
Changes in the Comprehensiveness of Rural Medical Care for Older Japanese Patients during the COVID-19 Pandemic



Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
2.2. Participants
2.3. Measurements
2.4. Analysis
2.5. Ethical Considerations
3. Results
3.1. Participant Demographics
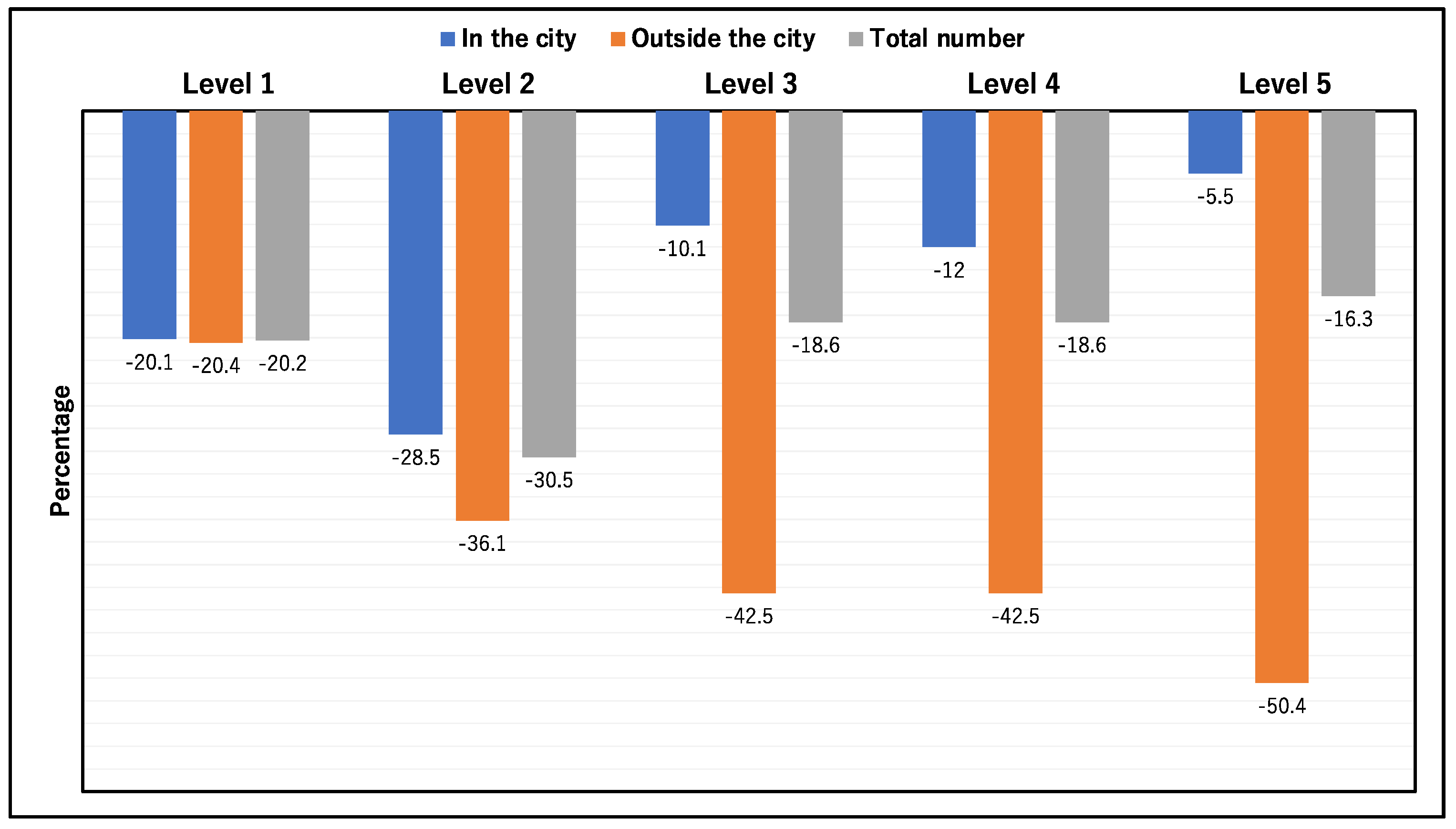
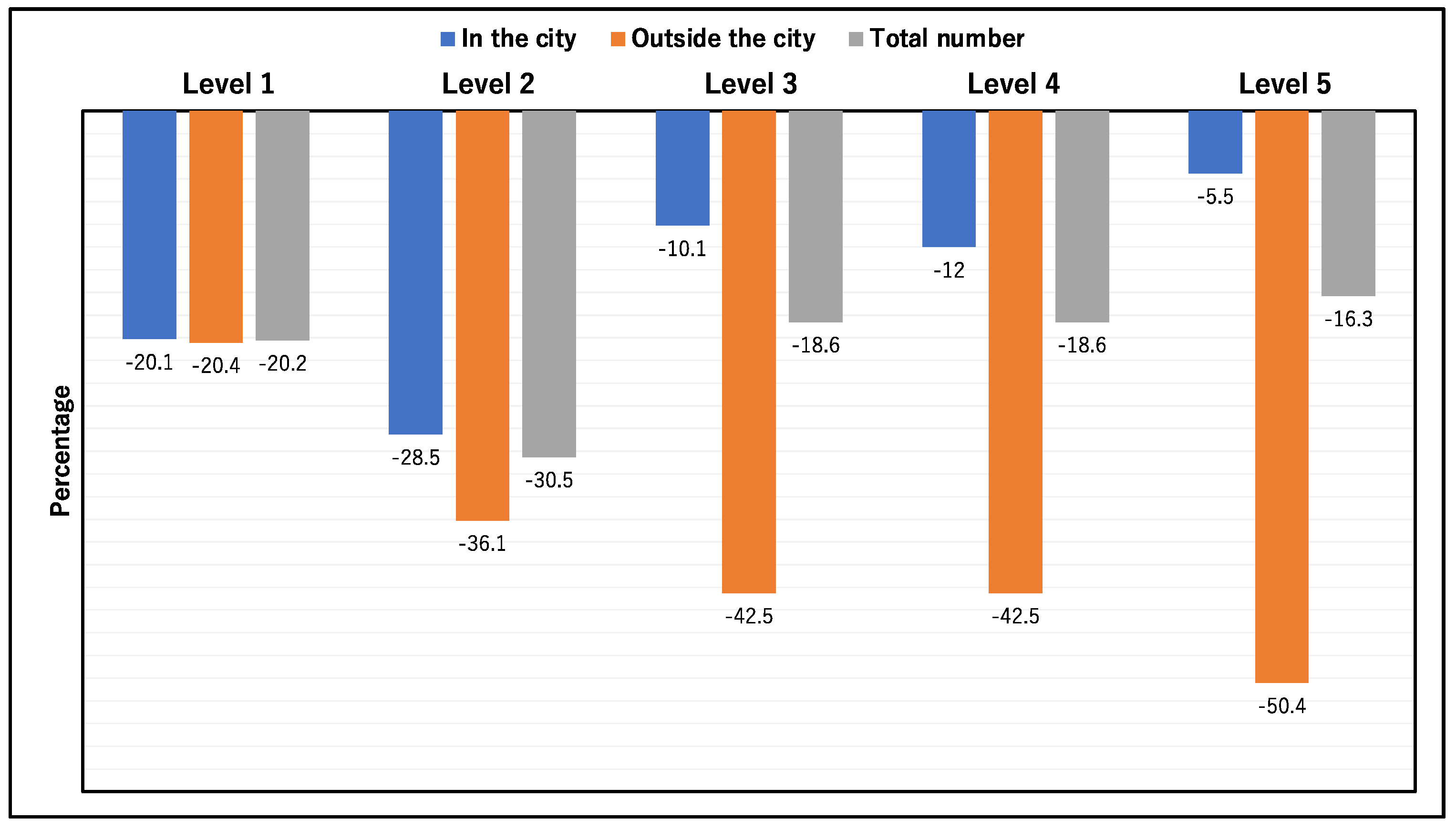
3.2. Change in Comprehensiveness of Medical Care
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hester, C.A.; Bs, N.K.; Rich, N.E.; Augustine, M.; Mansour, J.C.; Polanco, P.M.; Porembka, M.R.; Wang, S.C.; Zeh, H.J.; Singal, A.G.; et al. Effect of fragmentation of cancer care on treatment use and survival in hepatocellular carcinoma. Cancer 2019, 125, 3428–3436. [Google Scholar] [CrossRef] [PubMed]
- Clarfield, A.M.; Bergman, H.; Kane, R. Fragmentation of care for frail older people—An international problem. Experience from three countries: Israel, Canada, and the United States. J. Am. Geriatr. Soc. 2001, 49, 1714–1721. [Google Scholar] [CrossRef] [PubMed]
- Stange, K.C. The Problem of Fragmentation and the Need for Integrative Solutions. Ann. Fam. Med. 2009, 7, 100–103. [Google Scholar] [CrossRef] [Green Version]
- Wallis, K.A.; Andrews, A.; Henderson, M. Swimming against the Tide: Primary Care Physicians’ Views on Deprescribing in Everyday Practice. Ann. Fam. Med. 2017, 15, 341–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fox, A.; Reeves, S. Interprofessional collaborative patient-centred care: A critical exploration of two related discourses. J. Interprofess. Care 2015, 29, 113–118. [Google Scholar] [CrossRef]
- De Lepeleire, J.; Iliffe, S.; Mann, E.; Degryse, J.M. Frailty: An emerging concept for general practice. Br. J. Gen. Pr. 2009, 59, e177–e182. [Google Scholar] [CrossRef]
- Chiu, T.Y.; Yu, H.W.; Goto, R.; Lai, W.L.; Li, H.C.; Tsai, E.T.; Chen, Y.M. From fragmentation toward integration: A preliminary study of a new long-term care policy in a fast-aging country. BMC Geriatr. 2019, 19, 159. [Google Scholar] [CrossRef] [PubMed]
- Tsai, T.C.; Orav, E.J.; Jha, A.K. Care Fragmentation in the postdischarge period: Surgical readmissions, distance of travel, and postoperative mortality. JAMA Surg. 2015, 150, 59–64. [Google Scholar] [CrossRef] [Green Version]
- Ohta, R.; Ueno, A.; Kitayuguchi, J.; Moriwaki, Y.; Otani, J.; Sano, C. Comprehensive care through family medicine: Improving the sustainability of aging societies. Geriatrics 2021, 6, 59. [Google Scholar] [CrossRef]
