
Physical Activity Patterns of Women with a Twin Pregnancy—A Cross-Sectional Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
2.2. The Questionnaire
2.3. Sampling
2.4. Variables
2.5. Statistical Analysis
2.6. Ethic Committee Approval
3. Results
3.1. Study Population
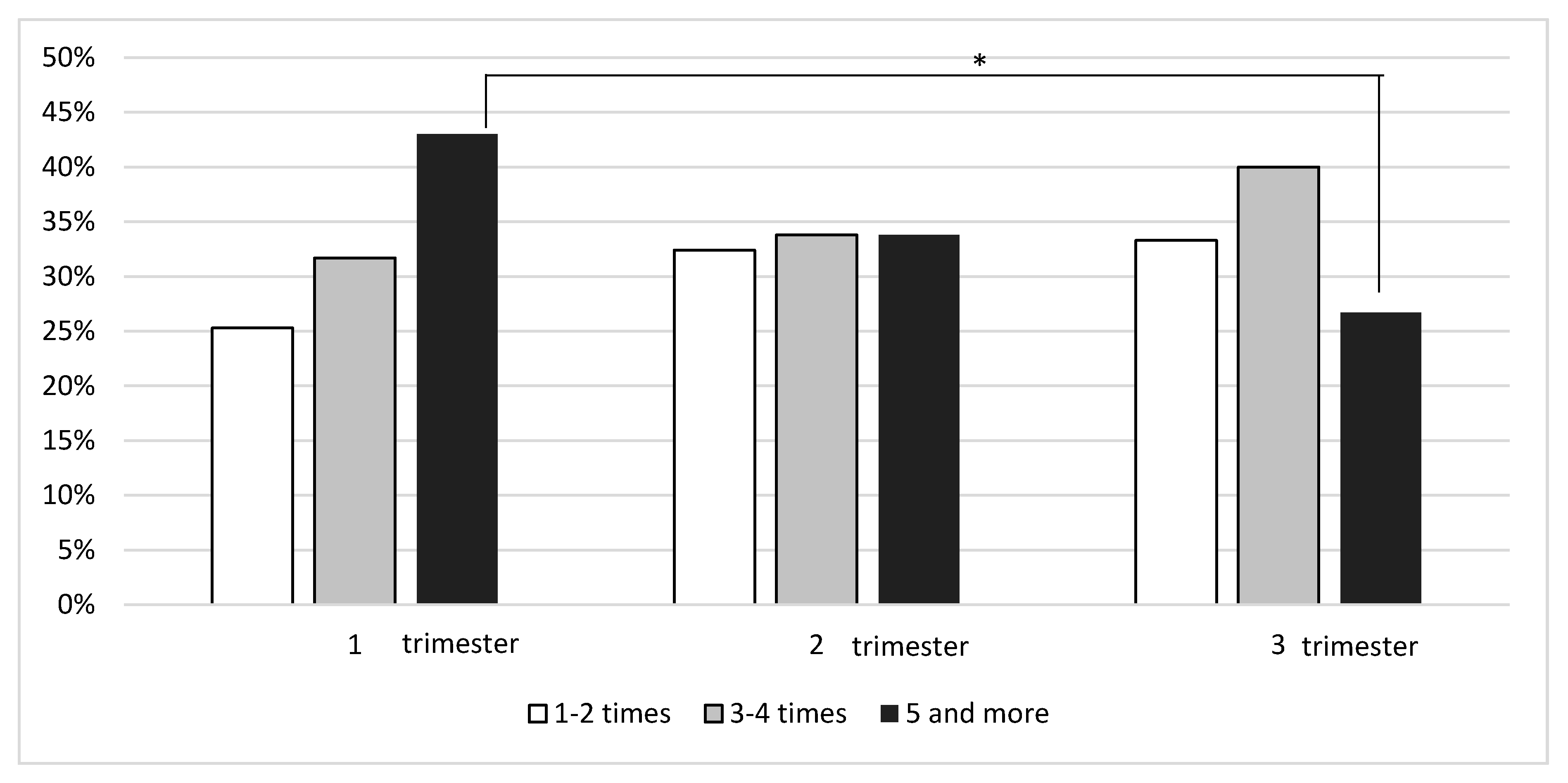
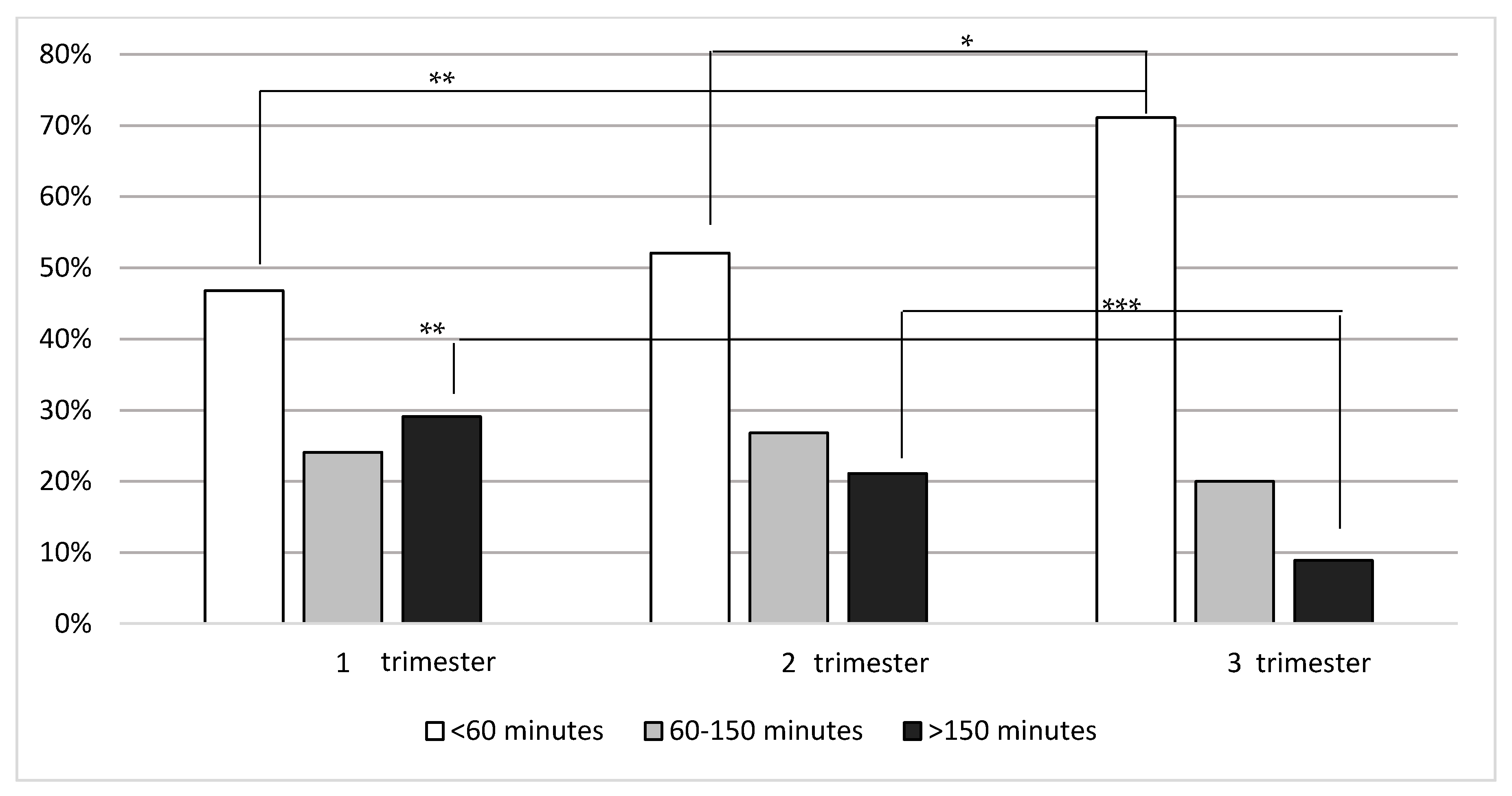
3.2. Physical Activity during Pregnancy
3.3. Pregnancy Ailments
3.4. The Course of Pregnancy and Delivery
3.5. The Sources of Information about Physical Activity during Pregnancy
3.6. Social Attitude toward Physical Activity during Pregnancy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cordero, Y.; Mottola, M.F.; Vargas, J.; Blanco, M.; Barakat, R. Exercise Is Associated with a Reduction in Gestational Diabetes Mellitus. Med. Sci. Sports Exerc. 2015, 47, 1328–1333. [Google Scholar] [CrossRef] [Green Version]
- Magro-Malosso, E.R.; Saccone, G.; Di Tommaso, M.; Roman, A.; Berghella, V. Exercise during pregnancy and risk of gestational hypertensive disorders: A systematic review and meta-analysis. Acta Obstet. Gynecol. Scand. 