
COVID-19 Impact on Adolescent 24 h Movement Behaviors

Abstract
:1. Introduction
2. Materials and Methods
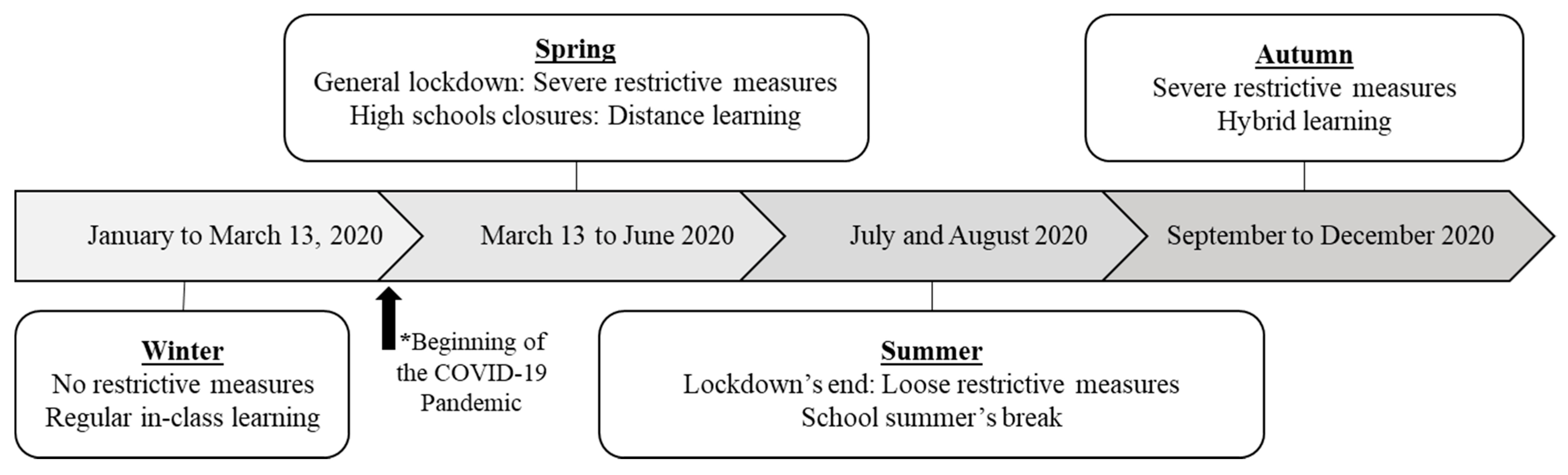
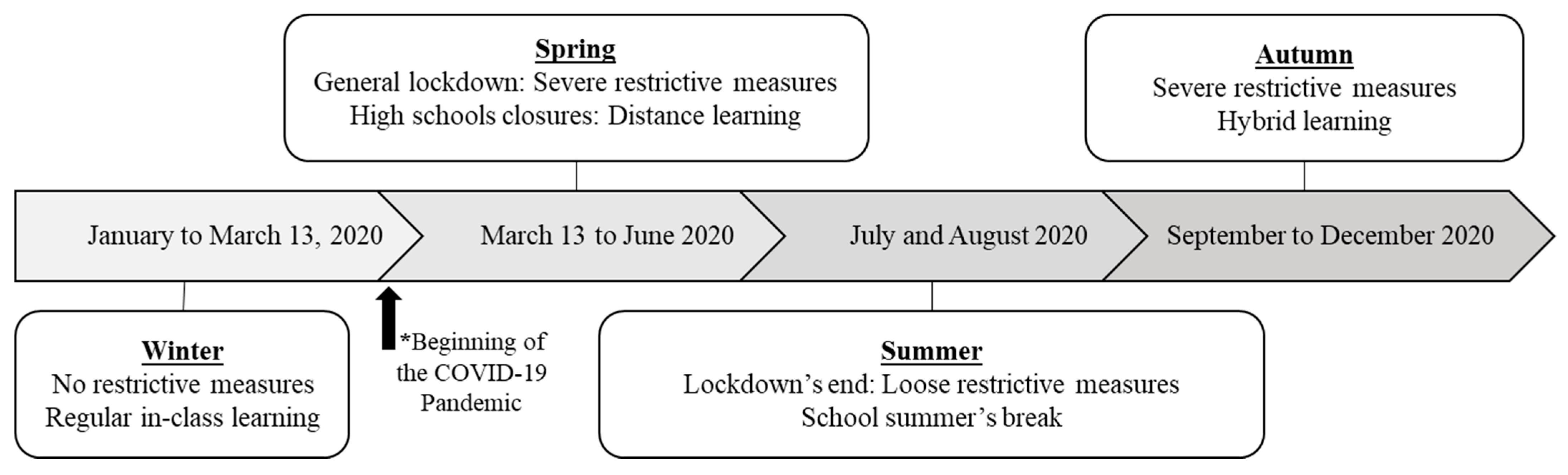
2.1. Overview
2.2. Participants
2.3. Questionnaire
2.4. Statistical Analysis
3. Results
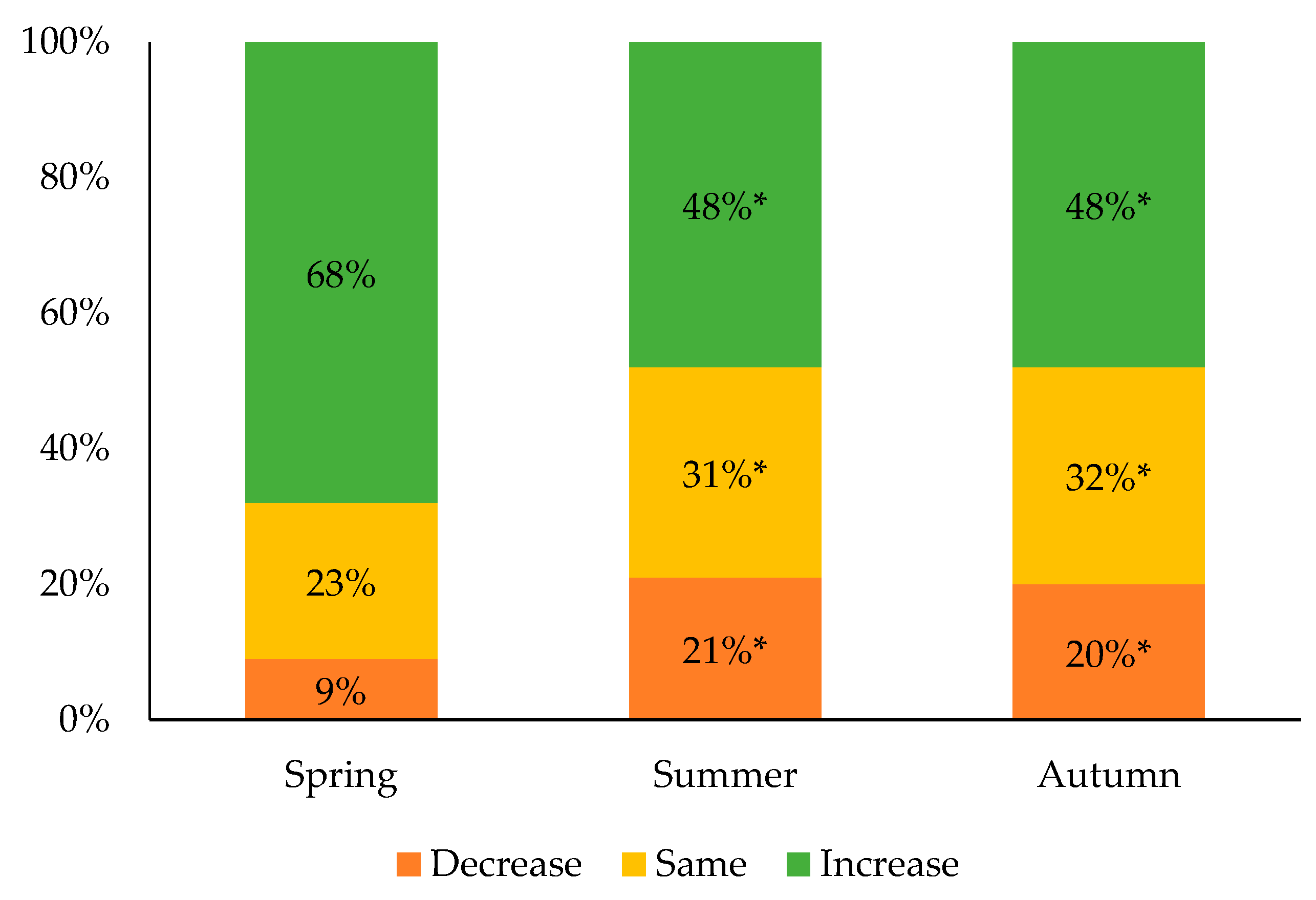
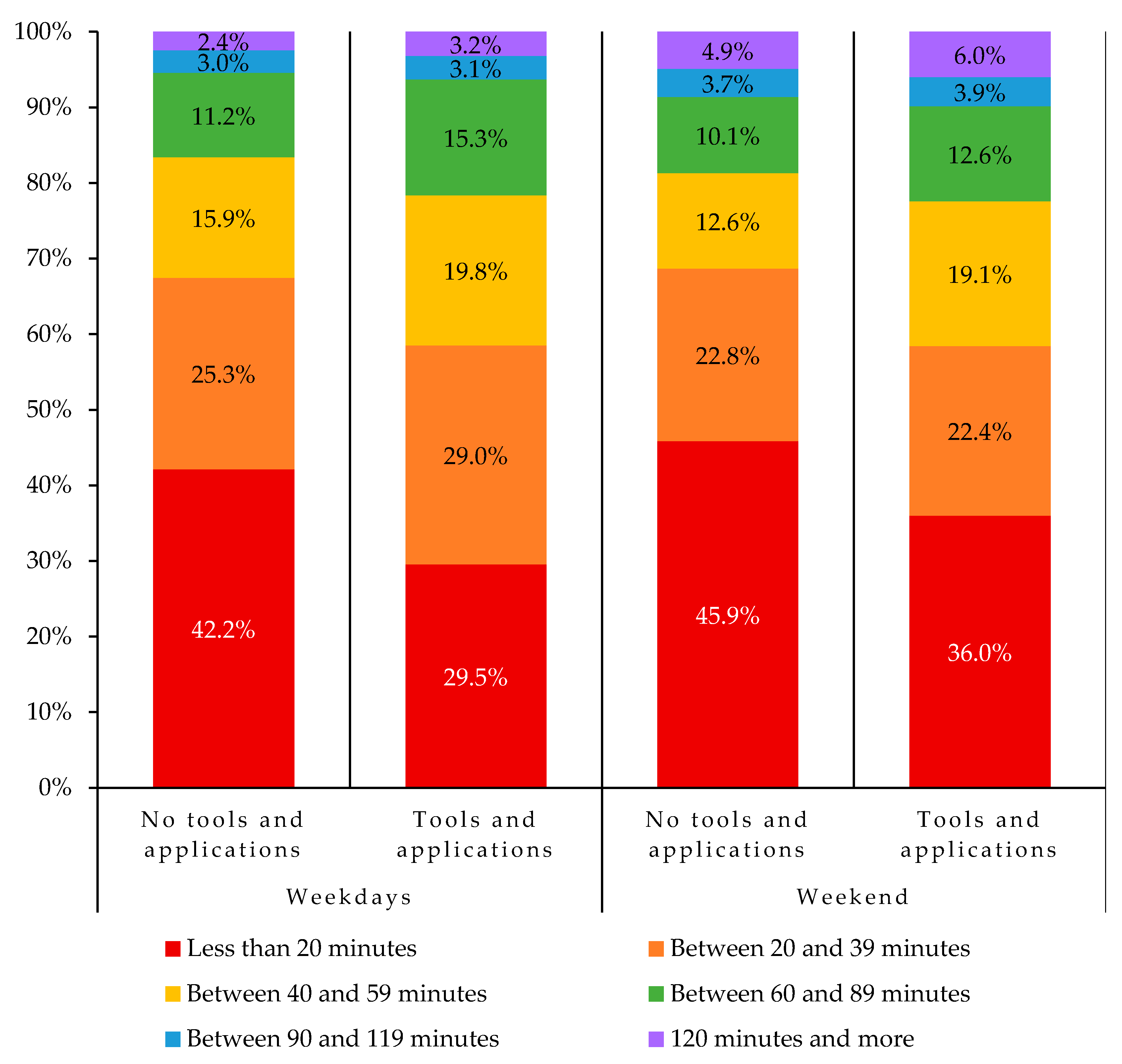
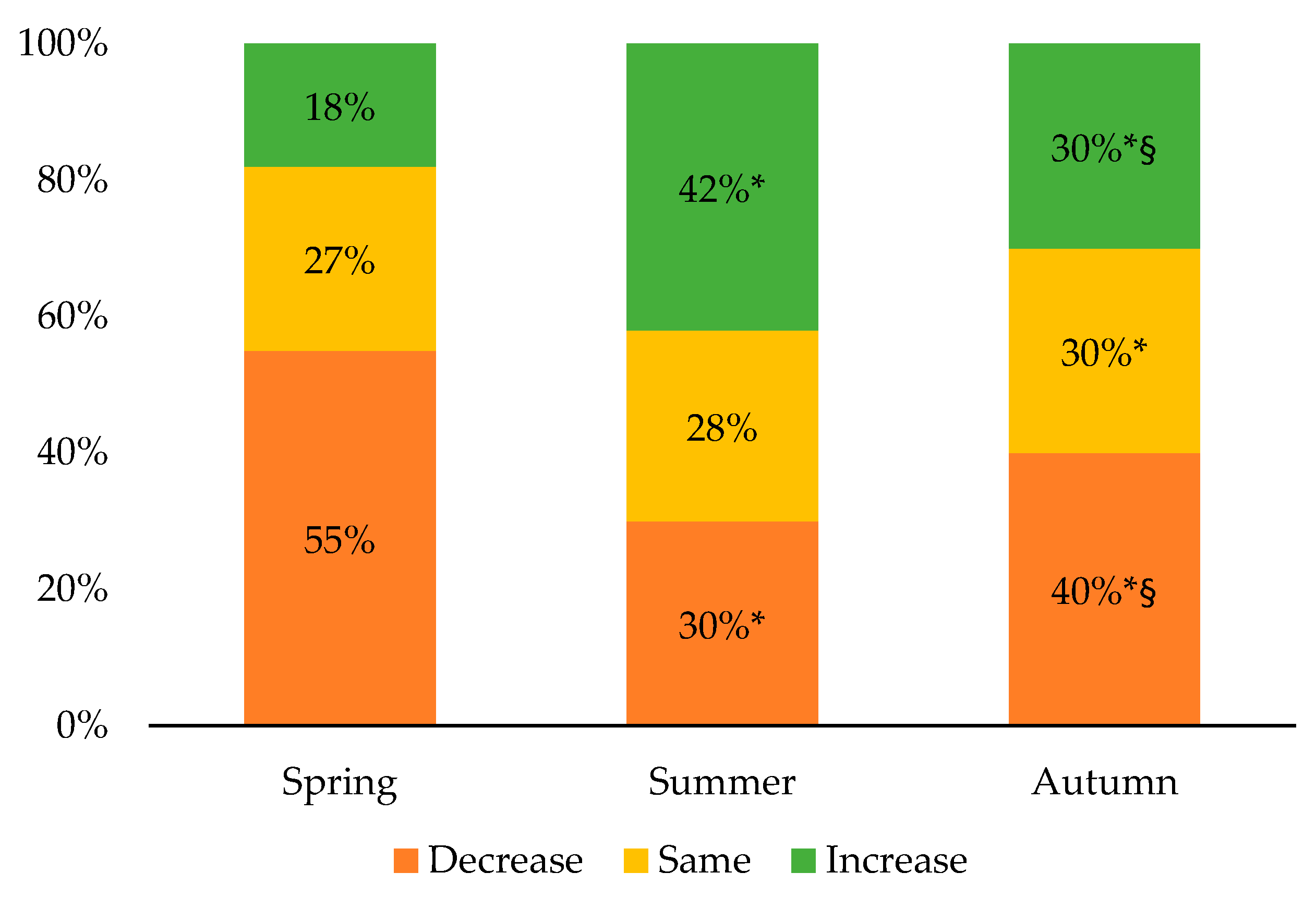
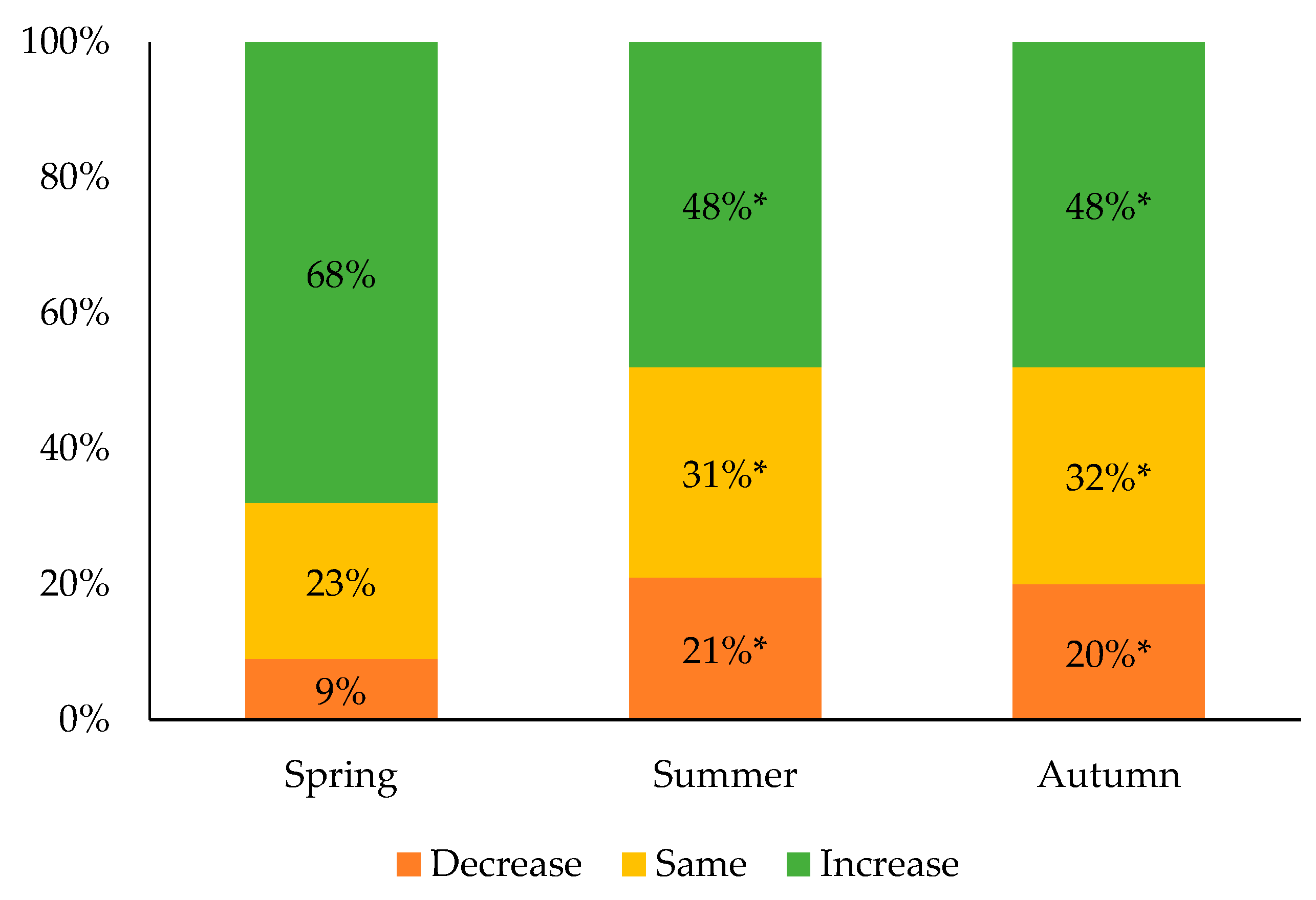
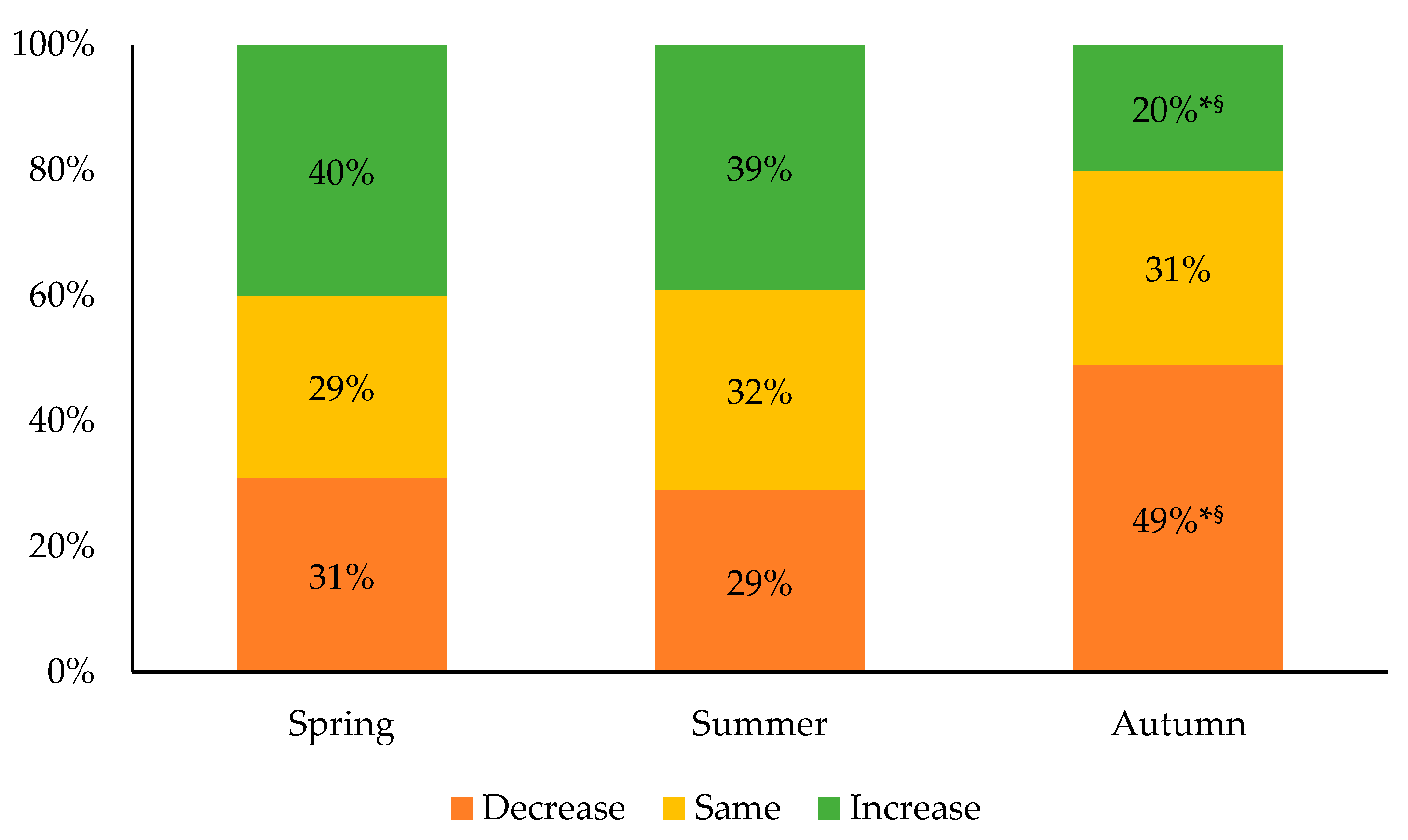
3.1. Evolution of the 24 h Movement Behaviors
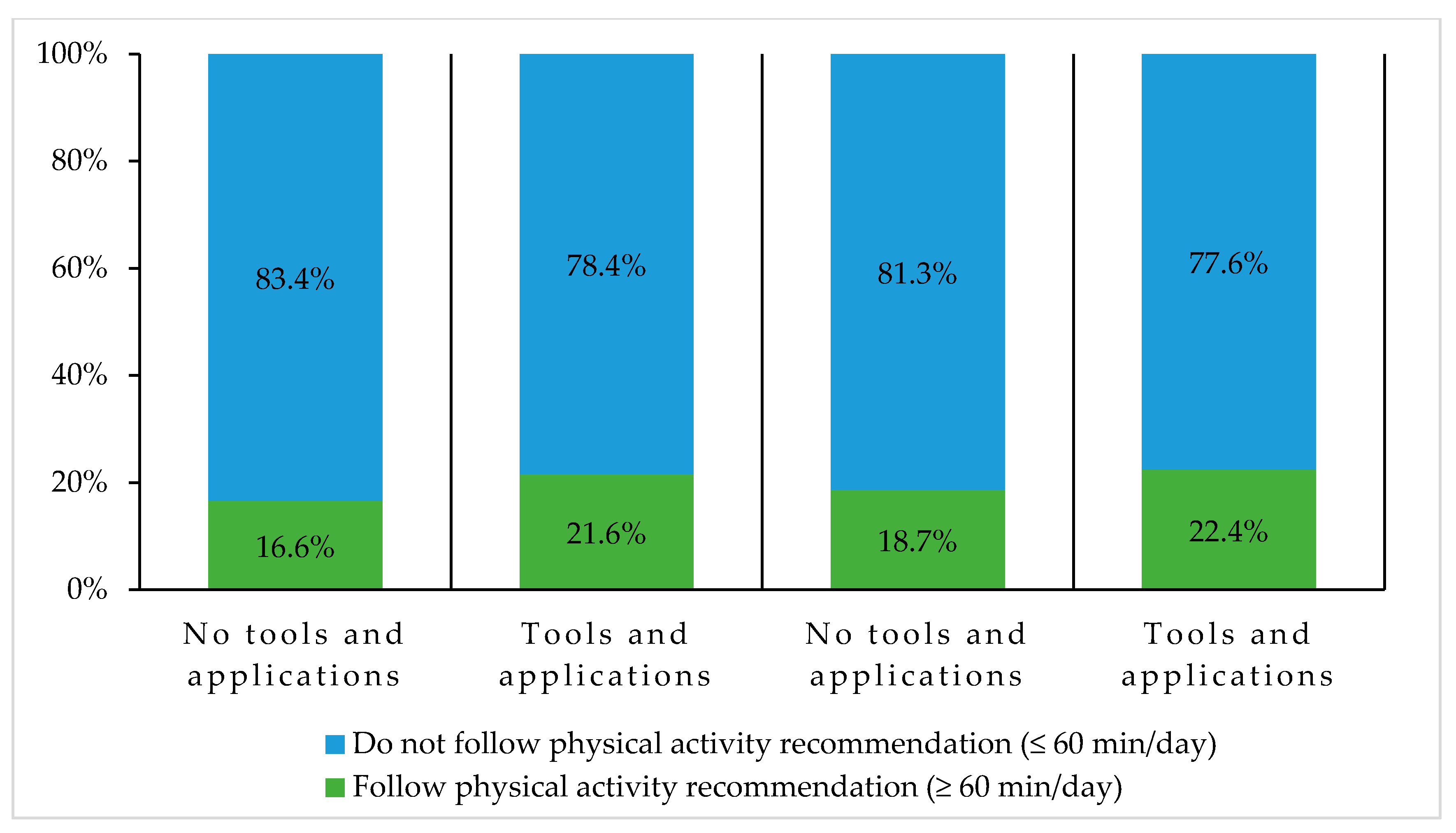
3.2. Meeting the 24 h Movement Recommendations
4. Discussion
4.1. Evolution of the 24 h Movement Behaviors
4.2. Meeting the 24 h Movement Recommendations
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tremblay, M.S.; Carson, V.; Chaput, J.P.; Connor Gorber, S.; Dinh, T.; Duggan, M.; Faulkner, G.; Gray, C.E.; Gruber, R.; Janson, K.; et al. Canadian 24-Hour Movement Guidelines for children and youth: An integration of physical activity, sedentary behaviour, and sleep. Appl. Physiol. Nutr. Metab. 2016, 41, S311–S327. [Google Scholar] [CrossRef] [PubMed]
