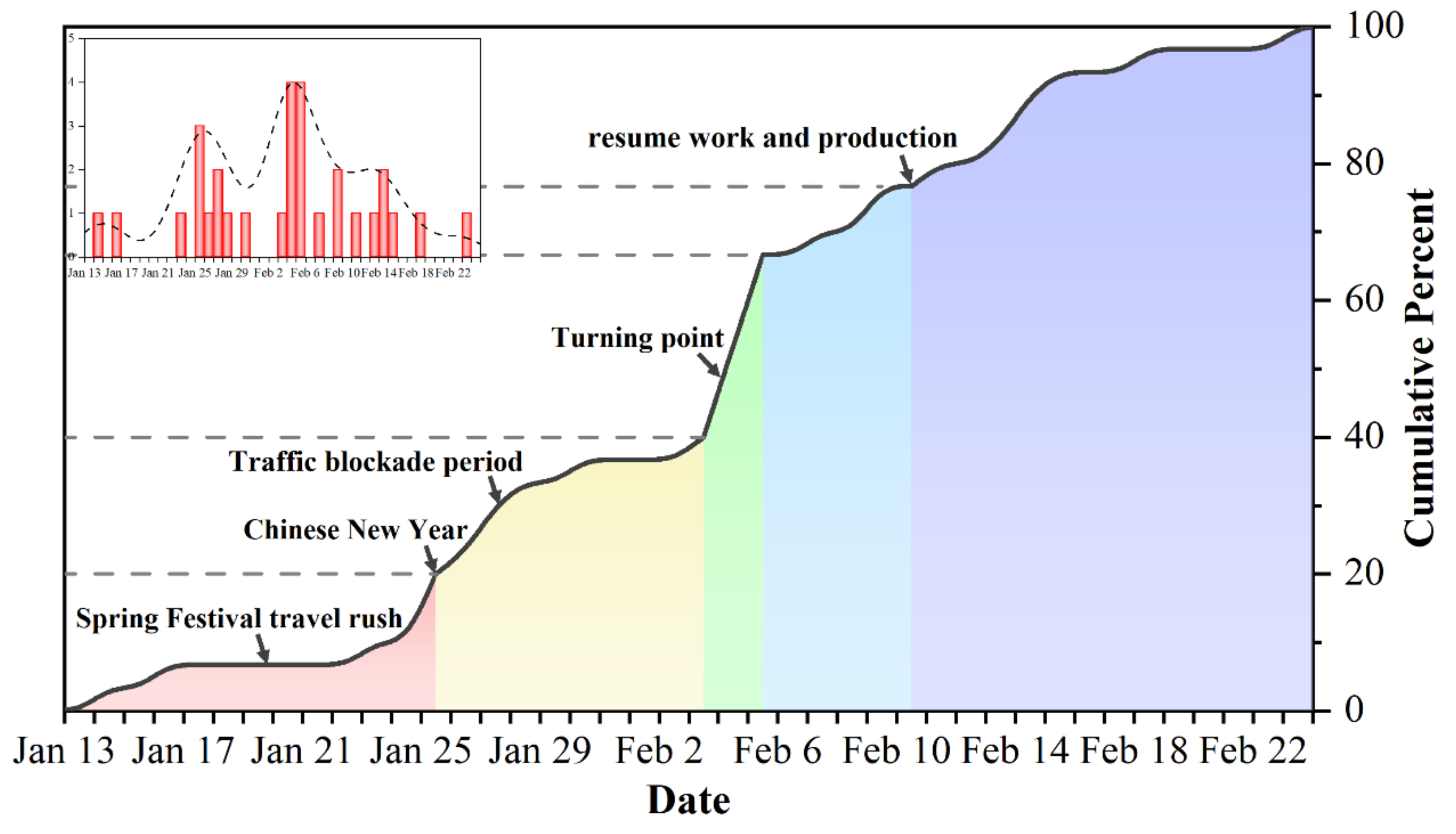
2.3.1. Mapping the Micro-Scale Spatiotemporal COVID-19 Risk
2.3.2. Facility Attractiveness (FA) and Optimized Gravity Model
- (1)
- We carried out a topology inspection and correction on OSM road network data and calculated the mileage sij between place i and place j. On this basis, the hierarchy of the OSM road network was considered as well as the actual situation of Qingdao, the average travel speed of roads was set for all levels, and the travel time tij was calculated. These two data points were used to replace the role of dij in the traditional gravity model in this study (Table 1).
