
Association of Food Intake Quality with Vitamin D in SARS-CoV-2 Positive Patients from Mexico: A Cross-Sectional Study

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Settings and Participants
2.2. Measurements and Data Collection
2.3. Statistical Analysis
3. Results
3.1. Clinical Features of SARS-CoV-2 Positive Patients
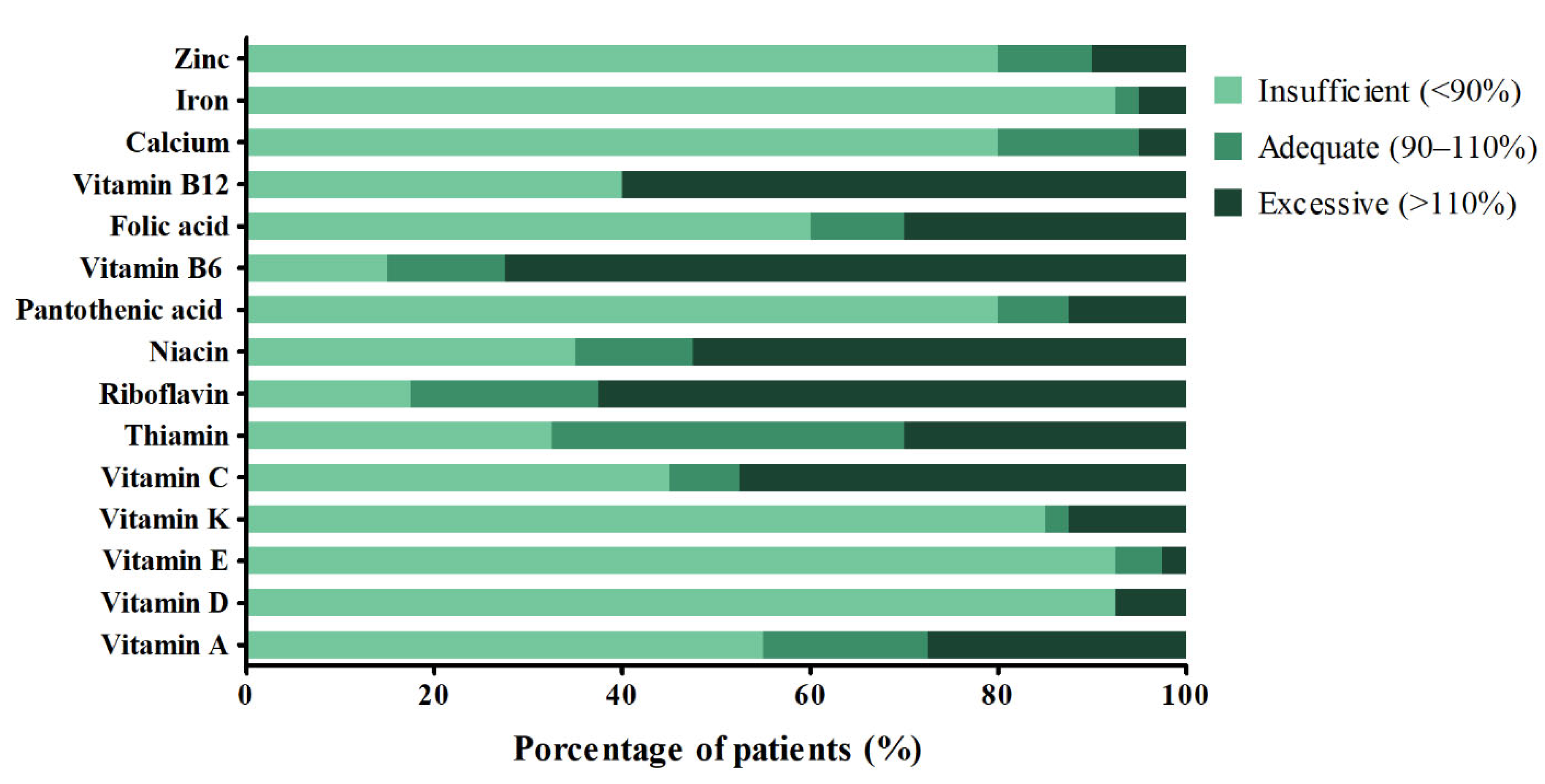
