
Effect of Tooth Agenesis on Mandibular Morphology and Position



Abstract
:1. Introduction
2. Materials and Methods
- Age above 9 and below 18 years;
- Confirmed congenital lack of at least 2 permanent tooth buds in the maxilla and/or mandible;
- Patients with agenesis, without loss of teeth caused by other factors (caries, injuries);
- Patients without a history of orthodontic treatment;
- Good-quality panoramic radiograph;
- Digital lateral cephalogram.
- Age below 9 or above 18 years;
- Patients with congenital malformations of the facial skeleton accompanied by congenital lack of permanent tooth buds, e.g., Down syndrome, cleft lip and palate;
- Patients with a history of injuries to the facial skeleton;
- Patients during or after orthodontic treatment;
- Patients with premature loss of deciduous teeth;
- Patients with premature loss of permanent teeth;
- Patients with hypo-hyperdontia or anodontia of permanent dentition.
- Age above 9 and below 18 years;
- Generally healthy patients;
- Patients without a history of orthodontic treatment;
- Good-quality panoramic radiograph;
- Digital lateral cephalogram.
- Age below 9 or above 18 years;
- Congenital malformations and dysmorphism of the facial skeleton, e.g., Down syndrome, cleft lip and palate;
- A history of injuries to the facial skeleton;
- Premature loss of deciduous teeth;
- Premature loss of permanent teeth;
- Patients during or after orthodontic treatment.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Song, S.; Han, D.; Qu, H.; Gong, Y.; Wu, H.; Zhang, X.; Zhong, N.; Feng, H. EDA gene mutations underlie non-syndromic oligodontia. J. Dent. Res. 2009, 88, 126–131. [Google Scholar] [CrossRef] [Green Version]
- Celikoglu, M.; Kazanci, F.; Miloglu, O.; Oztek, O.; Kamak, H.; Ceylan, I. Frequency and characteristics of tooth agenesis among an orthodontic patient population. Med. Oral Patol. Oral Cir. Bucal 2010, 15, e797–e801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parkin, N.; Elcock, C.; Smith, R.; Griffin, R.; Brook, A. The aetiology of hypodontia: The prevalence, severity and location of hypodontia within families. Arch. Oral Biol. 2009, 54, S52–S56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gracco, A.L.T.; Zanatta, S.; Valvecchi, F.F.; Bignotti, D.; Perri, A.; Baciliero, F. Prevalence of dental agenesis in a sample of Italian orthodontic patients: An epidemiological study. Prog. Orthod. 2017, 18, 1–7. [Google Scholar] [CrossRef]