- (2)
- During the pandemic in the first half of 2020, almost all public transportation was suspended in most parts of China, which made self-driving travel the only realistic and convenient way to travel long distances. Since Chinese laws prohibit citizens under the age of 18 and over the age of 70 from obtaining a motor vehicle driving license, the possible travel modes used by people of different age groups would have been quite different in the pandemic era. In order to take into account the heterogeneity of the mobility and travel range of the age-hierarchical population, the total population was divided into three groups according to their ages: 0–19 years old (adolescent group), 20–69 years old (adult group), and 70+ years old (elderly group). According to the previous references and the research group’s visit to Qingdao [52,53,54,55]:
- Due to campus closures and the strict community control measures implemented during the first wave of the pandemic, most students (under 20 years old) received their education online and lacked sufficient time or motivation to travel [53]. Therefore, this group, which also had extremely limited travel possibilities, was not included in the model used in this study.
- As most elderly people over 70 years old do not live with their children in China, this group are likely to have a high travel frequency in order to carry out necessary daily [56]. However, due to the limitations of transportation modes and mobility levels, the range of activities of elderly people is generally limited to less than 1200 m [57,58]. Therefore, in this model we set 1200 m as the travel threshold for the 70+ age group in order to calculate the attractiveness of various facilities to the elderly more reasonably.
- Qingdao has become one of the cities in China with the longest average travel times due to the separation of occupation areas and residential spaces [59]. The 20–69 age group is the most active group and has the largest travel range. Given the diversity of their travel modes, setting our search threshold according to mileage will lead to great deviations. Therefore, in this study referred to survey results and adopted a travel time of 1 h (3600 s) as the travel threshold for the 20–69 age group.
- Possible travel routes exceeding the travel threshold of the two age groups mentioned above were not considered in this model.
- (3)
- We replaced the power function distance decay function in (1) with the Gaussian distance decay function corresponding to the travel threshold of each age group.
- (4)
- We then summed the calculation results of the multi-age models.
2.3.3. Geographically and Temporally Weighted Regression (GTWR)
3. Model Results
4. Discussion
4.1. Comparison of Model Performance between FD and FA
4.1.1. Global Explanatory Ability of the Models
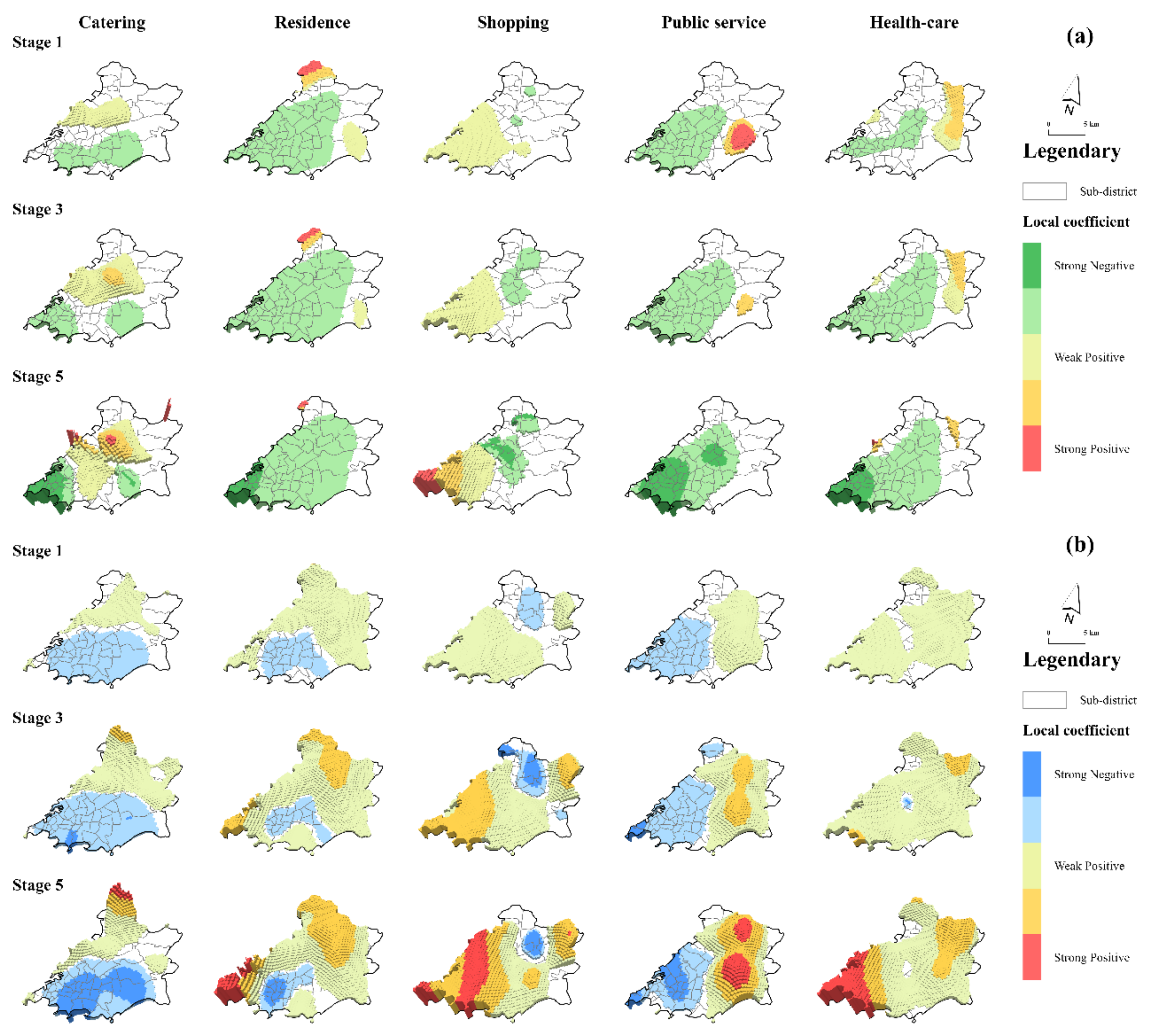
4.1.2. Local Explanatory Ability of Grids with Different Risk Levels
4.1.3. Local Explanatory Ability of Grids in Different Administrative Regions
4.2. Limitation and Prospection
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wu, F.; Zhao, S.; Yu, B.; Chen, Y.-M.; Wang, W.; Song, Z.-G.; Hu, Y.; Tao, Z.-W.; Tian, J.-H.; Pei, Y.-Y.; et al. A new coronavirus associated with human respiratory disease in China. Nature 2020, 579, 265–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Dorn, A.; Cooney, R.E.; Sabin, M.L. COVID-19 exacerbating inequalities in the US. Lancet 2020, 395, 1243–1244. [Google Scholar] [CrossRef]
- Zambrano-Monserrate, M.A.; Ruano, M.A.; Sanchez-Alcalde, L. Indirect effects of COVID-19 on the environment. Sci. Total Environ. 2020, 728, 138813. [Google Scholar] [CrossRef] [PubMed]