2017, 96, 921–931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magro-Malosso, E.R.; Saccone, G.; Di Mascio, D.; Di Tommaso, M.; Berghella, V. Exercise during pregnancy and risk of preterm birth in overweight and obese women: A systematic review and meta-analysis of ran-domized controlled trials. Acta Obstet. Gynecol. Scand. 2017, 96, 263–273. [Google Scholar] [CrossRef] [Green Version]
- Price, B.B.; Amini, S.B.; Kappeler, K. Exercise in pregnancy: Effect on fitness and obstetric outcomes-a ran-domized trial. Med. Sci. Sports Exerc. 2012, 44, 2263–2269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakamura, A.; van der Waerden, J.; Melchior, M.; Bolze, C.; El-Khoury, F.; Pryor, L. Physical activity during pregnancy and postpartum depression: Systematic review and meta-analysis. J. Affect. Disord. 2019, 246, 29–41. [Google Scholar] [CrossRef]
- American College of Obstetricians and Gynecologists. ACOG Committee Opinion No. 650: Physical activity and exercise during pregnancy and the postpartum period. Obstet. Gynecol. 2015, 126, e135–e142. [Google Scholar] [CrossRef]
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World. 2018. Available online: https://www.who.int/ncds/prevention/physical-activity/global-action-plan-2018-2030/en/ (accessed on 20 May 2021).
- Mottola, M.F.; Davenport, M.H.; Ruchat, S.-M.; Davies, G.A.; Poitras, V.J.; Gray, C.; Garcia, A.J.; Barrowman, N.; Adamo, K.B.; Duggan, M.; et al. 2019 Canadian guideline for physical activity throughout pregnancy. Br. J. Sports Med. 2018, 52, 1339–1346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamilton, B.E.; Martin, J.A.; Osterman, M.J.K. Births: Preliminary Data for 2015. Natl. Vital. Stat. Rep. 2016, 65, 1–15. [Google Scholar]
- Central Statistical Office. Demographic Yearbook of Poland; Głównego Urzędu Statystycznego (GUS): Warsaw, Poland, 2014.
- Whitaker, K.M.; Baruth, M.; Schlaff, R.A.; Talbot, H.; Connolly, C.P.; Liu, J.; Wilcox, S. Provider advice on physical activity and nutrition in twin pregnancies: A cross-sectional electronic survey. BMC Pregnancy Childbirth 2019, 19, 418. [Google Scholar] [CrossRef]
- Central Statistical Office. Demographic Yearbook of Poland; Głównego Urzędu Statystycznego (GUS): Warsaw, Poland, 2019.
