
Effects of Olympic Combat Sports on Older Adults’ Health Status: A Systematic Review


 ,
,  ,
,  ,
, 
 and
and 
Abstract
1. Introduction
2. Methods
2.1. Eligibility Criteria
2.2. Information and Database Search Process
2.3. Studies Selection and Data Collection Process
2.4. Methodological Quality Assessment
2.5. Data Synthesis
2.6. Synthesis Measures for Meta-Analysis
3. Results
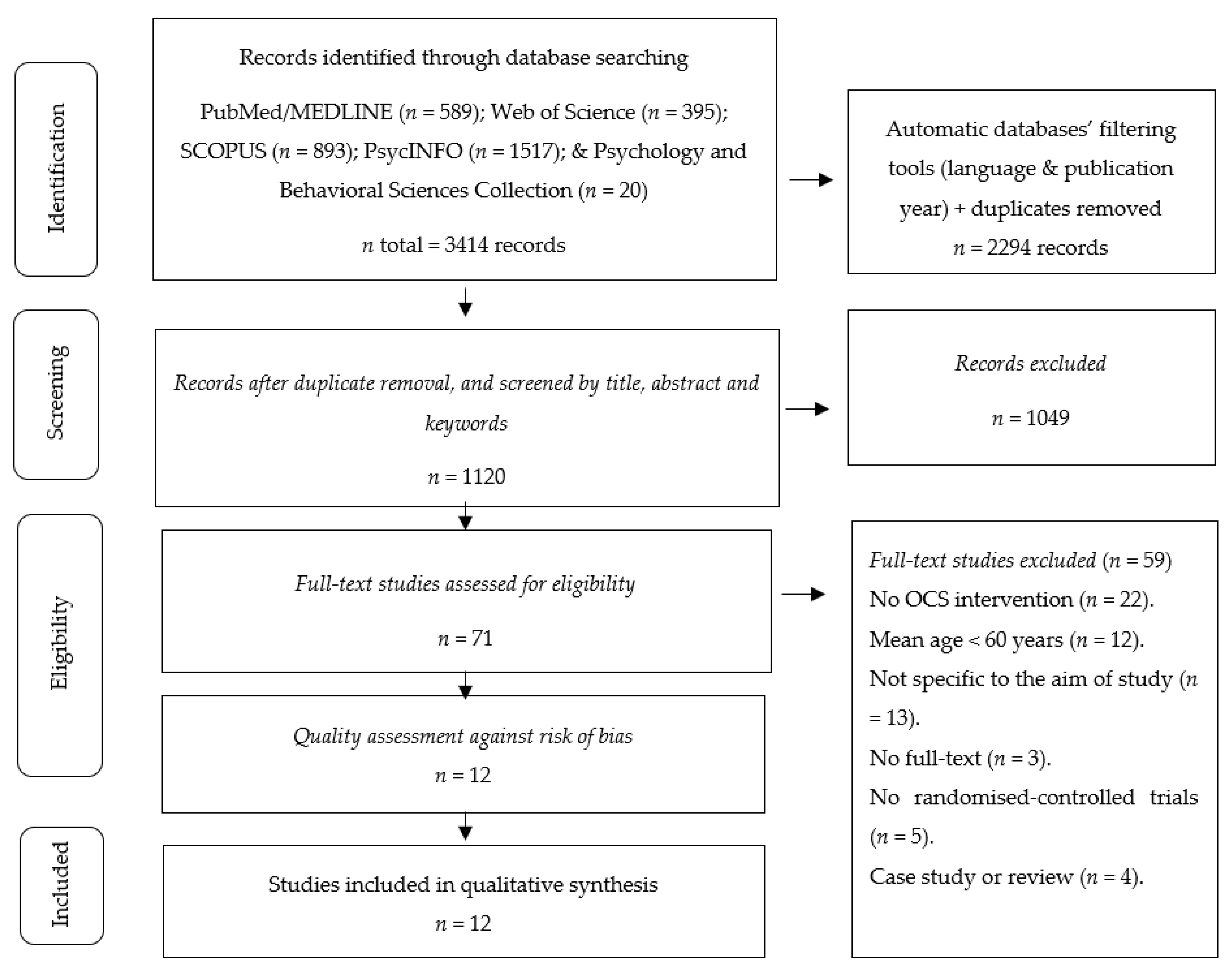
3.1. Studies Selection
3.2. Methodological Quality
3.3. Studies Characteristics
3.4. Sample Characteristics
3.5. Interventions Conducted and Dosing
3.6. Analysed Variables and Data Collection Instruments
3.7. Outcomes
3.7.1. Physical-Functional Outcomes
3.7.2. Physiological Outcomes
3.7.3. Psychoemotional Outcomes
3.8. Adherence and Drop-Out
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yerrakalva, D.; Yerrakalva, D.; Hajna, S.; Griffin, S. Effects of Mobile Health App Interventions on Sedentary Time, Physical Activity, and Fitness in Older Adults: Systematic Review and Meta-Analysis. J. Med. Internet Res. 2019, 21, e14343. [Google Scholar] [CrossRef]
- Chang, Y.-K.; Pan, C.-Y.; Chen, F.-T.; Tsai, C.-L.; Huang, C.-C. Effect of Resistance-Exercise Training on Cognitive Function in Healthy Older Adults: A Review. J. Aging Phys. Act. 2012, 20, 497–517. [Google Scholar] [CrossRef]
- Fragala, M.S.; Cadore, E.L.; Dorgo, S.; Izquierdo, M.; Kraemer, W.J.; Peterson, M.D.; Ryan, E.D. Resistance Training for Older Adults. J. Strength Cond. Res. 2019, 33, 2019–2052. [Google Scholar] [CrossRef] [PubMed]
- Grande, G.H.D.; Oliveira, C.B.; Morelhão, P.K.; Sherrington, C.; Tiedemann, A.; Pinto, R.Z.; Franco, M.R. Interventions Promoting Physical Activity Among Older Adults: A Systematic Review and Meta-Analysis. Gerontologist 2020, 60, e583–e599. [Google Scholar] [CrossRef]
- Zubala, A.; MacGillivray, S.; Frost, H.; Kroll, T.; Skelton, D.A.; Gavine, A.; Gray, N.M.; Toma, M.; Morris, J. Promotion of physical activity interventions for community dwelling older adults: A systematic review of reviews. PLoS ONE 2017, 12, e0180902. [Google Scholar] [CrossRef] [PubMed]
- Valdés-Badilla, P.A.; Gutiérrez-García, C.; Pérez-Gutiérrez, M.; Vargas-Vitoria, R.; López-Fuenzalida, A. Effects of Physical Activity Governmental Programs on Health Status in Independent Older Adults: A Systematic Review. J. Aging Phys. Act. 2019, 27, 265–275. [Google Scholar] [CrossRef] [PubMed]
- He, W.G.; Kowal, P. USS Census Bureau, International Population Reports, P95/16-1, An Aging World: 2015 Washington, DC, USA. Available online: https://www.census.gov/content/dam/Census/library/publications/2016/demo/p95-16-1.pdf (accessed on 15 November 2020).
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.-M.; Nieman, D.C.; Swain, D.P. Quantity and Quality of Exercise for Developing and Maintaining Cardiorespiratory, Musculoskeletal, and Neuromotor Fitness in Apparently Healthy Adults: Guidance for Prescribing Exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef] [PubMed]
- Reis, R.S.; Salvo, D.; Ogilvie, D.; Lambert, E.; Goenka, S.; Brownson, R.C. Scaling up physical activity interventions worldwide: Stepping up to larger and smarter approaches to get people moving. Lancet 2016, 388, 1337–1348. [Google Scholar] [CrossRef]
- Galloza, J.; Castillo, B.; Micheo, W. Benefits of Exercise in the Older Population. Phys. Med. Rehabil. Clin. North Am. 2017, 28, 659–669. [Google Scholar] [CrossRef] [PubMed]
