
Psychosocial Working Conditions and Social Participation. A 10-Year Follow-Up of Senior Workers

 , ,
, ,  and
and
Abstract
1. Introduction
- to investigate whether psychosocial demands and their combinations predict social participation among 55-year or older working people in a 10-year follow-up when they were not working.
- to investigate if high decision latitude was associated with social participation at baseline and predicted high social participation at follow-up.
2. Material and Methods
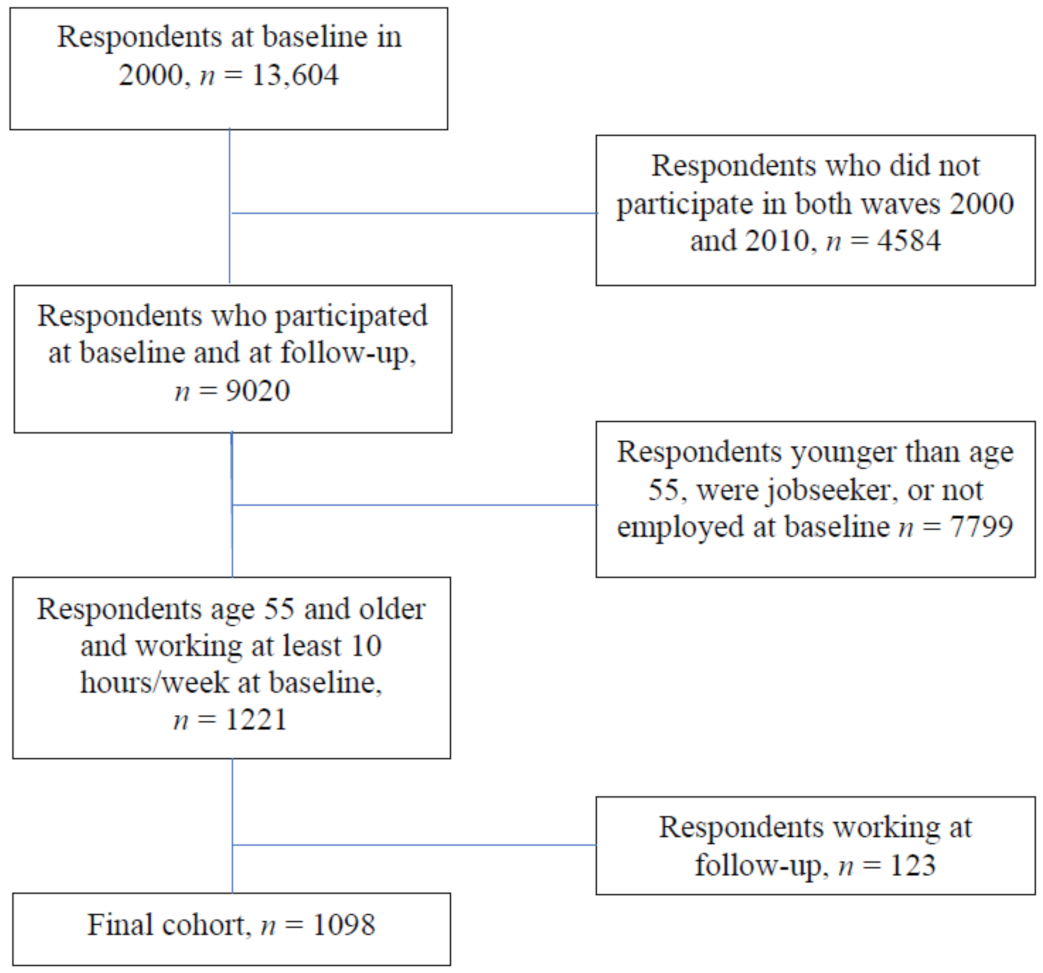
2.1. Sample and Settings
2.2. Outcome Variables
2.3. Exposure Variable
2.4. Other Baseline Characteristics
2.5. Statistical Analysis
2.6. Ethics
3. Results
3.1. Descriptive Results
3.2. Variations in Social Participation between Different Job Type
3.3. Associations between Potential Confounders and High Social Participation
4. Discussion
4.1. Main Findings
4.2. Methodological Considerations
4.3. Possible Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zaninotto, P.; Steptoe, A. Association Between Subjective Well-being and Living Longer Without Disability or Illness. JAMA Netw. Open 2019, 2, e196870. [Google Scholar] [CrossRef]
- WHO. Decade of Healthy Ageing: Baseline Report. Geneva. Available online: https://www.who.int/publications/i/item/9789240023307 (accessed on 26 August 2021).
