
Patient-Reported Questionnaires to Identify Adverse Drug Reactions: A Systematic Review

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
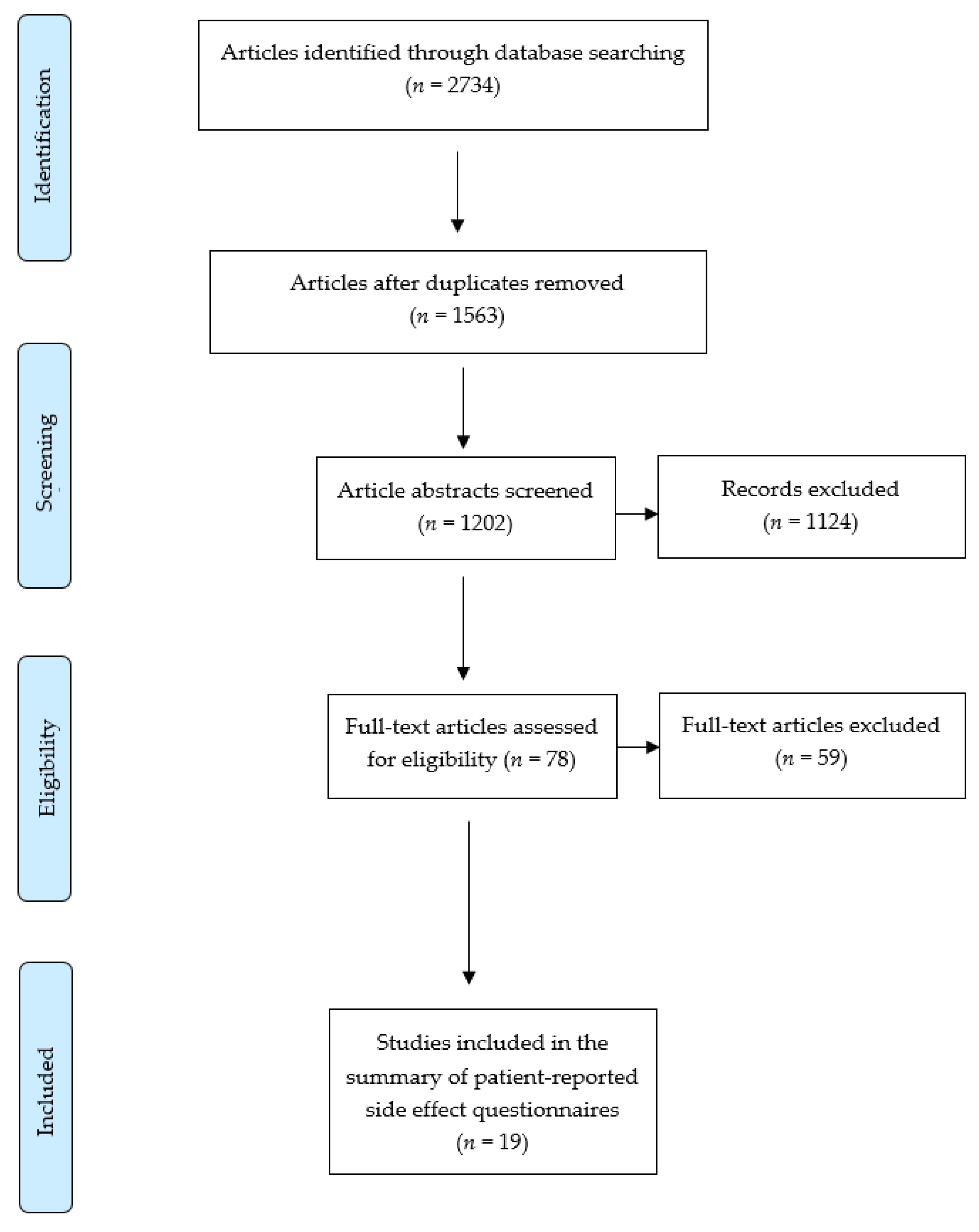
2.1. Search Strategy and Study Selection
2.2. Data Extraction
2.3. Assessment of Methodological Quality
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Medication without Harm: WHO Global Patient Safety Challenge; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Pharmaceutical Society of Australia. Medicine Safety: Take Care; Pharmaceutical Society of Australia: Canberra, Australia, 2019. [Google Scholar]
- Edwards, I.R.; Aronson, J.K. Adverse drug reactions: Definitions, diagnosis, and management. Lancet 2000, 356, 1255–1259. [Google Scholar] [CrossRef]
- Insani, W.N.; Whittlesea, C.; Alwafi, H.; Man, K.K.C.; Chapman, S.; Wei, L. Prevalence of adverse drug reactions in the primary care setting: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0252161. [Google Scholar] [CrossRef]
- Pharmacy Programs Administrator. Home Medicines Review. 2018. Available online: https://www.ppaonline.com.au/programs/medication-management-programs/home-medicines-review (accessed on 30 August 2021).
