
Patients’ Access to Their Psychiatric Notes: Current Policies and Practices in Sweden

 , , , and
, , , and
Abstract
:1. Introduction
Sharing Psychiatric Notes in Sweden
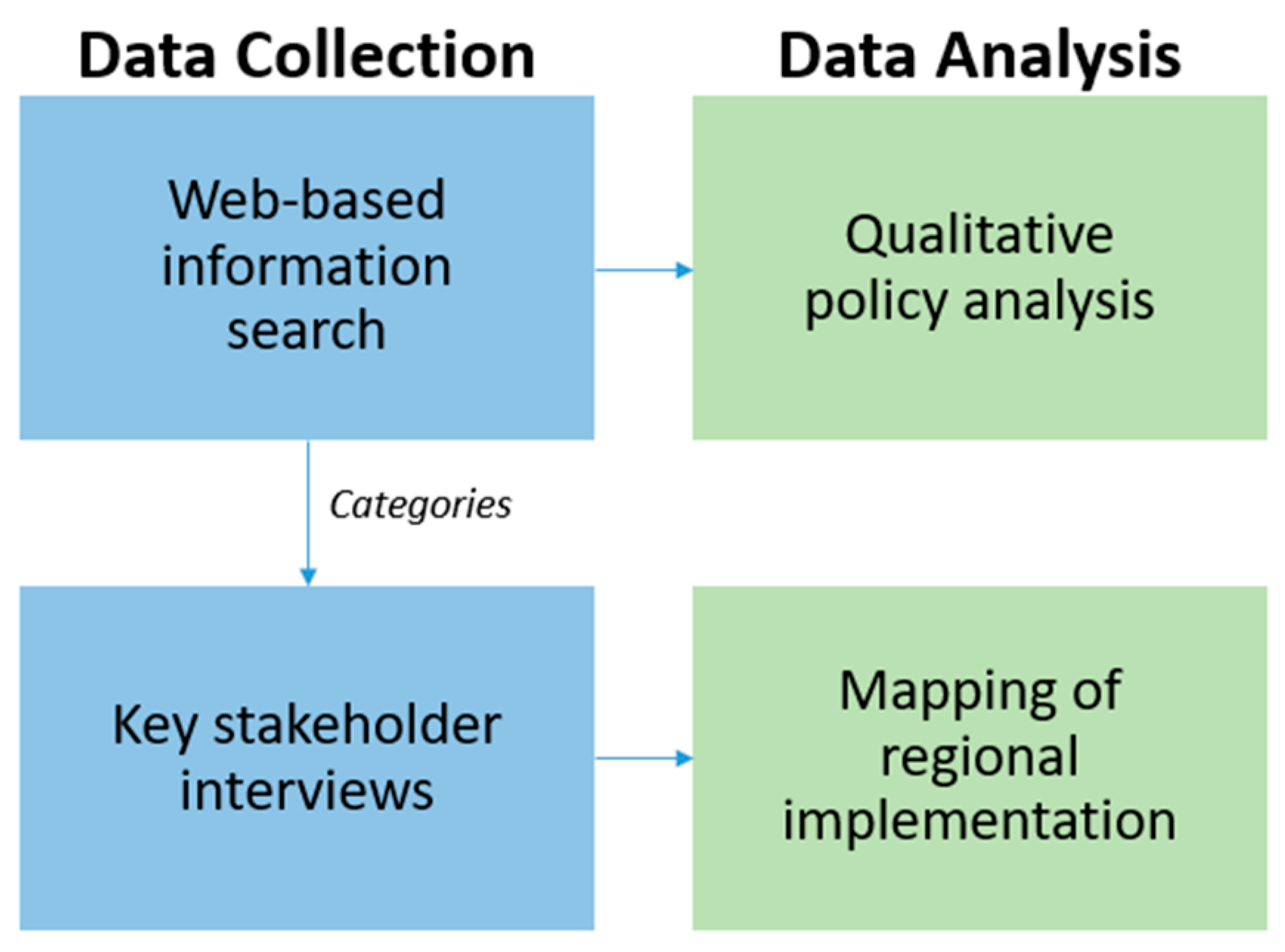
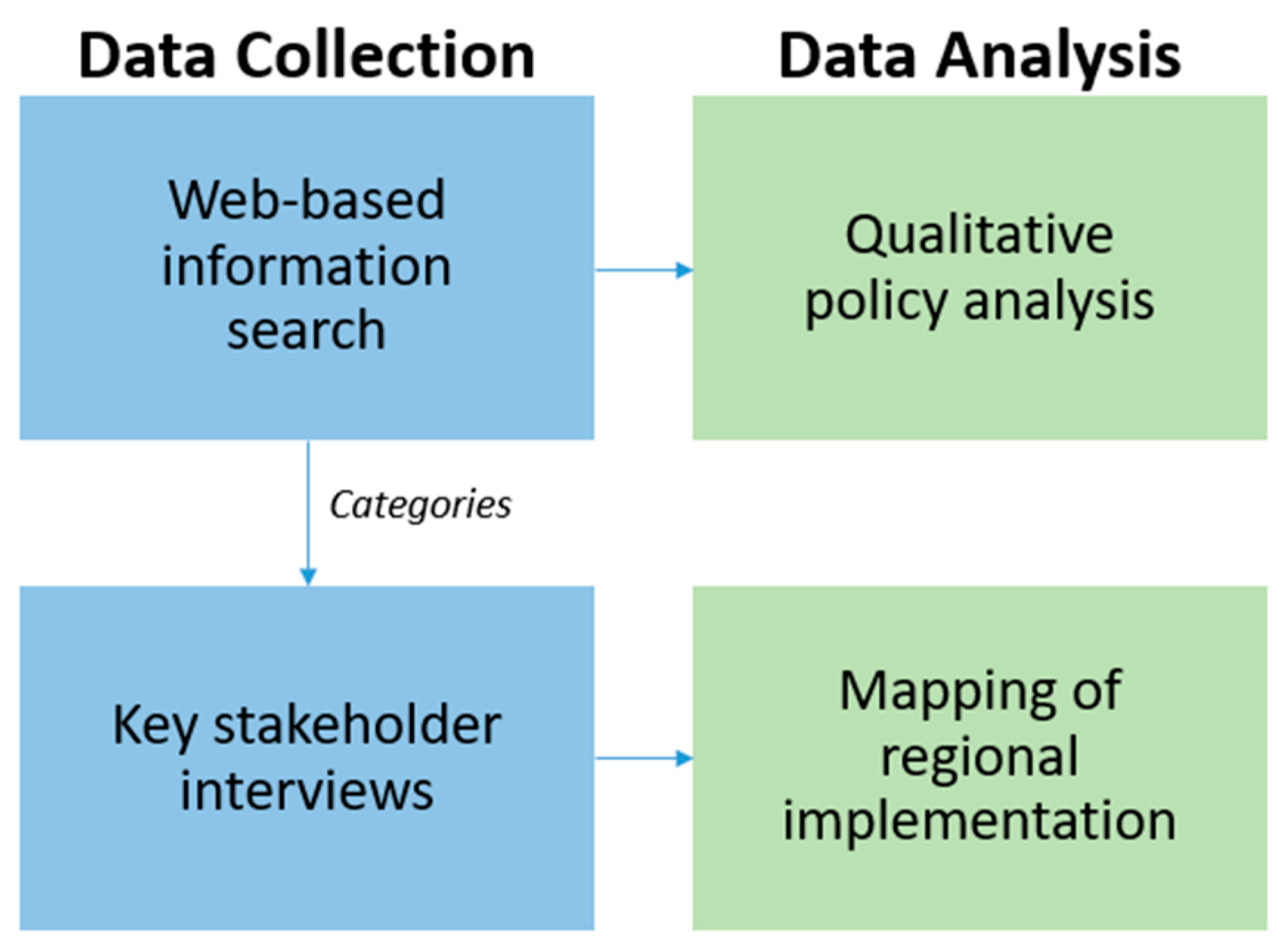
2. Materials and Methods
3. Results
3.1. Sharing Notes in Psychiatric Care
3.2. Regional Policies and Regulatory Documents
4. Discussion
Limitations and Future Work
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- How do you relate to the regions regarding publication of health records online (Journalen)?
- If you do not relate to the regions, do you have your own policy?
- IF YES, can we take part in it/them?
- IF YES, please answer the following questions (numbers 3 and 4).
- Do patients have access to their psychiatric notes?
- IF YES,
- From which psychiatric care setting (forensic, paediatric and adolescent, and adult)?
- From both inpatient and outpatient care? Or only from one, in such cases, which one?