- WHO. World Report on Ageing and Health. Geneva. Available online: https://www.who.int/publications/i/item/9789241565042 (accessed on 26 August 2021).
- Hovbrandt, P.; Fridlund, B.; Carlsson, G. Very old people’s experience of occupational performance outside the home: Possibilities and limitations. Scand. J. Occup. Ther. 2007, 14, 77–89. [Google Scholar] [CrossRef] [PubMed]
- Levasseur, M.; Richard, L.; Gauvin, L.; Raymond, E. Inventory and analysis of definitions of social participation found in the aging literature: Proposed taxonomy of social activities. Soc. Sci. Med. 2010, 71, 2141–2149. [Google Scholar] [CrossRef] [PubMed]
- Gibson, H.J.; Singleton, J.F. Leisure and Aging: Theory and Practice; Human Kinetics: Champaign, IL, USA, 2012. [Google Scholar]
- Huxhold, O.; Miche, M.; Schüz, B. Benefits of having friends in older ages: Differential effects of informal social activities on well-being in middle-aged and older adults. J. Gerontol. Ser. B-Psychol. Sci. 2014, 69, 366–375. [Google Scholar] [CrossRef] [PubMed]
- Klugar, M.; Cáp, J.; Klugaróva, J.; Marecová, J.; Roberson, D.; Kelnarova, Z. The personal active ageing strategies of older adults in Europe: A systematic review of qualitative evidence. JBI Database Syst. Rev. Implement. Rep. 2016, 14, 193–257. [Google Scholar] [CrossRef]
- Bourassa, K.J.; Memel, M.; Woolverton, C.; Sbarra, D.A. Social participation predicts cognitive functioning in aging adults over time: Comparisons with physical health, depression, and physical activity. Aging Ment. Health 2017, 21, 133–146. [Google Scholar] [CrossRef]
- He, Q.; Cui, Y.; Liang, L.; Zhong, Q.; Li, J.; Li, Y.; Lv, X.; Huang, F. Social participation, willingness and quality of life: A population-based study among older adults in rural areas of China. Geriatrics Gerontol. Int. 2017, 17, 1593–1602. [Google Scholar] [CrossRef]
- Hughes, T.F.; Flatt, J.D.; Fu, B.; Chang, C.C.; Ganguli, M. Engagment in social activities and progression from mild to severe cognitive impairment: The MYHAT study. Int. Psychogeriatr. 2013, 25, 587–595. [Google Scholar] [CrossRef]
- Li, C.; Jiang, S.; Li, N.; Zhang, Q. Influence of social participation on life satisfaction and depression among Chinese elderly: Social support as a mediator. J. Community Psychol. 2018, 46, 345–355. [Google Scholar] [CrossRef]
- Paillard-Borg, S.; Fratiglioni, L.; Xu, W.; Winblad, B.; Wang, H.-X. An Active Lifestyle Postpones Dementia Onset by More than One Year in Very Old Adults. J. Alzheimer’s Dis. 2012, 31, 835–842. [Google Scholar] [CrossRef]
- Santini, Z.I.; Jose, P.E.; Koyanagi, A.; Meilstrup, C.; Nielsen, L.; Madsen, K.R.; Koushede, V. Formal social participation protects physical health through enhanced mental health: A longitudinal mediation analysis using three consecutive waves of the Survey of Health, Ageing and Retirement in Europe (SHARE). Soc. Sci. Med. 2020, 251, 112906. [Google Scholar] [CrossRef]
- Atchley, R.C. A Continuity Theory of Normal Aging. Gerontologist 1989, 29, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Agahi, N.; Ahacic, K.; Parker, M.G. Continuity of leisure participation from middle age to old age. J. Gerontol. Ser. B 2006, 61, S340–S346. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, K. Why work beyond 65? Discourse on the Decision to Continue Working or Retire Early. Nord. J. Work. Life Stud. 2012, 2, 7–28. [Google Scholar] [CrossRef]