- Witard, O.C.; McGlory, C.; Hamilton, D.; Phillips, S. Growing older with health and vitality: A nexus of physical activity, exercise and nutrition. Biogerontology 2016, 17, 529–546. [Google Scholar] [CrossRef]
- Izquierdo, M.; Casas-Herrero, A.; Zambom-Ferraresi, F.; Martínez-Velilla, N.; Alonso-Bouzón, C.; Rodríguez-Mañas, L. VIVIFRAIL, Multi-Component Physical Exercise Program. VIVIFRAIL. Practical Guide for the Prescription of a Multi-Component Physical Training Program for the Prevention of Frailty and falls in People over 70 Years of Age; Mikel Izquierdo: Navarra, Spain, 2017; (s.l.: Erasmus+ Programme of the European Union). [Google Scholar]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Ramirez-Campillo, R.; Alvarez, C.; Garcìa-Hermoso, A.; Celis-Morales, C.; Ramirez-Velez, R.; Gentil, P.; Izquierdo, M. High-speed resistance training in elderly women: Effects of cluster training sets on functional performance and quality of life. Exp. Gerontol. 2018, 110, 216–222. [Google Scholar] [CrossRef]
- Martínez-Velilla, N.; Casas-Herrero, A.; Zambom-Ferraresi, F.; De Asteasu, M.L.S.; Lucia, A.; Galbete, A.; García-Baztán, A.; Alonso-Renedo, J.; González-Glaría, B.; Gonzalo-Lázaro, M.; et al. Effect of Exercise Intervention on Functional Decline in Very Elderly Patients During Acute Hospitalization. JAMA Intern. Med. 2019, 179, 28–36. [Google Scholar] [CrossRef]
- Gayman, A.M.; Fraser-Thomas, J.; Dionigi, R.A.; Horton, S.; Baker, J. Is sport good for older adults? A systematic review of psychosocial outcomes of older adults’ sport participation. Int. Rev. Sport Exerc. Psychol. 2016, 10, 164–185. [Google Scholar] [CrossRef]
- Herrera-Valenzuela, T.; Chile, U.D.S.D.; Castillo-Fuentes, B.; Cuadra-Aguilar, D.; Zubieta-Planella, B.; Valdés-Badilla, P.; Cofre-Bolados, C.; Del Maule, U.C. Artes marciales y deportes de combate: Una alternativa para mejorar la salud. Hacia la Promoción de la Salud 2019, 24, 11–13. [Google Scholar] [CrossRef]
- Chen, Y.-W.; Hunt, M.A.; Campbell, K.L.; Peill, K.; Reid, W.D. The effect of Tai Chi on four chronic conditions—cancer, osteoarthritis, heart failure and chronic obstructive pulmonary disease: A systematic review and meta-analyses. Br. J. Sports Med. 2015, 50, 397–407. [Google Scholar] [CrossRef] [PubMed]
- Yu, A.P.; Tam, B.T.; Lai, C.W.; Yu, D.S.; Woo, J.; Chung, K.-F.; Hui, S.S.-C.; Liu, J.Y.; Wei, G.X.; Siu, P.M. Revealing the Neural Mechanisms Underlying the Beneficial Effects of Tai Chi: A Neuroimaging Perspective. Am. J. Chin. Med. 2018, 46, 231–259. [Google Scholar] [CrossRef]
- Rios, S.O.; Marks, J.; Estevan, I.; Barnett, L.M. Health benefits of hard martial arts in adults: A systematic review. J. Sports Sci. 2017, 36, 1614–1622. [Google Scholar] [CrossRef]
- Lee, S.; Lee, T. Analysis on the Amount of Physical Activities of Taekwondo Taegeuk Pumsae Using Accelerometers. J. Converg. Inf. Technol. 2010, 5, 48–53. [Google Scholar] [CrossRef]
- Bromley, S.J.; Drew, M.K.; Talpey, S.; McIntosh, A.S.; Finch, C.F. A systematic review of prospective epidemiological research into injury and illness in Olympic combat sport. Br. J. Sports Med. 2018, 52, 8–16. [Google Scholar] [CrossRef]
- Peset Mancebo, M.F.; Ferrer Sapena, A.; Villamón Herrera, M.; González Moreno, L.M.; Toca Herrera, J.-L. Aleixandre Benavent, R. Scientific literature analysis of Judo in Web of Science. Arch Budo. 2013, 9, 81–91. [Google Scholar] [CrossRef]
