
Effect of Water Amount Intake before Scuba Diving on the Risk of Decompression Sickness



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Experimental Design
2.3. Experimental Protocol
2.4. Statistical Analyses
3. Results
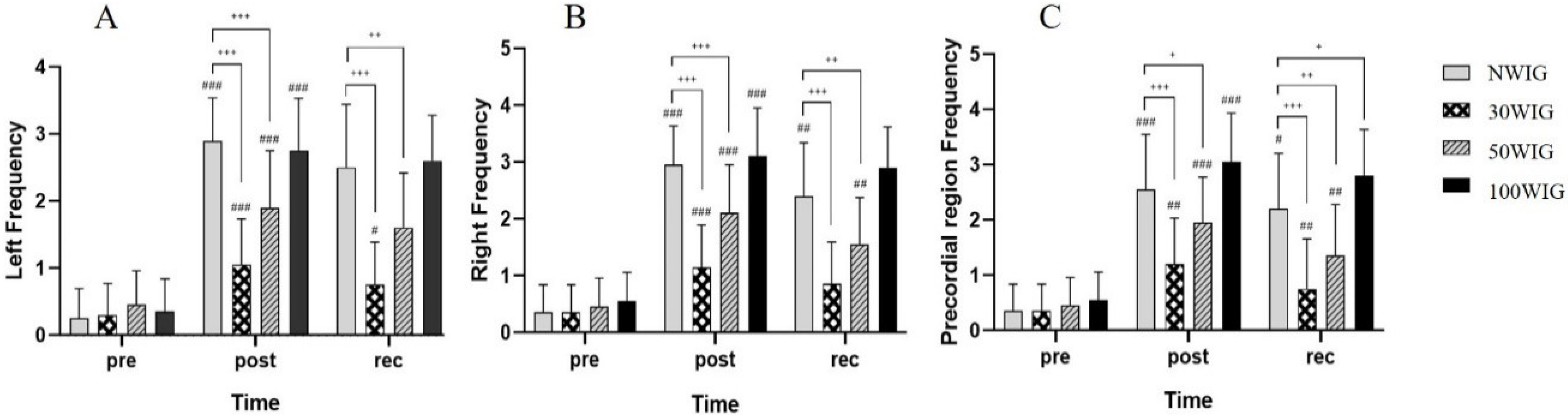
3.1. Changes in Frequency in the Left and Right Subclavian Veins and Precordial Region
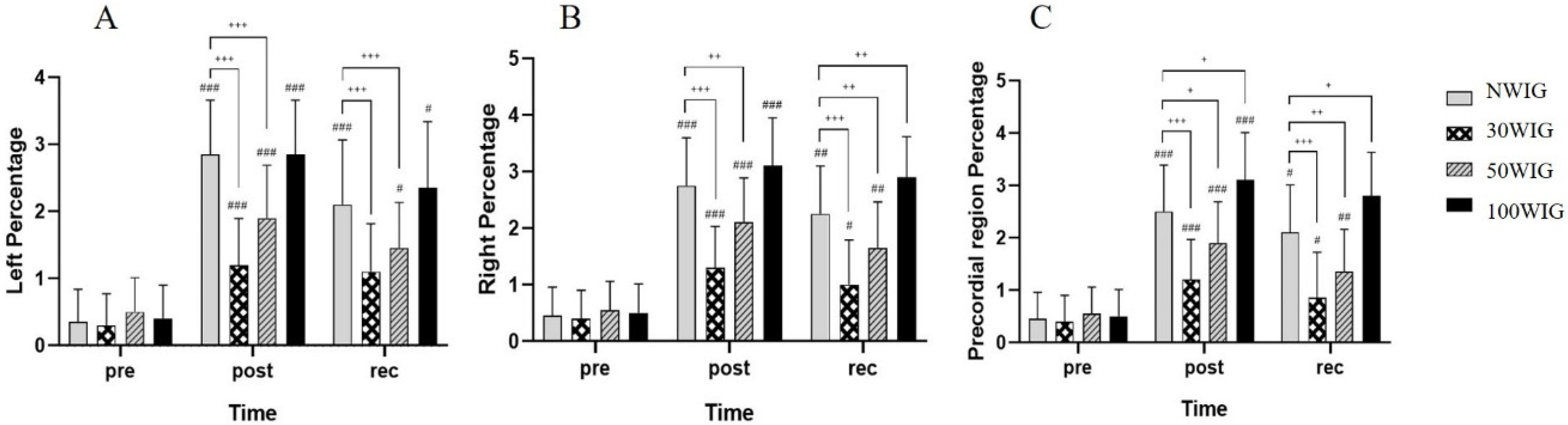
3.2. Changes of Percentage in the Left and Right Subclavian Veins and Precordial Region
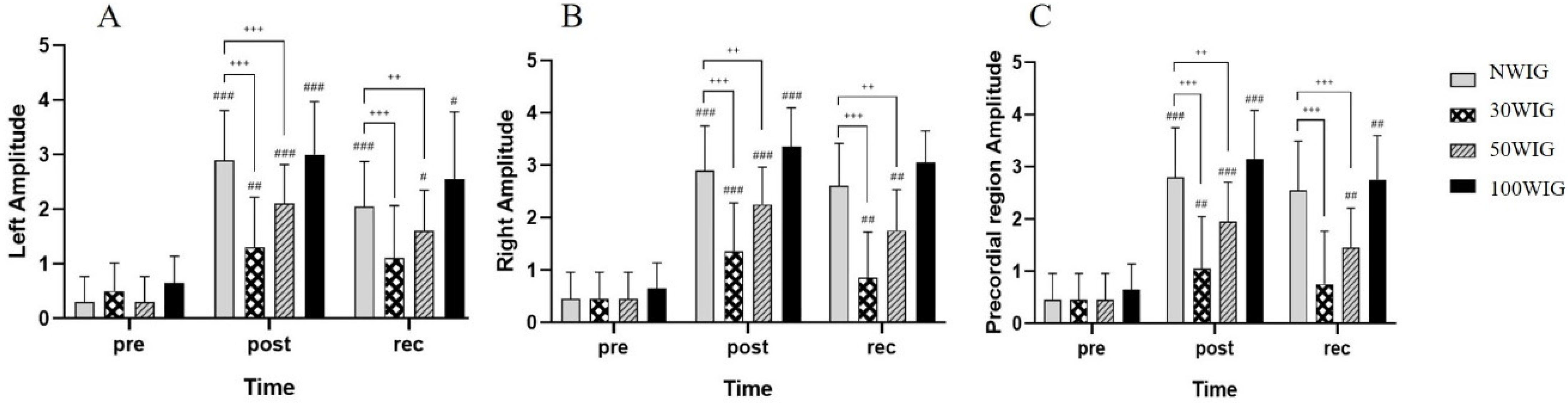
3.3. Changes of Amplitude in the Left and Right Subclavian Veins and Precordial Region
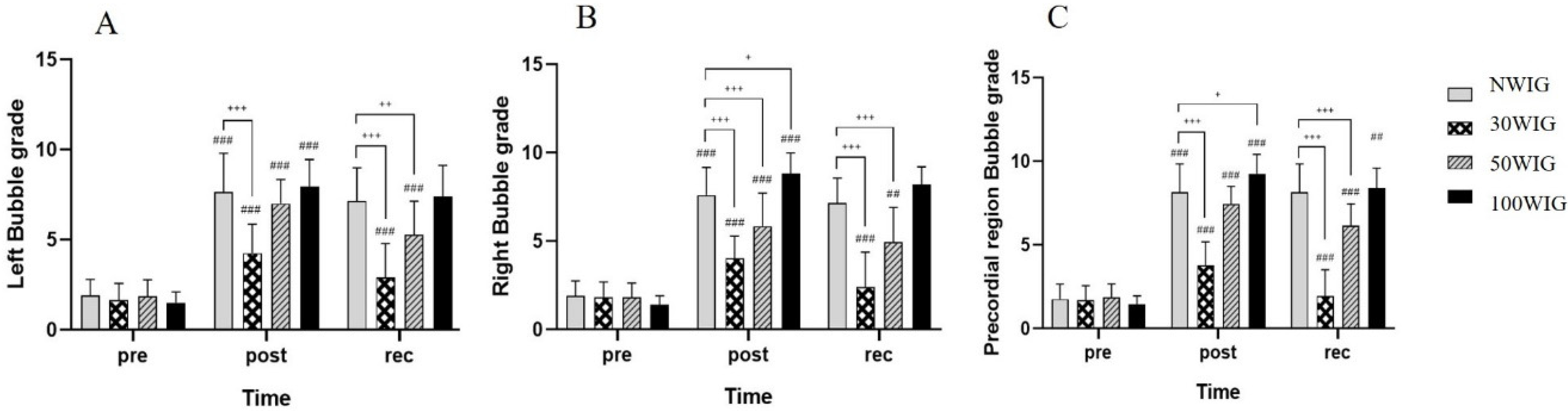
3.4. Bubble Grade Score at Pre-Dive, Post-Dive, and 30 Min into Recovery after Scuba Diving
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lynch, P.R. Historical and basic perspectives of SCUBA Diving. Med. Sci. Sports Exerc. 1996, 28, 570–572. [Google Scholar]
- Gempp, E.; Blatteau, J.-E. Preconditioning Methods and Mechanisms for Preventing the Risk of Decompression Sickness in Scuba Divers: A Review. Res. Sports Med. 2010, 18, 205–218. [Google Scholar] [CrossRef]