- Nilsson, K. The ability and desire to extend working life. In Healthy Workplaces for Men and Women in All Ages Knowledge Compilation; V.E. Swedish Work Environment Authority: Stockholm, Sweden, 2016; pp. 36–59. [Google Scholar]
- Christiansen, C.; Townsend, E. The occupational nature of social groups. In Introduction to Occupation: The Art and Science of Living, International Edition, 2nd ed.; Christiansen, C., Townsend, E., Eds.; Pearson Education, Inc.: Upper Saddle River, NJ, USA, 2010; pp. 175–210. [Google Scholar]
- Hovbrandt, P.; Carlsson, G.; Nilsson, K.; Albin, M.; Håkansson, C. Occupational balance as described by older workers over the age of 65. J. Occup. Sci. 2018, 26, 40–52. [Google Scholar] [CrossRef]
- Nilsson, I.; Löfgren, B.; Fisher, A.G.; Bernspång, B. Focus on Leisure Repertoire in the Oldest Old: The Umeå 85+ Study. J. Appl. Gerontol. 2006, 25, 391–405. [Google Scholar] [CrossRef]
- Karasek, R.; Theorell, T. Healthy Work: Stress, Productivity, and the Reconstruction of Working Life; Basic Books: New York, NY, USA, 1990. [Google Scholar]
- Kivimäki, M.; Jokela, M.; Nyberg, S.T.; Singh-Manoux, A.; Fransson, E.; Alfredsson, L.; Bjorner, J.B.; Borritz, M.; Burr, H.; Casini, A.; et al. Long working hours and risk of coronary heart disease and stroke: A systematic review and meta-analysis of published and unpublished data for 603,838 individuals. Lancet 2015, 386, 1739–1746. [Google Scholar] [CrossRef]
- Kraatz, S.; Lang, J.; Kraus, T.; Münster, E.; Ochsmann, E. The incremental effect of psychosocial workplace factors on the development of neck and shoulder disorders: A systematic review of longitudinal studies. Int. Arch. Occup. Envir. Health 2013, 86, 375–395. [Google Scholar] [CrossRef] [PubMed]
- Madsen, I.E.; Nyberg, S.T.; Hanson, L.M.; Ferrie, J.E.; Ahola, K.; Alfredsson, L.; Batty, G.D.; Bjorner, B.; Borritz, M.; Burr, H.; et al. Job strain as a risk factor for clinical depression: Systematic review and meta-analysis with additional individual participant data. Psychol. Med. 2017, 47, 1342–1356. [Google Scholar] [CrossRef] [PubMed]
- Falk, A.; Hanson, B.S.; Isacsson, S.-O.; Ostergren, P.-O. Job strain and mortality in elderly men: Social network, support, and influence as buffers. Amer. J. Public Health 1992, 82, 1136–1139. [Google Scholar] [CrossRef]
- Lindström, M. Psychosocial work conditions, social participation and social capital: A causal pathway investigated in a longitunal study. Soc. Sci. Med. 2006, 62, 280–291. [Google Scholar] [CrossRef]
- Nilsen, C.; Agahi, N.; Kåreholt, I. Work stressors in late midlife and physical functioning in old age. J. Aging Health 2017, 29, 893–911. [Google Scholar] [CrossRef] [PubMed]
- James, B.; Wilson, R.; Barnes, L.; Bennet, D. Late-life social activity and cognitive decline in old age. J. Int. Neuropsychol. Soc. 2011, 17, 998–1005. [Google Scholar] [CrossRef] [PubMed]
- Carlsson, F.; Merlo, J.; Lindström, M.; Östergren, P.-O.; Lithman, T. Representativity of a postal public health questionnaire survey in Sweden, with special reference to ethnic differences in participation. Scand. J. Public Health 2006, 34, 132–139. [Google Scholar] [CrossRef]
- Lindström, M.; Merlo, J.; Ostergren, P.-O. Individual and neighbourhood determinants of social participation and social capital: A multilevel analysis of the city of Malmö, Sweden. Soc. Sci. Med. 2002, 54, 1779–1791. [Google Scholar] [CrossRef]