- Lopriore, E.; Stroeken, H.; Sueters, M.; Meerman, R.J.; Walther, F.; Vandenbussche, F. Term perinatal mortal-ity and morbidity in monochorionic and dichorionic twin pregnancies: A retrospective study. Acta Obstet. Gynecol. Scand. 2008, 87, 541–545. [Google Scholar] [CrossRef]
- Tarter, J.G.; Khoury, A.; Barton, J.R.; Jacques, D.L.; Sibai, B.M. Demographic and obstetric factors influencing pregnancy outcome in twin gestations. Am. J. Obstet. Gynecol. 2002, 186, 910–912. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, L.; Surita, F.G.; Cecatti, J.G. Physical exercise during pregnancy: A systematic review. Curr. Opin. Obstet. Gynecol. 2012, 24, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Nazik, E.; Eryilmaz, G. Incidence of pregnancy-related discomforts and management approaches to relieve them among pregnant women. J. Clin. Nurs. 2013, 23, 1736–1750. [Google Scholar] [CrossRef]
- Walasik, I.; Kwiatkowska, K.; Kaczyńska, K.K.; Szymusik, I. Physical Activity Patterns among 9000 Pregnant Women in Poland: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 1771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Institute of Medicine. Weight Gain during Pregnancy: Re-Examining the Guidelines; The National Academies Press: Washington, DC, USA, 2009. [Google Scholar]
- Ghi, T.; Prefumo, F.; Fichera, A.; Lanna, M.; Periti, E.; Persico, N.; Viora, E.; Rizzo, G. Società Italiana di Eco-grafia Ostetrica e Ginecologica Working Group on Fetal Biometric Charts. Development of customized fetal growth charts in twins. Am. J. Obstet. Gynecol. 2017, 216, e1–e514. [Google Scholar]
- Evenson, K.R.; Savitz, A.; Huston, S.L. Leisure-time physical activity among pregnant women in the US. Paediatr. Périnat. Epidemiol. 2004, 18, 400–407. [Google Scholar] [CrossRef]
- Evenson, K.R.; Wen, F. National trends in self-reported physical activity and sedentary behaviors among pregnant women: NHANES 1999–2006. Prev. Med. 2010, 50, 123–128. [Google Scholar] [CrossRef]
- Sprague, A.E.; O’Brien, B.; Newburn-Cook, C.; Heaman, M.; Nimrod, C. Bed rest and activity restriction for women at risk for preterm birth: A survey of Canadian prenatal care providers. J. Obstet. Gynaecol. Can. 2008, 30, 317–326. [Google Scholar] [CrossRef]
- Fox, N.S.; Gelber, S.E.; Kalish, R.B.; Chasen, S.T. The recommendation for bed rest in the setting of arrested preterm labor and premature rupture of membranes. Am. J. Obstet. Gynecol. 2009, 200, 165.e1–165.e6. [Google Scholar] [CrossRef] [PubMed]
- Lopes, K.D.S.; Takemoto, Y.; Ota, E.; Tanigaki, S.; Mori, R. Bed rest with and without hospitalisation in multiple pregnancy for improving perinatal outcomes. Cochrane Database Syst. Rev. 2017, 3, CD012031. [Google Scholar] [CrossRef]
- Kovacevich, G.J.; Gaich, S.A.; Lavin, J.P.; Hopkins, M.P.; Crane, S.S.; Stewart, J.; Nelson, D.; Lavin, L.M. The prevalence of thromboembolic events among women with extended bed rest prescribed as part of the treatment for premature labor or preterm premature rupture of membranes. Am. J. Obstet. Gynecol. 2000, 182, 1089–1092. [Google Scholar] [CrossRef] [PubMed]
- Promislow, J.H.; Hertz-Picciotto, I.; Schramm, M.; Watt-Morse, M.; Anderson, J.J. Bed rest and other deter-minants of bone loss during pregnancy. Am. J. Obstet. Gynecol. 2004, 191, 1077–1083. [Google Scholar] [CrossRef] [PubMed]
- A Maloni, J.; Chance, B.; Zhang, C.; Cohen, A.W.; Betts, D.; Gange, S.J. Physical and psychosocial side effects of antepartum hospital bed rest. Nurs. Res. 1993, 42, 197–203. [Google Scholar] [CrossRef]