- Elliot, D.H.; Moon, R.E. Manifestations of the Decompression Disorders. In The Physiology and Medicine of Diving, 4th ed.; Bennett, P.B., Elliott, D.H., Eds.; W.B. Saunders: London, UK, 1993; p. 22. [Google Scholar]
- Landolfi, A.; Yang, Z.J.; Savini, F.; Camporesi, E.M.; Faralli, F.; Bosco, G.; Landolfi, A.; Yang, Z.J.; Savini, F.; Camporesi, E.M.; et al. Pre-treatment with hyperbaric oxygenation reduces bubble formation and platelet activation. Sport Sci. Health 2006, 1, 122–128. [Google Scholar] [CrossRef]
- Fahlman, A.; Dromsky, D.M. Dehydration effects on the risk of severe decompression sickness in a swine model. Aviat. Space Environ. Med. 2006, 77, 102–106. [Google Scholar]
- Blatteau, J.-E.; Boussuges, A.; Gempp, E.; Pontier, J.-M.; Castagna, O.; Robinet, C.; Galland, F.-M.; Bourdon, L. Haemodynamic changes induced by submaximal exercise before a dive and its consequences on bubble formation. Br. J. Sports Med. 2007, 41, 375–379. [Google Scholar] [CrossRef]
- Blatteau, J.-E.; Gempp, E.; Balestra, C.; Mets, T.; Germonpre, P. Predive sauna and venous gas bubbles upon decompression from 400 kPa. Aviat. Space Environ. Med. 2008, 79, 1100–1105. [Google Scholar] [CrossRef] [PubMed]