- Are both signed and unsigned notes shared?
- i.
- If only signed notes are shared, are there any plans in the future to include unsigned notes as well?
- Is there 14 days of respite?
- i.
- If yes, are there any plans in the future to remove the delay of notes?
- IF NO,
- Are there any plans to make psychiatric notes available for patients in the future?
- i
- If yes, what is your timeline?
- 4.
- Is there a written policy/regulation document of documentation of psychiatric notes?
- IF YES, can we take part in it/them?
- IF NO, is there anything else (document) that supports you?
References
- Blease, C.; Salmi, L.; Rexhepi, H.; Hägglund, M.; DesRoches, C.M. Patients, clinicians and open notes: Information blocking as a case of epistemic injustice. J. Med. Ethics 2021. [Google Scholar] [CrossRef]
- Moll, J.; Rexhepi, H.; Cajander, Å.; Grünloh, C.; Huvila, I.; Hägglund, M.; Myreteg, G.; Scandurra, I.; Åhlfeldt, R.-M. Patients’ Experiences of Accessing Their Electronic Health Records: National Patient Survey in Sweden. J. Med. Internet Res. 2018, 20, e278. [Google Scholar] [CrossRef]
- Delbanco, T.; Walker, J.; Bell, S.K.; Darer, J.D.; Elmore, J.G.; Farag, N.; Feldman, H.J.; Mejilla, R.; Ngo, L.; Ralston, J.D.; et al. Inviting Patients to Read Their Doctors’ Notes: A Quasi-experimental Study and a Look Ahead. Ann. Intern. Med. 2012, 157, 461–470. [Google Scholar] [CrossRef]
- Walker, J.; Leveille, S.; Bell, S.; Chimowitz, H.; Dong, Z.; Elmore, J.G.; Fernandez, L.; Fossa, A.; Gerard, M.; Fitzgerald, P.; et al. OpenNotes After 7 Years: Patient Experiences With Ongoing Access to Their Clinicians’ Outpatient Visit Notes. J. Med. Internet Res. 2019, 21, e13876. [Google Scholar] [CrossRef]
- Kristiansen, E.; Johansen, M.A.; Zanaboni, P. Healthcare personnels’ experience with patients’ online access to electronic health records Differences between professions, regions, and somatic and psychiatric healthcare. Linköp. Electron. Conf. Proc. 2019, 161, 93–98. [Google Scholar]
- Jormanainen, V.; Parhiala, K.; Niemi, A.; Erhola, M.; Keskimäki, I.; Kaila, M. Half of the Finnish population accessed their own data: Comprehensive access to personal health information online is a corner-stone of digital revolution in Finnish health and social care. FinJeHeW 2019, 11, 298–310. [Google Scholar] [CrossRef] [Green Version]
- Nøhr, C.; Parv, L.; Kink, P.; Cummings, E.; Almond, H.; Nørgaard, J.R.; Turner, P. Nationwide citizen access to their health data: Analysing and comparing experiences in Denmark, Estonia and Australia. BMC Health Serv. Res. 2017, 17, 534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, J.; Meltsner, M.; Delbanco, T. US experience with doctors and patients sharing clinical notes. BMJ 2015, 350, g7785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Neill, S.; Blease, C.; Delbanco, T. Open Notes Become Law: A Challenge for Mental Health Practice. Psychiatr. Serv. 2021, 72, 750–751. [Google Scholar] [CrossRef]
- Wiljer, D.; Urowitz, S.; Apatu, E.; DeLenardo, C.; Eysenbach, G.; Harth, T.; Pai, H.; Leonard, K.J.; Canadian Committee for Patient Accessible Health Records (CCPAEHR). Patient accessible electronic health records: Exploring recommendations for successful implementation strategies. J. Med. Internet Res. 2008, 10, e34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blease, C.; Walker, J.; Torous, J.; O’Neill, S. Sharing Clinical Notes in Psychotherapy: A New Tool to Strengthen Patient Autonomy. Front. Psychiatry 2020, 11, 527872. [Google Scholar] [CrossRef]
- Blease, C.; O’Neill, S.; Walker, J.; Hägglund, M.; Torous, J. Sharing notes with mental health patients: Balancing risks with respect. Lancet Psychiatry 2020, 7, 924–925. [Google Scholar] [CrossRef]
- Denneson, L.M.; Chen, J.I.; Pisciotta, M.; Tuepker, A.; Dobscha, S.K. Patients’ Positive and Negative Responses to Reading Mental Health Clinical Notes Online. Psychiatr. Serv. 2018, 69, 593–596. [Google Scholar] [CrossRef] [PubMed]
