
Co-Creating an Occupational Health Intervention within the Construction Industry in Sweden: Stakeholder Perceptions of the Process and Output

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting and Design
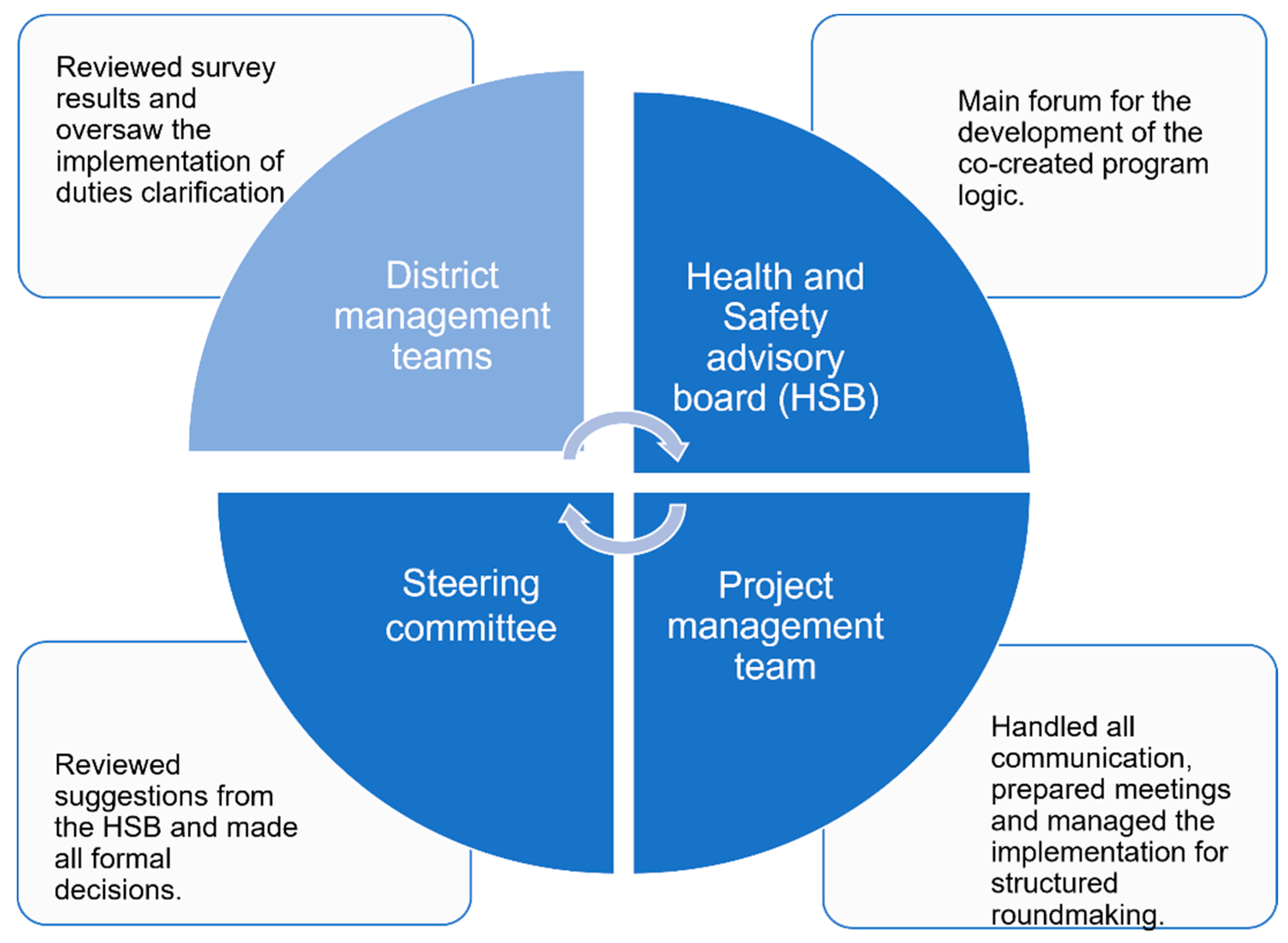
2.2. The Co-Creation
2.3. Participants for the Interviews for the Research Study
2.4. Data Collection
2.5. Data Analysis
3. Results
3.1. Building Awareness about the Organization
3.1.1. Improved Understanding of the Mental Health Status and Organizational Values
“One thing I take with me is that my company is actually investing in these matters (mental health). It is valuable to see that there is actually an ongoing work within the company, and even higher up in the chain, they take these matters seriously and engage in what we are going to work with. So, it feels good.”Safety representative (6)
3.1.2. Increased Learning about the Psychosocial Work Environment and Stress
“So, the region has gotten a lot out of this (the project) I would say, and we as individuals have got a language, we had never used the word role clarity before, but I have done so now. Yes, so we have learned and gotten a lot out of this.”Manager CCF/GF (12)
3.2. Enabling a Satisfying Co-Creation Process
3.2.1. Good Partner Fit
“We have tried to take responsibility and we have, among other things, influenced the questionnaire in a way which suited us. So, we have felt an ownership, I hope not too much.”Manager CCF/GF (5)
3.2.2. Building on Existing Formal Structures
3.2.3. Well-Structured and Responsive Collaboration
3.3. Tailoring of Intervention Activities and Implementation Strategies into the Context
3.3.1. Performance and Health in Tandem
“I absolutely think that the intervention activities are fully relevant to work with, and I think it will lead to, well…better structure in the projects, which I think leads to better mental health as well.”Manager CCF/GF (2)
3.3.2. Dig Where You Stand
“But I have faith in the model (implementation support) that we select projects which are at the right stage (of production) and that we coach them based on their goals rather than sending individuals on a course and then they should come back and change something. That´s what I believe in”.Manager CCF/GF (5)
4. Discussion
4.1. Strengths and Limitations
4.2. Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Niedhammer, I.; Bertrais, S.; Witt, K. Psychosocial work exposures and health outcomes: A meta-review of 72 literature reviews with meta-analysis. Scand. J. Work. Environ. Health 2021, 47, 489–508. [Google Scholar] [CrossRef] [PubMed]
- Harvey, S.B.; Modini, M.; Joyce, S.; Milligan-Saville, J.S.; Tan, L.; Mykletun, A.; Bryant, R.A.; Christensen, H.; Mitchell, P.B. Can work make you mentally ill? A systematic meta-review of work-related risk factors for common mental health problems. Occup. Environ. Med. 2017, 74, 301–310. [Google Scholar] [CrossRef]
- Ruotsalainen, J.H.; Verbeek, J.H.; Mariné, A.; Serra, C. Preventing occupational stress in healthcare workers. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef]