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Gössling, S.; Scott, D.; Hall, C.M. Pandemics, tourism and global change: A rapid assessment of COVID-19. J. Sustain. Tour. 2020, 29, 1–20. [Google Scholar] [CrossRef]
- Clark, A.; Jit, M.; Warren-Gash, C.; Guthrie, B.; Wang, H.H.X.; Mercer, S.W.; Sanderson, C.; McKee, M.; Troeger, C.; Ong, K.L.; et al. Global, regional, and national estimates of the population at increased risk of severe COVID-19 due to underlying health conditions in 2020: A modelling study. Lancet Glob. Health 2020, 8, e1003–e1017. [Google Scholar] [CrossRef]
- Sun, Z.; Di, L.; Sprigg, W.; Tong, D.; Casal, M. Community venue exposure risk estimator for the COVID-19 pandemic. Health Place 2020, 66, 102450. [Google Scholar] [CrossRef]
- Studdert, D.M.; Hall, M.A. Disease Control, Civil Liberties, and Mass Testing—Calibrating Restrictions during the Covid-19 Pandemic. N. Engl. J. Med. 2020, 383, 102–104. [Google Scholar] [CrossRef]
- Pearce, N.; Vandenbroucke, J.P.; VanderWeele, T.J.; Greenland, S. Accurate Statistics on COVID-19 Are Essential for Policy Guidance and Decisions. Am. J. Public Health 2020, 110, 949–951. [Google Scholar] [CrossRef]
- Jaya, I.G.N.M.; Folmer, H. Bayesian spatiotemporal forecasting and mapping of COVID-19 risk with application to West Java Province, Indonesia. J. Reg. Sci. 2021, 61, 849–881. [Google Scholar] [CrossRef]
- Jiang, P.; Fu, X.; Van Fan, Y.; Klemeš, J.J.; Chen, P.; Ma, S.; Zhang, W. Spatial-temporal potential exposure risk analytics and urban sustainability impacts related to COVID-19 mitigation: A perspective from car mobility behaviour. J. Clean. Prod. 2021, 279, 123673. [Google Scholar] [CrossRef]
- Li, J.; Wang, X.; He, Z.; Zhang, T. A personalized activity-based spatiotemporal risk mapping approach to the COVID-19 pandemic. Cartogr. Geogr. Inf. Sci. 2021, 48, 275–291. [Google Scholar] [CrossRef]
- Franch-Pardo, I.; Napoletano, B.M.; Rosete-Verges, F.; Billa, L. Spatial analysis and GIS in the study of COVID-19. A review. Sci. Total Environ. 2020, 739, 140033. [Google Scholar] [CrossRef]
- Zhou, C.; Su, F.; Pei, T.; Zhang, A.; Du, Y.; Luo, B.; Cao, Z.; Wang, J.; Yuan, W.; Zhu, Y.; et al. COVID-19: Challenges to GIS with Big Data. Geogr. Sustain. 2020, 1, 77–87. [Google Scholar] [CrossRef]
- Rader, B.; Scarpino, S.V.; Nande, A.; Hill, A.L.; Adlam, B.; Reiner, R.C.; Pigott, D.M.; Gutierrez, B.; Zarebski, A.E.; Shrestha, M.; et al. Crowding and the shape of COVID-19 epidemics. Nat. Med. 2020, 26, 1829–1834. [Google Scholar] [CrossRef]
- Hamidi, S.; Sabouri, S.; Ewing, R. Does Density Aggravate the COVID-19 Pandemic? Early Findings and Lessons for planners. J. Am. Plan. Assoc. 2020, 86, 495–509. [Google Scholar] [CrossRef]
- Hamidi, S.; Zandiatashbar, A. Compact development and adherence to stay-at-home order during the COVID-19 pandemic: A longitudinal investigation in the United States. Landsc. Urban Plan. 2020, 205, 103952. [Google Scholar] [CrossRef]
- Banai, R. Pandemic and the planning of resilient cities and regions. Cities 2020, 106, 102929. [Google Scholar] [CrossRef]
- Barak, N.; Sommer, U.; Mualam, N. Urban attributes and the spread of COVID-19: The effects of density, compliance and socio-political factors in Israel. Sci. Total Environ. 2021, 793, 148626. [Google Scholar] [CrossRef]
- Rocklöv, J.; Sjödin, H. High population densities catalyse the spread of COVID-19. J. Travel Med. 2020, 27, taaa038. [Google Scholar] [CrossRef]