- Germonpré, P.; Pontier, J.-M.; Gempp, E.; Blatteau, J.-E.; Deneweth, S.; Lafère, P.; Marroni, A.; Balestra, C. Pre-dive vibration effect on bubble formation after a 30-m dive requiring a decompression stop. Aviat. Space Environ. Med. 2009, 80, 1044–1048. [Google Scholar] [CrossRef][Green Version]
- Gempp, E.; E Blatteau, J.; Pontier, J.-M.; Balestra, C.; Louge, P. Preventive effect of pre-dive hydration on bubble formation in divers. Br. J. Sports Med. 2009, 43, 224–228. [Google Scholar] [CrossRef]
- Gandy, J. Water intake: Validity of population assessment and recommendations. Eur. J. Nutr. 2015, 54, 11–16. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products Nutrition and Allergies (NDA). Scientific opinion on dietary reference values for water. EFSA J. 2010, 8, 1459. [Google Scholar]
- Institute of Medicine, Food and Nutrition Board. Dietary Reference Intakes for Water, Potassium, Sodium, Chloride and Sulfate; The National Academies Press: Washington, DC, USA, 2004. [Google Scholar]
- Reclamation Diving Safety Advisory Board. Diving Safe Practices Manual: Underwater Inspection Program; 2021; pp. 20–28. Available online: https://www.usbr.gov/safety/rshs/documents/diving/DivingManual.pdf (accessed on 5 May 2021).