- Carson, V.; Chaput, J.P.; Janssen, I.; Tremblay, M.S. Health Associations with meeting new 24-Hour Movement Guidelines for Canadian children and youth. Prev. Med. 2017, 95, 7–13. [Google Scholar] [CrossRef] [PubMed]
- ParticipACTION. The role of the family in the physical activity, sedentary and sleep behaviours of children and youth. In The 2020 ParticipACTION Report Card on Physical Activity for Children and Youth; ParticipACTION: Toronto, ON, Canada, 2020. [Google Scholar]
- Moore, S.A.; Faulkner, G.; Rhodes, R.E.; Brussoni, M.; Chulak-Bozzer, T.; Ferguson, L.J.; Mitra, R.; O’Reilly, N.; Spence, J.C.; Vanderloo, L.M.; et al. Impact of the COVID-19 Virus outbreak on movement and play behaviours of Canadian children and youth: A national survey. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 85. [Google Scholar] [CrossRef] [PubMed]
- Parker, K.; Uddin, R.; Ridgers, N.D.; Brown, H.; Veitch, J.; Salmon, J.; Timperio, A.; Sahlqvist, S.; Cassar, S.; Toffoletti, K.; et al. The use of digital platforms for adults’ and adolescents’ physical activity during the COVID-19 pandemic (Our Life at Home): Survey study. J. Med. Internet Res. 2021, 23, e23389. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Koenigstorfer, J. Determinants of physical activity maintenance during the COVID-19 Pandemic: A focus on fitness apps. Transl. Behav. Med. 2020, 10, 835–842. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J.; Reynolds, C.F., III; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Bates, L.C.; Zieff, G.; Stanford, K.; Moore, J.B.; Kerr, Z.Y.; Hanson, E.D.; Barone Gibbs, B.; Kline, C.E.; Stoner, L. COVID-19 Impact on behaviors across the 24-hour day in children and adolescents: Physical activity, sedentary behavior, and sleep. Children 2020, 7, 138. [Google Scholar] [CrossRef] [PubMed]
- Munasinghe, S.; Sperandei, S.; Freebairn, L.; Conroy, E.; Jani, H.; Marjanovic, S.; Page, A. The impact of physical distancing policies during the COVID-19 pandemic on health and well-being among Australian adolescents. J. Adolesc. Health 2020, 67, 653–661. [Google Scholar] [CrossRef] [PubMed]
- Dutta, K.; Mukherjee, R.; Sen, D.; Sahu, S. Effect of COVID-19 lockdown on sleep behavior and screen exposure time: An observational study among Indian school children. Biol. Rhythm Res. 2020, 1–12. [Google Scholar] [CrossRef]
- Pietrobelli, A.; Pecoraro, L.; Ferruzzi, A.; Heo, M.; Faith, M.; Zoller, T.; Antoniazzi, F.; Piacentini, G.; Fearnbach, S.N.; Heymsfield, S.B. Effects of COVID-19 lockdown on lifestyle behaviors in children with obesity living in Verona, Italy: A longitudinal study. Obesity 2020, 28, 1382–1385. [Google Scholar] [CrossRef] [PubMed]
- Chastin, S.F.M.; Palarea-Albaladejo, J.; Dontje, M.L.; Skelton, D.A. Combined effects of time spent in physical activity, sedentary behaviors and sleep on obesity and cardio-metabolic health markers: A novel compositional data analysis approach. PLoS ONE 2015, 10, e0139984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guan, H.; Okely, A.D.; Aguilar-Farias, N.; del Pozo Cruz, B.; Draper, C.E.; El Hamdouchi, A.; Florindo, A.A.; Jáuregui, A.; Katzmarzyk, P.T.; Kontsevaya, A. Promoting healthy movement behaviours among children during the COVID-19 pandemic. Lancet Child Adolesc. Health 2020, 4, 416–418. [Google Scholar] [CrossRef]