- Han, Y.; Yang, L.; Jia, K.; Li, J.; Feng, S.; Chen, W.; Zhao, W.; Pereira, P. Spatial distribution characteristics of the COVID-19 pandemic in Beijing and its relationship with environmental factors. Sci. Total Environ. 2021, 761, 144257. [Google Scholar] [CrossRef] [PubMed]
- Mollalo, A.; Vahedi, B.; Rivera, K.M. GIS-based spatial modeling of COVID-19 incidence rate in the continental United States. Sci. Total Environ. 2020, 728, 138884. [Google Scholar] [CrossRef] [PubMed]
- Kadi, N.; Khelfaoui, M. Population density, a factor in the spread of COVID-19 in Algeria: Statistic study. Bull. Natl. Res. Cent. 2020, 44, 138. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Song, Y.; Cai, J.; Zhu, H. Population mapping in China with Tencent social user and remote sensing data. Appl. Geogr. 2021, 130, 102450. [Google Scholar] [CrossRef]
- Yao, Y.; Liu, X.; Li, X.; Zhang, J.; Liang, Z.; Mai, K.; Zhang, Y. Mapping fine-scale population distributions at the building level by integrating multisource geospatial big data. Int. J. Geogr. Inf. Sci. 2017, 31, 1220–1244. [Google Scholar] [CrossRef]
- Bouffanais, R.; Lim, S.S. Cities—Try to predict superspreading hotspots for COVID-19. Nat. Cell Biol. 2020, 583, 352–355. [Google Scholar] [CrossRef]
- Zhou, Y.; Xu, R.; Hu, D.; Yue, Y.; Li, Q.; Xia, J. Effects of human mobility restrictions on the spread of COVID-19 in Shenzhen, China: A modelling study using mobile phone data. Lancet Digit. Health 2020, 2, e417–e424. [Google Scholar] [CrossRef]
- Zhan, C.; Tse, C.K.; Fu, Y.; Lai, Z.; Zhang, H. Modeling and prediction of the 2019 coronavirus disease spreading in China incorporating human migration data. PLoS ONE 2020, 15, e0241171. [Google Scholar] [CrossRef]
- Li, Q.; Bessell, L.; Xiao, X.; Fan, C.; Gao, X.; Mostafavi, A. Disparate patterns of movements and visits to points of interest located in urban hotspots across US metropolitan cities during COVID-19. R. Soc. Open Sci. 2021, 8, 201209. [Google Scholar] [CrossRef]
- Lak, A.; Sharifi, A.; Badr, S.; Zali, A.; Maher, A.; Mostafavi, E.; Khalili, D. Spatio-temporal patterns of the COVID-19 pandemic, and place-based influential factors at the neighborhood scale in Tehran. Sustain. Cities Soc. 2021, 72, 103034. [Google Scholar] [CrossRef]
- Zhang, S.; Yang, Z.; Wang, M.; Zhang, B. “Distance-Driven” Versus “Density-Driven”: Understanding the Role of “Source-Case” Distance and Gathering Places in the Localized Spatial Clustering of COVID-19—A Case Study of the Xinfadi Market, Beijing (China). GeoHealth 2021, 5, e2021GH000458. [Google Scholar] [CrossRef]
- Prem, K.; Liu, Y.; Russell, T.W.; Kucharski, A.J.; Eggo, R.M.; Davies, N.; Jit, M.; Klepac, P.; Flasche, S.; Clifford, S.; et al. The Effect of Control Strategies to Reduce Social Mixing on Outcomes of the COVID-19 Epidemic in Wuhan, China: A Modelling Study. Lancet Public Health 2020, 5, e261–e270. [Google Scholar] [CrossRef] [Green Version]
- Davies, N.G.; Klepac, P.; Liu, Y.; Prem, K.; Jit, M.; Eggo, R.M. Age-dependent effects in the transmission and control of COVID-19 epidemics. Nat. Med. 2020, 26, 1205–1211. [Google Scholar] [CrossRef]
- Illenberger, J.; Nagel, K.; Flötteröd, G. The Role of Spatial Interaction in Social Networks. Netw. Spat. Econ. 2013, 13, 255–282. [Google Scholar] [CrossRef]
- van den Berg, P.; Kemperman, A.; Timmermans, H. Social Interaction Location Choice: A Latent Class Modeling Approach. Ann. Assoc. Am. Geogr. 2014, 104, 959–972. [Google Scholar] [CrossRef]
- Birch, C.P.D.; Oom, S.P.; Beecham, J.A. Rectangular and hexagonal grids used for observation, experiment and simulation in ecology. Ecol. Model. 2007, 206, 347–359. [Google Scholar] [CrossRef]