- Molina, G.; Qadan, M. Addressing fragmentation of care requires strengthening of health systems and cross-institutional col-laboration. Cancer 2019, 125, 3296–3298. [Google Scholar] [CrossRef]
- Bergman, H.; Béland, F.; Lebel, P.; Contandriopoulos, A.P.; Tousignant, P.; Brunelle, Y.; Kaufman, T.; Leibovich, E.; Rodriguez, R.; Clarfield, M. Care for Canada’s frail elderly population: Fragmentation or integration? Can. Med. Assoc. J. 1997, 157, 1116–1121. [Google Scholar]
- Ford, J.A.; Turley, R.; Porter, T.; Shakespeare, T.; Wong, G.; Jones, A.P.; Steel, N. Access to primary care for so-cio-economically disadvantaged older people in rural areas: A qualitative study. PLoS ONE 2018, 13, e0193952. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, D.J. Community Susceptibility and Resiliency to COVID-19 Across the Rural-Urban Continuum in the United States. J. Rural. Health 2020, 36, 446–456. [Google Scholar] [CrossRef]
- Lawrence-Bourne, J.; Dalton, H.; Perkins, D.; Farmer, J.; Luscombe, G.; Oelke, N.; Bagheri, N. What Is Rural Adversity, How Does It Affect Wellbeing and What Are the Implications for Action? Int. J. Environ. Res. Public Health 2020, 17, 7205. [Google Scholar] [CrossRef] [PubMed]
- Hulland, E. COVID-19 and health care inaccessibility in sub-Saharan Africa. Lancet Healthy Longev. 2020, 1, e4–e5. [Google Scholar] [CrossRef]
- Cornally, N.; McCarthy, G. Help-seeking behaviour: A concept analysis. Int. J. Nurs. Pract. 2011, 17, 280–288. [Google Scholar] [CrossRef]
- Ohta, R.; Sato, M.; Ryu, Y.; Kitayuguchi, J.; Maeno, T.; Sano, C. What resources do elderly people choose for managing their symptoms? Clarification of rural older people’s choices of help-seeking behaviors in Japan. BMC Health Serv. Res. 2021, 21, 640. [Google Scholar] [CrossRef] [PubMed]
- Ohta, R.; Sato, M.; Kitayuguchi, J.; Maeno, T.; Sano, C. Potential Help-Seeking Behaviors Associated with Better Self-Rated Health among Rural Older Patients: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 9116. [Google Scholar] [CrossRef] [PubMed]
- Ohta, R.; Sato, M.; Kitayuguchi, J.; Maeno, T.; Sano, C. The Association between the Self-Management of Mild Symptoms and Quality of Life of Elderly Populations in Rural Communities: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 8857. [Google Scholar] [CrossRef] [PubMed]
