
“Getting Used to It, but Still Unwelcome”: A Grounded Theory Study of Physical Identity Development in Later Life


Abstract
:1. Introduction
2. Methods
2.1. Data Collection
2.2. Theoretical Sampling
2.3. Data Analysis
3. Results
3.1. Participants Overview
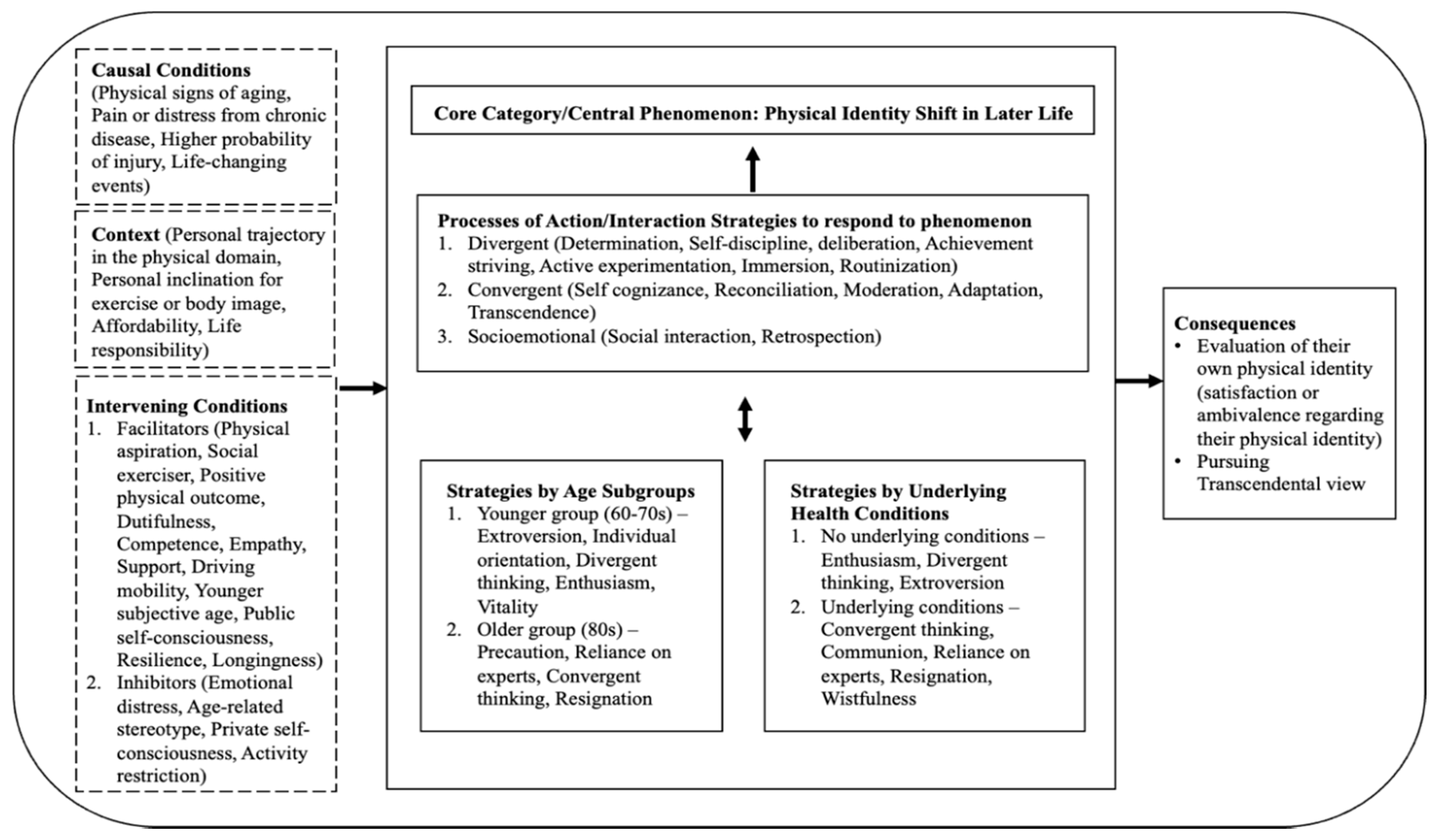
3.2. Core Category: Physical Identity Shift in Later Life
3.3. Three Traits of Processes in Action/Interactional Strategies
3.3.1. Divergent Process
“It works almost like a spring or a tension… when you take your golf swing, you go back here, you come through. This is you take it back here, and you caulk here. And then when you swing through you, and it gives it a lot more speed, a lot more power”.