- Wisth, P.J.; Thunold, K.; Bøe, O.E. The craniofacial morphology of individuals with hypodontia. Acta Odontol. Scand. 1974, 32, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Nodal, M.; Kjaer, I.; Solow, B. Craniofacial morphology in patients with multiple congenitally missing permanent teeth. Eur. J. Orthod. 1994, 16, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Øgaard, B.; Krogstad, O. Craniofacial structure and soft tissue profile in patients with severe hypodontia. Am. J. Orthod. Dentofac. Orthop. 1995, 108, 472–477. [Google Scholar] [CrossRef]
- Yüksel, S.; Üçem, T. The effect of tooth agenesis on dentofacial structures. Eur. J. Orthod. 1997, 19, 71–78. [Google Scholar] [CrossRef] [Green Version]
- Tavajohi-Kermani, H.; Kapur, R.; Sciote, J.J. Tooth agenesis and craniofacial morphology in an orthodontic population. Am. J. Orthod. Dentofac. Orthop. 2002, 122, 39–47. [Google Scholar] [CrossRef]
- Biedziak, B. Irregularities and deviations in the morphology of the facial skeleton in patients with oligodontia. Czas. Stomat. 2005, 58, 752–759. [Google Scholar]
- Endo, T.; Yoshino, S.; Ozoe, R.; Kojima, K.; Shimooka, S. Association of advanced hypodontia and craniofacial morphology in Japanese orthodontic patients. Odontology 2004, 92, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Endo, T.; Ozoe, R.; Yoshino, S.; Shimooka, S. Hypodontia patterns and variations in craniofacial morphology in Japanese orthodontic patients. Angle Orthod. 2006, 76, 996–1003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Acharya, P.N.; Jones, S.P.; Moles, D.; Gill, D.; Hunt, N.P. A cephalometric study to investigate the skeletal relationships in patients with increasing severity of hypodontia. Angle Orthod. 2010, 80, 699–706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kreczi, A.; Proff, P.; Reicheneder, C.; Faltermeier, A. Effects of hypodontia on craniofacial structures and mandibular growth pattern. Head Face Med. 2011, 7, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, S.K.; Lakshmi, A.V.V.; Namita, S.; Elumalai, M. Craniofacial Morphologic Variations and Its Association with Hypodontia Pattern (Anterior) in South Indian Female Population. Biosci. Biotechnol. Res. Asia 2013, 10, 325–328. [Google Scholar] [CrossRef]
- Zadurska, M. Oligodoncja w Aspekcie Wybranych Objawów Dysplazji Ektodermalnej. Habilitation’s Thesis, Warszawski Uniwersytet Medyczny, Warsaw, Poland, 2011; p. 114. [Google Scholar]
- Zadurska, M.; Krasny, M.; Jurek, A.; Gozdowski, D.; Sobieska, E. Zależność między liczbą brakujących zawiązków zębów stałych a długością podstawy szczęki i trzonu żuchwy u pacjentów z oligodoncją uzębienia stałego. Forum Ortod. 2016, 12, 165–173. [Google Scholar]
- Miševska, C.B.; Kanurkova, L.; Valjakova, E.B.; Georgieva, S.; Bajraktarova, B.; Georgiev, Z.; Ivkovska, A.S. Craniofacial morphology in individuals with increasing severity of hypodontia. South Eur. J. Orthod. Dentofac. Res. 2016, 3, 12–17. [Google Scholar] [CrossRef] [Green Version]