- Ling, C.; Wen, X. Community grid management is an important measure to contain the spread of novel coronavirus pneumonia (COVID-19). Epidemiol. Infect. 2020, 148, e167. [Google Scholar] [CrossRef]
- Li, Z.; Gao, G.F. Strengthening public health at the community-level in China. Lancet Public Health 2020, 5, e629–e630. [Google Scholar] [CrossRef]
- Schläpfer, M.; Dong, L.; O’Keeffe, K.; Santi, P.; Szell, M.; Salat, H.; Anklesaria, S.; Vazifeh, M.; Ratti, C.; West, G.B. The universal visitation law of human mobility. Nat. Cell Biol. 2021, 593, 522–527. [Google Scholar] [CrossRef]
- Luo, W.; Qi, Y. An enhanced two-step floating catchment area (E2SFCA) method for measuring spatial accessibility to primary care physicians. Health Place 2009, 15, 1100–1107. [Google Scholar] [CrossRef]
- Liu, S.; Qin, Y.; Xie, Z.; Zhang, J. The Spatio-Temporal Characteristics and Influencing Factors of Covid-19 Spread in Shenzhen, China—An Analysis Based on 417 Cases. Int. J. Environ. Res. Public Health 2020, 17, 7450. [Google Scholar] [CrossRef]
- Yao, Y.; Shi, W.; Zhang, A.; Liu, Z.; Luo, S. Examining the diffusion of coronavirus disease 2019 cases in a metropolis: A space syntax approach. Int. J. Health Geogr. 2021, 20, 17. [Google Scholar] [CrossRef]
- Carey, H.C. Principles of Social Science; JB Lippincott & Company: Philadelphia, PA, USA, 1867; Volume 3. [Google Scholar]
- Stewart, J.Q. Demographic Gravitation: Evidence and Applications. Sociometry 1948, 11, 31–58. [Google Scholar] [CrossRef]
- Flowerdew, R.; Aitkin, M. A method of fitting the gravity model based on the poisson distribution. J. Reg. Sci. 1982, 22, 191–202. [Google Scholar] [CrossRef]
- Dai, D. Black residential segregation, disparities in spatial access to health care facilities, and late-stage breast cancer diagnosis in metropolitan Detroit. Health Place 2010, 16, 1038–1052. [Google Scholar] [CrossRef]
- Luo, W.; Wang, F. Measures of Spatial Accessibility to Health Care in a GIS Environment: Synthesis and a Case Study in the Chicago Region. Environ. Plan. B Plan. Des. 2003, 30, 865–884. [Google Scholar] [CrossRef] [Green Version]
- McGrail, M.; Humphreys, J.S. Measuring spatial accessibility to primary health care services: Utilising dynamic catchment sizes. Appl. Geogr. 2014, 54, 182–188. [Google Scholar] [CrossRef]
- Liu, T.; Chai, Y. Daily life circle reconstruction: A scheme for sustainable development in urban China. Habitat Int. 2015, 50, 250–260. [Google Scholar] [CrossRef]
- Kraemer, M.U.G.; Yang, C.-H.; Gutierrez, B.; Wu, C.-H.; Klein, B.; Pigott, D.M.; Open COVID-19 Data Working Group; du Plessis, L.; Faria, N.R.; Li, R.; et al. The effect of human mobility and control measures on the COVID-19 epidemic in China. Science 2020, 368, 493–497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, L.; Du, Q.; Ren, F.; Ma, X. Assessing Spatial Accessibility to Hierarchical Urban Parks by Multi-Types of Travel Distance in Shenzhen, China. Int. J. Environ. Res. Public Health 2019, 16, 1038. [Google Scholar] [CrossRef] [Green Version]
- Shao, F.; Sui, Y.; Yu, X.; Sun, R. Spatio-temporal travel patterns of elderly people—A comparative study based on buses usage in Qingdao, China. J. Transp. Geogr. 2019, 76, 178–190. [Google Scholar] [CrossRef]
- Ministry of Education of China and Ministry of Industry and Information Technology of China. Notice of Arrangement for “Suspension of School Does Not Stop Learning” during the Postponement for the Opening of Primary and Secondary Schools. 2020. Available online: http://www.moe.gov.cn/srcsite/A06/s3321/202002/t20200212_420435.html (accessed on 12 February 2020).