3.3.2. Convergent Process
3.3.3. Socioemotional Process
3.4. Age Subgroups and Underlying Health Conditions
3.4.1. Younger-Old Group (60s–70s Age Group)
“Every day, every, every day, and most of the time I feel like I should be doing more. But the business has eaten up my time. We can be in the office all day. So, we’re making a concerted effort both my wife and myself making a concerted effort to try to carve out time each day for us to do that”.
“He (my son) has now gotten me, we are working on different sections to give those muscles a chance to recuperate, where I would work on chest and arms over and over again, and what he is teaching me is that when I do that, I tear the muscle down, but I don’t give the muscles the chance to recover”.
“My biggest concern is that I am energetic enough and enthusiastic enough that I find it very, very easy to overdo it. I can go too far. And I feel like I’m not doing enough again, need to do more … And my wife is constantly reminding me that I’m doing too much I’m trying to do too much. That’s the biggest issue”.
3.4.2. Older-Old Group (80s Age Group)
“I am more careful because I’m in that very dangerous age group. And I do have heart failure, so I’m aware that atrial fibrillation… I’m aware that I’m vulnerable. So, I’m very cautious. When they tell me to stay at home, I stay at home. They want us to wear the mask, I wear a mask”.
3.4.3. Without Underlying Health Conditions
“Just to be active and play regularly … And I go to tournaments every once in a while. I play two, three, couple, three tournaments a year that come up, where you’re playing against people from other states or other towns. Some of those are goals to keep yourself ready, capable to participate in those events”.
“Now it’s got to be sort of a challenge to be able to hit that 33 separate times in the morning. Someday will be a day in the future, whether that’s going to be tomorrow, or when it’s going to be a year or two years from now three years from now, I will be able to hit that”.
“Also doing things and then not keeping them up is also painful. You go through the process of exercising and go through that soreness period, and then you stop. And then you have to start all over again and go through that whole process again”.
3.4.4. With Underlying Health Conditions
3.5. Conceptualization of Physical Identity Shift in Later Life
4. Discussion
4.1. Physical Activities and Perceptions of Aging
4.2. Physical Identity Development through Exercise Engagement
4.3. Various Age Subgroups and Underlying Health Conditions
5. Limitations and Future Directions
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Moos, R.H.; Brennan, P.L.; Schutte, K.K.; Moos, B.S. Older adults’ coping with negative life events: Common processes of managing health, interpersonal, and financial/work stressors. Int. J. Aging Hum. Dev. 2006, 62, 39–59. [Google Scholar] [CrossRef] [PubMed]
- Whitbourne, S.K.; Whitbourne, S.B. Adult Development & Aging: Biopsychosocial Perspectives, 5th ed.; John Wiley & Sons: New York, NY, USA, 2014. [Google Scholar]
- Biasin, C.; Evans, K. Agency, identity and learning at turning points in women’s lives: A comparative UK-Italian analysis. Eur. J. Res. Educ. Learn. Adults 2019, 10, 47–63. [Google Scholar] [CrossRef]
- Jovic, E.; McMullin, J. Learning and aging. In Handbook of Sociology of Aging; Settersten, R.A., Angel, J.L., Eds.; Springer: New York, NY, USA, 2011; pp. 229–244. [Google Scholar]
- Nelson, M.E.; Rejeski, W.J.; Blair, S.N.; Duncan, P.W.; Judge, J.O.; King, A.C.; Macera, C.A.; Castaneda-Sceppa, C. Physical activity and public health in older adults: Recommendation from the American College of Sports Medicine and the American Heart Association. Circulation 2007, 116, 1094–1105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Capalb, D.J.; O’Halloran, P.; Liamputtong, P. Why older people engage in physical activity: An exploratory study of participants in a community-based walking program. Aust. J. Prim. Health 2014, 20, 74–78. [Google Scholar] [CrossRef] [Green Version]
- Stenner, B.J.; Mosewich, A.D.; Buckley, J.D. An exploratory investigation into the reasons why older people play golf. Qual. Res. Sport. Exerc. Health 2016, 8, 257–272. [Google Scholar] [CrossRef]
- Gray, P.; Murphy, M.; Gallagher, A.; Simpson, E.E.A. A qualitative investigation of physical activity compensation among older adults. Br. J. Health Psychol. 2018, 23, 208–224. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services. Physical Activity Guidelines for Americans. Available online: https://health.gov/paguidelines/second-edition/ (accessed on 26 June 2021).