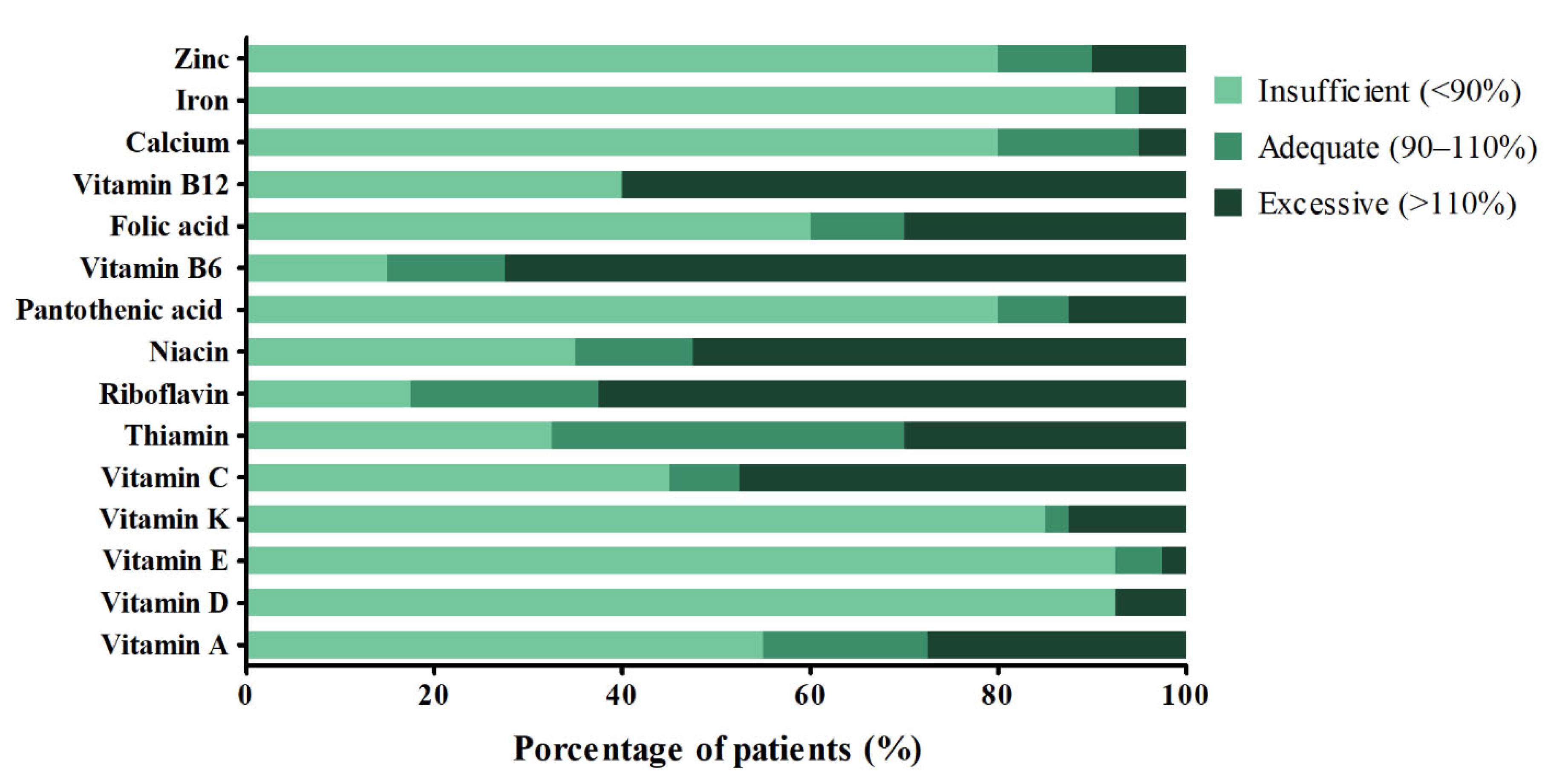
3.2. Dietary Micronutrient Intake of SARS-CoV-2 Positive Patients
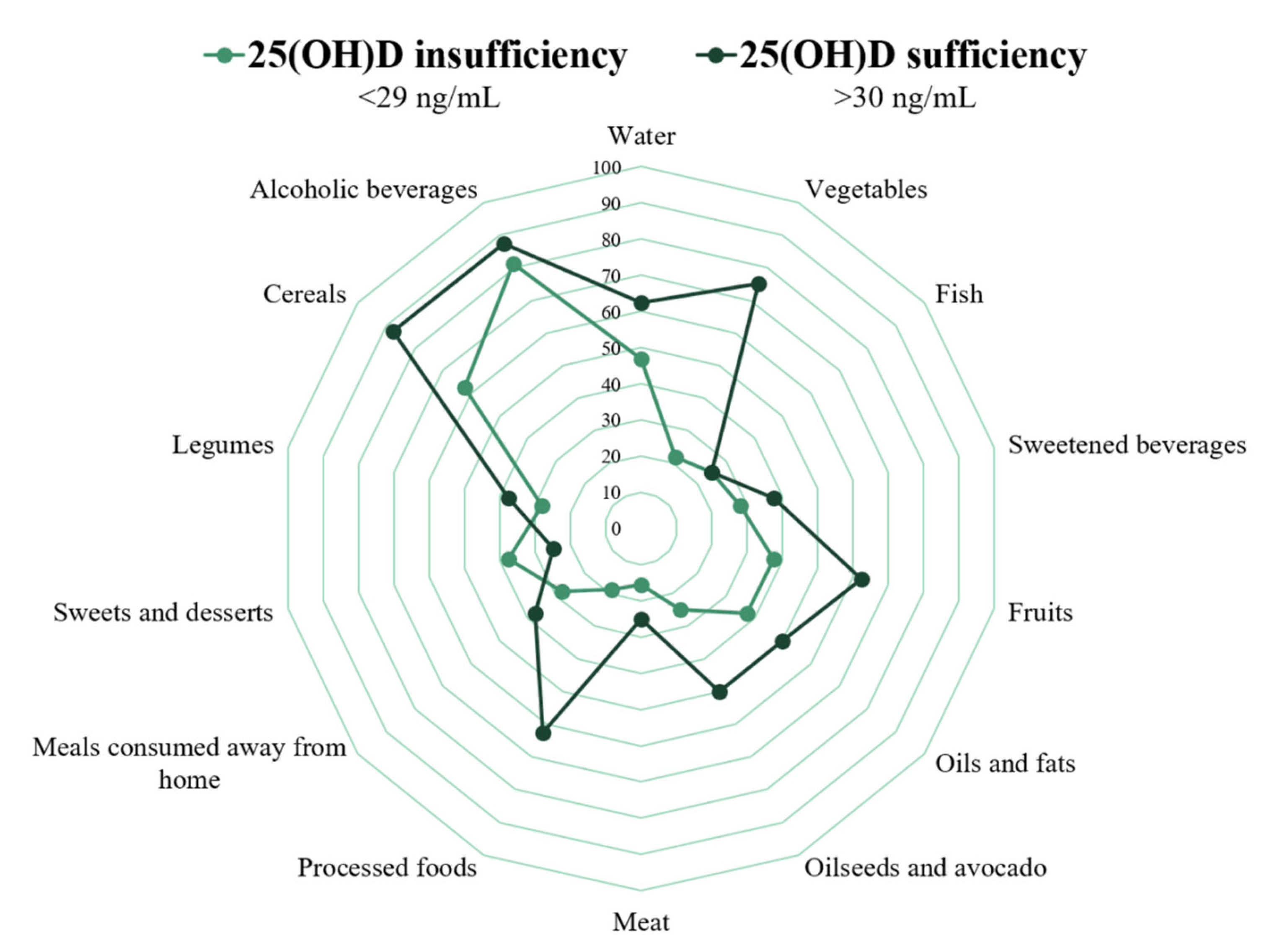
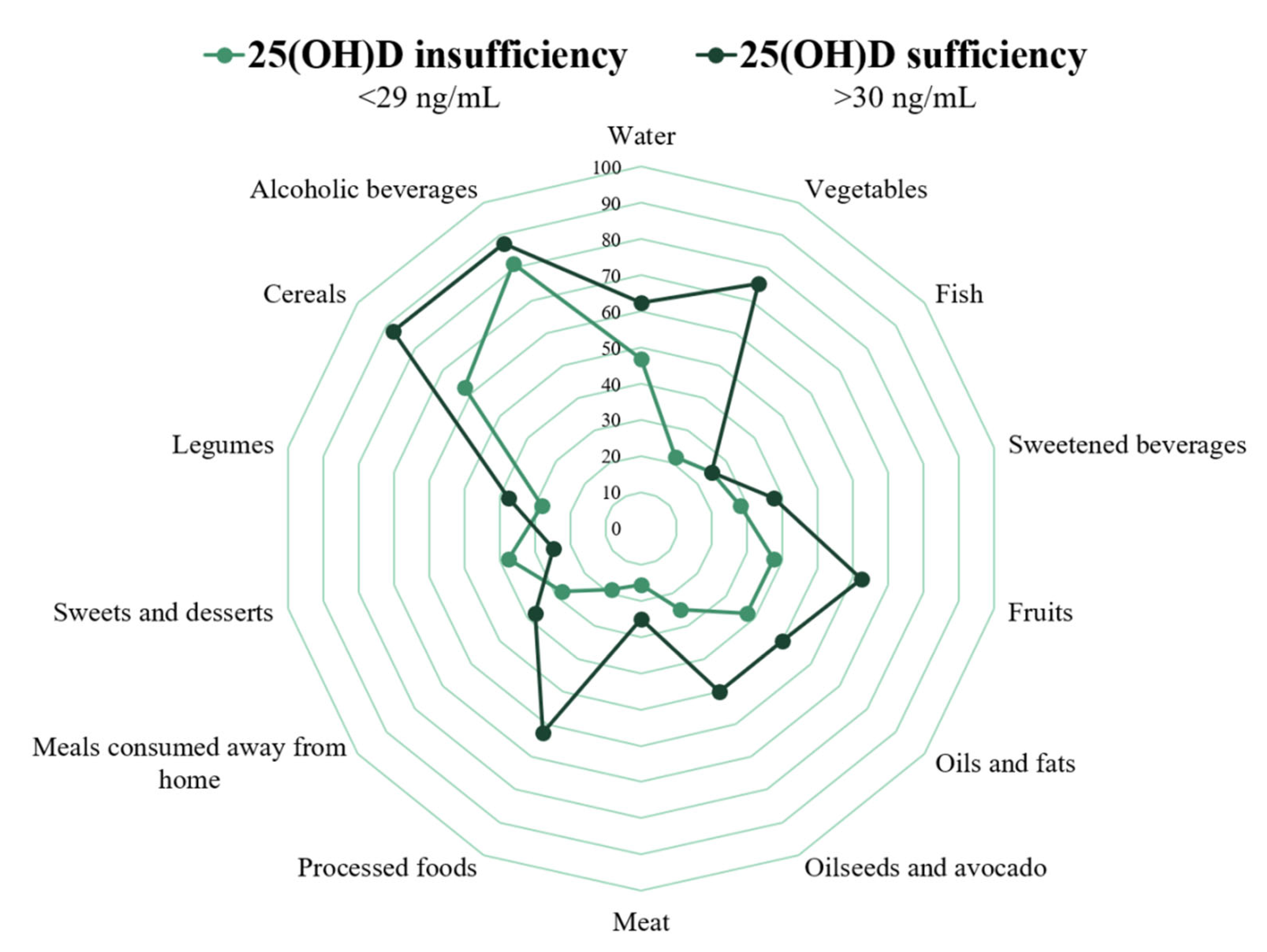
3.3. Comparison of Clinical Features and Food Intake Quality of SARS-CoV-2 Positive Patients with 25(OH)D Insufficiency and Sufficiency
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, H.; Li, X.; Li, T.; Zhang, S.; Wang, L.; Wu, X.; Liu, J. The Genetic Sequence, Origin, and Diagnosis of SARS-CoV-2. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 1629–1635. [Google Scholar] [CrossRef]
- Johns Hopkins University COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). Available online: https://coronavirus.jhu.edu/map.html (accessed on 31 May 2021).