- Gungor, A.Y.; Turkkahramanb, H. Effects of severity and location of nonsyndromic hypodontia on craniofacial morphology. Angle Orthod. 2013, 83, 584–590. [Google Scholar] [CrossRef]
- Lisson, J.A.; Scholtes, S. Investigation of Craniofacial Morphology in Patients with Hypo- and Oligodontia. J. Orofac. Orthop. 2005, 66, 197–207. [Google Scholar] [CrossRef]
- Taju, W.; Sherriff, M.; Bister, D.; Shah, S. Association between severity of hypodontia and cephalometric skeletal patterns: A retrospective study. Eur. J. Orthod. 2018, 40, 200–205. [Google Scholar] [CrossRef] [Green Version]
- Mayama, H.; Kuwajima, Y.; Da Silva, J.D.; Khorashadi, S.; Lambert, R.F.; Ishida, Y.; Ishikawa-Nagai, S.; Miura, H.; Satoh, K. Cephalometric measurements of non syndromic oligodontia in early dental age in a Japanese population. Clin. Cosmet. Investig. Dent. 2019, 11, 357–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Särnas, K.V.; Rune, B. The facial profilein advanced hypodontia: A mixed longitudinal study of 141 children. Eur. J. Orthod. 1983, 5, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Ben-Bassat, Y.; Brin, I. Skeletodental patterns in patients with multiple congenitally missing teeth. Am. J. Orthod. Dentofac. Orthop. 2003, 124, 521–525. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Cephalometric Points | Cephalometric Planes | Construction Points |
|---|---|---|
| Ar—articulare, the point of intersection of the inferior outline of the cranial base with the posterior outline of the mandibular neck | FOP—functional occlusal plane, passing through M and pM points | B′—the point of intersection of a straight line parallel to FOP passing through the B point with the PA line |
| B—supramentale, the deepest point located on the anterior outline of the mandible | HL—horizontal line, perpendicular to PM and passing through SE | B″—the point of intersection of a straight line parallel to FOP passing through the B point with the PM line |
| Ba—basion, the most posteroinferior point of the cancellous part of the clivus, lying in the median plane | NB—a vertical line marked by N and B points, defining anteroposterior position of mandible | FMS’—projection of the FMS point on the HL line |
| Co—condylion, the most posterior and superior point of the mandibular head | NPg—a vertical line determined by N and Pg points, defining an anteroposterior position of the chin | Go—gonion, the point of intersection of the line tangential to the lower margin of the mandible and tangential to the posterior outline of the mandibular ramus |