- Ohta, R.; Ryu, Y.; Kitayuguchi, J.; Sano, C.; Könings, K.D. Educational intervention to improve citizen’s healthcare participation perception in rural Japanese communities: A pilot study. Int. J. Environ. Res. Public Health 2021, 18, 1782. [Google Scholar] [CrossRef] [PubMed]
- Ohta, R.; Ryu, Y.; Kitayuguchi, J.; Gomi, T.; Katsube, T. Challenges and solutions in the continuity of home care for rural older people: A thematic analysis. Home Health Care Serv. Q. 2020, 39, 126–139. [Google Scholar] [CrossRef]
- Ohta, R.; Ryu, Y.; Sano, C. Fears Related to COVID-19 among Rural Older People in Japan. Healthcare 2021, 9, 524. [Google Scholar] [CrossRef]
- Ohta, R.; Ryu, Y.; Otani, J. Rural physicians’ perceptions about the challenges of participating in interprofessional collaboration: Insights from a focus group study. J. Interprof. Educ. Pract. 2020, 20, 100345. [Google Scholar] [CrossRef]
- Harden, K.; Price, D.M.; Mason, H.; Bigelow, A. COVID-19 Shines a Spotlight on the Age-Old Problem of Social Isolation. J. Hosp. Palliat. Nurs. 2020, 22, 435–441. [Google Scholar] [CrossRef] [PubMed]
- Dubey, S.; Biswas, P.; Ghosh, R.; Chatterjee, S.; Dubey, M.J.; Chatterjee, S.; Lahiri, D.; Lavie, C.J. Psychosocial impact of COVID-19. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 779–788. [Google Scholar] [CrossRef] [PubMed]
- Ohta, R.; Ryu, Y.; Sato, M.; Maeno, T. ICT-driven improvement of interprofessional collaboration between a rural clinic and nursing home: A mixed method. J. Interprofess. Educ. Pr. 2020, 21, 100380. [Google Scholar] [CrossRef]
- Ohta, R.; Ryu, Y.; Sano, C. Effects of Implementation of Infection Control Measures against COVID-19 on the Condition of Japanese Rural Nursing Homes. Int. J. Environ. Res. Public Health 2021, 18, 5805. [Google Scholar] [CrossRef] [PubMed]
- Ohta, R.; Ryu, Y.; Kataoka, D.; Sano, C. Effectiveness and Challenges in Local Self-Governance: Multifunctional Autonomy in Japan. Int. J. Environ. Res. Public Health 2021, 18, 574. [Google Scholar] [CrossRef] [PubMed]
- Ohta, R.; Ryu, Y. Improvement in palliative care quality in rural nursing homes through information and communication technology-driven interprofessional collaboration. Rural. Remote. Health 2021, 21, 6450. [Google Scholar] [CrossRef]
- Shimizutani, S. The Future of Long-term Care in Japan. Asia-Pac. Rev. 2014, 21, 88–119. [Google Scholar] [CrossRef] [Green Version]
- Kanda, Y. Investigation of the freely available easy-to-use software “EZR” for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef] [Green Version]