- Tarn, D.M.; Wenger, A.; Good, J.S.; Hoffing, M.; Scherger, J.E.; Wenger, N.S. Do physicians communicate the adverse effects of medications that older patients want to hear? Drugs Ther. Perspect. 2015, 31, 68–76. [Google Scholar] [CrossRef][Green Version]
- Jarernsiripornkul, N.; Krska, J.; Capps, P.A.G.; Richards, R.M.E.; Lee, A. Patient reporting of potential adverse drug reactions: A methodological study. Br. J. Clin. Pharmacol. 2002, 53, 318–325. [Google Scholar] [CrossRef]
- Caughey, G.E.; Tait, K.; Vitry, A.I.; Shakib, S. Influence of medication risks and benefits on treatment preferences in older patients with multimorbidity. Patient Prefer. Adherence 2017, 11, 131–140. [Google Scholar] [CrossRef] [PubMed]
- Vallano, A.; Cereza, G.; Pedròs, C.; Agustí, A.; Danés, I.; Aguilera, C.; Arnau, J.M. Obstacles and solutions for spontaneous reporting of adverse drug reactions in the hospital. Br. J. Clin. Pharm. 2005, 60, 653–658. [Google Scholar] [CrossRef] [PubMed]
- Cheema, E.; Haseeb, A.; Khan, T.M.; Sutcliffe, P.; Singer, D.R. Barriers to reporting of adverse drugs reactions: A cross sectional study among community pharmacists in United Kingdom. Pharm. Pract. 2017, 15, 931. [Google Scholar] [CrossRef] [PubMed]
- Hughes, M.L.; Weiss, M. Adverse drug reaction reporting by community pharmacists-The barriers and facilitators. Pharm. Drug Saf. 2019, 28, 1552–1559. [Google Scholar] [CrossRef]
- Irving, G.; Neves, A.L.; Dambha-Miller, H.; Oishi, A.; Tagashira, H.; Verho, A.; Holden, J. International variations in primary care physician consultation time: A systematic review of 67 countries. BMJ Open 2017, 7, e017902. [Google Scholar] [CrossRef]
- World Health Organization. Adherence to Long Term Therapies: Evidence for Action; World Health Organization: Geneva, Switerland, 2003. [Google Scholar]
- Foster, J.M.; van der Molen, T.; Caeser, M.; Hannaford, P. The use of questionnaires for measuring patient-reported side effects of drug: Its importance and methodological challenges. Pharmacoepidemiol. Drug Saf. 2008, 17, 278–296. [Google Scholar] [CrossRef]
- Wykes, T.; Evans, J.; Paton, C.; Barnes, T.R.E.; Taylor, D.; Bentall, R.; Dalton, B.; Ruffell, T.; Rose, D.; Vitoratou, S. What side effects are problematic for patients prescribed antipsychotic medication? The Maudsley Side Effects (MSE) measure for antipsychotic medication. Psychol. Med. 2017, 47, 2369–2378. [Google Scholar] [CrossRef] [PubMed]
- De Vries, S.T.; Mol, P.G.M.; De Zeeuw, D.; Haaijer-Ruskamp, F.M.; Denig, P. Development and Initial Validation of a Patient-Reported Adverse Drug Event Questionnaire. Drug Saf. 2013, 36, 765–777. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Covidence Systematic Review Software, Veritas Health Innovation, Melbourne, Australia. Available online: www.covidence.org (accessed on 7 June 2020).
- Australian Institute of Health and Welfare. Chronic Disease. Available online: https://www.aihw.gov.au/reports-data/health-conditions-disability-deaths/chronic-disease/overview (accessed on 7 June 2020).
- World Health Organization. Noncommunicable Diseases. 2021. Available online: https://www.who.int/health-topics/noncommunicable-diseases#tab=tab_1 (accessed on 12 August 2021).