- De Lusignan, S.; Dorward, J.; Correa, A.; Jones, N.; Akinyemi, O.; Amirthalingam, G.; Andrews, N.; Byford, R.; Dabrera, G.; Elliot, A.; et al. Risk Factors for SARS-CoV-2 among Patients in the Oxford Royal College of General Practitioners Research and Surveillance Centre Primary Care Network: A Cross-Sectional Study. Lancet Infect. Dis. 2020, 20, 1034–1042. [Google Scholar] [CrossRef]
- Zheng, Z.; Peng, F.; Xu, B.; Zhao, J.; Liu, H.; Peng, J.; Li, Q.; Jiang, C.; Zhou, Y.; Liu, S.; et al. Risk Factors of Critical & Mortal COVID-19 Cases: A Systematic Literature Review and Meta-Analysis. J. Infect. 2020, 81, e16–e25. [Google Scholar] [CrossRef]
- De Faria Coelho-Ravagnani, C.; Corgosinho, F.C.; Sanches, F.L.F.Z.; Prado, C.M.M.; Laviano, A.; Mota, J.F. Dietary Recommendations during the COVID-19 Pandemic. Nutr. Rev. 2021, 79, 382–393. [Google Scholar] [CrossRef]
- Calder, P.C.; Carr, A.C.; Gombart, A.F.; Eggersdorfer, M. Optimal Nutritional Status for a Well-Functioning Immune System Is an Important Factor to Protect against Viral Infections. Nutrients 2020, 12, 1181. [Google Scholar] [CrossRef] [Green Version]
- Liu, N.; Sun, J.; Wang, X.; Zhang, T.; Zhao, M.; Li, H. Low Vitamin D Status Is Associated with Coronavirus Disease 2019 Outcomes: A Systematic Review and Meta-Analysis. Int. J. Infect. Dis. 2021. [Google Scholar] [CrossRef]
- Pereira, M.; Dantas Damascena, A.; Galvão Azevedo, L.M.; de Almeida Oliveira, T.; da Mota Santana, J. Vitamin D Deficiency Aggravates COVID-19: Systematic Review and Meta-Analysis. Crit. Rev. Food Sci. Nutr. 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Turrubiates-Hernández, F.; Sánchez-Zuno, G.; González-Estevez, G.; Hernández-Bello, J.; Macedo-Ojeda, G.; Muñoz-Valle, J. Potential Immunomodulatory Effects of Vitamin D in the Prevention of Severe Coronavirus Disease 2019: An Ally for Latin America (Review). Int. J. Mol. Med. 2021, 47. [Google Scholar] [CrossRef] [PubMed]
- Nair, R.; Maseeh, A. Vitamin D: The “Sunshine” Vitamin. J. Pharmacol. Pharmacother. 2012, 3, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D Deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef]
- Ramírez-Silva, I.; Rodríguez-Ramírez, S.; Barragán-Vázquez, S.; Castellanos-Gutiérrez, A.; Reyes-García, A.; Martínez-Piña, A.; Pedroza-Tobías, A. Prevalence of Inadequate Intake of Vitamins and Minerals in the Mexican Population Correcting by Nutrient Retention Factors, Ensanut 2016. Salud Publica Mex. 2020, 62, 521–531. [Google Scholar] [CrossRef]
- Bracale, R.; Vaccaro, C.M. Changes in Food Choice Following Restrictive Measures Due to Covid-19. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 1423–1426. [Google Scholar] [CrossRef]
- Deschasaux-Tanguy, M.; Druesne-Pecollo, N.; Esseddik, Y.; de Edelenyi, F.S.; Allès, B.; Andreeva, V.A.; Baudry, J.; Charreire, H.; Deschamps, V.; Egnell, M.; et al. Diet and Physical Activity during the Coronavirus Disease 2019 (COVID-19) Lockdown (March-May 2020): Results from the French NutriNet-Santé Cohort Study. Am. J. Clin. Nutr. 2021, 113, 924–938. [Google Scholar] [CrossRef]
- Cicero, A.F.G.; Fogacci, F.; Giovannini, M.; Mezzadri, M.; Grandi, E.; Borghi, C.; Group, T.B.H.S. COVID-19-Related Quarantine Effect on Dietary Habits in a Northern Italian Rural Population: Data from the Brisighella Heart Study. Nutrients 2021, 13, 309. [Google Scholar] [CrossRef]
- Macedo-Ojeda, G.; Muñoz-Valle, J.; Yokogawa-Teraoka, P.; Machado-Sulbarán, A.; Loza-Rojas, M.; Arredondo, A.G.; Tejeda-Constantini, R.; Vega-Magaña, A.; González-Estevez, G.; García-Chagollán, M.; et al. COVID-19 Screening By Anti-SARS-CoV-2 Antibody Seropositivity: Clinical and Epidemiological Characteristics, Comorbidities, and Food Intake Quality. ResearchSquare: Rs-154551/v1 [Preprint]. Available online: https://www.researchsquare.com/article/rs-154551/v1 (accessed on 26 March 2021).
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, Treatment, and Prevention of Vitamin D Deficiency: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ward, W.; Lambreton, F.; Goel, N.; Yu, J.; Farma, J. Clinical Presentation and Staging of Melanoma. In Cutaneous Melanoma: Etiology and Therapy; Ward, W.H., Farma, J.M., Eds.; TABLE 1, Fitzpatrick Classification of Skin Types I through VI. Available online: https://www.ncbi.nlm.nih.gov/books/NBK481857/table/chapter6.t1/doi:10.15586/codon.cutaneousmelanoma.2017.ch6 (accessed on 2 March 2021).
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- Weir, C.; Jan, A. BMI Classification Percentile and Cut off Points. Available online: https://www.ncbi.nlm.nih.gov/books/NBK541070/ (accessed on 2 March 2021).