- Wang, X.; Lei, S.M.; Le, S.; Yang, Y.; Zhang, B.; Yao, W.; Gao, Z.; Cheng, S. Bidirectional Influence of the COVID-19 Pandemic Lockdowns on Health Behaviors and Quality of Life among Chinese Adults. Int. J. Environ. Res. Public Health 2020, 17, 5575. [Google Scholar] [CrossRef]
- Lee, P.M.Y.; Huang, B.; Liao, G.; Chan, C.K.; Tai, L.-B.; Tsang, C.Y.J.; Leung, C.C.; Kwan, M.-P.; Tse, L.A. Changes in physical activity and rest-activity circadian rhythm among Hong Kong community aged population before and during COVID-19. BMC Public Health 2021, 21, 836. [Google Scholar] [CrossRef]
- Sun, X.; Lucas, H.; Meng, Q.; Zhang, Y. Associations between living arrangements and health-related quality of life of urban elderly people: A study from China. Qual. Life Res. 2011, 20, 359–369. [Google Scholar] [CrossRef]
- Xu, Y.; Zhou, D.; Liu, K. Research on The Elderly Space-time Behavior Visualization and Community Healthy Livable Environment. Archit. J. 2019, S1, 90–95. [Google Scholar]
- Liu, S.; Wang, Y.; Zhou, D.; Kang, Y. Two-Step Floating Catchment Area Model-Based Evaluation of Community Care Facilities’ Spatial Accessibility in Xi’an, China. Int. J. Environ. Res. Public Health 2020, 17, 5086. [Google Scholar] [CrossRef]
- Wang, Z.; Gao, G.; Liu, X.; Lyu, W. Verification and Analysis of Traffic Evaluation Indicators in Urban Transportation System Planning Based on Multi-Source Data–A Case Study of Qingdao City, China. IEEE Access 2019, 7, 110103–110115. [Google Scholar] [CrossRef]
- Brunsdon, C.; Fotheringham, S.; Charlton, M. Geographically Weighted Regression. J. R. Stat. Soc. Ser. D 1998, 47, 431–443. [Google Scholar] [CrossRef]
- Huang, B.; Wu, B.; Barry, M. Geographically and temporally weighted regression for modeling spatio-temporal variation in house prices. Int. J. Geogr. Inf. Sci. 2010, 24, 383–401. [Google Scholar] [CrossRef]
- Wang, H.; Wang, J.; Huang, B. Prediction for spatio-temporal models with autoregression in errors. J. Nonparametric Stat. 2012, 24, 217–244. [Google Scholar] [CrossRef]
- Wu, B.; Li, R.; Huang, B. A geographically and temporally weighted autoregressive model with application to housing prices. Int. J. Geogr. Inf. Sci. 2014, 28, 1186–1204. [Google Scholar] [CrossRef]
- Ge, L.; Zhao, Y.; Sheng, Z.; Wang, N.; Zhou, K.; Mu, X.; Guo, L.; Wang, T.; Yang, Z.; Huo, X. Construction of a Seasonal Difference-Geographically and Temporally Weighted Regression (SD-GTWR) Model and Comparative Analysis with GWR-Based Models for Hemorrhagic Fever with Renal Syndrome (HFRS) in Hubei Province (China). Int. J. Environ. Res. Public Health 2016, 13, 1062. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Chen, M.; Huang, B.; Wu, C.; Shi, W. Modeling the Spatiotemporal Association Between COVID-19 Transmission and Population Mobility Using Geographically and Temporally Weighted Regression. GeoHealth 2021, 5. [Google Scholar] [CrossRef]
- Burnham, K.P.; Anderson, D.R. Multimodel Inference: Understanding AIC and BIC in Model Selection. Sociol. Methods Res. 2004, 33, 261–304. [Google Scholar] [CrossRef]
- Wu, S.-S.; Zhuang, Y.; Chen, J.; Wang, W.; Bai, Y.; Lo, S.-M. Rethinking bus-to-metro accessibility in new town development: Case studies in Shanghai. Cities 2019, 94, 211–224. [Google Scholar] [CrossRef]
- Zhao, P.; Wan, J. Land use and travel burden of residents in urban fringe and rural areas: An evaluation of urban-rural integration initiatives in Beijing. Land Use Policy 2021, 103, 105309. [Google Scholar] [CrossRef]