- Montano, D.; Hoven, H.; Siegrist, J. Effects of organisational-level interventions at work on employees’ health: A systematic review. BMC Public Health 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richardson, K.M.; Rothstein, H.R. Effects of occupational stress management intervention programs: A meta-analysis. J. Occup. Health Psychol. 2008, 13, 69. [Google Scholar] [CrossRef] [PubMed]
- Schelvis, R.M.; Wiezer, N.M.; Van der Beek, A.J.; Twisk, J.W.; Bohlmeijer, E.T.; Hengel, K. The effect of an organizational level participatory intervention in secondary vocational education on work-related health outcomes: Results of a controlled trial. BMC Public Health 2017, 17, 141. [Google Scholar] [CrossRef] [Green Version]
- Arapovic-Johansson, B.; Jensen, I.; Wahlin, C.; Bjorklund, C.; Kwak, L. Process Evaluation of a Participative Organizational Intervention as a Stress Preventive Intervention for Employees in Swedish Primary Health Care. Int. J. Environ. Res. Public Health 2020, 17, 7285. [Google Scholar] [CrossRef]
- Murta, S.G.; Sanderson, K.; Oldenburg, B. Process evaluation in occupational stress management programs: A systematic review. Am. J. Health Promot. 2007, 21, 248–254. [Google Scholar] [CrossRef]
- Nielsen, K.; Randall, R. Opening the black box: Presenting a model for evaluating organizational-level interventions. Eur. J. Work Org. Psychol. 2013, 22, 601–617. [Google Scholar] [CrossRef]
- Moore, G.F.; Evans, R.E. What theory, for whom and in which context? Reflections on the application of theory in the development and evaluation of complex population health interventions. SSM Popul. Health 2017, 3, 132–135. [Google Scholar] [CrossRef] [PubMed]
- Randall, R.; Nielsen, K.; Tvedt, S.D. The development of five scales to measure employees’ appraisals of organizational-level stress management interventions. Work Stress 2009, 23, 1–23. [Google Scholar] [CrossRef]
- Billsten, J.; Fridell, M.; Holmberg, R.; Ivarsson, A. Organizational Readiness for Change (ORC) test used in the implementation of assessment instruments and treatment methods in a Swedish National study. J. Subst. Abuse Treat. 2018, 84, 9–16. [Google Scholar] [CrossRef]
- Zamenopoulos, T.; Alexiou, K. Co-Design as Collaborative Research. In Connected Communities Foundation Series; University of Bristol/AHRC Connected Communities Programme Bristol: Bristol, UK, 2018. [Google Scholar]
- Schwarz, U.V.; Nielsen, K.; Edwards, K.; Hasson, H.; Ipsen, C.; Savage, C.; Abildgaard, J.S.; Richter, A.; Lornudd, C.; Mazzocato, P.; et al. How to design, implement and evaluate organizational interventions for maximum impact: The Sigtuna Principles. Eur. J. Work Org. Psychol. 2021, 30, 415–427. [Google Scholar] [CrossRef] [PubMed]
- Leask, C.F.; Sandlund, M.; Skelton, D.A.; Altenburg, T.M.; Cardon, G.; Chinapaw, M.J.M.; de Bourdeaudhuij, I.; Verloigne, M.; Chastin, S.F.M. Framework, principles and recommendations for utilising participatory methodologies in the co-creation and evaluation of public health interventions. Res. Involv. Engagem. 2019, 5, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Jagosh, J.; Macaulay, A.C.; Pluye, P.; Salsberg, J.; Bush, P.L.; Henderson, J.; Sirett, E.; Wong, G.; Cargo, M.; Herbert, C.P.; et al. Uncovering the Benefits of Participatory Research: Implications of a Realist Review for Health Research and Practice. Milbank Q. 2012, 90, 311–346. [Google Scholar] [CrossRef] [Green Version]