- Pontier, J.-M.; Guerrero, F.; Castagna, O. Bubble formation and endothelial function before and after 3 months of dive training. Aviat. Space Environ. Med. 2009, 80, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Nishi, R.Y.; Brubakk, A.O.; Eftedal, O.S. Bubble Detection. In Bennett and Elliot’s Physiology and Medicine of Diving, 5th ed.; Brubakk, A.O., Neuman, T.S., Eds.; WB Saunders: London, UK, 2003; p. 419. [Google Scholar]
- Eatock, B.C.; Nishi, R.Y. Procedures for Doppler Ultrasonic Monitoring of Divers for Intravascular Bubbles; Defense Technical Information Center: Fort Belvoir, VA, USA, 1986; Pagination or Media Count: 31.0.
- Jeanningros, O.; Lagre, F.X.; Pontus, N. Haemodynamic Consequences of Dive-Induced Weight Loss and Diuresis Are Greater After the Second than the First Dive. In Proceedings of the XXVth Annual Meeting of the European Underwater and Baromedical Society, Haifa-Eilat, Israel, 28 August–2 September 1999. [Google Scholar]
- Blogg, S.L.; Gennser, M.; Møllerløkken, A.; Brubakk, A.O. Ultrasound detection of vascular decompression bubbles: The influence of new technology and considerations on bubble load. Diving Hyperb. Med. 2014, 44, 35–44. [Google Scholar] [PubMed]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef]
- Scott, E.M.; Greenwood, J.P.; Gilbey, S.G.; Stoker, J.B.; Mary, D.A. Water ingestion increases sympathetic vasoconstrictor discharge in normal human subjects. Clin. Sci. 2001, 100, 335–342. [Google Scholar] [CrossRef]
- Henrykowska, G.; Soin, J.; Siermontowski, P. Scuba Diving as a Form of Rehabilitation for People with Physical Disabilities. Int. J. Environ. Res. Public Health 2021, 18, 5678. [Google Scholar] [CrossRef] [PubMed]
- Haydn, T.; Brenneis, C.; Schmutzhard, J.; Gerstenbrand, F.; Saltuan, L.; Schmutzhard, E. Scuba diving—A therapeutic option for patients with paraplegia. Neuropsychiatry 2007, 21, 226–229. [Google Scholar]
- Bartels, E.M.; Juhl, C.B.; Christensen, R.; Hagen, K.B.; Danneskiold-Samsøe, B.; Dagfinrud, H.; Lund, H. Aquatic exercise for the treatment of knee and hip osteoarthritis. Cochrane Database Syst. Rev. 2016, 3, CD005523. [Google Scholar] [CrossRef]
- Geytenbeek, J. Evidence for Effective Hydrotherapy. Physiotherapy 2002, 88, 514–529. [Google Scholar] [CrossRef]
- McMillan, J. The role of water in rehabilitation. Fysioterapeuten 1978, 45, 87–90. [Google Scholar]
- Garcia, M.K.; Joares, E.C.; Silva, M.A.; Bissolotti, R.R.; Oliveira, S.; Battistella, L.R. The Halliwick Concept, inclusion and participation through aquatic functional activities. Acta Fisiátrica 2012, 19, 142–150. [Google Scholar] [CrossRef][Green Version]