- Ramírez-Silva, I.; Barragán-Vázquez, S.; Rodríguez-Ramírez, S.C.; Rivera-Dommarco, J.A.; Mejía-Rodríguez, F.; Barquera-Cervera, S.; Tolentino-Mayo, L.; Flores-Aldana, M.; Villalpando-Hernández, S.; Ancira-Moreno, M.; et al. Base de Alimentos de México (BAM): Compilación de La Composición de Los Alimentos Frecuentemente Consumidos En El País. Versión 18.1.1. 2019. Available online: http://kin.insp.mx/aplicaciones/Redpidieta (accessed on 1 April 2021).
- Bernal-Orozco, M.F.; Salmeron-Curiel, P.B.; Prado-Arriaga, R.J.; Orozco-Gutiérrez, J.F.; Badillo-Camacho, N.; Márquez-Sandoval, F.; Altamirano-Martínez, M.B.; González-Gómez, M.; Gutiérrez-González, P.; Vizmanos, B.; et al. Second Version of a Mini-Survey to Evaluate Food Intake Quality (Mini-ECCA v.2): Reproducibility and Ability to Identify Dietary Patterns in University Students. Nutrients 2020, 12, 809. [Google Scholar] [CrossRef] [Green Version]
- Haua-Navarro, K. Alimentación: Estrategias de evaluación. In El ABCD de la Evaluación del Estado de Nutrición; McGraw-Hill: Ciudad de México, Mexico, 2010; pp. 225–252. [Google Scholar]
- Meza-Meza, M.R.; Vizmanos-Lamotte, B.; Muñoz-Valle, J.F.; Parra-Rojas, I.; Garaulet, M.; Campos-López, B.; Montoya-Buelna, M.; Cerpa-Cruz, S.; Martínez-López, E.; Oregon-Romero, E.; et al. Relationship of Excess Weight with Clinical Activity and Dietary Intake Deficiencies in Systemic Lupus Erythematosus Patients. Nutrients 2019, 11, 2683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernández, J.L.; Nan, D.; Fernandez-Ayala, M.; García-Unzueta, M.; Hernández-Hernández, M.A.; López-Hoyos, M.; Muñoz-Cacho, P.; Olmos, J.M.; Gutiérrez-Cuadra, M.; Ruiz-Cubillán, J.J.; et al. Vitamin D Status in Hospitalized Patients with SARS-CoV-2 Infection. J. Clin. Endocrinol. Metab. 2021, 106, e1343–e1353. [Google Scholar] [CrossRef] [PubMed]
- Hutchings, N.; Babalyan, V.; Baghdasaryan, S.; Qefoyan, M.; Sargsyants, N.; Aghajanova, E.; Martirosyan, A.; Harutyunyan, R.; Lesnyak, O.; Formenti, A.M.; et al. Patients Hospitalized with COVID-19 Have Low Levels of 25-Hydroxyvitamin D. Endocrine 2021, 71, 267–269. [Google Scholar] [CrossRef] [PubMed]
- Carpagnano, G.E.; Di Lecce, V.; Quaranta, V.N.; Zito, A.; Buonamico, E.; Capozza, E.; Palumbo, A.; Di Gioia, G.; Valerio, V.N.; Resta, O. Vitamin D Deficiency as a Predictor of Poor Prognosis in Patients with Acute Respiratory Failure Due to COVID-19. J. Endocrinol. Investig. 2021, 44, 765–771. [Google Scholar] [CrossRef]
- De Smet, D.; De Smet, K.; Herroelen, P.; Gryspeerdt, S.; Martens, G.A. Serum 25(OH)D Level on Hospital Admission Associated With COVID-19 Stage and Mortality. Am. J. Clin. Pathol. 2021, 155, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Mardani, R.; Alamdary, A.; Mousavi Nasab, S.D.; Gholami, R.; Ahmadi, N.; Gholami, A. Association of Vitamin D with the Modulation of the Disease Severity in COVID-19. Virus Res. 2020, 289, 198148. [Google Scholar] [CrossRef] [PubMed]
- Ye, K.; Tang, F.; Liao, X.; Shaw, B.A.; Deng, M.; Huang, G.; Qin, Z.; Peng, X.; Xiao, H.; Chen, C.; et al. Does Serum Vitamin D Level Affect COVID-19 Infection and Its Severity?-A Case-Control Study. J. Am. Coll. Nutr. 2020, 1–8. [Google Scholar] [CrossRef]
- Bogataj Jontez, N.; Novak, K.; Kenig, S.; Petelin, A.; Jenko Pražnikar, Z.; Mohorko, N. The Impact of COVID-19-Related Lockdown on Diet and Serum Markers in Healthy Adults. Nutrients 2021, 13, 1082. [Google Scholar] [CrossRef]
- Dimakopoulos, I.; Magriplis, E.; Mitsopoulou, A.-V.; Karageorgou, D.; Bakogianni, I.; Micha, R.; Michas, G.; Chourdakis, M.; Chrousos, G.P.; Roma, E.; et al. Intake and Contribution of Food Groups to Vitamin D Intake in a Representative Sample of Adult Greek Population. Nutrition 2020, 72, 110641. [Google Scholar] [CrossRef] [PubMed]
- Yoo, K.; Cho, J.; Ly, S. Vitamin D Intake and Serum 25-Hydroxyvitamin D Levels in Korean Adults: Analysis of the 2009 Korea National Health and Nutrition Examination Survey (KNHANES IV-3) Using a Newly Established Vitamin D Database. Nutrients 2016, 8, 610. [Google Scholar] [CrossRef] [Green Version]