- Centers for Disease Control and Prevention. Adults Need More Physical Activity. Available online: https://www.cdc.gov/physicalactivity/inactivity-among-adults-50plus/index.html (accessed on 26 June 2021).
- Hardcastle, S.; Taylor, A.H. Finding an exercise identity in an older body: “It’s redefining yourself and working out who you are”. Psychol. Sport Exerc. 2005, 6, 173–188. [Google Scholar] [CrossRef]
- Kenter, E.J.; Gebhardt, W.A.; Lottman, I.; van Rossum, M.; Bekedam, M.; Crone, M.R. The influence of life events on physical activity patterns of Dutch older adults: A life history method. Psychol. Health 2015, 30, 627–651. [Google Scholar] [CrossRef]
- Anderson, D.F.; Cychosz, C.M. Development of an exercise identity scale. Percept. Mot. Ski. 1994, 78, 747–751. [Google Scholar] [CrossRef]
- Bocknek, G.; Perna, F. Studies in self-representation beyond childhood. In Empirical Perspectives on Object Relations Theory; Masling, J.M., Bornstein, R.F., Eds.; American Psychological Association: Washington, DC, USA, 1994; pp. 29–58. [Google Scholar] [CrossRef]
- Rhodes, R.E.; Kaushal, N.; Quinlan, A. Is physical activity a part of who I am? A review and meta-analysis of identity, schema and physical activity. Health Psychol. Rev. 2016, 10, 204–225. [Google Scholar] [CrossRef]
- Strachan, S.M.; Brawley, L.R. Reactions to a perceived challenge to identity: A focus on exercise and healthy eating. J. Health Psychol. 2008, 13, 575–588. [Google Scholar] [CrossRef]
- Gardner, P. The role of social engagement and identity in community mobility among older adults aging in place. Disabil. Rehabil. 2014, 36, 1249–1257. [Google Scholar] [CrossRef]
- Graves, S.B.; Larkin, E. Lessons from Erikson: A look at autonomy across the lifespan. J. Intergener. Relatsh. 2006, 4, 61–71. [Google Scholar] [CrossRef]
- Griffith, J.; Caron, C.D.; Desrosiers, J.; Thibeault, R. Defining spirituality and giving meaning to occupation: The perspective of community-dwelling older adults with autonomy loss. Can. J. Occup. Ther. 2007, 74, 78–90. [Google Scholar] [CrossRef] [PubMed]
- Strachan, S.M.; Brawley, L.R.; Spink, K.; Glazebrook, K. Older adults’ physically-active identity: Relationships between social cognitions, physical activity and satisfaction with life. Psychol. Sport Exerc. 2010, 11, 114–121. [Google Scholar] [CrossRef]
- Pelssers, J.; Hurkmans, E.; Scheerder, J.; Vanbeselaere, N.; Vos, S.; Smits, T.; Boen, F. Acting one’s age in physical exercise: Do perceived age norms explain autonomous motivation among older adults? J. Aging Phys. Act. 2018, 26, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Dionigi, R.A. Older sportswomen: Personal and cultural meanings of resistance and conformity. Int. J. Interdiscip. Soc. Sci. 2010, 5, 395–408. [Google Scholar] [CrossRef] [Green Version]
- Perras, M.G.; Strachan, S.M.; Fortier, M.S. Possible selves and physical activity in retirees: The mediating role of identity. Res. Aging 2016, 38, 819–841. [Google Scholar] [CrossRef] [PubMed]
- Strauss, A.; Corbin, J. Basics of Qualitative Research: Grounded Theory Procedures and Techniques; Sage: New York, NY, USA, 1990. [Google Scholar]
- Strauss, A.L.; Corbin, J.M. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory, 2nd ed.; Sage: New York, NY, USA, 1998. [Google Scholar]