- McNamara, R.J.; McKeough, Z.J.; McKenzie, D.K.; Alison, J.A. Water-based exercise in COPD with physical comorbidities: A randomised controlled trial. Eur. Respir. J. 2013, 41, 1284–1291. [Google Scholar] [CrossRef]
- Hjelde, A.; Koteng, S.; Eftedal, O.; Brubakk, O. Surface tension and bubble formation after decompression in the pig. Appl. Cardiopulm. Pathophysiol. 2000, 9, 47–52. [Google Scholar]
- Walder, D.N. Serum surface tension and its relation to the decompression sickness of aviators. J. Physiol. 1948, 107, 43–44. [Google Scholar]
- Møllerløkken, A.; Blogg, S.L.; Doolette, D.J.; Nishi, R.Y.; Pollock, N.W. Consensus guidelines for the use of ultrasound for diving research. Diving Hyperb. Med. J. 2016, 46, 26–32. [Google Scholar]
- Balestra, C.; Theunissen, S.; Papadopoulou, V.; Le Mener, C.; Germonpré, P.; Guerrero, F.; Lafère, P. Pre-dive Whole-Body Vibration Better Reduces Decompression-Induced Vascular Gas Emboli than Oxygenation or a Combination of Both. Front. Physiol. 2016, 7, 586. [Google Scholar] [CrossRef] [PubMed]
- Germonpré, P.; Balestra, C. Preconditioning to Reduce Decompression Stress in Scuba Divers. Aerosp. Med. Hum. Perform. 2017, 88, 114–120. [Google Scholar] [CrossRef]
- Imbert, J.-P.; Egi, S.M.; Germonpré, P.; Balestra, C. Static Metabolic Bubbles as Precursors of Vascular Gas Emboli During Divers’ Decompression: A Hypothesis Explaining Bubbling Variability. Front. Physiol. 2019, 10, 807. [Google Scholar] [CrossRef]
- House, C.M.; House, J.; Oakley, E.H. Findings from a simulated disabled submarine survival trial. Undersea Hyperb. Med. 2000, 27, 175–183. [Google Scholar]
- Hyun, G.-S.; Jee, Y.-S.; Park, J.-M.; Cho, N.-H.; Cha, J.-Y. Injury survey in scuba divers of British Sub-Aqua Club: A retrospective study. J. Exerc. Rehabil. 2015, 11, 331–336. [Google Scholar] [CrossRef]
- Gerth, W.A.; Ruterbusch, V.L.; Long, E.T. The Influence of Thermal Exposure on Diver Susceptibility to Decompression Sickness; Defense Technical Information Center (DTIC): Fort Belvoir, VA, USA, 2007.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Items | Groups | |||
|---|---|---|---|---|
| NWIG | 30WIG | 50WIG | 100WIG | |
| Diving environment | ||||
| Date | 10 February 2019 | 12 February 2019 | 14 February 2019 | 16 February 2019 |
| Temperature | 31.23 ± 0.12 °C | 29.92 ± 1.03 °C | 31.13 ± 0.13 °C | 31.41 ± 0.12 °C |
| Humidity | 78.22 ± 0.35% | 79.31 ± 0.24% | 79.83 ± 0.31% | 78.47 ± 0.22% |
| Water temperature | 28.75 ± 1.02 °C | 28.52 ± 1.38 °C | 28.92 ± 1.15 °C | 28.83 ± 1.72 °C |