- Leung, K.; Clark, C.; Sakal, M.; Friesen, M.; Strudwick, G. Patient and Family Member Readiness, Needs, and Perceptions of a Mental Health Patient Portal: A Mixed Methods Study. Stud. Health Technol. Inform. 2019, 257, 266–270. [Google Scholar] [PubMed]
- Peck, P.; Torous, J.; Shanahan, M.; Fossa, A.; Greenberg, W. Patient access to electronic psychiatric records: A pilot study. Health Policy Technol. 2017, 6, 309–315. [Google Scholar] [CrossRef]
- O’Neill, S.; Chimowitz, H.; Leveille, S.; Walker, J. Embracing the new age of transparency: Mental health patients reading their psychotherapy notes online. J. Ment. Health 2019, 28, 527–535. [Google Scholar] [CrossRef] [PubMed]
- Salmi, L.; Brudnicki, S.; Isono, M.; Riggare, S.; Rodriques, C.; Schaper, L.K.; Walker, J.; Delbanco, T. Six countries, six individuals: Resourceful patients navigating medical records in Australia, Canada, Chile, Japan, Sweden and the USA. BMJ Open 2020, 10, e037016. [Google Scholar] [CrossRef] [PubMed]
- Cromer, R.; Denneson, L.M.; Pisciotta, M.; Williams, H.; Woods, S.; Dobscha, S.K. Trust in Mental Health Clinicians Among Patients Who Access Clinical Notes Online. Psychiatr. Serv. 2017, 68, 520–523. [Google Scholar] [CrossRef]
- Pisciotta, M.; Denneson, L.M.; Williams, H.B.; Woods, S.; Tuepker, A.; Dobscha, S.K. Providing mental health care in the context of online mental health notes: Advice from patients and mental health clinicians. J. Ment. Health 2019, 28, 64–70. [Google Scholar] [CrossRef]
- Blease, C.R.; O’Neill, S.F.; Torous, J.; DesRoches, C.M.; Hägglund, M. Patient Access to Mental Health Notes: Motivating Evidence-Informed Ethical Guidelines. J. Nerv. Ment. Dis. 2021, 209, 265–269. [Google Scholar] [CrossRef]
- Rexhepi, H.; Moll, J.; Huvila, I. Online electronic healthcare records: Comparing the views of cancer patients and others. Health Inform. J. 2020, 26, 2915–2929. [Google Scholar] [CrossRef] [PubMed]
- Moll, J.; Cajander, Å. Oncology health-care professionals’ perceived effects of patient accessible electronic health records 6 years after launch: A survey study at a major university hospital in Sweden. Health Inform. J. 2020, 26, 1392–1403. [Google Scholar] [CrossRef] [Green Version]
- Petersson, L.; Erlingsdottir, G. Open Notes in Swedish Psychiatric Care (Part 1): Survey Among Psychiatric Care Professionals. JMIR Ment. Health 2018, 5, e11. [Google Scholar] [CrossRef] [PubMed]
- Dobscha, S.K.; Denneson, L.M.; Jacobson, L.E.; Williams, H.B.; Cromer, R.; Woods, S. VA mental health clinician experiences and attitudes toward OpenNotes. Gen. Hosp. Psychiatry 2016, 38, 89–93. [Google Scholar] [CrossRef]
- Petersson, L.; Erlingsdottir, G. Open Notes in Swedish Psychiatric Care (Part 2): Survey Among Psychiatric Care Professionals. JMIR Ment. Health 2018, 5, e10521. [Google Scholar] [CrossRef] [PubMed]
- Strudwick, G.; Clark, C.; Sanches, M.; Strauss, J. Predicators of Mental Health Professionals’ Perceptions of Patient Portals. AMIA Annu. Symp. Proc. 2018, 2018, 989–997. [Google Scholar]
- Denneson, L.M.; Cromer, R.; Williams, H.B.; Pisciotta, M.; Dobscha, S.K. A Qualitative Analysis of How Online Access to Mental Health Notes Is Changing Clinician Perceptions of Power and Therapeutic Relationship. J. Med. Internet Res. 2017, 19, e208. [Google Scholar] [CrossRef] [Green Version]
- Chimowitz, H.; O’Neill, S.; Leveille, S.; Welch, K.; Walker, J. Sharing Psychotherapy Notes with patients: Therapists’ Attitudes and Experiences. Soc. Work 2020, 65, 159–168. [Google Scholar] [CrossRef]
- Erlingsdóttir, G.; Petersson, L.; Jonnergård, K.A. A Theoretical Twist on the Transparency of Open Notes: Qualitative Analysis of Health Professionals’ Free-text Answers. J. Med. Internet Res. 2019, 21, e14347. [Google Scholar] [CrossRef]
- Bärkås, A.; Scandurra, I.; Hägglund, M. Analysis of Voluntary User Feedback of the Swedish National PAEHR Service. Stud. Health Technol. Inform. 2019, 264, 1126–1130. [Google Scholar] [CrossRef]
- Journalen. Available online: https://www.inera.se/tjanster/alla-tjanster-a-o/journalen/ (accessed on 14 June 2021).