- Hanson, B.S.; Östergren, P.-O.; Elmståhl, S.; Isacsson, S.-O.; Ranstam, J. Reliability and validity assessments of measures of social networks, social support and control—Results from the Malmö Shoulder and Neck Study. Scand. J. Soc. Med. 1997, 25, 249–257. [Google Scholar] [CrossRef]
- Karasek, R.; Brisson, C.; Kawakami, N.; Houtman, I.; Bongers, P.; Amick, B. The Job Content Questionnaire (JCQ): An instrument for internationally comparative assessments of psychosocial job characteristics. J. Occup Health Psychol. 1998, 3, 322. [Google Scholar] [CrossRef]
- Karasek, R. Job demands, job decision latitude, and mental strain: Implication for job redesign. Admin. Sci. Quart. 1979, 24, 285–308. [Google Scholar] [CrossRef]
- Kaplan, G.A.; Camacho, T. Perceived health and mortality: A nine-year follow-up of the human population laboratory cohort. Amer. J. Epidemiol. 1983, 117, 292–304. [Google Scholar] [CrossRef]
- Schnittker, J.; Baćak, V. The Increasing Predictive Validity of Self-Rated Health. PLoS ONE 2014, 9, e84933. [Google Scholar] [CrossRef]
- Ware, J.E.; Kosinski, M.; Keller, S.D. A 12-Item Short-Form Health Survey: Construction of Scales and Preliminary Tests of Reliability and Validity. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef] [PubMed]
- Björner, J.; Sondergaard, K.T.; Orth-Gomér, K.; Tibblin, G.; Sullivan, M.; Westerholm, P. Self-Rated Health: A Useful Concept in Research, Prevention and Clinical Medicine; Swedish Council for Planning and Coordonation of Research: Stockholm, Sweden, 1996. [Google Scholar]
- Rothman, J. Modern Epidemiology; Little, Brown and Company: Boston, MD, USA, 1986. [Google Scholar]
- Marmot, M. Social determinants of health inequalities. Lancet 2005, 365, 1099–1104. [Google Scholar] [CrossRef]
- Fransson, E.I.; Heikkilä, K.; Nyberg, S.T.; Zins, M.; Westerlund, H.; Westerholm, P.; Väänänen, A.; Virtanen, M.; Vahtera, J.; Theorell, T.; et al. Job strain as a risk factor for leisure-time physical inactivity: An individual-participant meta-analysis of up to 170,000 men and women: The IPD-Work Consortium. Amer. J. Epidemiol. 2012, 176, 1078–1089. [Google Scholar] [CrossRef]
- Heikkilä, K.; Fransson, E.I.; Nyberg, S.T.; Zins, M.; Westerlund, H.; Westerholm, P.; Virtanen, M.; Vahtera, J.; Suominen, S.; Steptoe, A.; et al. Job strain and health-related lifestyle: Findings from an individual-participant meta-analysis of 118,000 working adults. Amer. J. Public Health 2013, 103, 2090–2097. [Google Scholar] [CrossRef]
- Breheny, M.; Griffiths, Z. “I had a good time when I was young”: Interpreting descriptions of continuity among older people. J. Aging Stud. 2017, 41, 36–43. [Google Scholar] [CrossRef]
- Utz, R.L.; Carr, D.; Nesse, R.; Wortman, C.B. The effect of widowhood on older adults’ social participation: An evaluation of activity, disengagement, and continuity theories. Gerontologist 2002, 42, 522–533. [Google Scholar] [CrossRef]
- Kulmala, J.; von Bonsdorff, M.B.; Stenholm, S.; Törmäkangas, T.; von Bonsdorff, M.E.; Nygård, C.H.; Klockars, M.; Seitsamo, J.; Ilmarinen, J.; Rantanen, R. Perceived stress symptoms in midlife predict disability in old age: A 28-year prospective cohort study. J. Gerontol. Ser. A 2013, 68, 984–991. [Google Scholar] [CrossRef]
- Kulmala, J.; Hinrichs, T.; Törmäkangas, T.; von Bonsdorff, M.; von Bonsdorff, M.; Nygård, C.-H.; Klockars, M.; Seitsamo, J.; Ilmarinen, J.; Rantanen, T. Work-related stress in midlife is associated with higher number of mobility limitation in older age—Results from the FLAME study. AGE 2014, 36, 9722. [Google Scholar] [CrossRef][Green Version]