- Maloni, J.A.; Alexander, G.R.; Schluchter, M.D.; Shah, D.M.; Park, S. Antepartum Bed Rest: Maternal Weight Change and Infant Birth Weight. Biol. Res. Nurs. 2004, 5, 177–186. [Google Scholar] [CrossRef]
- Maloni, A.; Kasper, C.E. Physical and psychosocial effects of antepartum hospital bedrest: A review of the literature. IMAGE J. Nurs. Scholarsh. 1991, 23, 187–192. [Google Scholar] [CrossRef]
- May, K.A. Impact of prescribed activity restriction during pregnancy on women and families. Health Care Women Int. 2001, 22, 29–47. [Google Scholar] [CrossRef] [PubMed]
- Wender-Ożegowska, E.; Bomba-Opoń, D.; Brązert, J.; Celewicz, Z.; Czajkowski, K.; Gutaj, P.; Malinowska-Polubiec, A.; Zawiejska, A.; Wielgoś, M. Standards of Polish Society of Gynecologists and Obstetricians in management of women with diabetes. Ginekol. Pol. 2018, 89, 341–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Findley, A.; Smith, D.M.; Hesketh, K.; Keyworth, C. Exploring womens’ experiences and decision making about physical activity during pregnancy and following birth: A qualitative study. BMC Pregnancy Childbirth 2020, 20, 54. [Google Scholar] [CrossRef] [Green Version]
- Barakat, R.; Pelaez, M.; Lopez, C.; Montejo, R.; Coteron, J. Exercise during pregnancy reduces the rate of ce-sarean and instrumental deliveries: Results of a randomized controlled trial. J. Matern. Fetal Neonat. Med. 2012, 25, 2372–2376. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Study Group N = 652 | Physically Active N = 162 | Physically Non-Active N = 490 | ||
|---|---|---|---|---|
| % (N) | % (N) | % (N) | p | |
| Age (years) | ||||
| <20 | 0 (2) | 0 (0) | 0 (2) | 1.00 |
| 21–30 | 59 (382) | 56 (90) | 60 (292) | 0.41 |
| 31–40 | 40 (264) | 43 (70) | 40 (194) | 0.46 |
| 41–50 | 1 (4) | 1 (2) | 0 (2) | 0.26 |
| Education | ||||
| Basic | 1 (4) | 0 (0) | 1 (4) | 0.58 |
| Secondary | 31 (204) | 22 (36) | 34 (168) | 0.004 |
| Higher | 63 (412) | 74 (120) | 60 (292) | 0.001 |
| Vocational | 5 (32) | 4 (6) | 5 (26) | 0.53 |
| Inhabitancy | ||||
| Countryside | 27 (178) | 14 (22) | 32 (156) | <0.001 |
| Town < 50,000 | 18 (116) | 27 (44) | 15 (72) | 0.001 |
| City 50,000–100,000 | 14 (94) | 12 (20) | 15 (74) | 0.44 |
| City 100,000–500,000 | 18 (114) | 22 (36) | 16 (78) | 0.07 |
| City > 500,000 | 23 (150) | 25 (40) | 22 (110) | 0.59 |
| Parity | ||||
| Primiparous | 60 (388) | 59 (96) | 60 (292) | 1.00 |
| Multiparous | 40 (264) | 41 (66) | 40 (198) | 1.00 |
| Physical activity before pregnancy | ||||
| I didn’t exercise | 37 (242) | 10 (16) | 46 (226) | <0.001 |
| Less than 6 months | 13 (82) | 6 (10) | 15 (72) | 0.03 |
| 6 months–2 years | 22 (144) | 28 (46) | 20 (98) | 0.02 |
| >2 years | 28 (184) | 56 (90) | 19 (94) | <0.001 |
| Pre-pregnancy BMI a | ||||
| Underweight | 8 (54) | 6 (10) | 9 (44) | 0.32 |
| Normal | 61 (398) | 67 (108) | 59 (290) | 0.09 |
| Overweight | 21 (136) | 20 (32) | 21 (104) | 0.74 |
| Obese | 10 (64) | 7 (12) | 11 (52) | 0.29 |
| Gestational weight gain | ||||
| Normal weight N = 398 | ||||
| adequate | 39 (154) | 37 (40) | 39 (114) | 0.73 |
| inadequate | 53 (210) | 52 (56) | 53 (154) | 0.91 |
| excessive | 8 (34) | 11 (12) | 8 (22) | 0.31 |
| Overweight N = 136 | ||||
| adequate | 43 (58) | 44 (14) | 42 (44) | 1.00 |
| inadequate | 44 (60) | 44 (14) | 44 (46) | 1.00 |
| excessive | 13 (18) | 12 (4) | 14 (14) | 1.00 |
| Obese N = 64 | ||||
| adequate | 34 (22) | 50 (6) | 31(16) | 0.31 |