- Weiner, B.J.; Amick, H.; Lee, S.-Y.D. Review: Conceptualization and Measurement of Organizational Readiness for Change: A Review of the Literature in Health Services Research and Other Fields. Med. Care Res. Rev. 2008, 65, 379–436. [Google Scholar] [CrossRef] [PubMed]
- Weiner, B.J. A theory of organizational readiness for change. Implement. Sci. 2009, 4, 67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Redman, S.; Greenhalgh, T.; Adedokun, L.; Staniszewska, S.; Denegri, S. Co-production of knowledge: The future. BMJ 2021, 372, n434. [Google Scholar] [CrossRef]
- Goodyear-Smith, F.; Jackson, C.; Greenhalgh, T. Co-design and implementation research: Challenges and solutions for ethics committees. BMC Med. Ethics 2015, 16, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Ward, M.E.; De Brún, A.; Beirne, D.; Conway, C.; Cunningham, U.; English, A.; Fitzsimons, J.; Furlong, E.; Kane, Y.; Kelly, A.; et al. Using Co-Design to Develop a Collective Leadership Intervention for Healthcare Teams to Improve Safety Culture. Int. J. Environ. Res. Public Health 2018, 15, 1182. [Google Scholar] [CrossRef] [Green Version]
- Wolfenden, L.; Yoong, S.L. Workplace wellness programmes to improve health. Lancet Public Health 2021, 6, e625. [Google Scholar] [CrossRef]
- Voorberg, W.H.; Bekkers, V.; Tummers, L.G. A Systematic Review of Co-Creation and Co-Production: Embarking on the social innovation journey. Public Manag. Rev. 2015, 17, 1333–1357. [Google Scholar] [CrossRef] [Green Version]
- Abildgaard, J.S.; Hasson, H.; Schwarz, U.V.; Lovseth, L.T.; Ala-Laurinaho, A.; Nielsen, K. Forms of participation: The development and application of a conceptual model of participation in work environment interventions. Econ. Ind. Democr. 2018, 41, 746–769. [Google Scholar] [CrossRef] [Green Version]
- Fox, K.E.; Johnson, S.T.; Berkman, L.F.; Sianoja, M.; Soh, Y.; Kubzansky, L.D.; Kelly, E.L. Organisational- and group-level workplace interventions and their effect on multiple domains of worker well-being: A systematic review. Work Stress 2021, 1–30. [Google Scholar] [CrossRef]
- Nielsen, K.; Randall, R. The importance of employee participation and perceptions of changes in procedures in a teamworking intervention. Work Stress 2012, 26, 91–111. [Google Scholar] [CrossRef] [Green Version]
- Ravalier, J.M.; Wainwright, E.; Smyth, N.; Clabburn, O.; Wegrzynek, P.; Loon, M. Co-Creating and Evaluating an App-Based Well-Being Intervention: The HOW (Healthier Outcomes at Work) Social Work Project. Int. J. Environ. Res. Public Health 2020, 17, 8730. [Google Scholar] [CrossRef]
- Cedstrand, E.; Nyberg, A.; Bodin, T.; Augustsson, H.; Johansson, G. Study protocol of a co-created primary organizational-level intervention with the aim to improve organizational and social working conditions and decrease stress within the construction industry—A controlled trial. BMC Public Health 2020, 20, 424. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [Green Version]