| Diving methods | ||||
| Wave/maximum depth | 1 m/30 m | |||
| Bottom time/total diving time | 25 min/35 min | |||
| Ascent rate vs. ascent rate after deco | 9 m/min vs. 3 m/min | |||
| Deco time | 5 min at 5 m | |||
| Bubble Signals | Code | Frequency | Percentage | Amplitude | ||||
| 0 | 0 | 0 | No | |||||
| 1 | 1–2 | 1–10 | Ab << Ac | |||||
| 2 | 3–8 | 10–50 | Ab < Ac | |||||
| 3 | 9–40 | 50–99 | Ab = Ac | |||||
| 4 | Continuation | 100 | Ab > Ac | |||||
| KM code for bubble grade | f p a | g | f p a | g | f p a | g | f p a | g |
| 111 | I− | 211 | I− | 311 | I | 411 | II− | |
| 112 | I | 212 | I | 312 | II− | 412 | II | |
| 113 | I | 213 | I+ | 313 | II | 413 | II+ | |
| 114 | I+ | 214 | II− | 314 | II | 414 | III− | |
| 121 | I+ | 221 | II− | 321 | II | 421 | III− | |
| 122 | II | 222 | II | 322 | II+ | 422 | III | |
| 123 | II | 223 | II+ | 323 | III− | 423 | III | |
| 124 | II | 224 | II+ | 324 | III | 424 | III+ | |
| 131 | II | 231 | II | 331 | III− | 431 | III | |
| 132 | II | 232 | III− | 332 | III | 432 | III+ | |
| 133 | III− | 233 | III | 333 | III | 433 | IV− | |
| 134 | III− | 234 | III | 334 | III+ | 434 | IV | |
| 141 | II | 241 | III− | 341 | III | 441 | III+ | |
| 142 | III− | 242 | III | 342 | III+ | 442 | IV | |
| 143 | III | 243 | III | 343 | III+ | 443 | IV | |
| 144 | III | 244 | III+ | 344 | IV− | 444 | IV | |
| Conversion from KM grade to Spencer scale | Conversion from KM code (grade) to Spencer grade | |||||||
| KM grade | Spencer grade | |||||||
| 000 | 0 | |||||||
| 111 (I−), 112 (I), 113 (I), 211 (I−), 212 (I), 213 (I+) | I | |||||||
| 212 (I+), 122 (II), 123 (II), 221 (II−), 222 (II), 223 (II+) | II | |||||||
| 232 (III−), 233 (III), 242 (III), 243 (III), 332 (III), 333 (III), 342 (III+), 342 (III+) | III | |||||||
| 444 (IV) | IV | |||||||
| Regions | Groups | Times | ||
|---|---|---|---|---|
| Pre | Post | Rec 30 Min | ||
| Left subclavian vein | NWIG | 0.25 ± 0.44 | 2.90 ± 0.64 | 2.50 ± 0.95 |
| 30WIG | 0.30 ± 0.47 | 1.05 ± 0.68 | 0.75 ± 0.63 | |
| 50WIG | 0.45 ± 0.51 | 1.90 ± 0.85 | 1.60 ± 0.82 | |
| 100WIG | 0.35 ± 0.49 | 2.75 ± 0.78 | 2.60 ± 0.68 | |
| Right subclavian vein | NWIG | 0.35 ± 0.49 | 2.95 ± 0.68 | 2.55 ± 0.94 |
| 30WIG | 0.35 ± 0.49 | 1.15 ± 0.75 | 0.85 ± 0.74 | |
| 50WIG | 0.45 ± 0.51 | 2.12 ± 0.85 | 1.55 ± 0.82 | |
| 100WIG | 0.49 ± 0.51 | 3.10 ± 0.52 | 2.90 ± 0.72 | |
| Precordial region | NWIG | 0.35 ± 0.48 | 2.55 ± 0.99 | 2.20 ± 1.00 |
| 30WIG | 0.35 ± 0.48 | 1.20 ± 0.83 | 0.75 ± 0.91 | |
| 50WIG | 0.45 ± 0.51 | 1.95 ± 0.82 | 1.35 ± 0.93 | |