- Souza, A.C.; Alexandre, N.M.C.; Guirardello, E.B. Psychometric properties in instruments evaluation of reliability and validity. Epidemiol. E Serv. De Saude Rev. Do Sist. Unico De Saude Do Bras. 2017, 26, 649–659. [Google Scholar] [CrossRef]
- Fayers, P.M.; Machin, D. Scores and measurements: Validity, reliability, sensitivity. In Quality of life: The Assessment, Analysis and Interpretation of Patient-Reported Outcomes, 2nd ed.; John Wiley & Sons Ltd: Chichester, UK, 2007; pp. 77–108. [Google Scholar]
- Cronbach, L.J. Coefficient alpha and the internal structure of tests. Psychometrika 1951, 16, 297–334. [Google Scholar] [CrossRef]
- Deyo, R.A.; Diehr, P.; Patrick, D.L. Reproducibility and responsiveness of health status measures. Statistics and strategies for evaluation. Control Clin. Trials 1991, 12, 142s–158s. [Google Scholar] [CrossRef]
- Mokkink, L.B.; de Vet, H.C.W.; Prinsen, C.A.C.; Patrick, D.L.; Alonso, J.; Bouter, L.M.; Terwee, C.B. COSMIN Risk of Bias checklist for systematic reviews of Patient-Reported Outcome Measures. Qual. Life Res. 2018, 27, 1171–1179. [Google Scholar] [CrossRef] [PubMed]
- Ashoorian, D.M.; Davidson, R.M.; Rock, D.J.T.; Seubert, L.J.; Clifford, R.M. Development of the My Medicines and Me (M3Q) side effect questionnaire for mental health patients: A qualitative study. Ther. Adv. Psychopharmacol. 2015, 5, 289–303. [Google Scholar] [CrossRef]
- Atkinson, M.J.; Sinha, A.; Hass, S.L.; Colman, S.S.; Kumar, R.N.; Brod, M.; Rowland, C.R. Validation of a general measure of treatment satisfaction, the Treatment Satisfaction Questionnaire for Medication (TSQM), using a national panel study of chronic disease. Health Qual. Life Outcomes 2004, 2, 12. [Google Scholar] [CrossRef]
- Campbell, J.L.; Kiebert, G.M.; Partridge, M.R. Development of the satisfaction with inhaled asthma treatment questionnaire. Eur. Respir. J. 2003, 22, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Carpay, J.A.; Aldenkamp, A.P.; van Donselaar, C.A. Complaints associated with the use of antiepileptic drugs: Results from a community-based study. Seizure 2005, 14, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Dott, S.G.; Weiden, P.; Hopwood, P.; Awad, A.G.; Hellewell, J.S.E.; Knesevich, J.; Kopala, L.; Miller, A.; Salzman, C. An innovative approach to clinical communication in schizophrenia: The Approaches to Schizophrenia Communication checklists. CNS Spectr. 2001, 6, 333–338. [Google Scholar] [CrossRef]
- Feleppa, M.; Sheftell, F.D.; Ciannella, L.; D’Alessio, A.; Apice, G.; Capobianco, N.N.; Saracino, D.M.T.; Di Iorio, W.; Bigal, M.E. A new questionnaire for assessment of adverse events associated with triptans: Methods of assessment influence the results. Preliminary results. J. Headache Pain 2004, 5, S112–S116. [Google Scholar] [CrossRef]
- Foster, J.M.; Aucott, L.; van der Werf, R.H.W.; van der Meijden, M.J.; Schraa, G.; Postma, D.S.; van der Molen, T. Higher patient perceived side effects related to higher daily doses of inhaled corticosteroids in the community: A cross-sectional analysis. Respir. Med. 2006, 100, 1318–1336. [Google Scholar] [CrossRef]
- Gater, A.; Reaney, M.; Findley, A.; Brun-Strang, C.; Burrows, K.; Nguyen-Pascal, M.L.; Roborel de Climens, A. Development and First Use of the Patient’s Qualitative Assessment of Treatment (PQAT) Questionnaire in Type 2 Diabetes Mellitus to Explore Individualised Benefit-Harm of Drugs Received During Clinical Studies. Drug Saf. 2020, 43, 119–134. [Google Scholar] [CrossRef] [PubMed]
- Haddad, P.M.; Fleischhacker, W.W.; Peuskens, J.; Cavallaro, R.; Lean, M.E.; Morozova, M.; Reynolds, G.; Azorin, J.-M.; Thomas, P.; Möller, H.-J. SMARTS (Systematic Monitoring of Adverse events Related to TreatmentS): The development of a pragmatic patient-completed checklist to assess antipsychotic drug side effects. Ther. Adv. Psychopharmacol. 2014, 4, 15–21. [Google Scholar] [CrossRef]
- Mojtabai, R.; Corey-Lisle, P.K.; Ip, E.H.S.; Kopeykina, I.; Haeri, S.; Cohen, L.J.; Shumaker, S. The Patient Assessment Questionnaire: Initial validation of a measure of treatment effectiveness for patients with schizophrenia and schizoaffective disorder. Psychiatry Res. 2012, 200, 857–866. [Google Scholar] [CrossRef]