- Pérez-Gutiérrez, M.; Valdés-Badilla, P.; Gutiérrez-García, C.; Herrera-Valenzuela, T. Taekwondo Scientific Production Published on the Web of Science (1988-2016): Collaboration and Topics. Movimento 2017, 23, 1325–1340. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Smart, N.; Waldron, M.; Ismail, H.; Giallauria, F.; Vigorito, C.; Cornelissen, V.; Dieberg, G. Validation of a new tool for the assessment of study quality and reporting in exercise training studies. Int. J. Evidence-Based Health 2015, 13, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Valentine, J.C.; Pigott, T.D.; Rothstein, H.R. How many studies do you need? A primer on statistical power for meta-analysis. J. Educ. Behav. Stat. 2010, 35, 215–247. [Google Scholar] [CrossRef]
- García-Hermoso, A.; Ramírez-Campillo, R.; Izquierdo, M. Is Muscular Fitness Associated with Future Health Benefits in Children and Adolescents? A Systematic Review and Meta-Analysis of Longitudinal Studies. Sports Med. 2019, 49, 1079–1094. [Google Scholar] [CrossRef] [PubMed]
- Skrede, T.; Steene-Johannessen, J.; Anderssen, S.A.; Resaland, G.K.; Ekelund, U. The prospective association between objectively measured sedentary time, moderate-to-vigorous physical activity and cardiometabolic risk factors in youth: A systematic review and meta-analysis. Obes. Rev. 2018, 20, 55–74. [Google Scholar] [CrossRef] [PubMed]
- Deeks, J.J.; Higgins, J.P.; Altman, D.G. Analysing data and undertaking meta-analyses. In: Higgins JP, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Handb. Syst. Rev. Interv. 2019, 241–284. [Google Scholar] [CrossRef]
- Kontopantelis, E.; Springate, D.A.; Reeves, D. A Re-Analysis of the Cochrane Library Data: The Dangers of Unobserved Heterogeneity in Meta-Analyses. PLoS ONE 2013, 8, e69930. [Google Scholar] [CrossRef]
- Hopkins, W.; Marshall, S.; Batterham, A.; Hanin, J. Progressive Statistics for Studies in Sports Medicine and Exercise Science. Med. Sci. Sports Exerc. 2009, 41, 3. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Duval, S.; Tweedie, R. Trim and Fill: A Simple Funnel-Plot-Based Method of Testing and Adjusting for Publication Bias in Meta-Analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Shi, L.; Lin, L. The trim-and-fill method for publication bias: Practical guidelines and recommendations based on a large database of meta-analyses. Medicine 2019, 98, e15987. [Google Scholar] [CrossRef]
- Cho, S.-Y.; Roh, H.-T. Taekwondo Enhances Cognitive Function as a Result of Increased Neurotrophic Growth Factors in Elderly Women. Int. J. Environ. Res. Public Health 2019, 16, 962. [Google Scholar] [CrossRef]
- Ciaccioni, S.; Capranica, L.; Forte, R.; Chaabene, H.; Pesce, C.; Condello, G. Effects of a Judo Training on Functional Fitness, Anthropometric, and Psychological Variables in Old Novice Practitioners. J. Aging Phys. Act. 2019, 27, 831–842. [Google Scholar] [CrossRef]
- Ciaccioni, S.; Capranica, L.; Forte, R.; Pesce, C.; Condello, G. Effects of a 4-month judo program on gait performance in older adults. J. Sports Med. Phys. Fit. 2020, 60, 685–692. [Google Scholar] [CrossRef]
- Combs, S.A.; Diehl, M.D.; Chrzastowski, C.; Didrick, N.; McCoin, B.; Mox, N.; Staples, W.H.; Wayman, J. Community-based group exercise for persons with Parkinson disease: A randomized controlled trial. NeuroRehabilitation 2013, 32, 117–124. [Google Scholar] [CrossRef]
- Hu, J.-P.; Guo, Y.-H.; Wang, F.; Zhao, X.-P.; Zhang, Q.-H.; Song, Q.-H. Exercise improves cognitive function in aging patients. Int. J. Clin. Exp. Med. 2014, 7, 3144–3149. [Google Scholar]