- May, T. Lockdown-type measures look effective against covid-19. BMJ 2020, 370, m2809. [Google Scholar] [CrossRef] [PubMed]
- Lundberg, A.; Hillebrecht, A.; McKenna, G.; Srinivasan, M. COVID-19: Impacts on oral healthcare delivery in dependent older adults. Gerodontology 2021, 38, 174–178. [Google Scholar] [CrossRef] [PubMed]
- Arthur-Holmes, F.; Agyemang-Duah, W. Reaching older adults during the COVID-19 pandemic through social networks and Social Security Schemes in Ghana: Lessons for considerations. J. Gerontol. Soc. Work. 2020, 63, 699–701. [Google Scholar] [CrossRef] [PubMed]
- Jiang, P.; Klemeš, J.; Fan, Y.; Fu, X.; Bee, Y. More is Not Enough: A Deeper Understanding of the COVID-19 Impacts on Healthcare, Energy and Environment is Crucial. Int. J. Environ. Res. Public Health 2021, 18, 684. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, R. Telehealth and COVID-19: Using technology to accelerate the curve on access and quality healthcare for citizens in India. Technol. Soc. 2021, 64, 101465. [Google Scholar] [CrossRef]
- Chan, N.H.; Lee, S.Y.; Cheng, N.H.Y.; Wong, H.Y.; Lo, W.K.; Lung, D.C. Hospital infection control best practice: Five essential elements to successfully minimize healthcare-associated COVID-19. Infect. Prev. Pract. 2021, 3, 100110. [Google Scholar] [CrossRef]
- Chou, E.; Hsieh, Y.-L.; Wolfshohl, J.; Green, F.; Bhakta, T. Onsite telemedicine strategy for coronavirus (COVID-19) screening to limit exposure in ED. Emerg. Med. J. 2020, 37, 335–337. [Google Scholar] [CrossRef]
- Ohta, R.; Yoshinori, R.; Sato, M.; Maeno, T. Challenges of using ICT regarding acute conditions in rural home care: A thematic analysis. J. Interprof. Educ. Pract. 2020, 20, 100349. [Google Scholar] [CrossRef]
- Kronenfeld, J.P.; Penedo, F.J. Novel Coronavirus (COVID-19): Telemedicine and remote care delivery in a time of medical crisis, implementation, and challenges. Transl. Behav. Med. 2021, 11, 659–663. [Google Scholar] [CrossRef]
- Hoot, N.R.; Aronsky, D. Systematic Review of Emergency Department Crowding: Causes, Effects, and Solutions. Ann. Emerg. Med. 2008, 52, 126–136.e1. [Google Scholar] [CrossRef]
- Huang, M.; van der Borght, C.; Leithaus, M.; Flamaing, J.; Goderis, G. Patients’ perceptions of frequent hospital admissions: A qualitative interview study with older people above 65 years of age. BMC Geriatr. 2020, 20, 332. [Google Scholar] [CrossRef]