- Gould, G.S.; Bar-Zeev, Y.; Bovill, M.; Atkins, L.; Gruppetta, M.; Clarke, M.J.; Bonevski, B. Designing an implementation intervention with the Behaviour Change Wheel for health provider smoking cessation care for Australian Indigenous pregnant women. Implement. Sci. 2017, 12, 114. [Google Scholar] [CrossRef] [Green Version]
- Michie, S.; Whittington, C.; Hamoudi, Z.; Zarnani, F.; Tober, G.; West, R. Identification of behaviour change techniques to reduce excessive alcohol consumption. Addiction 2012, 107, 1431–1440. [Google Scholar] [CrossRef]
- Powell, B.J.; Waltz, T.J.; Chinman, M.J.; Damschroder, L.J.; Smith, J.L.; Matthieu, M.M.; Proctor, E.K.; Kirchner, J.E. A refined compilation of implementation strategies: Results from the Expert Recommendations for Implementing Change (ERIC) project. Implement. Sci. 2015, 10, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Braun, V.; Clarke, V. Reflecting on reflexive thematic analysis. Qual. Res. Sport Exerc. Health 2019, 11, 589–597. [Google Scholar] [CrossRef]
- Schwarz, U.V.; Augustsson, H.; Hasson, H.; Stenfors-Hayes, T. Promoting Employee Health by Integrating Health Protection, Health Promotion, and Continuous Improvement A Longitudinal Quasi-Experimental Intervention Study. J. Occup. Environ. Med. 2015, 57, 217–225. [Google Scholar] [CrossRef]
- Gupta, N.; Wåhlin-Jacobsen, C.D.; Abildgaard, J.S.; Henriksen, L.N.; Nielsen, K.; Holtermann, A. Effectiveness of a participatory physical and psychosocial intervention to balance the demands and resources of industrial workers: A cluster-randomized controlled trial. Scand. J. Work Environ. Health 2018, 44, 58–68. [Google Scholar] [CrossRef] [Green Version]
- Cedstrand, E.; Nyberg, A.; Sanchez-Bengtsson, S.; Alderling, M.; Augustsson, H.; Bodin, T.; Molsted Alvesson, H.; Johansson, G. A Participatory Intervention to Improve the Psychosocial Work Environment and Mental Health in Human Service Organisations. A Mixed Methods Evaluation Study. Int. J. Environ. Res. Public Health 2021, 18, 3546. [Google Scholar] [CrossRef]
- Pallesen, K.S.; Rogers, L.; Anjara, S.; De Brún, A.; McAuliffe, E. A qualitative evaluation of participants’ experiences of using co-design to develop a collective leadership educational intervention for health-care teams. Health Expect. 2020, 23, 358–367. [Google Scholar] [CrossRef] [Green Version]
- von Thiele Schwarz, U.; Richter, A.; Hasson, H. Getting everyone on the same page: Cocreated program logic (COP). In Organizational Interventions for Health and Well-Being; Nielsen, K., Noblet, A., Eds.; Routledge: Oxfordshire, UK, 2018; pp. 58–83. [Google Scholar]
- Peñalvo, J.L.; Sagastume, D.; Mertens, E.; Uzhova, I.; Smith, J.; Wu, J.H.Y.; Bishop, E.; Onopa, J.; Shi, P.; Micha, R.; et al. Effectiveness of workplace wellness programmes for dietary habits, overweight, and cardiometabolic health: A systematic review and meta-analysis. Lancet Public Health 2021, 6, e648–e660. [Google Scholar] [CrossRef]
- Mellor, N.; Mackay, C.; Packham, C.; Jones, R.; Palferman, D.; Webster, S.; Kelly, P. ‘Management standards’ and work-related stress in Great Britain: Progress on their implementation. Saf. Sci. 2011, 49, 1040–1046. [Google Scholar] [CrossRef]