- Jones, K.S.; Assar, S.; Harnpanich, D.; Bouillon, R.; Lambrechts, D.; Prentice, A.; Schoenmakers, I. 25(OH)D2 Half-Life Is Shorter than 25(OH)D3 Half-Life and Is Influenced by DBP Concentration and Genotype. J. Clin. Endocrinol. Metab. 2014, 99, 3373–3381. [Google Scholar] [CrossRef] [Green Version]
- Tønnesen, R.; Hovind, P.H.; Jensen, L.T.; Schwarz, P. Determinants of Vitamin D Status in Young Adults: Influence of Lifestyle, Sociodemographic and Anthropometric Factors. BMC Public Health 2016, 16, 385. [Google Scholar] [CrossRef] [Green Version]
- Manios, Y.; Moschonis, G.; Lambrinou, C.P.; Mavrogianni, C.; Tsirigoti, L.; Hoeller, U.; Roos, F.F.; Bendik, I.; Eggersdorfer, M.; Celis-Morales, C.; et al. Associations of Vitamin D Status with Dietary Intakes and Physical Activity Levels among Adults from Seven European Countries: The Food4Me Study. Eur. J. Nutr. 2018, 57, 1357–1368. [Google Scholar] [CrossRef] [Green Version]
- Fernandes, M.R.; Barreto, W.D.R.J. Association between Physical Activity and Vitamin D: A Narrative Literature Review. Rev. Assoc. Med. Bras. 2017, 63, 550–556. [Google Scholar] [CrossRef] [Green Version]
- Valtueña, J.; Dominguez, D.; Til, L.; González-Gross, M.; Drobnic, F. High Prevalence of Vitamin D Insufficiency among Elite Spanish Athletes the Importance of Outdoor Training Adaptation. Nutr. Hosp. 2014, 30, 124–131. [Google Scholar] [CrossRef]
- Maïmoun, L.; Sultan, C. Effect of Physical Activity on Calcium Homeostasis and Calciotropic Hormones: A Review. Calcif. Tissue Int. 2009, 85, 277–286. [Google Scholar] [CrossRef]
- Touvier, M.; Deschasaux, M.; Montourcy, M.; Sutton, A.; Charnaux, N.; Kesse-Guyot, E.; Assmann, K.E.; Fezeu, L.; Latino-Martel, P.; Druesne-Pecollo, N.; et al. Determinants of Vitamin D Status in Caucasian Adults: Influence of Sun Exposure, Dietary Intake, Sociodemographic, Lifestyle, Anthropometric, and Genetic Factors. J. Investig. Dermatol. 2015, 135, 378–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scott, D.; Blizzard, L.; Fell, J.; Ding, C.; Winzenberg, T.; Jones, G. A Prospective Study of the Associations between 25-Hydroxy-Vitamin D, Sarcopenia Progression and Physical Activity in Older Adults. Clin. Endocrinol. 2010, 73, 581–587. [Google Scholar] [CrossRef] [PubMed]
- Gómez, J.M. The Role of Insulin-like Growth Factor I Components in the Regulation of Vitamin D. Curr. Pharm. Biotechnol. 2006, 7, 125–132. [Google Scholar] [CrossRef]
- Greene, M.W.; Roberts, A.P.; Frugé, A.D. Negative Association Between Mediterranean Diet Adherence and COVID-19 Cases and Related Deaths in Spain and 23 OECD Countries: An Ecological Study. Front. Nutr. 2021, 8, 591964. [Google Scholar] [CrossRef]
- Davis, C.; Bryan, J.; Hodgson, J.; Murphy, K. Definition of the Mediterranean Diet; a Literature Review. Nutrients 2015, 7, 9139–9153. [Google Scholar] [CrossRef] [PubMed]
- Tavakol, Z.; Ghannadi, S.; Tabesh, M.R.; Halabchi, F.; Noormohammadpour, P.; Akbarpour, S.; Alizadeh, Z.; Nezhad, M.H.; Reyhan, S.K. Relationship between Physical Activity, Healthy Lifestyle and COVID-19 Disease Severity; a Cross-Sectional Study. Z. Gesundh. Wiss. 2021, 1–9. [Google Scholar] [CrossRef]
- Charland, K.M.; Buckeridge, D.L.; Hoen, A.G.; Berry, J.G.; Elixhauser, A.; Melton, F.; Brownstein, J.S. Relationship between Community Prevalence of Obesity and Associated Behavioral Factors and Community Rates of Influenza-Related Hospitalizations in the United States. Influenza Other Respi. Viruses 2013, 7, 718–728. [Google Scholar] [CrossRef]
- Neelakantan, N.; Koh, W.-P.; Yuan, J.-M.; van Dam, R.M. Diet-Quality Indexes Are Associated with a Lower Risk of Cardiovascular, Respiratory, and All-Cause Mortality among Chinese Adults. J. Nutr. 2018, 148, 1323–1332. [Google Scholar] [CrossRef]
- Gombart, A.F.; Pierre, A.; Maggini, S. A Review of Micronutrients and the Immune System-Working in Harmony to Reduce the Risk of Infection. Nutrients 2020, 12, 236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vogel-González, M.; Talló-Parra, M.; Herrera-Fernández, V.; Pérez-Vilaró, G.; Chillón, M.; Nogués, X.; Gómez-Zorrilla, S.; López-Montesinos, I.; Arnau-Barrés, I.; Sorli-Redó, M.L.; et al. Low Zinc Levels at Admission Associates with Poor Clinical Outcomes in SARS-CoV-2 Infection. Nutrients 2021, 13, 562. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Kubota, Y.; Chernov, M.; Kasuya, H. Potential Role of Zinc Supplementation in Prophylaxis and Treatment of COVID-19. Med. Hypotheses 2020, 144, 109848. [Google Scholar] [CrossRef] [PubMed]