| D—in our study, the most posterior point on the posterior outline of the mandibular symphysis | ML—a mandibular base line, the line indicated by Me and tgo1 points | Id′—the point of intersection of a straight line parallel to FOP passing through the Id point with the PA line |
| FMS—frontomaxillary nasal suture, the most superior point of the suture at the anterior connection of the nasal bone and maxilla | MT—a line of the posterior margin of the mandibular ramus, indicated by Ar and tgo2 points | Id″—the point of intersection of a straight line parallel to FOP passing through the Id point with the PM line |
| Gn—gnathion, the most anterior and inferior point on the lower outline of the chin | PA—a straight line parallel to the PM passing through FMS | Pg′—the point of intersection of a straight line parallel to FOP passing through the Pg point with the PA line |
| Id—the point on margin of the mandibular alveolar process between central incisors, or on top of the alveolar process in the midline in case of mandibular incisor agenesis | PM—a vertical line passing through the SE and Pm points | Pg″—the point of intersection of a straight line parallel to FOP passing through the Pg point with the PM line |
| M—the most posterior and inferior contact point of the last erupted upper molar with the opposite tooth | PgB—a line passing through Pg and B points | Sd′—the point of intersection of a straight line parallel to FOP passing through the Sd point with the PA line |
| N—nasion, the most anterior point of the frontonasal suture | PgId—the line passing through Pg and Id points | Sd″—the point of intersection of a straight line parallel to FOP passing through the Sd point with the PM line |
| Pg—pogonion, the most anterior point on the outline of the chin | ||
| pM—a contact point of the most mesially located premolars, deciduous molars or canines in the case of agenesis of all deciduous premolars and molars | ||
| Pm—pterygomaxillare, the point of intersection of the outline of the posterior maxillary contour or the anterior contour of the pterygopalatine fossa with the outline of the hard palate | ||
| S—sella, the point located in the geometric center of the sella turcica, in the medial plane | ||
| SE—sphenoethmoidal, the point located at the intersection of the cranial base and the greater wings of the sphenoid bone | ||
| tgo1—the point on the inferior margin of the mandibular angle at the point connecting a line tangential to the lower margin of the mandibular body | ||
| tgo2—the point on the posterior margin of the mandibular angle at the point connecting a line tangential to the posterior margin of the mandibular body |
| Linear Measurements | |
|---|---|
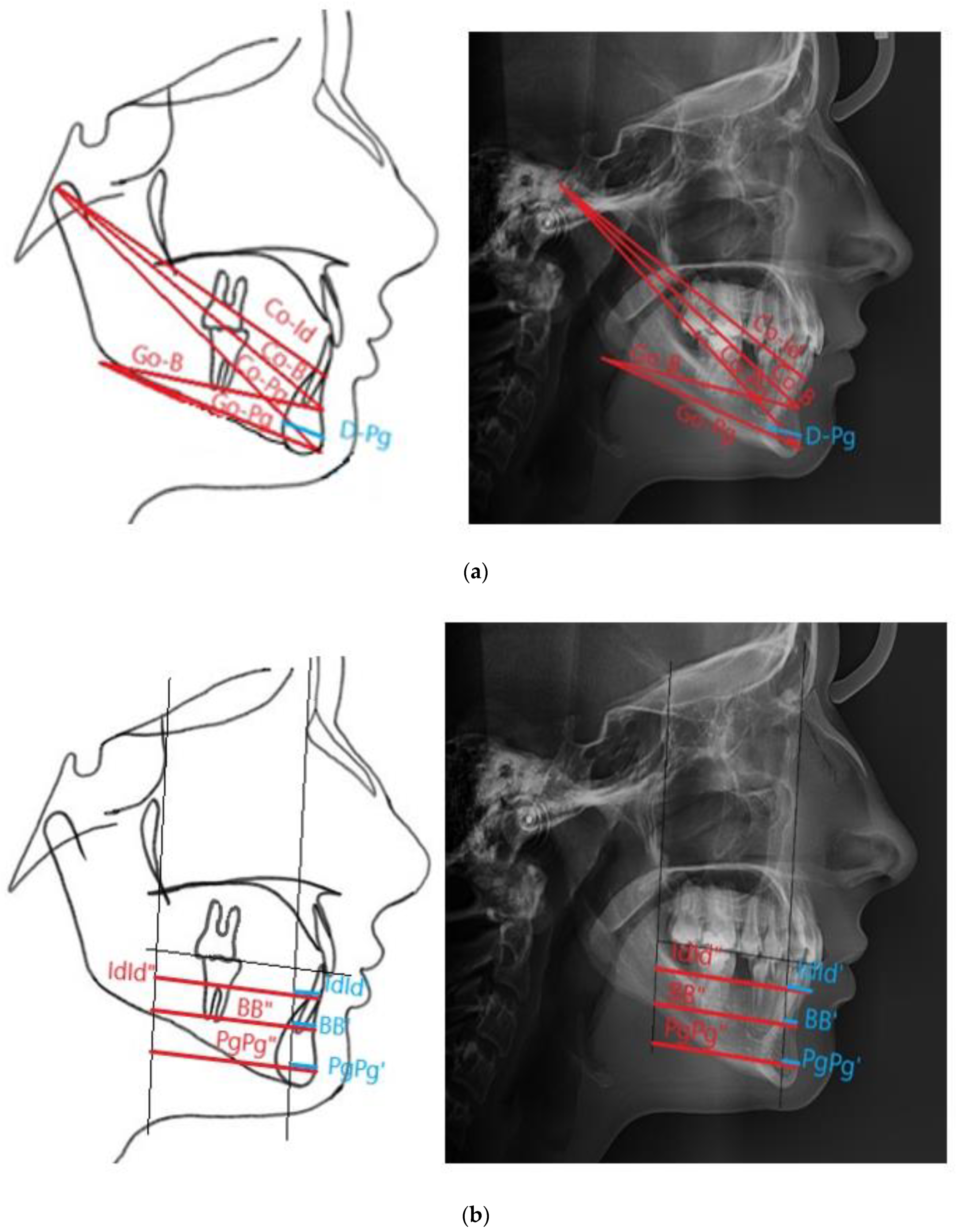