- Hesse-Biber, S.N. The Practice of Qualitative Research: Engaging Students in the Research Process, 3rd ed.; Sage: New York, NY, USA, 2017. [Google Scholar]
- Forrester, M.A.; Sullivan, C. Doing Qualitative Research in Psychology: A Practical Guide, 2nd ed.; Sage: New York, NY, USA, 2019. [Google Scholar]
- Denzin, N.K.; Lincoln, Y.S. The Sage Handbook of Qualitative Research, 5th ed.; Sage: New York, NY, USA, 2018. [Google Scholar]
- Glaser, B.G.; Strauss, A.L. The Discovery of Grounded Theory: Strategies for Qualitative Research; Aldine Pub. Co.: New Brunswick, NJ, USA, 1967. [Google Scholar]
- Charmaz, K. Constructing Grounded Theory: A Practical Guide through Qualitative Analysis; Sage: New York, NY, USA, 2006. [Google Scholar]
- Glaser, B. Theoretical Sensitivity: Advances in the Methodology of Grounded Theory; Sociology Press: Mill Valley, CA USA, 1978. [Google Scholar]
- Birks, M.; Mills, J. Grounded Theory: A Practical Guide, 2nd ed.; Sage: New York, NY, USA, 2015. [Google Scholar]
- Brady, M.; Loonam, J. Exploring the use of entity-relationship diagramming as a technique to support grounded theory inquiry. Qual. Res. Organ. Manag. 2010, 5, 224–237. [Google Scholar] [CrossRef] [Green Version]
- Clarke, A.E. Situational Analysis: Grounded Theory after the Postmodern Turn; Sage: New York, NY, USA, 2005. [Google Scholar] [CrossRef]
- Guilford, J.P. The Nature of Human Intelligence; McGraw-Hill: New York, NY, USA, 1967. [Google Scholar]
- Hommel, B.; Colzato, L.S.; Fischer, R.; Christoffels, I. Bilingualism and creativity: Benefits in convergent thinking come with losses in divergent thinking. Front. Psychol. 2011, 2, 273. [Google Scholar] [CrossRef] [Green Version]
- Michael, W.B.; Wright, C.R. Psychometric issues in the assessment of creativity. In Handbook of Creativity; Glover, J.A., Ronning, R.R., Reynolds, C.R., Eds.; Plenum: New York, NY, USA, 1989; pp. 33–52. [Google Scholar]
- Runco, M.A. Creativity. Annu. Rev. Psychol. 2004, 55, 657–687. [Google Scholar] [CrossRef]
- Zhu, W.; Shang, S.; Jiang, W.; Pei, M.; Su, Y. Convergent thinking moderates the relationship between divergent thinking and scientific creativity. Creat. Res. J. 2019, 31, 320–328. [Google Scholar] [CrossRef]
- Rathunde, K.; Isabella, R. Play, flow, and tailoring identity in middle adulthood. In Identity Flexibility during Adulthood; Sinnott, J.D., Ed.; Springer: New York, NY, USA, 2017; pp. 211–232. [Google Scholar]
- Rathunde, K.; Csikszentmihalyi, M. The developing person: An experiential perspective. In Handbook of Child Psychology; Lerner, R.M., Ed.; Wiley: Hoboken, NJ, USA, 2006; Volume 1, pp. 465–515. [Google Scholar]
- Erden, A.; Güner, S.G. Impact of exercise on quality of life, body awareness, kinesiophobia and the risk of falling among young older adults. Çukurova Med. J. 2018, 43, 941–950. [Google Scholar]
- Fougner, M.; Bergland, A.; Lund, A.; Debesay, J. Aging and exercise: Perceptions of the active lived-body. Physiother. Theory Pract. 2019, 35, 651–662. [Google Scholar] [CrossRef]
- World Health Organization. Active Ageing: A Policy Framework. Available online: https://apps.who.int/iris/bitstream/handle/10665/67215/WHO_NMH_NPH_02.8.pdf;jsessionid=0C2F7C5651F6E54C96C2CA8394676B22?sequence=1 (accessed on 28 June 2021).