- Oh-hora, M.; Rao, A. Calcium Signaling in Lymphocytes. Curr. Opin. Immunol. 2008, 20, 250–258. [Google Scholar] [CrossRef] [Green Version]
- Suardi, C.; Cazzaniga, E.; Graci, S.; Dongo, D.; Palestini, P. Link between Viral Infections, Immune System, Inflammation and Diet. Int. J. Environ. Res. Public Health 2021, 18, 2455. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, L.D.M.; Teixeira, F.M.E.; Sato, M.N. Impact of Retinoic Acid on Immune Cells and Inflammatory Diseases. Mediat. Inflamm. 2018, 2018, 3067126. [Google Scholar] [CrossRef] [Green Version]
- Jones, B.G.; Oshansky, C.M.; Bajracharya, R.; Tang, L.; Sun, Y.; Wong, S.S.; Webby, R.; Thomas, P.G.; Hurwitz, J.L. Retinol Binding Protein and Vitamin D Associations with Serum Antibody Isotypes, Serum Influenza Virus-Specific Neutralizing Activities and Airway Cytokine Profiles. Clin. Exp. Immunol. 2016, 183, 239–247. [Google Scholar] [CrossRef] [Green Version]
- Rudraraju, R.; Jones, B.G.; Surman, S.L.; Sealy, R.E.; Thomas, P.G.; Hurwitz, J.L. Respiratory Tract Epithelial Cells Express Retinaldehyde Dehydrogenase ALDH1A and Enhance IgA Production by Stimulated B Cells in the Presence of Vitamin A. PLoS ONE 2014, 9, e86554. [Google Scholar] [CrossRef] [Green Version]
- Maggini, S.; Pierre, A.; Calder, P.C. Immune Function and Micronutrient Requirements Change over the Life Course. Nutrients 2018, 10, 1531. [Google Scholar] [CrossRef] [Green Version]
- Müller, O.; Krawinkel, M. Malnutrition and Health in Developing Countries. CMAJ 2005, 173, 279–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reider, C.A.; Chung, R.-Y.; Devarshi, P.P.; Grant, R.W.; Hazels Mitmesser, S. Inadequacy of Immune Health Nutrients: Intakes in US Adults, the 2005-2016 NHANES. Nutrients 2020, 12, 1735. [Google Scholar] [CrossRef] [PubMed]
- Roman Viñas, B.; Ribas Barba, L.; Ngo, J.; Gurinovic, M.; Novakovic, R.; Cavelaars, A.; de Groot, L.C.P.G.M.; van’t Veer, P.; Matthys, C.; Serra Majem, L. Projected Prevalence of Inadequate Nutrient Intakes in Europe. Ann. Nutr. Metab. 2011, 59, 84–95. [Google Scholar] [CrossRef] [PubMed]
- Derbyshire, E.; Delange, J. COVID-19: Is There a Role for Immunonutrition, Particularly in the over 65s? BMJ Nutr. Prev. Health 2020, 3, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Quintela, A.; Milton-Laskibar, I.; Trepiana, J.; Gómez-Zorita, S.; Kajarabille, N.; Léniz, A.; González, M.; Portillo, M.P. Key Aspects in Nutritional Management of COVID-19 Patients. J. Clin. Med. 2020, 9, 2589. [Google Scholar] [CrossRef]
- Grant, W.B.; Lahore, H.; McDonnell, S.L.; Baggerly, C.A.; French, C.B.; Aliano, J.L.; Bhattoa, H.P. Evidence That Vitamin D Supplementation Could Reduce Risk of Influenza and COVID-19 Infections and Deaths. Nutrients 2020, 12, 988. [Google Scholar] [CrossRef] [Green Version]
- Polero, P.; Rebollo-Seco, C.; Adsuar, J.C.; Pérez-Gómez, J.; Rojo-Ramos, J.; Manzano-Redondo, F.; Garcia-Gordillo, M.Á.; Carlos-Vivas, J. Physical Activity Recommendations during COVID-19: Narrative Review. Int. J. Environ. Res. Public Health 2020, 18, 65. [Google Scholar] [CrossRef]
- Aktug, Z.B.; Demir, N.A. An Exercise Prescription for COVID-19 Pandemic. Pak. J. Med. Sci. 2020, 36, 1732–1736. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variable | Total n = 40 |
|---|---|
| Female, n (%) | 24 (60) |
| Age (years) 1 | 43.98 ± 13.65 |
| BMI (kg/m2) 1 | 26.4 ± 5.26 |
| BMI classification, n (%) | |
| Normal weight | 16 (40) |
| Overweight | 16 (40) |
| Obesity | 8 (20) |
| Waist (cm) 1 | 91.02 ± 14.07 |
| Central obesity, n (%) | |
| Female (≥88 cm) | 11 (45.8) |
| Male (≥102 cm) | 5 (31.3) |
| Systolic (mmHg) 1 | 111.6 ± 18.33 |
| Diastolic (mmHg) 1 | 74.7 ± 14.1 |
| Oxygen saturation (SpO2%) 2 | 93 (86.1–97) |
| Heart rate (bpm) 1 | 79.6 ± 12.37 |