- Jansen, P.; Dahmen-Zimmer, K. Effects of Cognitive, Motor, and Karate Training on Cognitive Functioning and Emotional Well-Being of Elderly People. Front. Psychol. 2012, 3, 40. [Google Scholar] [CrossRef]
- Jansen, P.; Dahmen-Zimmer, K.; Kudielka, B.M.; Schulz, A. Effects of Karate Training Versus Mindfulness Training on Emotional Well-Being and Cognitive Performance in Later Life. Res. Aging 2017, 39, 1118–1144. [Google Scholar] [CrossRef]
- Lee, S.H.; Scott, S.D.; Pekas, E.J.; Lee, S.; Lee, S.H.; Park, S.Y. Taekwondo training reduces blood catecholamine levels and arterial stiffness in postmenopausal women with stage-2 hypertension: Randomized clinical trial. Clin. Exp. Hypertens. 2018, 41, 675–681. [Google Scholar] [CrossRef]
- Filho, B.J.P.L.; De Oliveira, C.R.; Gottlieb, M.G.V. Effects of karate-dô training in older adults cognition: Randomized controlled trial. Rev. da Educ. Física/UEM 2018, 30, 3030. [Google Scholar] [CrossRef]
- Pliske, G.; Emmermacher, P.; Weinbeer, V.; Witte, K. Changes in dual-task performance after 5 months of karate and fitness training for older adults to enhance fall prevention. Aging Clin. Exp. Res. 2015, 28, 1179–1186. [Google Scholar] [CrossRef]
- Witte, K.; Emmermacher, P.; Pliske, G. Improvement of Balance and General Physical Fitness in Older Adults by Karate: A Randomized Controlled Trial. Complement. Med. Res. 2017, 24, 390–393. [Google Scholar] [CrossRef]
- Witte, K.; Kropf, S.; Darius, S.; Emmermacher, P.; Böckelmann, I. Comparing the effectiveness of karate and fitness training on cognitive functioning in older adults—A randomized controlled trial. J. Sport Health Sci. 2016, 5, 484–490. [Google Scholar] [CrossRef] [PubMed]
- Bu, B.; Haijun, H.; Yong, L.; Chaohui, Z.; Xiaoyuan, Y.; Singh, M.F. Effects of martial arts on health status: A systematic review. J. Evid. Based Med. 2010, 3, 205–219. [Google Scholar] [CrossRef]
- Dunsky, A.; Zach, S.; Zeev, A.; Goldbourt, U.; Shimony, T.; Goldsmith, R.; Netz, Y. Level of physical activity and anthropometric characteristics in old age—results from a national health survey. Eur. Rev. Aging Phys. Act. 2014, 11, 149–157. [Google Scholar] [CrossRef]
- Valdés-Badilla, P.; Guzmán-Muñoz, E.; Ramírez-Campillo, R.; Godoy-Cumillaf, A.; Concha-Cisternas, Y.; Ortega-Spuler, J.; Magnani-Branco, B.H. Changes in anthropometric parameters and physical fitness in older adults after participating in a 16-week physical activity program. Rev. Fac. Med. 2020, 68, 375–382. [Google Scholar] [CrossRef]
- Huang, T.; Larsen, K.T.; Ried-Larsen, M.; Møller, N.C.; Andersen, L.B. The effects of physical activity and exercise on brain-derived neurotrophic factor in healthy humans: A review. Scand. J. Med. Sci. Sports 2013, 24, 1–10. [Google Scholar] [CrossRef]
- Zouhal, H.; Jacob, C.; Delamarche, P.; Gratas-Delamarche, A. Catecholamines and the Effects of Exercise, Training and Gender. Sports Med. 2008, 38, 401–423. [Google Scholar] [CrossRef] [PubMed]
- Kelly, M.E.; Loughrey, D.; Lawlor, B.A.; Robertson, I.H.; Walsh, C.; Brennan, S. The impact of exercise on the cognitive functioning of healthy older adults: A systematic review and meta-analysis. Ageing Res. Rev. 2014, 16, 12–31. [Google Scholar] [CrossRef]
- Zou, L.; Huang, T.; Tsang, T.; Pan, Z.; Wang, C.; Liu, Y.; Wang, H. Hard martial arts for cognitive function across the lifespan: A systematic review. Arch. Budo. 2018, 14, 41–58. Available online: http://files.4medicine.pl (accessed on 30 November 2020).