- Matthews, K.A.; Ullrich, F.; Gaglioti, A.H.; Dugan, S.; Chen, M.S.; Hall, D.M. Nonmetropolitan COVID-19 Incidence and Mortality Rates Surpassed Metropolitan Rates Within the First 24 Weeks of the Pandemic Declaration: United States, March 1–October 18, 2020. J. Rural Health 2021, 37, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.; Lin, Q.; Ran, J.; Musa, S.S.; Yang, G.; Wang, W.; Lou, Y.; Gao, D.; Yang, L.; He, D.; et al. Preliminary estimation of the basic reproduction number of novel coronavirus (2019-nCoV) in China, from 2019 to 2020: A data-driven analysis in the early phase of the outbreak. Int. J. Infect. Dis. 2020, 92, 214–217. [Google Scholar] [CrossRef] [Green Version]
- Alberti, T.; Faranda, D. On the uncertainty of real-time predictions of epidemic growths: A COVID-19 case study for China and Italy. Commun. Nonlinear Sci. Numer. Simul. 2020, 90, 105372. [Google Scholar] [CrossRef]
- Neuberger, A.; Paul, M.; Nizar, A.; Raoult, D. Modelling in infectious diseases: Between haphazard and hazard. Clin. Microbiol. Infect. 2013, 19, 993–998. [Google Scholar] [CrossRef] [Green Version]
- House, T.; Keeling, M.J. Epidemic prediction and control in clustered populations. J. Theor. Biol. 2011, 272, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Anirudh, A. Mathematical modeling and the transmission dynamics in predicting the Covid-19—What next in combating the pandemic. Infect. Dis. Model. 2020, 5, 366–374. [Google Scholar] [CrossRef]
- Caruso, B.A.; Freeman, M.C. Shared sanitation and the spread of COVID-19: Risks and next steps. Lancet Planet. Health 2020, 4, E173. [Google Scholar] [CrossRef]
- Courtemanche, C.; Garuccio, J.; Le, A.; Pinkston, J.; Yelowitz, A. Strong Social Distancing Measures in the United States Reduced The COVID-19 Growth Rate. Health Aff. 2020, 39, 1237–1246. [Google Scholar] [CrossRef]
- Chu, D.K.; Akl, E.A.; Duda, S.; Solo, K.; Yaacoub, S.; Schünemann, H.J.; EI-harakeh, A.; Bognanni, A.; Lotfi, T.; Loeb, M.; et al. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: A systematic review and meta-analysis. Lancet 2020, 395, 1973–1987. [Google Scholar] [CrossRef]
- Bambra, C.; Riordan, R.; Ford, J.; Matthews, F. The COVID-19 pandemic and health inequalities. J. Epidemiol. Community Health 2020, 74, 964–968. [Google Scholar] [CrossRef]
- Sasikumar, K.; Nath, D.; Nath, R.; Chen, W. Impact of Extreme Hot Climate on COVID-19 Outbreak in India. GeoHealth 2020, 4, e2020GH000305. [Google Scholar] [CrossRef]
- Menebo, M.M. Temperature and precipitation associate with Covid-19 new daily cases: A correlation study between weather and Covid-19 pandemic in Oslo, Norway. Sci. Total Environ. 2020, 737, 139659. [Google Scholar] [CrossRef]
- Qi, H.; Xiao, S.; Shi, R.; Ward, M.P.; Chen, Y.; Tu, W.; Su, Q.; Wang, W.; Wang, X.; Zhang, Z. COVID-19 transmission in Mainland China is associated with temperature and humidity: A time-series analysis. Sci. Total Environ. 2020, 728, 138778. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Trip Mode | Road Classification | Speed (km/h) |
|---|---|---|
| Walk | Footway, Living Street, Path, Pedestrian, Residential, Service, Steps | 5 |
| Drive | Tertiary/Unclassified/Secondary/Primary/Trunk | 10/20/30/40/50 |
| Variables | Characteristic | Mean | Std. Dev. | Min | Max | VIF | |
|---|---|---|---|---|---|---|---|