- Podsakoff, P.M.; MacKenzie, S.B.; Lee, J.Y.; Podsakoff, N.P. Common method biases in behavioral research: A critical review of the literature and recommended remedies. J. Appl. Psychol. 2003, 88, 879–903. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Activity | 2019 | 2020 | 2021 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Q2 | Q3 | Q4 | Q1 | Q2 | Q3 | Q4 | Q1 | Q2 | Q3 | Q4 | |
| Meetings Health and Safety Advisory Board | 1 | 2 | 2 | 1 | 1 | 1 | |||||
| Meetings Highest management team | 1 | 2 | 2 | 1 | 1 | 1 | |||||
| Meetings Project management team | 2 | 1 | 1 | 1 | 1 | 1 | 1 | ||||
| Needs assessment Interviews with employees and managers from all levels to inform the survey. | 25 | ||||||||||
| Survey Questionnaire on psychosocial work factors and stress. | NA | B | Fu | Fu | |||||||
| Feedback meetings Results from the surveys, District management teams | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 2 | 2 | 2 | |
| Interviews First-line managers and safety representatives | 10 | ||||||||||
| Implementation support meetings Production Academy (4 projects) | 2 | 1 | 1 | ||||||||
| Participant | Professional Role | Group Affiliation in the Co-Creation Project (Figure 1) |
|---|---|---|
| 1 | Core Corporate Functions and Group Functions (CCF/GF). | Project management team, HSB 1 |
| 2 | Manager CCF/GF. | Project management team, HSB |
| 3 | Safety representative | HSB |
| 4 | Safety representative | HSB |
| 5 | Manager CCF/GF. | Project management team, HSB |
| 6 | Safety representative | HSB |
| 7 | Manager production | HSB |
| 8 | Manager production | Highest management team |
| 9 | Manager production | Highest management team |
| 10 | CCF/GF. | HSB |
| 11 | CCF/GF. | HSB |
| 12 | Manager CCF/GF. | Project management team, HSB |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cedstrand, E.; Mølsted Alvesson, H.; Augustsson, H.; Bodin, T.; Bodin, E.; Nyberg, A.; Johansson, G. Co-Creating an Occupational Health Intervention within the Construction Industry in Sweden: Stakeholder Perceptions of the Process and Output. Int. J. Environ. Res. Public Health 2021, 18, 12872. https://doi.org/10.3390/ijerph182412872
Cedstrand E, Mølsted Alvesson H, Augustsson H, Bodin T, Bodin E, Nyberg A, Johansson G. Co-Creating an Occupational Health Intervention within the Construction Industry in Sweden: Stakeholder Perceptions of the Process and Output. International Journal of Environmental Research and Public Health. 2021; 18(24):12872. https://doi.org/10.3390/ijerph182412872
Chicago/Turabian StyleCedstrand, Emma, Helle Mølsted Alvesson, Hanna Augustsson, Theo Bodin, Erika Bodin, Anna Nyberg, and Gun Johansson. 2021. "Co-Creating an Occupational Health Intervention within the Construction Industry in Sweden: Stakeholder Perceptions of the Process and Output" International Journal of Environmental Research and Public Health 18, no. 24: 12872. https://doi.org/10.3390/ijerph182412872
APA StyleCedstrand, E., Mølsted Alvesson, H., Augustsson, H., Bodin, T., Bodin, E., Nyberg, A., & Johansson, G. (2021). Co-Creating an Occupational Health Intervention within the Construction Industry in Sweden: Stakeholder Perceptions of the Process and Output. International Journal of Environmental Research and Public Health, 18(24), 12872. https://doi.org/10.3390/ijerph182412872