- Pearce, A.; Haas, M.; Viney, R.; Pearson, S.A.; Haywood, P.; Brown, C.; Ward, R. Incidence and severity of self-reported chemotherapy side effects in routine care: A prospective cohort study. PLoS ONE 2017, 12, e0184360. [Google Scholar] [CrossRef]
- Schoenmakers, T.W.; Teichert, M.; Wensing, M.; de Smet, P.A. Evaluation of Potentially Drug-Related Patient-Reported Common Symptoms Assessed During Clinical Medication Reviews: A Cross-Sectional Observational Study. Drug Saf. 2017, 40, 419–430. [Google Scholar] [CrossRef]
- Uher, R.; Farmer, A.; Henigsberg, N.; Rietschel, M.; Mors, O.; Maier, W.; Kozel, D.; Hauser, J.; Souery, D.; Placentino, A.; et al. Adverse reactions to antidepressants. Br. J. Psychiatry 2009, 195, 202–210. [Google Scholar] [CrossRef]
- Uijl, S.G.; Uiterwaal, C.S.; Aldenkamp, A.P.; Carpay, J.A.; Doelman, J.C.; Keizer, K.; Vecht, C.J.; de Krom, M.C.; van Donselaar, C.A. A cross-sectional study of subjective complaints in patients with epilepsy who seem to be well-controlled with anti-epileptic drugs. Seizure 2006, 15, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Waddell, L.; Taylor, M. A new self-rating scale for detecting atypical or second-generation antipsychotic side effects. J. Psychopharmacol. 2008, 22, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Wolters, H.A.; Knegtering, R.; Wiersma, D.; van den Bosch, R.J. Evaluation of the subjects’ response to antipsychotics questionnaire. Int. Clin. Psychopharmacol. 2006, 21, 63–69. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Marcinowicz, L.; Chlabicz, S.; Grebowski, R. Open-ended questions in surveys of patients’ satisfaction with family doctors. J. Health Serv. Res. Policy 2007, 12, 86–89. [Google Scholar] [CrossRef] [PubMed]
- Ashoorian, D.; Davidson, R.; Rock, D.; Gudka, S.; Clifford, R. A review of self-report medication side effect questionnaires for mental health patients. Psychiatry Res. 2014, 219, 664–673. [Google Scholar] [CrossRef]
- Terwee, C.; Bot, S.; Boer, M.; van der Windt, D.; Knol, D.; Dekker, J.; Bouter, L.; De Vet, H. Quality criteria were proposed for measurement properties of health status questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef]
- Staniszewska, S.; Haywood, K.L.; Brett, J.; Tutton, L. Patient and public involvement in patient-reported outcome measures: Evolution not revolution. Patient 2012, 5, 79–87. [Google Scholar] [CrossRef]
- Van Strien, A.M.; Keijsers, C.J.; Derijks, H.J.; van Marum, R.J. Rating scales to measure side effects of antipsychotic medication: A systematic review. J. Psychopharmacol. 2015, 29, 857–866. [Google Scholar] [CrossRef]


{kind=link}
| General vs. Focusing on Specific Medications or Disease/Health Conditions | Name of Questionnaire |
|---|---|
| Mental health medications, n = 8 [15,27,31,35,36,39,41,42] | My Medicines and Me (M3Q) Approaches to Schizophrenia Communication Self-Report Checklist (ASC-SR) Subjects’ Response to Antipsychotics (SRA) Glasgow Antipsychotic Side-Effect Scale (GASS) Patient Assessment Questionnaire (PAQ) Systematic Monitoring of Adverse Events Related to Treatments (SMARTS) Maudsley Side-Effects (MSE) measure Antidepressant Side-Effect Checklist (ASEC) |
| General questionnaires, n = 4 [7,16,28,38] | Generic symptoms questionnaire Treatment Satisfaction Questionnaire for Medication (TSQM) Patient-Reported Adverse Drug Event Questionnaire Patient-Reported Outcome Measure Inquiry into Side-Effects (PROMISE) |
| Antiepileptics, n = 2 [30,40] | Side-Effect Checklist Assessment of Side-Effects in AED treatment (SIDAED) |
| Asthma and chronic obstructive pulmonary disease, n = 2 [29,33] | Satisfaction with Asthma Treatment Questionnaire Inhaled Corticosteroids Questionnaire (ICQ) |
| Diabetes, n = 1 [34] | Patient’s Qualitative Assessment of Treatment (PQAT) |
| Chemotherapy, n = 1 [37] | Common Terminology Criteria for Adverse Events Side-Effects Questionnaire |
| Triptans, n = 1 [32] | Triptans Questionnaire |
| Questionnaire Name, Primary Author, Year, and Country | Participant Demographics for Development | General vs. Focusing on Specific Medications or Disease/Health Conditions | Number of Side-Effect-Related Items | Domains | Response Categories | Scoring | Patients Nominate Bothersome Side-Effects | Open-Ended Questions | Asking Whether Side-Effects Likely Medication-Related |
|---|---|---|---|---|---|---|---|---|---|