| inadequate | 53 (34) | 50 (6) | 54 (28) | 1.00 |
| excessive | 13 (8) | 0 (0) | 15 (8) | 0.33 |
| Study Group N = 652 | Physically Active N = 162 | Physically Non-Active N = 490 | ||
|---|---|---|---|---|
| % (N) | % (N) | % (N) | p | |
| Constipation | 43 (280) | 41 (66) | 44 (214) | 0.52 |
| Leg swelling | 54 (352) | 53 (86) | 54 (266) | 0.86 |
| Back pain | 65 (426) | 57 (92) | 68 (334) | 0.01 |
| Mood swings | 45 (296) | 47 (76) | 45 (220) | 0.72 |
| Fatigue | 78 (506) | 68 (110) | 81 (396) | 0.001 |
| Sleeping problems | 60 (394) | 53 (86) | 63 (308) | 0.03 |
| Decreased libido | 33 (212) | 32 (52) | 33 (160) | 0.92 |
| Heartburn | 67 (436) | 63 (102) | 68 (334) | 0.25 |
| Leg cramps | 36 (234) | 31 (50) | 38 (184) | 0.13 |
| Varicose veins | 13 (82) | 12 (20) | 13 (62) | 1.00 |
| Study Group N = 652 | Physically Active N = 162 | Physically Non-Active N = 490 | ||
|---|---|---|---|---|
| %/N | %/N | %/N | p | |
| Gestational age at delivery (weeks) | ||||
| <30 | 3 (22) | 0 (0) | 5 (22) | 0.002 |
| <34 | 25 (166) | 21 (34) | 27 (132) | 0.15 |
| <37 | 67 (436) | 60 (98) | 69 (338) | 0.05 |
| ≥37 | 33 (216) | 40 (64) | 31 (152) | 0.05 |
| GH a/PE b | 9 (58) | 9 (14) | 9 (44) | 1.00 |
| ICP c | 6 (38) | 4 (6) | 7 (32) | 0.2 |
| GDM d treated with diet | 32 (206) | 41 (66) | 29 (140) | 0.04 |
| Vaginal delivery | 7 (48) | 11 (18) | 6 (30) | 0.05 |
| Cesarean section | 93 (604) | 89 (144) | 94 (460) | 0.05 |
| Delivery onset | N e 48 | N e 18 | N e 30 | |
| Spontaneous | 79 (38) | 67 (12) | 87 (26) | 0.145 |
| Induced | 21 (10) | 33 (6) | 13 (4) | 0.145 |
| First win Dichorionic | N = 484 | N = 120 | N = 364 | |
| <10th | 4 (21) | 7 (8) | 4 (13) | 0.18 |
| <2500 g | 51 (248) | 55 (66) | 50 (182) | 0.35 |
| >2500 g | 49 (236) | 45 (54) | 50 (182) | 0.35 |
| Second twin Dichorionic | ||||
| <10th | 7 (36) | 8 (9) | 7 (27) | 1.00 |
| <2500 g | 56 (272) | 52 (62) | 58 (210) | 0.29 |
| >2500 g | 44 (212) | 48 (58) | 42 (154) | 0.29 |
| First twin Monochorionic diamniotic | N = 168 | N = 42 | N = 126 | |
| <10th | 8 (13) | 10 (4) | 7 (9) | 0.73 |
| <2500 g | 71 (120) | 52 (22) | 78 (98) | 0.003 |
| >2500 g | 29 (48) | 48 (20) | 22 (28) | 0.003 |
| Second twin Monochorionic diamniotic | ||||
| <10th | 8 (13) | 5 (2) | 9 (11) | 0.50 |
| <2500 g | 68 (114) | 62 (26) | 70 (88) | 0.35 |
| >2500 g | 32 (54) | 38 (16) | 30 (38) | 0.35 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwiatkowska, K.; Kosińska-Kaczyńska, K.; Walasik, I.; Osińska, A.; Szymusik, I. Physical Activity Patterns of Women with a Twin Pregnancy—A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 7724. https://doi.org/10.3390/ijerph18157724
Kwiatkowska K, Kosińska-Kaczyńska K, Walasik I, Osińska A, Szymusik I. Physical Activity Patterns of Women with a Twin Pregnancy—A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2021; 18(15):7724. https://doi.org/10.3390/ijerph18157724
Chicago/Turabian StyleKwiatkowska, Katarzyna, Katarzyna Kosińska-Kaczyńska, Izabela Walasik, Agnieszka Osińska, and Iwona Szymusik. 2021. "Physical Activity Patterns of Women with a Twin Pregnancy—A Cross-Sectional Study" International Journal of Environmental Research and Public Health 18, no. 15: 7724. https://doi.org/10.3390/ijerph18157724
APA StyleKwiatkowska, K., Kosińska-Kaczyńska, K., Walasik, I., Osińska, A., & Szymusik, I. (2021). Physical Activity Patterns of Women with a Twin Pregnancy—A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 18(15), 7724. https://doi.org/10.3390/ijerph18157724