- Sparling, P.B.; Howard, B.J.; Dunstan, D.; Owen, N. Recommendations for physical activity in older adults. BMJ 2015, 350, h100. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | Elegibility Criteria Specified | Randomly Allocated Participants | Allocation Concealed | Gorups Similar at Baseline | Assessors Blinded | Outcome Measures Assesed >85% of Participants * | Intention to Treat Analysis | Reporting of between Group Statistical Comparisons | Point Measures and Measures of Variability Reported ** | Activity Monitoring in Control Group | Relative Exercise Intensity Reviewed | Exercise Volume and Energy Expended | Overall TESTEX # |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cho & Roh [37] | Yes | Yes | Yes | Yes | Unclear | Yes (2) | Yes | Yes | Yes (1) | No | Yes | Yes | 11/15 |
| Ciaccioni et al. [38] | Yes | Yes | Yes | Yes | Unclear | Yes (3) | Yes | Yes | Yes (2) | No | Yes | Yes | 13/15 |
| Ciaccioni et al. [39] | Yes | Yes | Yes | Yes | Unclear | Yes (3) | Yes | Yes | Yes (2) | Yes | Yes | Yes | 14/15 |
| Combs et al. [40] | Yes | Yes | Yes | Yes | No | Yes (3) | Yes | Yes | Yes (2) | Yes | No | Yes | 13/15 |
| Hu et al. [41] | Yes | Yes | Yes | Yes | No | Yes (3) | Yes | Yes | Yes (1) | Yes | No | Yes | 12/15 |
| Jansen & Dahmen-Zimmer [42] | Yes | Yes | Yes | No | Unclear | Yes (2) | Yes | Yes | Yes (1) | Yes | No | Yes | 10/15 |
| Jansen et al. [43] | Yes | Yes | Yes | Yes | Unclear | Yes (3) | Yes | Yes | Yes (2) | Yes | No | Yes | 13/15 |
| Lee et al. [44] | Yes | Yes | Yes | Yes | Unclear | Yes (2) | Yes | Yes | Yes (1) | Yes | Yes | Yes | 12/15 |
| Pacheco Lopes et al. [45] | Yes | Yes | Yes | Yes | Unclear | Yes (2) | Yes | Yes | Yes (1) | No | No | Yes | 10/15 |
| Pliske et al. [46] | Yes | Yes | Yes | Yes | Unclear | Yes (1) | Yes | Yes | Yes (1) | No | No | Yes | 9/15 |
| Witte et al. [47] | Yes | Yes | Yes | Yes | No | Yes (3) | Yes | Yes | Yes (2) | No | No | Yes | 12/15 |
| Witte et al. [48] | Yes | Yes | Yes | Yes | Unclear | Yes (3) | Yes | Yes | Yes (2) | No | No | Yes | 12/15 |
| Study | Country | Modality of OCS | Sample | Activities Developed in the Intervention | Training Volume | Training Intensity | ||
|---|---|---|---|---|---|---|---|---|
| Total Duration (Weeks) | Frequency (Weekly) | Time Per Session (Min) | ||||||
| Cho & Roh [37] | South Korea | Taekwondo | 37 older women (mean age 68.9 years) | |||||
| Taekwondo group (n = 19) | Stretching, basic taekwondo movement (stance, block, punch, strike, thrust). Poomsae (Taegeuk 1–4 chapter). Kicking (front kick, side kick, roundhouse kick, downward kick). Step (forward, side, backward). Practice mitt kicking. Taekwon gymnastics (2 music-based gymnastics). | 16 | 5 | 60 | Exercise at 50–80% HRmax | |||
| Control group (n = 18) | They were asked to maintain their usual activities. | 16 | NR | NR | NR | |||
| Ciaccioni et al. [38] | Italy | Judo | 40 older adults (age between 64 and 77 years) | |||||
| Judo group (n = 19, 10 men and 9 women) | 10-min judo-specific warm-up (e.g., light activities and gentle routines of judo postures, movements, and techniques performed at slow speed). 30-min judo (e.g., ne-waza—ground technique, tachi-waza—standing techniques, kata—sequences of specific movements, ukemi—judo falling techniques). A 20-min judo cooldown (e.g., judo kata focused on stretching and relaxation). | 16 | 2 | 60 | Moderate to vigorous | |||
| Control group (n = 21, 12 men and 9 women) | They were asked to maintain their usual activities. | 16 | NR | NR | NR | |||
| Ciaccioni et al. [39] | Italy | Judo | 30 older adults (mean age 69.7 years) | |||||
| Judo group (n = 16, 8 men and 8 women) | 10-min judo-specific warm-up (e.g., light routines and dynamic movements of the whole body mimicking the judo techniques). 30-min judo central part (e.g., standing, ground and ukemi breaking-fall techniques, as uchi-komi repetition training in couple and kata sequences of specific movements, individually and in couple). A 20-min cool-down (e.g., stretching and relaxation using judo techniques performed as kata). | 15 | 2 | 60 | Moderate to vigorous | |||
| Control group (n = 14, 9 men and 5 women) | They were asked to maintain their usual activities. | 15 | NR | NR | NR | |||
| Combs et al. [40] | United States of America | Boxing | 31 older adults (mean age 67.3 years) | |||||
| Boxing group (n = 17, 11 men and 6 women) | Boxing-specific activities via a circuit training, as well as general endurance activities. Activities were self-progressed by encouraging participants to train as intensely as they could tolerate and by striving to complete more repetitions during each training bout. Participants wore boxing gloves and hit boxing-specific punching bags, but did not contact other people while boxing. | 12 | 2–3 | 90 | NR | |||
| Traditional exercise group (n = 14, 10 men and 4 women) | Each traditional group exercise session began with a 15-min warm-up period consisting of various seated exercises such as multi-planar axial and extremity active range of motion and stretching. The next hour consisted of strengthening exercises, endurance training, and balance activities. Endurance activities included walking in- or out-doors at a self-selected pace and stair climbing. Static and dynamic standing balance activities were performed on different support surfaces and visual input (eyes open and closed). Ended with a 15 m seated cool-down similar to the warm-up plus breathing exercises for relaxation | 12 | 2–3 | 90 | NR | |||
| Hu et al. [41] | China | Boxing | 198 older adults (mean age 70 years, 145 men and 53 women) | |||||