- Mandelkorn, U.; Genzer, S.; Choshen-Hillel, S.; Reiter, J.; Cruz, M.M.e.; Hochner, H.; Kheirandish-Gozal, L.; Gozal, D.; Gileles-Hillel, A. Escalation of sleep disturbances amid the COVID-19 pandemic: A cross-sectional international study. J. Clin. Sleep Med. 2021, 17, 45–53. [Google Scholar] [CrossRef]
- Brazendale, K.; Beets, M.W.; Weaver, R.G.; Russell, R.P.; Turner-McGrievy, G.M.; Kaczynski, A.T.; Chandler, J.L.; Bohnert, A.; von Hippel, P.T. Understanding differences between summer vs. school obesogenic behaviors of children: The Structured Days Hypothesis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 100. [Google Scholar] [CrossRef] [PubMed]
- Pinto, A.J.; Dunstan, D.W.; Owen, N.; Bonfá, E.; Gualano, B. Combating physical inactivity during the COVID-19 pandemic. Nat. Rev. Rheumatol. 2020, 16, 347–348. [Google Scholar] [CrossRef] [PubMed]
- Mitra, R.; Moore, S.A.; Gillespie, M.; Faulkner, G.; Vanderloo, L.M.; Chulak-Bozzer, T.; Rhodes, R.E.; Brussoni, M.; Tremblay, M.S. Healthy movement behaviours in children and youth during the COVID-19 pandemic: Exploring the role of the neighbourhood environment. Health Place 2020, 65, 102418. [Google Scholar] [CrossRef] [PubMed]