- Iwasaki, A.; Grubaugh, N.D. Why does Japan have so few cases of COVID-19? EMBO. Mol. Med. 2020, 12, e12481. [Google Scholar]
- Rivera-Hernandez, M.; Ferdows, N.B.; Kumar, A. The Impact of the COVID-19 Epidemic on Older Adults in Rural and Urban Areas in Mexico. J. Gerontol. Ser. B 2021, 76, e268–e274. [Google Scholar] [CrossRef] [PubMed]
- Van Dyck, L.I.; Wilkins, K.M.; Ouellet, J.; Ouellet, G.M.; Conroy, M.L. Combating Heightened Social Isolation of Nursing Home Elders: The Telephone Outreach in the COVID-19 Outbreak Program. Am. J. Geriatr. Psychiatry 2020, 28, 989–992. [Google Scholar] [CrossRef] [PubMed]
- Hossain, M.A.; Jahid, I.K.; Hossain, K.M.A.; Walton, L.M.; Uddin, Z.; Haque, O.; Kabir, F.; Arafat, S.M.Y.; Sakel, M.; Faruqui, R.; et al. Knowledge, attitudes, and fear of COVID-19 during the Rapid Rise Period in Bangladesh. PLoS ONE 2020, 15, e0239646. [Google Scholar] [CrossRef] [PubMed]
- Liapikou, A.; Tzortzaki, E.; Hillas, G.; Markatos, M.; Papanikolaou, I.; Kostikas, K. Outpatient Management of COVID-19 Disease: A Holistic Patient-Centered Proposal Based on the Greek Experience. J. Pers. Med. 2021, 11, 709. [Google Scholar] [CrossRef] [PubMed]
- Rossi, A.A.; Marconi, M.; Taccini, F.; Verusio, C.; Mannarini, S. From fear to hopelessness: The buffering effect of patient-centered communication in a sample of oncological patients during COVID-19. Behav. Sci. 2021, 11, 87. [Google Scholar] [CrossRef] [PubMed]
- Record, J.D.; Ziegelstein, R.C.; Christmas, C.; Rand, C.S.; Hanyok, L.A. Delivering personalized care at a distance: How telemedicine can foster getting to know the patient as a person. J. Pers. Med. 2021, 11, 137. [Google Scholar] [CrossRef]
- Shaw, C.; Brittain, K.; Tansey, R.; Williams, K. How people decide to seek health care: A qualitative study. Int. J. Nurs. Stud. 2008, 45, 1516–1524. [Google Scholar] [CrossRef]

{kind=link}
| Total | Care Level 1 (%) | Care Level 2 (%) | Care Level 3 (%) | Care Level 4 (%) | Care Level 5 (%) | p | |
|---|---|---|---|---|---|---|---|
| Men | |||||||
| 2018 | 575 | 123 (21.4) | 153 (26.6) | 129 (22.4) | 87 (15.1) | 83 (14.4) | 0.691 |
| 2020 | 437 | 96 (22.0) | 103 (23.6) | 94 (22.0) | 78 (17.8) | 66 (15.1) | |
| Women | |||||||
| 2018 | 1480 | 347 (23.4) | 387 (26.1) | 263 (17.8) | 265 (17.9) | 218 (14.7) | 0.691 |
| 2020 | 1252 | 274 (21.9) | 291 (23.3) | 255 (20.4) | 229 (18.3) | 203 (13.4) | |
| Age | |||||||
| 80> | |||||||
| 2018 | 135 | 39 (28.9) | 47 (34.8) | 23 (17.0) | 16 (11.9) | 10 (7.4) | 0.633 |