| Boxing group (n = 96) | The program consisted of jogging for 30 min and shadowboxing for 60 min once a week. | 24 | 1 | 90 | NR | |||
| Control group (n = 102) | NR | 24 | NR | NR | NR | |||
| Jansen & Dahmen-Zimmer [42] | Germany | Karate | 45 older adults (mean age 78.8 years). | |||||
| Karate group (n = 12, 4 men and 8 women). | Training was performed accordingly the guidelines of the German-Karate Federation. Long sequences of arm and leg movements were taught. | 24 | 1 | 60 | NR | |||
| Physical exercise group (n = 12, 5 men and 7 women). | Training included simple exercises for strength, mobilization, stretching, and relaxation. Everyday objects such as towels, chairs, etc., were used as exercise equipment. Each session was preceded by warming-up and ended with cooling-down. | 24 | 1 | 60 | NR | |||
| Cognitive group (n = 12, 5 men and 7 women | The program consists of 121 tasks, 104 inductive thinking tasks (13 generalizations, 15 discrimination, 17 cross-classification, 32 relations, 14 relation differentiation, and 13 system-building tasks), and 17 deductive thinking and concentration tasks. Tasks appear in a specific order to allow the participants to become familiarized with the task. | 24 | 1 | 60 | NR | |||
| Control group (n = 9, 1 men and 8 women). | NR | 24 | NR | NR | NR | |||
| Jansen et al. [43] | Germany | Karate | 54 older adults (mean age 63.5 years). | |||||
| Karate group (n = 23, 6 men and 17 women) | Karate-Do involves Kihon, Kumite, and Kata. Kihon involves performing specific movements with legs or arms and combinations of both, kumite consists of training with a partner, kata is the execution of a variety of tactical fighting exercises. Participants learned simultaneous movements of legs and arms and exercised partner training. | 8 | 2 | 60 | NR | |||
| Mindfulness-based stress reduction (n = 14, 6 men and 8 women) | The MBSR is composed of didactic and practice elements. It incorporates sitting and walking meditation, body scan exercises, and mindfulness communication. Training focuses on the perception of and attention to one’s own body, mental states, and emotions in all these elements. | 8 | 2 | 60 | NR | |||
| Control group (n = 17, 9 men and 8 women) | NR | 8 | NR | NR | NR | |||
| Lee et al. [44] | South Korea | Taekwondo | 20 older women (mean age 70 years) | |||||
| Taekwondo group (n = 10) | Dynamic stretching warm-up for 10 min, then Taekwondo training for 40-min. This consisted of kicks, punches, steps and step-sparring while facing an opponent. They then spent the remaining time practicing Taekwondo forms and then walked, jogged or ran, depending on what intensity was desired. A 10-min, static stretching cool-down. | 12 | 3 | 60 | 30–40% HRmax (4-w). 40–50% HRmax (4-w). 50–60% HRmax (4-w). | |||
| Control group (n = 10) | They were asked to maintain their usual activities. | 12 | 3 | 60 | NR | |||
| Pacheco Lopes et al. [45] | Brazil | Karate | 33 older adults (mean age 68.7 years) | |||||
| Karate group (n = 16, 1 men and 15 women) | Training session consisted of brief warmup (5–10 min); Kihon exercises, kata (sequences of Karate-Do movements), kumite and breathing techniques (40–45 min) and relaxation through brief meditation exercises tailored to the needs of the participants (10 min). | 12 | 2 | 60 | NR | |||
| Control group (n = 17, 1 men and 16 women). | They were asked to maintain their usual activities. | 12 | NR | NR | NR | |||
| Pliske et al. [46] | Germany | Karate | 68 older adults (mean age 69 years, 29 men and 39 women). | |||||
| Karate group (n = 25) | Training session consisted of basic techniques and katas. Kumite and self-defence were no components of the training. The training were adapted to the subjects’ age. | 20 | 2 | 60 | NR | |||
| Fitness group (n = 24) | Specific exercises for balance, strength and coordination as well as simple team sports and games were practiced. The individual exercises, except for sports games, had a non-competitive character. | 20 | 2 | 60 | NR | |||
| Control group (n = 19) | They were asked to maintain their usual activities. | 20 | NR | NR | NR | |||
| Witte et al. [47] | Germany | Karate | 90 older adults (mean age 69.3 years, 35 men and 55 women). | |||||
| Karate group (n = 30) | The training was as follows: several stances (forward stance, back stance, and straddle-leg stance), several arm techniques during standing, and forward and backward stances (downward block, lunge punch, reverse punch), and upper blocks. Furthermore, the participants learned simple attacks and defense exercises with their partners and a simple kata. | 20 | 2 | 60 | NR | |||
| Fitness group (n = 30) | The fitness training included elements of gymnastics, running exercises, practices with a ball and other hand devices, and strengthening exercises. | 20 | 2 | 60 | NR | |||
| Control group (n = 30) | They were asked to maintain their usual activities. | 20 | NR | NR | NR | |||
| Witte et al. [48] | Germany | Karate | 89 older adults (mean age 70 years, 36 men and 53 women) | |||||
| Karate group (n = 30) | They included stances such as forward stances, back stances, and straddle-leg stances to train leg and trunk musculature and balance skills; also included were several arm techniques in standing positions and forward and backward walking (downward-block), lunge punches, reverse punches, and upper blocks to improve arm–leg coordination, and a special karate form | 20 | 2 | 60 | NR | |||
| Fitness group (n = 30) | The training unit contained elements of gymnastics, running exercises, practices with balls and other hand devices, age-related games and strengthening exercises. | 20 | 2 | 60 | NR | |||