| Generic Symptoms Questionnaire Jarernsiripornkul, 2001, UK [7] | 837 patients, mean age 50.5, 34% male | General | 22 | 18 categories of body systems | Yes/no or ticking checkbox of potential side-effects | None | Yes | Yes | Yes |
| Treatment Satisfaction Questionnaire for Medication (TSQM) Atkinson 2004, USA [28] | 567 patients, mean age 50.5 years | General | 5 | 4 domains: effectiveness, side-effects, treatment satisfaction, and convenience | 7-point scale ranging from ‘extremely satisfied’ to ‘extremely dissatisfied’ | 0–100 | No | None | Yes |
| Patient-Reported Adverse Drug Event Questionnaire Vries, 2013, Netherlands [16] | 135 patients, mean age 65 years, 60% male | General | 252 ADEs categorised in body categories | 16 categories of body systems | Yes/no | None | Yes | Yes | Yes |
| Patient-Reported Outcome Measure, Inquiry into Side-Effects (PROMISE) Schoenmakers, 2017, Netherlands [38] | 180 patients, mean age 73 years, 48% male | General | One item with 22 symptoms | 5 domains: health status, beliefs and concerns about medicines, self-efficacy in understanding and using medicines, medication adherence, and potentially drug-related symptoms | Yes/no | None | No | Yes | Yes |
| My Medicines and Me (M3Q) Ashoorian 2015, Australia [27] | 78 (10 patients, 8 carers, 28 physicians, 10 nurses, and 22 pharmacists), age range 21–80, 40% male | Mental health | 32 | 3 domains: current medications, side-effects, and general questions | Yes/no | None | Yes | Yes | Yes |
| Approaches to Schizophrenia Communication Self-Report Checklist (ASC-SR) Dott 2001, US, Canada, and UK [31] | 152 patients and 21 psychiatrists and case workers | Antipsychotics | 17 | 1 domain: side-effects | ‘I have had this experience recently’ and ‘I would like to talk about this to a nurse of doctor’ | None | Yes | Yes | No |
| Subjects’ Response to Antipsychotics (SRA) Wolters 2006, Netherlands [42] | 320 patients, mean age 35 years, 73% male | Antipsychotics | 74 | 9 domains: weight gain, sexual anhedonia, sedation, affective flattening, extrapyramidal symptoms, diminished sociability, increased sleep, recovery, and other | ‘No’, ‘yes to a certain degree’, and ‘yes to a high degree’ | Range of total scores not explicitly mentioned | No | None | No |
| Glasgow Antipsychotic Side-Effect Scale (GASS) Waddell, 2008, UK [41] | 50 patients, age range 18–65 years, 47% male | Second generation antipsychotics | 22 | 9 domains: sedation and central nervous system (CNS), cardiovascular, extrapyramidal, anticholinergic, gastrointestinal, genitourinary, screening for diabetes mellitus, prolactinaemia, and weight gain | Q1–30 scored 0 (never) to 3 (everyday), Q21–22 scored 0 for no and 3 for yes. | Divided into 3 sections; 0–21 = absent/mild side-effects; 22–42 = moderate side-effects, and 43–63 = severe side-effects. | Yes | None | No |
| Patient Assessment Questionnaire (PAQ) Mojtabai 2012, US [36] | 300 patients, mean age 46.7 years, 57% male | Antipsychotics | 40 | 5 domains: general distress, side-effects, psychotic symptoms, cognitive symptoms, and sleep | 0 = ‘not at all’ to 4 = ‘extremely/very much’ | Maximum total score of 160 | No | None | No |
| Systematic Monitoring of Adverse Events Related to Treatments (SMARTS) Haddad, 2014, UK [35] | Not specified | Antipsychotic | 12 | 9 domains: extrapyramidal symptoms, sexual dysfunction, hyperprolactinaemia, postural hypotension, sedation, appetite and weight change, gastrointestinal side-effects, urinary symptoms, and affective side-effects | Yes/no | None | Yes | Yes | No |
| Maudsley Side-Effects (MSE) measure Wykes 2017, UK, USA, and Spain [15] | 108 (patients, psychiatrists and pharmacists), mean age 44.2 years, 46.3% male | Antipsychotics | 53 | 2 domains: demographics and side-effects | Rating from ‘not at all’ to ‘severe’ | Total side-effects (0–53), total intensity (0–159), total distress (0–53), and total life impact (0–159) | Yes | Yes | No |
| Antidepressant Side-Effect Checklist (ASEC) Uher 2009, Europe [39] | 811 patients, mean age 42.5 years, 36.6% male | Antidepressants, SSRI (escitalopram) and TCA (nortriptyline) | 21 | 3 domains: potential side-effects, any treatment for side-effects, and if side-effects led to antidepressant discontinuation | 4-point scale ranging from 0 = absent to 3 = severe | Range of total scores not explicitly mentioned | No | Yes | Yes |