- Walker, A. A strategy for active ageing. Int. Soc. Secur. Rev. 2002, 55, 121–139. [Google Scholar] [CrossRef]
- Boulton-Lewis, G.M.; Buys, L.; Lovie-Kitchin, J. Learning and active aging. Educ. Gerontol. 2006, 32, 271–282. [Google Scholar] [CrossRef]
- Mendoza-Ruvalcaba, N.M.; Arias-Merino, E.D. “I am active”: Effects of a program to promote active aging. Clin. Interv. Aging 2015, 10, 829–837. [Google Scholar] [CrossRef] [Green Version]
- Tulle, E. Acting your age? Sports science and the ageing body. J. Aging Stud. 2008, 22, 340–347. [Google Scholar] [CrossRef]
- Vincent, J.A. Ageing contested: Anti-ageing science and the cultural construction of old age. Sociology 2006, 40, 681–698. [Google Scholar] [CrossRef]
- Marcia, J.E. Identity in adolescence. In Handbook of Adolescent Psychology; Adelson, J., Ed.; Wiley: Hoboken, NJ, USA, 1980; pp. 159–187. [Google Scholar]
- Berlyne, D.E. Aesthetics and Psychobiology; Appleton-Century-Crofts: Norwalk, CT, USA, 1971. [Google Scholar]
- Baltes, P.B. On the incomplete architecture of human ontogeny: Selection, optimization and compensation as foundation of developmental theory. Am. Psychol. 1997, 52, 366–380. [Google Scholar] [CrossRef]
- Breakwell, G.M. Coping with Threatened Identities; Psychology Press: London, UK, 1986. [Google Scholar]
- Whitbourne, S.K. The Me I Know: A Study of Adult Identity; Springer: New York, NY, USA, 1986. [Google Scholar]
- Jaspal, R.; Cinnirella, M. Coping with potentially incompatible identities: Accounts of religious, ethnic, and sexual identities from British Pakistani men who identify as Muslim and gay. Br. J. Soc. Psychol. 2010, 49, 849–870. [Google Scholar] [CrossRef] [PubMed]
- Cappeliez, P.; Robitaille, A. Coping mediates the relationships between reminiscence and psychological well-being among older adults. Aging Ment. Health 2010, 14, 807–818. [Google Scholar] [CrossRef] [PubMed]
- Rothermund, K.; Brandstädter, J. Coping with deficits and losses in later life: From compensatory action to accommodation. Psychol. Aging 2003, 18, 896–905. [Google Scholar] [CrossRef] [PubMed]
- Frazier, L.D.; Newman, F.L.; Jaccard, J. Psychosocial outcomes in later life: A multivariate model. Psychol. Aging 2007, 22, 676–689. [Google Scholar] [CrossRef]
- Whitbourne, S.K.; Sneed, J.R. The paradox of well-being, identity processes, and stereotype threat: Ageism and its potential relationships to Ethe self in later life. In Ageism: Stereotyping and Prejudice against Older Persons; Nelson, T.D., Ed.; MIT Press: Cambridge, MA, USA, 2002; pp. 247–273. [Google Scholar]
- Koo, Y.W.; Kõlves, K.; De Leo, D. Suicide in older adults: Differences between the young-old, middle-old, and oldest old. Int. Psychogeriatr. 2017, 29, 1297–1306. [Google Scholar] [CrossRef]
- Zizza, C.A.; Ellison, K.J.; Wernette, C.M. Total water intakes of community-living middle-old and oldest-old adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2009, 64, 481–486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.B.; Oh, J.H.; Park, J.H.; Choi, S.P.; Wee, J.H. Differences in youngest-old, middle-old, and oldest-old patients who visit the emergency department. Clin. Exp. Emerg. Med. 2018, 5, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Jin, B.; Kim, J.; Baumgartner, L.M. Informal learning of older adults in using mobile devices: A review of the literature. Adult Educ. Q. 2019, 69, 120–141. [Google Scholar] [CrossRef]
- Hardy, S.E.; Studenski, S.A. Qualities of fatigue and associated chronic conditions among older adults. J. Pain Symptom Manag. 2010, 39, 1033–1042. [Google Scholar] [CrossRef]
- Colón-Emeric, C.S.; Whitson, H.E.; Pavon, J.; Hoenig, H. Functional decline in older adults. Am. Fam. Physician 2013, 88, 388–394. [Google Scholar]
- Chen, L.K.; Kim, Y.S.; Moon, P.; Merriam, S.B. A review and critique of the portrayal of older adult learners in adult education journals, 1980–2006. Adult Educ. Q. 2008, 59, 3–21. [Google Scholar] [CrossRef]
- Kelley-Moore, J.A.; Lin, J. Widening the view: Capturing “unobserved” heterogeneity in studies of age and the life course. In Handbook of Sociology of Aging; Settersten, R.A., Angel, J.L., Eds.; Springer: New York, NY, USA, 2011; pp. 51–68. [Google Scholar]