| BB′ | The distance between B and B′, in the authors’ study defined as the length of the anterior mandibular segment (the authors’ measurement) |
| BB″ | The distance between B and B″ |
| Co-B | The distance measured between Co and B points (the authors’ measurement) |
| Co-Id | The distance measured between Co and Id points (the authors’ measurement) |
| Co-Pg | The total mandibular length, the distance measured between Co and Pg points |
| D-Pg | The cross-sectional diameter of the mandibular symphysis, the distance between D and Pg points |
| Go-B | The length of the mandibular alveolar part, distances between Go and B points (the authors’ measurement) |
| Go-Pg | The mandibular body length, the distance between Go and Pg points |
| IdId′ | The distance between Id and Id′, defined as the anterior length of the mandibular alveolar part (the authors’ measurement) |
| IdId″ | The distance between Id and Id″ |
| PgPg′ | The distance between Pg and Pg′, defined as the length of the anterior mandibular part at the Pg height (the authors’ measurement) |
| PgPg″ | The distance between Pg and Pg″ |
| Angular Measurements | |
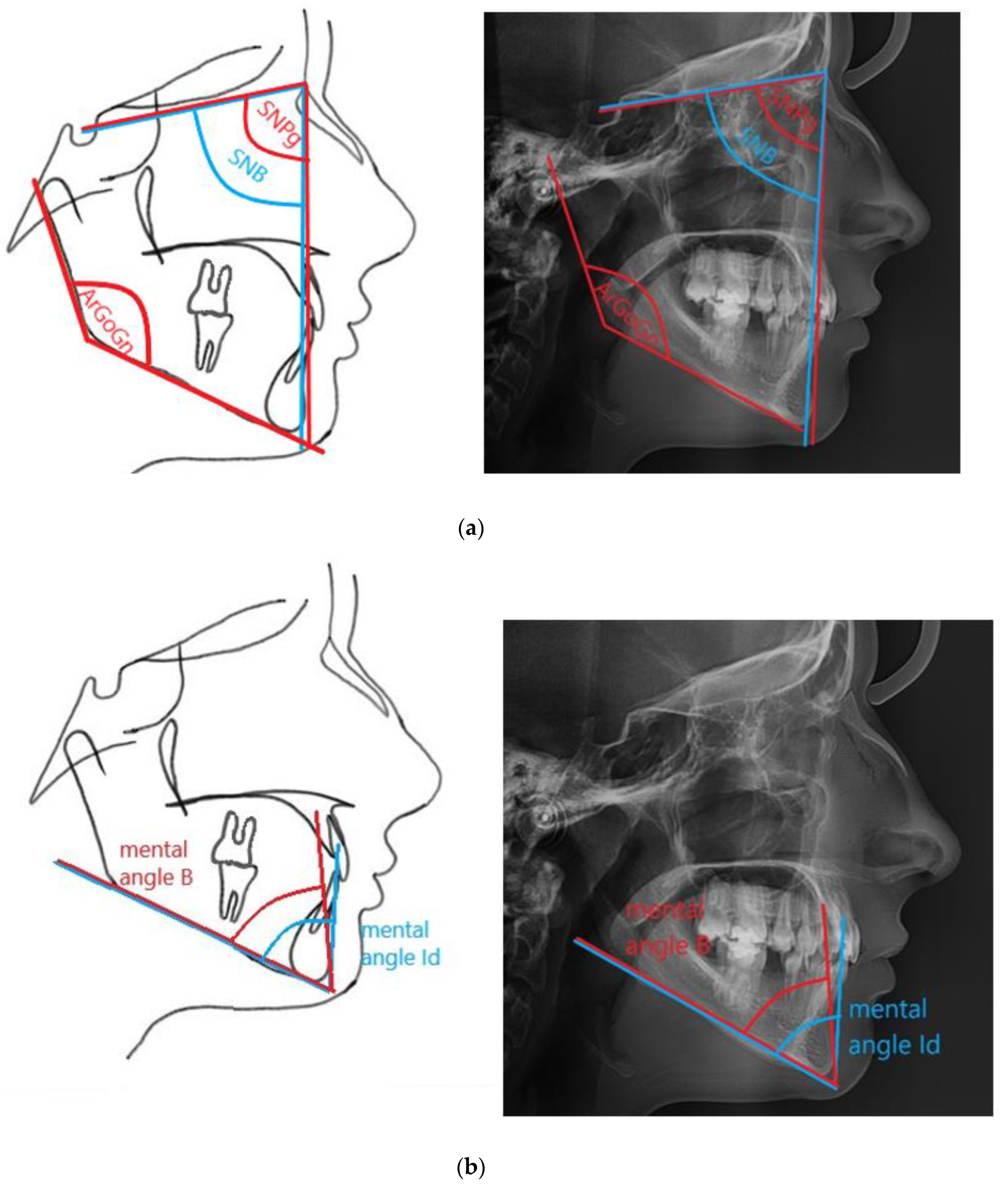
| ArGoGn | The mandibular angle, the angle betweenArGo andGoGn lines |
| Mental angle B | The angle between the ML mandibular plane and PgB line, determining the anteroposterior position of the B point, relative to the Pg point (the authors’ measurement) |
| Mental angle Id | The angle between the ML mandibular plane and the PgId line, determining the anteroposterior position of the Id point, relative to the Pg point |
| SNB | The angle determined by the SN and NB lines that determines the anteroposterior position of the mandible |
| SNPg | The angle determined by the SN and NPg lines that determines the anteroposterior position of the chin |
| Number of Missing Teeth | Number of Patients | Percent Value |
|---|---|---|
| 2 | 33 | 28.7% |
| 3 | 5 | 4% |
| 4 | 10 | 9% |
| 5 | 12 | 10.4% |
| 6 | 14 | 12.2% |
| 7 | 5 | 4% |
| 8 | 9 | 8% |
| 9 | 4 | 3.4% |
| 10 | 6 | 5% |
| 11 | 4 | 3.4% |
| 12 | 2 | 2% |
| 13 | 2 | 2% |
| 14 | 4 | 3.4% |
| 15 | 2 | 2% |
| 16 | 2 | 2% |
| 18 | 1 | 0.9% |
| 22 | 1 | 0.9% |
| Tooth (Maxilla) | Number of Missing Teeth in the Study Group | % of Missing Teeth in the Whole Group | Tooth (Mandible) | Number of Missing Teeth in the Whole Group | % of Missing Teeth in the Study Group |
|---|---|---|---|---|---|
| 11 | 2 | 0.28% | 31 | 37 | 5.14% |
| 12 | 56 | 7.8% | 32 | 16 | 2.2% |
| 13 | 13 | 1.8% | 33 | 10 | 1.4% |
| 14 | 30 | 4.16% | 34 | 24 | 3.3% |
| 15 | 55 | 7.64% | 35 | 70 | 9.7% |
| 16 | 7 | 0.97% | 36 | 2 | 0.28% |
| 17 | 18 | 2.5% | 37 | 28 | 3.9% |
| 21 | 4 | 0.55% | 41 | 39 | 5.42% |
| 22 | 53 | 7.9% | 42 | 13 | 1.8% |