| Side-Effect Checklist Carpay 2005, Netherlands [30] | 346 patients, mean age 51.9 years, 50.4% male | Antiepileptics | 30 | 8 domains: general CNS, motor problems, gastrointestinal complaints, cognition, visual, mood, behaviour, cosmetic, and sleep problems | Side-effects dichotomised as present or not present, side-effect severity rating: 4-point scale ranging from ‘none’ to ‘very severe’ | Range of total scores not explicitly mentioned | No | None | No |
| Assessment of Side-Effects in AED Treatment (SIDAED) Uijl 2006, Netherlands [40] | 173 patients, mean age 48 years, 50% male | Antiepileptics | 46 | 10 domains: general CNS, behaviour, depressive symptoms, cognitive function, motor problems/coordination, visual complaints, headache, cosmetic and dermatological complaints, gastrointestinal complaints, and sexuality and menses | Severity rating from 0 = ‘no problem’ to 3 = ‘serious problem’, duration of complaints also scored (for example, since a few weeks vs. since months) | 0–138 | No | None | No |
| Satisfaction with Asthma Treatment Questionnaire Campbell, 2003, UK [29] | 131 patients, mean age 45, 34% male | Inhaled asthma medicines | 26 | 4 domains: effectiveness of treatment, ease of use, medication burden, and side-effects and worries | 1 (strongly disagree) to 7 (strongly agree) | None | No | None | No |
| Inhaled Corticosteroids Questionnaire (ICQ) Foster 2006, Netherlands and Scotland [33] | 395 patients, mean age 50 years, 47% male | Inhaled corticosteroids | 57 | 8 domains: voice, cough, oropharynx, taste, mouth, skin, mood, and other | 7-point scale ranging from 0 = ‘not at all’ to 6 = ‘a very great deal’ | Out of 100 | No | Yes | No |
| Patient’s Qualitative Assessment of Treatment (PQAT) Gater, 2020, UK [34] | 57 patients, mean age 57, 58% male | Type 1 and 2 diabetes | 4 | 4 domains: benefits of the drug, disadvantages of the drug, willingness to continue with the drug, and balance between benefits and disadvantages | Combination of qualitative answers, yes/no and scales of 0–10 and −3 to 3 | Range of total scores not explicitly mentioned | No | Yes | No |
| Common Terminology Criteria for Adverse Events Side-Effects Questionnaire Pearce, 2017, Australia [37] | 441 patients, majority (59.7%) in the 45–65 years group, 26.1% male | Chemotherapy | 9 | 9 domains: diarrhoea, vomiting, chest pain or angina, constipation, dyspnoea, fatigue, mucositis, pain, and rash | 0 = not present to 5 = severe | None | No | None | No |
| Triptans Questionnaire Feleppa, 2004, Italy [32] | 108 patients, mean age 39.5, 13% male | Triptans | 2 | 2 domains: unprompted side-effects and prompted side-effects | Combination of free text, yes/no, rating 1 = mild to 3 = severe | None | No | Yes | No |
| Validity | Reliability | Responsiveness | |||||
|---|---|---|---|---|---|---|---|
| Questionnaire Name, Primary Author, Year, and Country | Literature Review | Delphi/Expert Panel (Content Validity) | Patient Input | Criterion or Construct Testing | Internal Consistency | Test–Retest Reliability | Ability to Detect Change over Time |
| Generic Symptoms Questionnaire Jarernsiripornkul, 2001, UK [7] | Previously published work used as a basis | Unclear | Initially piloted in 11 patients followed by further patient pilot groups | Reporters of musculoskeletal symptoms taking statins had significantly higher mean creatinine kinase level than those not reporting any musculoskeletal symptoms (207.35 ± 155.40 vs. 143.95 ± 83.07 U/L, respectively; p = 0.037) | None | None | None |
| Treatment Satisfaction Questionnaire for Medication (TSQM) Atkinson 2004, USA [28] | Literature review regarding patient satisfaction with medications across various therapeutic areas | Unclear | Three focus group with patients allowing integration of the patients’ perspectives and initial item reduction and scaling | Multistep exploratory factor analyses (EFA) used. First EFA produced three factors (eigenvalue more than 1.7 explaining 75.6% of overall variance); second EFA yielded final instrument (eigenvalue =2.3 explaining 79.1% of total variance) | High Cronbach’s α of around 0.88 for each domain | ICC values were high when comparing results at two timepoints separated by 7–4 days: 0.784 for effectiveness, 0.737 for convenience and 0.759 for t global satisfaction | None |