- Leyton-Román, M.; Núñez, J.L.; Jiménez-Castuera, R. The importance of supporting student autonomy in physical education classes to improve intention to be physically active. Sustainability 2020, 12, 4251. [Google Scholar] [CrossRef]
- Leyton-Román, M.; de la Vega, R.; Jiménez-Castuera, R. Motivation and commitment to sports practice during the lockdown caused by COVID-19. Front. Psychol. 2021, 11, 3846. [Google Scholar] [CrossRef] [PubMed]
- Van de Mortel, T.F. Faking It: Social desirability response bias in self-report research. Aust. J. Adv. Nurs. 2008, 25, 40. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 24 h Movement Behavior Recommendations | Weekdays | Weekend | ||||||
|---|---|---|---|---|---|---|---|---|
| All Students n = 2661 | Girls n = 1417 | Boys n = 1154 | Gender-Diverse n = 33 | All Students n = 2661 | Girls n = 1417 | Boys n = 1154 | Gender-Diverse n = 33 | |
| Specific recommendations | ||||||||
| Physical activity (≥60 min/day) | 18.3 [16.8–19.8] | 15.8 [13.9–17.7] | 21.2 [18.8–23.6] | 28.1 § [12.5–43.7] | 20.1 [18.6–21.6] | 15.2 [13.3–17.1] | 25.9 [23.3–28.5] | 34.4 § [17.9–50.9] |
| Recreational screen time (≤2 h/day) | 27.4 [25.6–29.2] | 25.0 [22.7–27.3] | 31.0 [28.2–33.8] | 13.3 § [11.5–25.5] | 14.0 [12.6–15.4] | 13.2 [11.4–15.0] | 15.0 [12.8–17.2] | 6.7 [0.0–15.6] |