| Control group (n = 29) | They were asked to maintain their usual activities. | 20 | NR | NR | NR | |||
| Study | Analysed Variables | Data Collection Instruments | Main Outcomes |
|---|---|---|---|
| Cho & Roh [37] | Physical-functional level Muscle strength (lower body). Muscle strength (upper body). Flexibility (lower body). Flexibility (upper body). Endurance fitness. Agility and dynamic balance. | Chair stand test Arm curl test Chair sit-and-reach test Back scratch test 2-min step test Timed Up-and-go test | There significant increases (p < 0.05) in chair stand test, chair sit-&-reach test, 2-min step test, in the level of BDNF, VEGF, and IGF-1, and the Color-Word component score in the taekwondo group, without reporting changes in the rest of the variables. Furthermore, there were no significant changes in any of the variables in the control group, nor were there differences between the groups. |
| Physiological level Serum levels of neurotrophic growth factors (BDNF, VEGF, IGF-1; systolic, diastolic, and mean blood flow velocity and pulsatility index of the middle cerebral artery). | ELISA kit | ||
| Psychoemotional level Cognitive functions | MMSE-DS. Stroop colour and word test | ||
| Ciaccioni et al. [38] | Physical-functional level Anthropometric measurements Body weight. Height. Body mass index. Wrist circumference. Hip circumference. | Digital scale Stadiometer kg/m2 Measuring tape (cm) Measuring tape (cm) | The judo group showed reductions of waist circumference (Δ = −1%, d = 0.2) and improvements for lower and upper body flexibility (Δ = +69%, d = 0.4 and Δ = +126%, d = 0.5, respectively) and strength (Δ = +12%, d = 0.6 and Δ = +31%, d = 1.6, respectively). The control group showed a decline in lower body strength (Δ = −12%, d = 0.8). Psychological variables did not reveal significant effects. |
| Physical-functional measurements Grip strength. Muscle strength (lower body). Muscle strength (upper body). Flexibility (lower body). Flexibility (upper body). Inter-limb coordination. Low risk of falls. | Handgrip dynamometer Chair stand test Arm curl test Chair sit-and-reach test Back scratch test Digital metronome Berg balance scale | ||
| Psychoemotional level Body image perception. Quality of life perception. Fear of falling. | Body image dimensional assessment SF-12v2 FES-I | ||
| Ciaccioni et al. [39] | Physical-functional level Gait stability (flat and hurdling conditions: gait cycle, speed, and cadence). | 10-m Optojump photocell system | A significant Time × Motor complexity × Group interaction was found for mean values and coefficients of variation. For mean values, Judo group showed improvements for flat and hurdling conditions in step length (flat: ∆ = +2.6%, d = 0.4; hurdling: ∆ = +3.2%, d = 0.4), gait cycle (flat: ∆ = −4.3%, d = 0.4; hurdling: ∆ = −4.0%, d = 0.5), speed (flat: ∆ = +6.6%, d = 0.7; hurdling: ∆ = +6.7%, d = 0.6) and cadence (flat: ∆ = 4.3%, d = 0.4; hurdling: ∆ = 3.9%, d = 0.5). For coefficients of variation, Judo group improved step length for flat (∆ = −20.9%, d = 0.6) and hurdling (∆ = −16.3%, d = 0.8) conditions, whereas control group showed a deterioration in the step length for the corridor condition (∆ = +22.3%, d = 0.7). |
| Combs et al. [40] | Physical-functional level Low risk of falls. Agility and dynamic balance. Agility and dynamic balance. Gait velocity. Endurance fitness. Activities-specific balance. | Berg balance scale Timed up-and-go test Dual-task timed up-and-go test Gait velocity 6-min Walk test ABC | The traditional exercise group demonstrated significantly greater gains in balance confidence than the boxing group (p < 0.025). Only the boxing group demonstrated significant improvements in gait velocity and endurance over time with a medium between-group effect size for the gait endurance (d = 0.65). Both groups demonstrated significant improvements with balance, mobility, and quality of life with large within-group effect sizes (d ≥ 0.80). |
| Psychoemotional level Quality of life perception. | PDQL | ||
| Hu et al. [41] | Physical-functional level Activity of Daily Living. Body movement testing. | AVD scale DDX-200 computer multifunction tester | Compared with control group, patients who exercised showed improved cognitive function in immediate memory (p < 0.001) and delayed recall (p = 0.004) function. In addition, activities associated with daily living showed improvement (p < 0.001), as did body movement (p < 0.05), arm stability (p < 0.001), and the appearance of rotation (p < 0.05). |
| Psychoemotional level Cognitive function. | Chinese MMSE | ||
| Jansen & Dahmen-Zimmer [42] | Psychoemotional level Cognitive speed. Memory performance. | ZVT and ZS Digit-span test. Figure test. Block-tapping test | No significant difference in cognitive improvement dependent on group between the three training conditions. However, a significant improvement was found in the emotional mental state measurement for the Karate group compared to the waiting control group. |
| Emotional mental state and depressive pathology. | CES-D | ||
| Jansen et al. [43] | Physiological level Perceived stress. Chronic stress. | TICS Hair cortisol concentration | Significant improvement (p < 0.05) for the karate group, but not the mindfulness-based stress reduction and control group, in subjective mental health and anxiety as well as cognitive processing speed. The mindfulness-based stress reduction group showed by trend as a decrease in stress. No significant correlation between pre assessment hair cortisol and post-assessment outcomes could be established. However, the higher the level of baseline self-reported perceived stress, the higher the increase in depression, anxiety, and chronic stress. |