| Patient-Reported Adverse Drug Event Questionnaire Vries, 2013, Netherlands [16] | Common Terminology Criteria for Adverse Events version 4.0 and existing symptom and ADE checklists used | Unclear | Cognitive debriefing interviewing with patients to eliminate ambiguity in questions | Construct validity—patients who reported side-effects (n = 37) had a lower general quality of life and physical health than those not reporting side-effects (p < 0.05). Concurrent validity—in comparison with TSQM, this questionnaire had a sensitivity of 38% and positive predictive value of 79% for assessing side-effects associated with metformin | None | Test–retest reliability was acceptable at patient level (k = 0.50, PPA 0.64) | None |
| Patient Reported Outcome Measure, Inquiry into Side-Effects (PROMISE) Schoenmakers, 2017, Netherlands [38] | Existing instruments and literature regarding side effects of drugs most frequently used in the Netherlands used | Unclear | Pretested in patients eligible for a medication review to assess whether the items were well understood | None | None | None | None |
| My Medicines and Me (M3Q) Ashoorian 2015, Australia [27] | Previous self-report questionnaires assessing subjective experiences of medication side-effects used | Focus groups with psychiatrists, general practitioners, mental health nurses, and pharmacists | Focus group with carers and mental health patients | Spearman’s nonparametric coefficient of correlation was high and statistically significant (ρ = 0.724, p < 0.001) | High Cronbach’s α of 0.929 | None | None |
| Approaches to Schizophrenia Communication Self-Report Checklist (ASC-SR) Dott 2001, US, Canada and UK [31] | Item generation through literature search | Steering group consisted of psychiatrists | Patient input regarding usefulness of checklist | None | None | None | None |
| Subjects’ Response to Antipsychotics (SRA) Wolters 2006, Netherlands [42] | Unclear | Clinical experts categorised items into subscales | Semi-structured interviews with 77 patients for item generation | Moderate to low correlations between SRA and Subjective Wellbeing on Neuroleptics (SWN) subscales | Cronbach’s α of the subscales were between 0.69 and 0.93 | Pearson’s r correlation between scores tested 1 week apart was 0.76 for all but two subscales (sexual anhedonia and affective flattening) | None |
| Glasgow Antipsychotic Side-Effect Scale (GASS) Waddell, 2008, UK [41] | Existing questionnaires and information from the British National Formulary and the pharmaceutical industry used | Discussion with members of the mental health team | Focus group of patients taking antipsychotics ranked the list of side-effects in terms of acceptability | GASS scores for two groups taking and not taking antipsychotics differed significantly (Mann–Whitney U-test, U = 2336, p < 0.0001) with a mean of 14.3 for those on antipsychotics and 3.6 for those not on antipsychotics | None | Good test–retest reliability, with κ = 0.72. | None |
| Patient Assessment Questionnaire (PAQ) Mojtabai 2012, US [36] | Unclear | Experts in psychiatry, social and behavioural sciences, and psychometrics used | Patient focus groups leading to questionnaire refinement | Exploratory factor analysis and visual inspection of scree plots identified five factors with eigenvalues more than 1 (accounting for 50.4% of the variance) | Cronbach’s α of 0.85 for the side effect subscale | None | None |
| Systematic Monitoring of Adverse Events Related to Treatments (SMARTS) Haddad, 2014, UK [35] | 11 side-effects included after literature search | Developed over a series of group meetings by an international faculty of 12 experts (including psychiatrists, a general physician, and psychopharmacologist) | No | None | None | None | None |
| Maudsley Side-Effects (MSE) measure Wykes 2017, UK, USA and Spain [15] | Published literature of antipsychotic side-effect rating scales used | Delphi exercise with psychiatrists and pharmacists | Patient focus groups used | Compared to the GASS tool, the MSE and GASS subscales were highly correlated (total side-effects: Pearson’s correlation, r = 0.8, intensity: r = 0.8, and distress: r = 0.7, p < 0.001 in all cases) | Cronbach’s α for the total side-effects score was 0.96 | Scores were highly correlated (0.81–0.96) between 6 and 8 days, with no statistically significant differences in the mean scores | None |