| 100WIG | 0.48 ± 0.51 | 3.05 ± 0.88 | 2.80 ± 0.83 | |
| Regions | Groups | Times | ||
|---|---|---|---|---|
| Pre | Post | Rec 30 Min | ||
| Left subclavian vein | NWIG | 0.35 ± 0.49 | 2.85 ± 0.81 | 2.45 ± 0.96 |
| 30WIG | 0.30 ± 0.47 | 1.40 ± 0.69 | 1.10 ± 0.71 | |
| 50WIG | 0.50 ± 0.51 | 1.90 ± 0.79 | 1.45 ± 0.68 | |
| 100WIG | 0.40 ± 0.50 | 2.85 ± 0.81 | 2.55 ± 0.98 | |
| Right subclavian vein | NWIG | 0.45 ± 0.51 | 2.75 ± 0.85 | 2.55 ± 0.85 |
| 30WIG | 0.40 ± 0.50 | 1.30 ± 0.73 | 1.00 ± 0.79 | |
| 50WIG | 0.55 ± 0.51 | 2.10 ± 0.78 | 1.85 ± 0.81 | |
| 100WIG | 0.50 ± 0.51 | 3.10 ± 0.85 | 2.90 ± 0.72 | |
| Precordial region | NWIG | 0.45 ± 0.51 | 2.50 ± 0.88 | 2.10 ± 0.91 |
| 30WIG | 0.40 ± 0.50 | 1.20 ± 0.76 | 0.85 ± 0.87 | |
| 50WIG | 0.55 ± 0.51 | 1.90 ± 0.78 | 1.35 ± 0.81 | |
| 100WIG | 0.50 ± 0.51 | 3.11 ± 0.91 | 2.80 ± 0.83 | |
| Regions | Groups | Times | ||
|---|---|---|---|---|
| Pre | Post | Rec 30 Min | ||
| Left subclavian vein | NWIG | 0.30 ± 0.47 | 2.90 ± 0.91 | 2.75 ± 0.82 |
| 30WIG | 0.50 ± 0.51 | 1.36 ± 0.92 | 1.08 ± 0.96 | |
| 50WIG | 0.30 ± 0.47 | 2.10 ± 0.72 | 1.60 ± 0.75 | |
| 100WIG | 0.65 ± 0.48 | 3.00 ± 0.97 | 2.75 ± 1.23 | |
| Right subclavian vein | NWIG | 0.45 ± 0.51 | 2.90 ± 0.85 | 2.60 ± 0.82 |
| 30WIG | 0.45 ± 0.51 | 1.35 ± 0.93 | 0.80 ± 0.87 | |
| 50WIG | 0.45 ± 0.51 | 2.25 ± 0.71 | 1.85 ± 0.78 | |
| 100WIG | 0.50 ± 0.48 | 3.35 ± 0.75 | 3.05 ± 0.60 | |
| Precordial region | NWIG | 0.45 ± 0.51 | 2.80 ± 0.95 | 2.55 ± 0.94 |
| 30WIG | 0.45 ± 0.51 | 1.05 ± 0.99 | 0.75 ± 1.01 | |
| 50WIG | 0.45 ± 0.51 | 1.95 ± 0.75 | 1.45 ± 0.75 | |
| 100WIG | 0.55 ± 0.48 | 3.15 ± 0.93 | 2.75 ± 0.85 | |
| Regions | Groups | Times | ||
|---|---|---|---|---|
| Pre | Post | Rec 30 Min | ||
| Left subclavian vein | NWIG | 2 | 8 | 8 |
| 30WIG | 1 | 4 | 3 | |
| 50WIG | 2 | 7 | 6 | |
| 100WIG | 1 | 8 | 8 | |
| Right subclavian vein | NWIG | 2 | 8 | 7 |
| 30WIG | 2 | 4 | 2 | |
| 50WIG | 2 | 6 | 5 | |
| 100WIG | 1 | 9 | 8 | |
| Precordial region | NWIG | 1.5 | 8 | 8 |
| 30WIG | 1.5 | 3 | 2 | |
| 50WIG | 2 | 8 | 6 | |
| 100WIG | 1 | 9 | 8 | |
| Region | Time | Spencer Grade | Protocols | Fisher’s Exact Test (p Value) | |||
|---|---|---|---|---|---|---|---|
| NWIG | 30WIG | 50WIG | 100WIG | ||||
| Left subclavian vein | Pre | I | 19 (95%) | 19 (95%) | 18 (90%) | 20 (100%) | 2.097 (0.899) |
| II | 1 (5%) | 1 (5%) | 2 (10%) | 0 (0%) | |||
| Post | I | 1 (5%) | 8 (40%) | 0 (0%) | 0 (0%) | 37.774 (<0.001) | |
| II | 4 (20%) | 10 (50%) | 9 (45%) | 3 (15%) | |||
| III | 11 (55%) | 2 (10%) | 10 (50%) | 15 (75%) | |||