- Spini, D.; Jopp, D.S.; Pin, S.; Stringhini, S. The multiplicity of aging: Lessons for theory and conceptual development from longitudinal studies. In Handbook of Theories of Aging; Bengtson, V.L., Settersten, R., Eds.; Springer: New York, NY, USA, 2016; pp. 669–690. [Google Scholar]

{kind=link}
| 60s–70s Age Group | 80s Age Group | |
|---|---|---|
| With Underlying Health Conditions | 72 years, pinched nerve in the back 76 years, heart failure, pacemaker 77 years, chronic back pain | 81 years, arthritis, osteoporosis, heart issue, replacement knee 83 years, scoliosis 83 years, vision impairment, heart failure 84 years, bad knee, feet issues, back pain 85 years, back issue 88 years, severe back problems, nerve pain 89 years, heart issue, hearing issue |
| Without Underlying Health Conditions | 67 years 69 years | Analytical need for participants who were in their 80s without underlying conditions |
| Elements of the Paradigm Model | Categories |
|---|---|
| Phenomenon | Physical identity shift in later life |
| Causal conditions | Physical signs of aging, pain or distress from chronic disease, a higher probability of injury, life-changing events |
| Context | Personal trajectory in the physical domain, personal inclination for exercise or body image, affordability, life responsibility |
| Intervening conditions (inhibitor) | Emotional distress, age-related stereotype, private self-consciousness, activity restriction |
| Intervening conditions (facilitator) | Physical aspiration, social exerciser, positive physical outcome, dutifulness, competence, empathy, supports, driving mobility, younger subjective age, public self-consciousness, resilience, longingness |
| Action/Interactional Strategies | Determination, self-discipline, deliberation, achievement striving, active experimentation, immersion, routinization, self-cognizance, reconciliation, moderation, adaptation, transcendence, social interaction, retrospection |
| Consequences | Evaluation of their own physical identity (satisfaction or ambivalence regarding their physical identity), transcendental views |
| Pseudonym | Gender | Age | Main Activity | Levels of Physical Activity | Exercise Status/Preference |
|---|---|---|---|---|---|
| Sherry | Female | 85 | Senior exercise program, gym, walking, water aerobics | Active | Active living, social exerciser |
| Karolyn | Female | 83 | Self-workout at home, Senior exercise program, walking | Active | Active living, social exerciser |
| Meghan | Female | 77 | Senior exercise program, self-workout at home, walking | Active | Active living, social exerciser |
| Bonnie | Female | 81 | Senior exercise program, walking, water aerobics | Highly active | Active living, social exerciser |
| Sean | Male | 69 | Golf, gym | Highly active | Solitary exerciser (but engaged in social exercise groups) |
| Nicole | Female | 84 | Senior exercise program, water aerobics, walking | Active | Active living, social exerciser |
| Artie | Female | 72 | Senior exercise program, walking, swimming | Active | Active living, solitary exercise |
| Tacey | Female | 88 | Senior exercise program, walking, water aerobics | Active | Active living, social exerciser |
| Kayla | Female | 89 | Senior exercise program, walking | Active | Active living, social exerciser |
| Emilia | Female | 83 | Senior exercise program, gym | Active | Social exerciser |
| Stanley | Male | 76 | Golf, walking, self-workout at home | Highly active | Active living, solitary exerciser |
| Annika | Female | 67 | Walking, self-workout at home | Highly active | Active living, solitary exerciser |
| Clifford | Male | 84 | Golf, gym, walking | Highly active | Social exerciser |
| Diane | Female | 74 | Walking, golf, cycling | Active | Solitary exerciser |
| Elvin | Male | 81 | Self-workout at home, golf, walking | Highly active | Active living, social exerciser |
| Trait of Process | Categories | Definition |
|---|---|---|
| Divergent | Determination | Strong decision to continue trying to do something despite the difficulty |
| Self-discipline | Ability to begin the exercise-related tasks and carry them through to the goal achievement | |
| Deliberation | Careful consideration before taking action or situations that occur | |
| Achievement striving | Attitude of seeking improvement to reach a goal with a lot of effort | |