| Sleep duration (8 to 11 h/night *) | 18.4 [16.9–19.9] | 15.2 [13.3–17.1] | 23.4 [20.8–26.0] | 6.5 § [0.0–15.2] | 39.4 [37.5–41.3] | 38.1 [35.5–40.7] | 42.2 [39.2–45.2] | 29.0 § [13.0–45.0] |
| Combination of recommendations | ||||||||
| Physical activity and recreational screen time | 5.0 [4.2–5.8] | 3.8 [2.8–4.8] | 6.5 [5.1–7.9] | 6.1 § [0.0–14.5] | 3.0 [2.3–3.7] | 1.7 [1.0–2.4] | 4.5 [3.3–5.7] | 3.0 § [0.0–8.8] |
| Physical activity and sleep duration | 3.4 [2.7–4.1] | 1.8 [1.1–2.5] | 5.3 [4.0–6.6] | 3.0 § [0.0–8.8] | 7.8 [6.8–8.8] | 5.9 [4.7–7.1] | 10.5 [8.7–12.3] | 6.1 § [0.0–14.3] |
| Recreational screen time and sleep duration | 6.1 [5.2–7.0] | 4.8 [3.7–5.9] | 8.2 [6.5–9.9] | 0.0 § [0.0–2.9] | 5.1 [4.2–6.0] | 4.4 [3.3–5.5] | 6.3 [4.8–7.8] | 0.0 § [0.0–2.9] |
| All three recommendations | 1.1 [0.7–1.5] | 0.5 [0.1–0.9] | 1.9 [1.1–2.7] | 0.0 § [0.0–2.9] | 1.4 [1.0–1.8] | 0.6 [0.2–1.0] | 2.5 § [1.6–3.4] | 0.0 § [0.0–2.9] |