- Nilsen, C.; Andel, R.; Fors, S.; Meinow, B.; Mattsson, A.D.; Kåreholt, I. Associations between work-related stress in late midlife, educational attainment, and serious health problems in old age: A longitudinal study with over 20 years of follow-up. BMC Public Health 2014, 14, 1–12. [Google Scholar] [CrossRef]
- Parker, V.; Andel, R.; Nilsen, C.; Kåreholt, I. The association between mid-life socioeconomic position and health after retirement—Exploring the role of working conditions. J. Aging Health 2013, 25, 863–881. [Google Scholar] [CrossRef]
- Sindi, S.; Hagman, G.; Håkansson, K.; Kulmala, J.; Nilsen, C.; Kåreholt, I.; Soininen, H.; Solomon, A.; Kivipelto, M. Midlife Work-Related Stress Increases Dementia Risk in Later Life: The CAIDE 30-Year Study. J. Gerontol. Ser. B 2016, 72, 1044–1053. [Google Scholar] [CrossRef] [PubMed]
- Howrey, B.T.; Hand, C. Measuring social participation in the and retirement study. Gerontologist 2019, 59, e415–e423. [Google Scholar] [CrossRef]
- Wilcock, A.; Hocking, C. An Occupational Perspective of Health, 3rd ed.; Slack Incorporated: Thorofare, NJ, USA, 2015. [Google Scholar]
- Sirven, N.; Debrand, T. Social participation and healthy ageing: An international comparison using SHARE data. Soc. Sci. Med. 2008, 67, 2017–2026. [Google Scholar] [CrossRef] [PubMed]
- Sirven, N.; Debrand, T. Social Participation of Elderly People in Europe. Retraite Soc. 2013, 2, 59–80. [Google Scholar] [CrossRef]
- European Union Information Agency for Occupational Safety and Health; European Centre for the Development of Vocational Trainong; European Foundation for the Improvement of Living and Working Conditions; European Institute for Gender Equality; Dubois, H.; Jungblut, J.-M.; Wilkens, M.; Vermeylen, G.; Vargas Llave, O. Towards Age-Friendly Work in Europe: A Life Course Perspective on Work and Ageing from EU Agencies; Publications Office of the European Union: Luxembourg, 2017. [Google Scholar]
- Nilsson, K. Interventions to reduce injuries among older workers in agriculture: A review of evaluated intervention projects. Work. 2016, 55, 471–480. [Google Scholar] [CrossRef]
- Nilsson, K. The influence of work environment and motivation factors on seniors’ attitudes to an extended working life or retire. A cross sectional study with employees 55–74 years of age. Open J. Soc. Sci. 2017, 5, 30. [Google Scholar]
- Anxo, D.; Ericson, T.; Herbert, A.; Rönnmar, M. To Stay or not to Stay. That is the Question: Beyond Retirement: Stayers on the Labour Market; Linnaeus University: Växjö, Sweden, 2017. [Google Scholar]
- Prakash, K.; Neupane, S.; Leino-Arjas, P.; von Bonsdorff, M.B.; Rantanen, T.; von Bonsdorff, M.E.; Seitsamo, J.; Ilmarinen, J.; Nygard, C.-H. Work-related biomechanical exposure and job strain as separate and joint predictors of musculoskeletal diseases: A 28-year prospective follow-up study. Amer. J. Epidemiol. 2017, 186, 1256–1267. [Google Scholar] [CrossRef]
- von Bonsdorff, M.E.; Rantanen, T.; Törmäkangas, T.; Kulmala, J.; Hinrichs, T.; Seitsamo, J.; Nygard, C.-H.; Ilmarinen, J.; von Bonsdorff, M.B. Midlife work ability and mobility limitation in old age among non-disability and disability retirees—A prospective study. BMC Public Health 2016, 16, 1–8. [Google Scholar] [CrossRef]