| 2020 | 84 | 18 (21.4) | 29 (34.5) | 17 (20.2) | 10 (11.9) | 10 (11.9) | |
| 80–84 | |||||||
| 2018 | 267 | 71 (26.6) | 81 (30.3) | 52 (19.5) | 32 (12.0) | 31 (11.6) | 0.184 |
| 2020 | 130 | 46 (35.4) | 31 (23.8) | 18 (13.8) | 14 (10.8) | 20 (15.4) | |
| 85–89 | |||||||
| 2018 | 626 | 158 (25.2) | 153 (24.4) | 110 (17.6) | 110 (17.6) | 95 (15.2) | 0.965 |
| 2020 | 495 | 121 (24.4) | 117 (23.6) | 87 (17.6) | 87 (17.6) | 83 (16.8) | |
| 90–94 | |||||||
| 2018 | 635 | 145 (22.8) | 171 (26.9) | 117 (18.4) | 111 (17.5) | 91 (14.3) | 0.297 |
| 2020 | 594 | 132 (22.2) | 131 (22.1) | 126 (21.2) | 112 (18.9) | 93 (15.7) | |
| 95≤ | |||||||
| 2018 | 392 | 57 (14.5) | 88 (22.4) | 90 (23.0) | 83 (21.2) | 74 (18.9) | 0.799 |
| 2020 | 387 | 53 (13.7) | 86 (22.2) | 101 (26.1) | 84 (21.7) | 63 (16.3) |
| Care Level | In the City | Outside the City | Total Number | Proportion of Comprehensiveness | p |
|---|---|---|---|---|---|
| Level 1 | |||||
| 2018 | 427 | 176 | 603 | 0.708 | 1 |
| 2020 | 341 | 140 | 481 | 0.709 | |
| Level 2 | |||||
| 2018 | 505 | 180 | 685 | 0.737 | 0.451 |
| 2020 | 361 | 115 | 476 | 0.758 | |
| Level 3 | |||||
| 2018 | 355 | 128 | 483 | 0.735 | 0.020 |
| 2020 | 319 | 78 | 410 | 0.778 | |
| Level 4 | |||||
| 2018 | 316 | 120 | 436 | 0.725 | 0.015 |
| 2020 | 278 | 69 | 355 | 0.783 | |
| Level 5 | |||||
| 2018 | 271 | 85 | 356 | 0.761 | 0.002 |
| 2020 | 256 | 42 | 298 | 0.859 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ohta, R.; Ueno, A.; Sano, C. Changes in the Comprehensiveness of Rural Medical Care for Older Japanese Patients during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 10772. https://doi.org/10.3390/ijerph182010772
Ohta R, Ueno A, Sano C. Changes in the Comprehensiveness of Rural Medical Care for Older Japanese Patients during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2021; 18(20):10772. https://doi.org/10.3390/ijerph182010772
Chicago/Turabian StyleOhta, Ryuichi, Akinori Ueno, and Chiaki Sano. 2021. "Changes in the Comprehensiveness of Rural Medical Care for Older Japanese Patients during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 18, no. 20: 10772. https://doi.org/10.3390/ijerph182010772
APA StyleOhta, R., Ueno, A., & Sano, C. (2021). Changes in the Comprehensiveness of Rural Medical Care for Older Japanese Patients during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 18(20), 10772. https://doi.org/10.3390/ijerph182010772