| Psychoemotional level Psychological measurements Emotional well-being. Anxiety and depression. Optimism and pessimism. Quality of life perception. | MDBF HADS LOT-R SF-12 | ||
| Cognitive measurements Mental rotation. Cognitive speed. Inhibition and Memory performance | The mental rotation test ZVT Stroop colour and word test. Digit-span test | ||
| Lee et al. [44] | Physical-functional level Muscle strength (lower body). Grip strength. | 1RM a leg extension machine Handgrip dynamometer | There were significant (p < 0.05) group by time interactions for resting epinephrine and Norepinephrine levels, with resting epinephrine decreasing in the taekwondo training group and norepinephrine increasing in the control group. Additionally, brachial-ankle pulse wave velocity, resting heart rate, and blood pressure were significantly decreased, while handgrip and leg strength were significantly increased in the taekwondo training group compared to the control group. |
| Physiological level Blood catecholamine levels of epinephrine and norepinephrine. | ELISA kit | ||
| Brachial-ankle pulse wave velocity. | Non-invasive arterial tonometry with SphygmoCor | ||
| Pacheco Lopes et al. [45] | Physical-functional level Motor sequencing capacity through hand movements. | Motor Task Sequence | Karate group shows significantly (p < 0.05) better results than the control group in visual memory tasks, executive functions, and memory complaints in post-intervention analysis. |
| Psychoemotional level Cognitive functions. Divided attention and visual processing speed. Concentrated attention and memory performance. Visual perception, and memory. Episodic verbal memory and recognition. Object-centered attention and visuospatial memory. | MMSE Trail making test Digit Span test Rey-Osterrieth complex figure Rey Auditory-Verbal Learning Test Visual Memory Span test Wisconsin Card Sorting Test. Verbal Fluency | ||
| Executive functioning, cognitive flexibility, lexical production and semantic memory. Depressive symptoms. The intensity of anxiety. Subjective complaints of memory. | Geriatric depression scale Beck Anxiety Inventory APT-II Attention Questionnaire PRMQ | ||
| Difficulties in prospective and retrospective memory. Complaints of memory problems. Subjective assessment of executive functions | Memory Complaint Questionnaire Dysexecutive Questionnaire | ||
| Pliske et al. [46] | Physical-functional level Normal walk. Motor dual task. | kinematic system for motion analysis | It could be seen that all groups significantly improved (p < 0.05) their gait parameters after a 5-month period, even the control group. A sporty intervention seems to affect mainly the temporal gait parameters positively. This effect was especially demonstrated for a normal walk and dual cognitive task. |
| Psychoemotional level Cognitive dual task. | kinematic system for motion analysis | ||
| Witte et al. [47] | Physical-functional level Muscle strength (lower body). Walk. Static and dynamic balance. | Chair stand test Walking speed Balance ability | Significant improvements (p < 0.01) in performance in the chair stand test were found in the three groups, but in the karate group it has a greater effect. The karate group and control group show significant improvements in walking speed (p < 0.05), but the improvement in the karate group is greater (p < 0.01). Significant changes (p < 0.05) in balance ability were found in the karate group and the control group. |
| Witte et al. [48] | Physical-functional level Motor reaction. | The rod test | Significant improvement (p < 0.10) in motor reactivity, stress tolerance, and divided attention only after the 5-month karate training period. Additionally, the results of the secondary study indicate further improvements after 10 months. |
| Psychoemotional level Cognitive performance. Reactive stress tolerance. Divided attention. | The DemTect test Determination Test Version S11 Test of Divided Attention |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valdés-Badilla, P.; Herrera-Valenzuela, T.; Ramirez-Campillo, R.; Aedo-Muñoz, E.; Báez-San Martín, E.; Ojeda-Aravena, A.; Branco, B.H.M. Effects of Olympic Combat Sports on Older Adults’ Health Status: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 7381. https://doi.org/10.3390/ijerph18147381
Valdés-Badilla P, Herrera-Valenzuela T, Ramirez-Campillo R, Aedo-Muñoz E, Báez-San Martín E, Ojeda-Aravena A, Branco BHM. Effects of Olympic Combat Sports on Older Adults’ Health Status: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(14):7381. https://doi.org/10.3390/ijerph18147381
Chicago/Turabian StyleValdés-Badilla, Pablo, Tomás Herrera-Valenzuela, Rodrigo Ramirez-Campillo, Esteban Aedo-Muñoz, Eduardo Báez-San Martín, Alex Ojeda-Aravena, and Braulio Henrique Magnani Branco. 2021. "Effects of Olympic Combat Sports on Older Adults’ Health Status: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 14: 7381. https://doi.org/10.3390/ijerph18147381
APA StyleValdés-Badilla, P., Herrera-Valenzuela, T., Ramirez-Campillo, R., Aedo-Muñoz, E., Báez-San Martín, E., Ojeda-Aravena, A., & Branco, B. H. M. (2021). Effects of Olympic Combat Sports on Older Adults’ Health Status: A Systematic Review. International Journal of Environmental Research and Public Health, 18(14), 7381. https://doi.org/10.3390/ijerph18147381