| None of the recommendations | 50.0 [48.0–52.0] | 54.0 [51.2–56.8] | 44.0 [40.9–47.1] | 57.1 § [38.8–75.4] | 41.7 [39.7–43.7] | 45.0 [42.2–47.8] | 37.1 [34.1–40.1] | 35.7 § [18.0–53.4] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dubuc, M.-M.; Berrigan, F.; Goudreault, M.; Beaudoin, S.; Turcotte, S. COVID-19 Impact on Adolescent 24 h Movement Behaviors. Int. J. Environ. Res. Public Health 2021, 18, 9256. https://doi.org/10.3390/ijerph18179256
Dubuc M-M, Berrigan F, Goudreault M, Beaudoin S, Turcotte S. COVID-19 Impact on Adolescent 24 h Movement Behaviors. International Journal of Environmental Research and Public Health. 2021; 18(17):9256. https://doi.org/10.3390/ijerph18179256
Chicago/Turabian StyleDubuc, Marie-Maude, Félix Berrigan, Marylène Goudreault, Sylvie Beaudoin, and Sylvain Turcotte. 2021. "COVID-19 Impact on Adolescent 24 h Movement Behaviors" International Journal of Environmental Research and Public Health 18, no. 17: 9256. https://doi.org/10.3390/ijerph18179256
APA StyleDubuc, M.-M., Berrigan, F., Goudreault, M., Beaudoin, S., & Turcotte, S. (2021). COVID-19 Impact on Adolescent 24 h Movement Behaviors. International Journal of Environmental Research and Public Health, 18(17), 9256. https://doi.org/10.3390/ijerph18179256