| 23 | 13 | 1.8% | 43 | 11 | 1.53% |
| 24 | 30 | 4.16% | 44 | 17 | 2.36% |
| 25 | 49 | 6.8% | 45 | 72 | 10% |
| 26 | 6 | 0.83% | 46 | 2 | 0.28% |
| 27 | 18 | 2.5% | 47 | 25 | 3.47% |
| Measurement | Mean ± Standard Deviation | p | Lower Quartile (Q1) and Upper Quartile (Q3) | ||
|---|---|---|---|---|---|
| Study Group | Control Group | Study Group | Control Group | ||
| Co-Pg | 103.17 ± 7.37 | 104.01 ± 6.43 | 0.354 | 98.9–107.5 | 100.5–109.5 |
| Co-B | 93.23 ± 6.37 | 93.73 ± 5.55 | 0.522 | 90.0–97.6 | 91.0–98.5 |
| Co-Id | 90.22 ± 7.95 | 91.71 ± 5.48 | 0.098 | 87.7–94.9 | 88.9–96.2 |
| SNB | 79.11 ± 4.52 | 78.79 ± 3.54 | 0.550 | 97.9–104.2 | 98.5–103.2 |
| SNPg | 80.57 ± 4.78 | 79.86 ± 3.63 | 0.206 | 96.5–102.8 | 97.1–102.6 |
| ArGoGn | 134.4 ± 6.41 | 133.84 ± 6.09 | 0.494 | 131.2–138.0 | 128.9–137.1 |
| D-Pg | 13.86 ± 2.15 | 14.64 ± 2.26 | 0.007 * | 12.7–15.1 | 13.1–15.7 |
| Go-B | 63.29 ± 5.59 | 63.91 ± 5.15 | 0.382 | 49.3–55.2 | 50.8–56.2 |
| Go-Pg | 68.35 ± 6.01 | 68.68 ± 5.02 | 0.652 | 64.0–72.2 | 66.0–73.0 |
| IdId″ | 43.07 ± 4.51 | 45.48 ± 4.27 | 0.000 * | 40.2–46.2 | 42.9–48.3 |
| IdId′ | 8.96 ± 5.59 | 12.59 ± 5.28 | 0.000 * | 4.7–13.7 | 9.7–16.2 |
| BB′ | 7.96 ± 5.64 | 10.61 ± 5.45 | 0.000 * | 3.8–12.5 | 6.9–14.6 |
| BB″ | 41.35 ± 5.13 | 43.08 ± 4.83 | 0.009 * | 38.5–44.5 | 39.9–46.6 |
| PgPg′ | 10.61 ± 6.91 | 13.03 ± 6.72 | 0.007 * | 5.3–16.3 | 8.4–17.5 |
| PgPg″ | 44.03 ± 6.4 | 45.38 ± 6.35 | 0.108 | 40.0–47.9 | 41.3–50.6 |
| Mental angle B | 60.48 ± 18.4 | 64.1 ± 5.9 | 0.045 * | 56.8–66.9 | 60.8–68.0 |
| Mental angle Id | 68.11 ± 18.12 | 73.35 ± 5.22 | 0.003 * | 65.2–73.9 | 69.8–76.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jurek, A.; Gozdowski, D.; Czochrowska, E.M.; Zadurska, M. Effect of Tooth Agenesis on Mandibular Morphology and Position. Int. J. Environ. Res. Public Health 2021, 18, 11876. https://doi.org/10.3390/ijerph182211876
Jurek A, Gozdowski D, Czochrowska EM, Zadurska M. Effect of Tooth Agenesis on Mandibular Morphology and Position. International Journal of Environmental Research and Public Health. 2021; 18(22):11876. https://doi.org/10.3390/ijerph182211876
Chicago/Turabian StyleJurek, Agnieszka, Dariusz Gozdowski, Ewa Monika Czochrowska, and Małgorzata Zadurska. 2021. "Effect of Tooth Agenesis on Mandibular Morphology and Position" International Journal of Environmental Research and Public Health 18, no. 22: 11876. https://doi.org/10.3390/ijerph182211876
APA StyleJurek, A., Gozdowski, D., Czochrowska, E. M., & Zadurska, M. (2021). Effect of Tooth Agenesis on Mandibular Morphology and Position. International Journal of Environmental Research and Public Health, 18(22), 11876. https://doi.org/10.3390/ijerph182211876