| IV | 4 (20%) | 0 (0%) | 1 (5%) | 2 (10%) | |||
| Rec 30 min | I | 1 (5%) | 12 (60%) | 6 (30%) | 0 (0%) | 36.291 (<0.001) | |
| II | 5 (25%) | 7 (35%) | 7 (35%) | 6 (30%) | |||
| III | 13 (65%) | 1 (5%) | 7 (35%) | 14 (70%) | |||
| IV | 1 (5%) | 0 (0%) | 0 (0%) | 0 (0%) | |||
| Right subclavian vein | Pre | I | 19 (95%) | 19 (95%) | 19 (95%) | 20 (100%) | 1.509 (1.000) |
| II | 1 (5%) | 1 (5%) | 1 (5%) | 0 (0%) | |||
| Post | I | 0 (0%) | 6 (30%) | 3 (15%) | 0 (0%) | 46.372 (<0.001) | |
| II | 6 (30%) | 14 (70%) | 9 (45%) | 1 (5%) | |||
| III | 11 (55%) | 0 (0%) | 7 (35%) | 13 (65%) | |||
| IV | 3 (15%) | 0 (0%) | 1 (5%) | 6 (30%) | |||
| Rec 30 min | I | 0 (0%) | 12 (60%) | 6 (30%) | 0 (0%) | 53.476 (<0.001) | |
| II | 8 (40%) | 8 (40%) | 40 (%) | 1 (5%) | |||
| III | 11 (55%) | 0 (0%) | 6 (30%) | 17 (85%) | |||
| IV | 1 (5%) | 0 (0%) | 0 (0%) | 2 (10%) | |||
| Precordial region | Pre | I | 19 (95%) | 19 (95%) | 19 (95%) | 20 (100%) | 1.509 (1.000) |
| II | 1 (5%) | 1 (5%) | 1 (5%) | 0 (0%) | |||
| Post | I | 1 (5%) | 12 (60%) | 0 (0%) | 0 (0%) | 62.542 (<0.001) | |
| II | 1 (5%) | 7 (35%) | 4 (20%) | 0 (0%) | |||
| III | 14 (70%) | 1 (5%) | 16 (80%) | 12 (60%) | |||
| IV | 4 (20%) | 0 (0%) | 0 (0%) | 8 (40%) | |||
| Rec 30 min | I | 1 (5%) | 17 (85%) | 0 (0%) | 0 (0%) | 82.698 (<0.001) | |
| II | 1 (5%) | 3 (15%) | 12 (60%) | 0 (0%) | |||
| III | 14 (70%) | 0 (0%) | 8 (40%) | 16 (80%) | |||
| IV | 4 (20%) | 0 (0%) | 0 (0%) | 4 (20%) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, K.-H.; Hyun, G.-S.; Jee, Y.-S.; Park, J.-M. Effect of Water Amount Intake before Scuba Diving on the Risk of Decompression Sickness. Int. J. Environ. Res. Public Health 2021, 18, 7601. https://doi.org/10.3390/ijerph18147601
Han K-H, Hyun G-S, Jee Y-S, Park J-M. Effect of Water Amount Intake before Scuba Diving on the Risk of Decompression Sickness. International Journal of Environmental Research and Public Health. 2021; 18(14):7601. https://doi.org/10.3390/ijerph18147601
Chicago/Turabian StyleHan, Kil-Hyung, Gwang-Suk Hyun, Yong-Seok Jee, and Jung-Min Park. 2021. "Effect of Water Amount Intake before Scuba Diving on the Risk of Decompression Sickness" International Journal of Environmental Research and Public Health 18, no. 14: 7601. https://doi.org/10.3390/ijerph18147601
APA StyleHan, K.-H., Hyun, G.-S., Jee, Y.-S., & Park, J.-M. (2021). Effect of Water Amount Intake before Scuba Diving on the Risk of Decompression Sickness. International Journal of Environmental Research and Public Health, 18(14), 7601. https://doi.org/10.3390/ijerph18147601