| Active experimentation | Process of trying out a new idea or method to find out more effective ways | |
| Immersion | Engrossment or active involvement in that activity | |
| Routinization | Practice of regularly performing activities that are performed as a normal part of daily life | |
| Convergent | Self-cognizance | Realization of one’s own physical and mental conditions and abilities |
| Reconciliation | Process of finding a way between seemingly opposite things in which both can be successful | |
| Moderation | Acting in a way that is not extreme | |
| Adaptation | Act of changing personal behaviors or beliefs to adapt to a new situation or purpose | |
| Transcendence | Insight or way of behaving that lie beyond the practical experience of ordinary people, and cannot be understood by ordinary reasoning | |
| Socioemotional (throughout the process) | Social interaction | Belief based on the notion that meanings are shared and constructed between people |
| Retrospection | Act of recalling things in the past, especially in one’s personal experience about physical activities |
| Property | Definition of Property |
|---|---|
| Extroversion | A tendency to be outgoing, talkative, and exhibit energetic behavior |
| Individual orientation | A tendency to emphasize one’s personal goals and achievement |
| Divergent thinking | A thought process distinguished by exploring multiple ideas to generate new possible solutions to problems |
| Enthusiasm | Great eagerness to be involved in a particular activity that one enjoys or thinks is important |
| Vitality | A state of being strong, active, and enthusiastic |
| Property | Definition of Property |
|---|---|
| Precaution | An action that is intended to prevent dangerous or unpleasant situations from happening |
| Reliance on experts | A tendency to do things and make decisions with advice from experts in terms of physical activity and health |
| Convergent thinking | A thought process of integration based on existing knowledge and experiences to come up with a single, well-established answer |
| Resignation | Acceptance with reluctant feelings, but knowing that something cannot be changed |
| Property | Definition of Property |
|---|---|
| Enthusiasm | Great eagerness to be involved in a particular activity that one enjoys or thinks is important |
| Divergent thinking | A thought process distinguished by exploring multiple ideas to generate new possible solutions to problems |
| Extroversion | A tendency to be outgoing, talkative, and do energetic behavior |
| Property | Definitions of Property |
|---|---|
| Convergent thinking | A thought process of integration of existing knowledge and experiences to come up with a single, well-established answer |
| Communion | A state of a sense by which one shares or exchanges intimate thoughts and feelings with others |
| Reliance on experts | A tendency to do things and make decisions as advised by experts |
| Resignation | Acceptance with reluctant feelings, but knowing that something cannot be changed |
| Wistfulness | A state of a sense of missing something that one can never regain |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jin, B.; Roumell, E.A. “Getting Used to It, but Still Unwelcome”: A Grounded Theory Study of Physical Identity Development in Later Life. Int. J. Environ. Res. Public Health 2021, 18, 9557. https://doi.org/10.3390/ijerph18189557
Jin B, Roumell EA. “Getting Used to It, but Still Unwelcome”: A Grounded Theory Study of Physical Identity Development in Later Life. International Journal of Environmental Research and Public Health. 2021; 18(18):9557. https://doi.org/10.3390/ijerph18189557
Chicago/Turabian StyleJin, Bora, and Elizabeth A. Roumell. 2021. "“Getting Used to It, but Still Unwelcome”: A Grounded Theory Study of Physical Identity Development in Later Life" International Journal of Environmental Research and Public Health 18, no. 18: 9557. https://doi.org/10.3390/ijerph18189557
APA StyleJin, B., & Roumell, E. A. (2021). “Getting Used to It, but Still Unwelcome”: A Grounded Theory Study of Physical Identity Development in Later Life. International Journal of Environmental Research and Public Health, 18(18), 9557. https://doi.org/10.3390/ijerph18189557