- Oakman, J.; Neupane, S.; Prakash, K.; Nygård, C.H. What are the key workplace influences on pathways of workability? A six-year follow up. Int. J. Environ. Res. Public Health 2019, 16, 2363. [Google Scholar] [CrossRef]
- Carr, E.; Hagger-Johnson, G.; Head, J.; Shelton, N.; Stafford, M.; Stansfeld, S.; Zaninotti, P. Working conditions as predictors of retirement intentions and exit from paid employment: A 10-year follow-up of the English Longitudinal Study of Ageing. Eur. J. Ageing 2016, 13, 39–48. [Google Scholar] [CrossRef]
- Hofacker, D.; Naumann, E. The emerging trend of work beyond retirement age in Germany. Z. Gerontol. Geriatr. 2015, 48, 473–479. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, K.; Hydbom, A.R.; Rylander, L. How are self-rated health and diagnosed disease related to early or deferred retirement? A cross-sectional study of employees aged 55–64. BMC Public Health 2016, 16, 886. [Google Scholar] [CrossRef] [PubMed]
- Sousa-Ribeiro, M.; Bernhard-Oettel, C.; Sverke, M.; Westerlund, H. Health and age-related workplace factors as predictors of preffered, ecpected, and actual retirement timing: Findings from a Swedish cohort study. Int. J. Environ. Res. Public Health 2021, 18, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, K. A sustainable working life for all ages—The swAge-model. Appl. Ergon. 2020, 86, 103082. [Google Scholar] [CrossRef]
- Nilsson, K. Conceptualisation of ageing in relation to factors of importance for extending working life —A review. Scand. J. Public Health 2016, 44, 490–505. [Google Scholar] [CrossRef]
- Nilsson, K.; Nilsson, E. Organisational measures and strategies for healthy and sustainable extended working life and employability—A deductive content analysis with data including employees, first line managers, trade union representatives and HR-practioners. Int. J. Environ. Res. Public Health 2021, 18, 5226. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | n of Respondents (Missing) | % |
|---|---|---|
| Sex | ||
| Men | 563 | 51 |
| Women | 535 | 49 |
| Married/cohabitating | 16 | 2 |
| Yes | 894 | 81 |
| No | 188 | 17 |
| Education | 34 | 3 |
| 12 years or less | 653 | 60 |
| 13 years or more | 411 | 37 |
| Financial stress | 11 | 1 |
| Yes | 19 | 2 |
| No | 1068 | 97 |
| Self-rated health | (11) | 1 |
| Good | 669 | 61 |
| Poor | 418 | 38 |
| Helping old or sick relative | (18) | 2 |
| Yes | 287 | 26 |
| No | 793 | 72 |
| Physical activity | (31) | 3 |
| Yes | 934 | 85 |
| No | 133 | 12 |
| Job type | (166) | 11 |
| Passive | 363 | 33 |
| Relaxed | 204 | 19 |
| Active | 227 | 20 |
| High strain | 188 | 17 |
| Passive, n = 363 (%) | p Value | Relaxed, n = 204 (%) | p Value | Active, n = 227 (%) | p Value | High Strain, n = 188 | p Value | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2000 | 2010 | 2000 | 2010 | 2000 | 2010 | 2000 | 2010 | |||||
| High | 282 (78) | 227 (62) | <0.001 | 181 (89) | 162 (79) | 0.004 | 206 (91) | 177 (78) | <0.001 | 155 (82) | 119 (63) | <0.001 |
| Low | 81 (22) | 136 (38) | 23 (11) | 42 (21) | 21(9) | 50 (22) | 33 (18) | 69 (37) | ||||
| Potential Confounders | OR (95% CI) |
|---|---|
| Female gender | 1.14 (0.88–1.48) |
| Good self-rated health | 2.11 (1.62–2.74) |
| Married/cohabiting | 1.25 (0.90–1.75) |
| Not caring for a sick relative | 1.44 (1.06–1.96) |
| High education level | 3.48 (2.56–4.73) |
| Financial stress | 0.60 (0.24–1.52) |