| Antidepressant Side-Effect Checklist (ASEC) Uher 2009, Europe [39] | List of adverse effects compiled from the literature | Scientists, clinicians, and industrial partners involved | No | Agreement between the self-rated ASEC and interviewer-rated UKU was good, with kappa ranging from 0.55 for insomnia to 0.89 for dry mouth | Average inter-item covariance was 0.05 and Cronbach’s α was 0.78 | None | Dryness of mouth was significantly more frequent during treatment with escitalopram (OR = 1.46) and nortriptyline (OR = 9.04) compared to antidepressant-free baseline |
| Side-Effect Checklist Carpay 2005, Netherlands [30] | Unclear | Unclear | Community-based patients completed the checklist | None | None | None | None |
| Assessment of Side-Effects in AED Treatment (SIDAED) Uijl 2006, Netherlands [40] | Unclear | Unclear | Patients asked to complete questionnaire | None | None | None | In a trial involving 111 adults with epilepsy randomised to either intervention (adjustment of antiepileptics based on SIDAED responses) or control (treatment unchanged) over 7 months, there was a decrease in complaints by intervention, rate ratio of 1.34 (not statistically significant) |
| Satisfaction with Asthma Treatment Questionnaire Campbell, 2003, UK [29] | Preliminary instrument based on literature review | Preliminary instrument based on expert opinion, focus groups, and literature findings | Two focus groups to understand patient perception of asthma treatment regimens and problems | Eight items showed factor loadings of <0.35 on any factor or had high factor loadings on more than one factor and were excluded | Cronbach’s α ranged from 0.71–0.88 | Test/retest reliability (intra correlation coefficients) ranged from 0.66–0.74 | None |
| Inhaled Corticosteroids Questionnaire (ICQ) Foster 2006, Netherlands and Scotland [33] | Unclear | Expert panel reviewed side-effect items | In-depth interviews and focus groups with patients to talk about their experiences of ICS side-effects | All three construct validity hypotheses were well supported: (i) statistically significant difference existed in scores for 14 domains with the high ICS dose group scoring highest; (ii) ICS dose independently predicted ICQ scoring after adjusting for confounders; (iii) greater convergence existed between local ICQ domains than between local and systemic domains | Excellent internal consistency: Cronbach’s α = 0.98 | Test–retest intraclass correlation coefficients were ≥0.69 for all but the ‘facial oedema’ domain | Comparing different dosing regimens of inhaled ciclesonide and fluticasone over 12 or 24 weeks, no significant score changes were observed from baseline |
| Patient’s Qualitative Assessment of Treatment (PQAT) Gater, 2020, UK [34] | Unclear | Initial items were developed by the experts | Cognitive testing of the initial version was conducted among 7 patients with type 1 and type 2 diabetes | No | None | None | None |
| Common Terminology Criteria for Adverse Events Side-Effects Questionnaire Pearce, 2017, Australia [37] | The National Cancer Institute Common Toxicity Criteria version 4 was adapted in English | Unclear | No | None | None | None | None |
| Triptans Questionnaire Feleppa, 2004, Italy [32] | Unclear | Unclear | No | None | None | None | None |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, R.; Ellett, L.K.; Roughead, E.E.; Cheah, P.Y.; Masnoon, N. Patient-Reported Questionnaires to Identify Adverse Drug Reactions: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 11877. https://doi.org/10.3390/ijerph182211877
Lim R, Ellett LK, Roughead EE, Cheah PY, Masnoon N. Patient-Reported Questionnaires to Identify Adverse Drug Reactions: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(22):11877. https://doi.org/10.3390/ijerph182211877
Chicago/Turabian StyleLim, Renly, Lisa Kalisch Ellett, Elizabeth E. Roughead, Phaik Yeong Cheah, and Nashwa Masnoon. 2021. "Patient-Reported Questionnaires to Identify Adverse Drug Reactions: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 22: 11877. https://doi.org/10.3390/ijerph182211877
APA StyleLim, R., Ellett, L. K., Roughead, E. E., Cheah, P. Y., & Masnoon, N. (2021). Patient-Reported Questionnaires to Identify Adverse Drug Reactions: A Systematic Review. International Journal of Environmental Research and Public Health, 18(22), 11877. https://doi.org/10.3390/ijerph182211877