| Dependent variable | Covid risk | Dynamic | 0.06 | 0.13 | 0 | 1.37 | - |
| Independent variables | Facility density (FD) | ||||||
| Catering | Static | 0.75 | 2.43 | 0 | 36 | 1.92 | |
| Residences | Static | 2.24 | 3.33 | 0 | 26 | 1.62 | |
| Shopping | Static | 1.55 | 5.05 | 0 | 80 | 1.97 | |
| Public services | Static | 0.88 | 1.76 | 0 | 13 | 2.03 | |
| Health-care | Static | 0.86 | 1.95 | 0 | 22 | 1.38 | |
| Facility attractiveness (FA) | |||||||
| Catering | Static | 0.62 | 2.05 | 0 | 30.77 | 1.94 | |
| Residences | Static | 1.83 | 2.81 | 0 | 22.18 | 1.67 | |
| Shopping | Static | 1.29 | 4.30 | 0 | 68.38 | 1.98 | |
| Public services | Static | 0.72 | 1.47 | 0 | 11.25 | 2.07 | |
| Health-care | Static | 0.71 | 1.62 | 0 | 18.78 | 1.39 | |
| Diagnostic Information | Facility Density (FD) | Facility Attractiveness (FA) | ||||||
|---|---|---|---|---|---|---|---|---|
| OLS | TWR | GWR | GTWR | OLS | TWR | GWR | GTWR | |
| Adjusted R2 | 0.0827 | 0.1594 | 0.4036 | 0.5159 | 0.0804 | 0.1555 | 0.4078 | 0.5694 |
| Residual sum of squares | 124.84 | 114.35 | 81.13 | 65.86 | 125.15 | 114.88 | 80.56 | 58.57 |
| AICc | −11,553 | −12,258 | −15,080 | −16,813 | −11,531 | −12,219 | −15,144 | −17,690 |
| Variables | Facility Density (FD) | Facility Attractiveness (FA) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Min | LQ | Med | UQ | Max | Min | LQ | Med | UQ | Max | |
| Catering | −10.57 | −0.72 | 0.7 | 1.32 | 10.22 | −18.33 | −4.62 | 0.4 | 2.79 | 38.7 |
| Residence | −63.57 | −6.82 | −2.61 | 0.07 | 4.73 | −7.63 | 0.87 | 3.39 | 7.22 | 25.9 |
| Shopping | −3.21 | −0.48 | 0.11 | 0.76 | 9.72 | −4.77 | 0.02 | 1.71 | 3.79 | 11.15 |
| Public service | −16.6 | −3.9 | −1.44 | −0.13 | 3.37 | −11.23 | −2.33 | 1.1 | 5.86 | 29.24 |
| Health-care | −19.71 | −2.4 | −0.57 | 1.11 | 6.21 | −1.41 | 2.49 | 5.2 | 9.61 | 40.35 |
| Constant | 0 | 0.02 | 0.04 | 0.09 | 0.53 | 0 | 0.01 | 0.03 | 0.07 | 0.42 |
| Epidemic Stage | Adjusted R2 | Improvement Rate | |
|---|---|---|---|
| Facility Density (FD) | Facility Attractiveness (FA) | ||
| Stage 1 | 0.3847 | 0.4808 | 24.99% |
| Stage 2 | 0.4190 | 0.4747 | 13.28% |
| Stage 3 | 0.5039 | 0.5629 | 11.72% |
| Stage 4 | 0.4950 | 0.5669 | 14.51% |
| Stage 5 | 0.5532 | 0.6179 | 11.70% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, S.; Wang, M.; Yang, Z.; Zhang, B. A Novel Predictor for Micro-Scale COVID-19 Risk Modeling: An Empirical Study from a Spatiotemporal Perspective. Int. J. Environ. Res. Public Health 2021, 18, 13294. https://doi.org/10.3390/ijerph182413294
Zhang S, Wang M, Yang Z, Zhang B. A Novel Predictor for Micro-Scale COVID-19 Risk Modeling: An Empirical Study from a Spatiotemporal Perspective. International Journal of Environmental Research and Public Health. 2021; 18(24):13294. https://doi.org/10.3390/ijerph182413294
Chicago/Turabian StyleZhang, Sui, Minghao Wang, Zhao Yang, and Baolei Zhang. 2021. "A Novel Predictor for Micro-Scale COVID-19 Risk Modeling: An Empirical Study from a Spatiotemporal Perspective" International Journal of Environmental Research and Public Health 18, no. 24: 13294. https://doi.org/10.3390/ijerph182413294
APA StyleZhang, S., Wang, M., Yang, Z., & Zhang, B. (2021). A Novel Predictor for Micro-Scale COVID-19 Risk Modeling: An Empirical Study from a Spatiotemporal Perspective. International Journal of Environmental Research and Public Health, 18(24), 13294. https://doi.org/10.3390/ijerph182413294