| Physically active | 2.40 (1.66–3.48) |
| 2000 | ||||||
|---|---|---|---|---|---|---|
| Variables | Model 1OR (95% CI) | Model 2 | Model 3 | Model 4 | Model 5 | Model 6 |
| High decision latitude | 2.29 (1.58–3.33) | 2.24 (1.53–3.27) | 2.12 (1.45–3.10) | 1.59 (1.06–2.38) | 1.58 (1.05–2.37) | |
| Physically active | 2.44 (1.55–3.86) | 2.23 (1.39–3.58) | 2.08 (1.27–3.39) | 2.08 (1.27–3.41) | ||
| Good self-rated health 1999 | 1.32 (0.90–1.94) | 1.20 (0.80–1.80) | 1.22 (0.81–1.84) | |||
| High educational level | 3.08 (1.93–4.92) | 3.01 (1.88–4.81) | ||||
| Not caring for a sick relative | 1.11 (0.72-1.70) | |||||
| 2010 | ||||||
| High decision latitude | 2.18 (1.64–2.91) | 2.13 (1.59–2.86) | 2.01 (1.49–2.70) | 1.53 (1.12–2.10) | 1.49 (1.09–2.05) | 1.37 (0.98–1.91) |
| Physically active | 2.38 (1.58–3.58) | 1.96 (1.29–2.99) | 1.79 (1.16–2.78) | 1.78 (1.15–2.77) | 1.51 (0.94–2.42) | |
| Good self-rated health 1999–2010 | 1.90 (1.41–2.55) | 1.90 (1.40–2.58) | 1.94 (1.42–2.64) | 1.92 (1.38–2.66) | ||
| High educational level | 3.01 (2.14–4.26) | 2.98 (2.11–4.21) | 2.50 (1.74–3.58) | |||
| Not caring for a sick relative | 1.43 (1.01–2.03) | 1.44 (0.99–2.08) | ||||
| High social participation at baseline | 6.29 (4.15–9.54) | |||||
| Decision Latitude and Self-Rated Health in 2000 | n | % Cases with High Social Participation | OR a | 95% CI b | SI c |
|---|---|---|---|---|---|
| Low latitude and poor health | 176 | 53 | 1 | ||
| Low latitude and good health | 369 | 68 | 1.4 | 0.9–2.1 | |
| High latitude and poor health | 90 | 64 | 1.7 | 0.9–3.3 | |
| High latitude and good health | 340 | 82 | 3.2 | 1.9–5.4 | 2.1 |
| 975 |
| Decision Latitude and Educational Level in 2000 | n | % Cases with High Social Participation | OR a | 95% CI b | SI c |
|---|---|---|---|---|---|
| Low latitude and low educational level | 386 | 56 | 1 | ||
| Low latitude and high educational level | 149 | 83 | 5.2 | 2.6–10.6 | |
| High latitude and low educational level | 195 | 71 | 2.1 | 1.3–3.3 | |
| High latitude and high educational level | 231 | 85 | 4.5 | 2.6–7.9 | 0.66 |
| 961 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hovbrandt, P.; Östergren, P.-O.; Canivet, C.; Albin, M.; Carlsson, G.; Nilsson, K.; Håkansson, C. Psychosocial Working Conditions and Social Participation. A 10-Year Follow-Up of Senior Workers. Int. J. Environ. Res. Public Health 2021, 18, 9154. https://doi.org/10.3390/ijerph18179154
Hovbrandt P, Östergren P-O, Canivet C, Albin M, Carlsson G, Nilsson K, Håkansson C. Psychosocial Working Conditions and Social Participation. A 10-Year Follow-Up of Senior Workers. International Journal of Environmental Research and Public Health. 2021; 18(17):9154. https://doi.org/10.3390/ijerph18179154
Chicago/Turabian StyleHovbrandt, Pia, Per-Olof Östergren, Catarina Canivet, Maria Albin, Gunilla Carlsson, Kerstin Nilsson, and Carita Håkansson. 2021. "Psychosocial Working Conditions and Social Participation. A 10-Year Follow-Up of Senior Workers" International Journal of Environmental Research and Public Health 18, no. 17: 9154. https://doi.org/10.3390/ijerph18179154
APA StyleHovbrandt, P., Östergren, P.-O., Canivet, C., Albin, M., Carlsson, G., Nilsson, K., & Håkansson, C. (2021). Psychosocial Working Conditions and Social Participation. A 10-Year Follow-Up of Senior Workers. International Journal of Environmental Research and Public Health, 18(17), 9154. https://doi.org/10.3390/ijerph18179154