- Scandurra, I.; Pettersson, M.; Eklund, B.; Lyttkens, L. Analysis of the Updated Swedish Regulatory Framework of the Patient Accessible Electronic Health Record in Relation to Usage Experience. Stud. Health Technol. Inform. 2017, 245, 798–802. [Google Scholar] [PubMed]
- Fricker, M. Epistemic Injustice: Power and the Ethics of Knowing; Oxford University Press: Oxford, UK, 2007. [Google Scholar]
- Essén, A.; Scandurra, I.; Gerrits, R.; Humphrey, G.; Johansen, M.A.; Kierkegaard, P.; Koskinen, J.; Liaw, S.-T.; Odeh, S.; Ross, P.; et al. Patient Access to Electronic Health Records: Differences Across Ten Countries. Health Policy Technol. 2018, 7, 44–56. [Google Scholar] [CrossRef]

{kind=link}
| Shared Notes in Psychiatric Care | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Regions/private care providers sharing psychiatric notes | YES | ||||||||||||||||||||||||
| NO | |||||||||||||||||||||||||
| Psychiatric care settings notes are available from | Adults | ||||||||||||||||||||||||
| Pediatrics–Adolescents | |||||||||||||||||||||||||
| Forensic | N/A | N/A | N/A | N/A | N/A | ||||||||||||||||||||
| How Psychiatric Notes are Shared | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Outpatient | |||||||||||||||||||
| Inpatient | N/A | ||||||||||||||||||
| Signed notes | |||||||||||||||||||
| Unsigned notes | |||||||||||||||||||
| Immediate access | |||||||||||||||||||
| Immediate access signed notes only | |||||||||||||||||||
| Immediate access outpatient only | |||||||||||||||||||
| Respite 14 days | |||||||||||||||||||
| Respite 14 days unsigned notes only | |||||||||||||||||||
| Respite 28 days inpatient only |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bärkås, A.; Scandurra, I.; Rexhepi, H.; Blease, C.; Cajander, Å.; Hägglund, M. Patients’ Access to Their Psychiatric Notes: Current Policies and Practices in Sweden. Int. J. Environ. Res. Public Health 2021, 18, 9140. https://doi.org/10.3390/ijerph18179140
Bärkås A, Scandurra I, Rexhepi H, Blease C, Cajander Å, Hägglund M. Patients’ Access to Their Psychiatric Notes: Current Policies and Practices in Sweden. International Journal of Environmental Research and Public Health. 2021; 18(17):9140. https://doi.org/10.3390/ijerph18179140
Chicago/Turabian StyleBärkås, Annika, Isabella Scandurra, Hanife Rexhepi, Charlotte Blease, Åsa Cajander, and Maria Hägglund. 2021. "Patients’ Access to Their Psychiatric Notes: Current Policies and Practices in Sweden" International Journal of Environmental Research and Public Health 18, no. 17: 9140. https://doi.org/10.3390/ijerph18179140
APA StyleBärkås, A., Scandurra, I., Rexhepi, H., Blease, C., Cajander, Å., & Hägglund, M. (2021). Patients’ Access to Their Psychiatric Notes: Current Policies and Practices in Sweden. International Journal of Environmental Research and Public Health, 18(17), 9140. https://doi.org/10.3390/ijerph18179140