| Temperature (°C) 1 | 36.8 ± 0.34 |
| Respiratory rate (BPM) 2 | 20 (15.05–30) |
| Transferrin (ng/mL) 2 | 236 (178.25–365.45) |
| Ferritin (ng/mL) 2 | 138.5 (8.64–533.75) |
| D-dimer (ng/mL) 2 | 294.45 (129.81–1229.83) |
| 25(OH)D (ng/mL) 2 | 22.7 (12.71–45.24) |
| Comorbidity, n (%) | 12 (30) |
| Moderate physical activity (min/d) 2 | 30 (0–360) |
| Intense physical activity (min/d) 2 | 0 (0–150) |
| Food intake quality, n (%) | |
| Healthy Food Intake | 15 (37.5) |
| Habits in Need of Improvement | 12 (30) |
| Unhealthy Food Intake | 13 (32.5) |
| COVID-19 Symptoms, n (%) | 38 (95) |
| Variable | Micronutrient Intake 1 n = 40 | RDA’s for Mexican Population | p-Value | Percentage of Adequacy 2 |
|---|---|---|---|---|
| Vitamin A (μg RE) | 508.35 ± 238.62 | 568 | 0.122 | 89.5 (76.06–102.94) |
| Vitamin D (μg) | 3.85 ± 5.03 | 10 | <0.0001 | 38.5 (22.41–54.6) |
| Vitamin E (mg) | 5.11 ± 3.42 | 11 | <0.0001 | 46.45 (36.5–56.41) |
| Vitamin K (μg) | 56.95 ± 74.37 | 78 | 0.081 | 73 (42.52–103.51) |
| Vitamin C (mg) | 80 ± 71.02 | 60 | 0.083 | 133.34 (95.48–171.19) |
| Thiamin (mg) | 0.91 ± 0.5 | 0.8 | 0.190 | 113.25 (93.18–133.32) |
| Riboflavin (mg) | 1.23 ± 0.61 | 0.84 | <0.001 | 146.49 (123.18–169.8) |
| Niacin (mg) | 14.61 ± 7.33 | 11 | 0.003 | 132.84 (111.55–154.14) |
| Pantothenic acid (mg) | 2.94 ± 1.73 | 4 | <0.001 | 73.61 (59.78–87.45) |
| Vitamin B6 (mg) | 1.68 ± 1.94 | 0.93 | 0.018 | 181.16 (114.51–247.81) |
| Folic acid (μg) | 498.53 ± 928.16 | 380 | 0.424 | 131.19 (53.08–209.31) |
| Vitamin B12 (μg) | 4.12 ± 6.26 | 2.1 | 0.048 | 196.09 (100.69–291.49) |
| Calcium (mg) | 644.46 ± 226.73 | 900 | <0.0001 | 71.61 (63.55–79.66) |
| Iron (mg) | 10.48 ± 5.14 | 17 | <0.0001 | 61.62 (51.96–71.29) |
| Zinc (mg) | 7.49 ± 3.05 | 10 | <0.0001 | 74.92 (65.15–84.69) |
| Variable | 25(OH)D Insufficiency <29 ng/mL n = 32 | 25(OH)D Sufficiency >30 ng/mL n = 8 | p-Value |
|---|---|---|---|
| BMI (kg/m2) 1 | 26.35 ± 4.74 | 26.58 ± 7.37 | 0.914 |
| Waist (cm) 1 | 92.18 ± 12.85 | 86.38 ± 18.46 | 0.302 |
| Food intake quality, n (%) 2 | |||
| Unhealthy Food Intake | 13 (40.6) | 0 (0) | |
| Habits in Need of Improvement | 10 (31.3) | 2 (25) | |
| Healthy Food Intake | 9 (28.1) | 6 (75) | 0.029 |
| Fitzpatrick skin phototype, n (%) 2 | |||
| Type I | 0 (0) | 0 (0) | 0.883 |
| Type II | 6 (18.8) | 1 (12.5) | |
| Type III | 13 (40.6) | 3 (37.5) | |
| Type IV | 12 (37.5) | 4 (50) | |
| Type V | 1 (3.1) | 0 (0) | |
| Type VI | 0 (0) | 0 (0) | |
| Sun exposure (min/d) 3 | 25 (0–243) | 120 (15–180) | 0.017 |
| Sun exposure (10 a.m.–3 p.m.), n (%) 4 | 10 (31.3) | 6 (75) | 0.154 |
| Sunscreen, n (%) 4 | 16 (50) | 2 (25) | 0.193 |
| Vitamin D (μg) 3 | 2.44 (0–13.81) | 2.39 (0–12.14) | 0.919 |
| Comorbidity, n (%) 4 | 10 (31.3) | 2 (25) | 0.548 |
| Moderate physical activity (min/d) 3 | 30 (0–402) | 45 (0–105) | 0.390 |
| Intense physical activity (min/d) 3 | 0 (0–101.25) | 80 (0–142.5) | 0.032 |
| COVID-19 Symptoms, n (%) 4 | 32 (100) | 6 (75) | 0.036 |
| Univariate Analysis | |||
|---|---|---|---|
| Variable | OR | 95% CI | p-value |
| Food intake quality | 5.51 | 1.27–24.02 | 0.023 |
| Intense physical activity (min/d) | 1.02 | 1.01–1.04 | 0.011 |
| Sun exposure (min/d) | 1.01 | 0.99–1.02 | 0.069 |
| Vitamin D intake (μg) | 1.16 | 0.99–1.35 | 0.054 |
| Multivariate Analysis | |||
| Variable | OR | 95% CI | p-value |
| Food intake quality 1 | 6.79 | 1.18–39.09 | 0.032 |
| Intense physical activity (min/d) 2 | 1.04 | 1.01–1.07 | 0.013 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
González-Estevez, G.; Turrubiates-Hernández, F.J.; Herrera-Jiménez, L.E.; Sánchez-Zuno, G.A.; Herrera-Godina, M.G.; Muñoz-Valle, J.F. Association of Food Intake Quality with Vitamin D in SARS-CoV-2 Positive Patients from Mexico: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 7266. https://doi.org/10.3390/ijerph18147266
González-Estevez G, Turrubiates-Hernández FJ, Herrera-Jiménez LE, Sánchez-Zuno GA, Herrera-Godina MG, Muñoz-Valle JF. Association of Food Intake Quality with Vitamin D in SARS-CoV-2 Positive Patients from Mexico: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2021; 18(14):7266. https://doi.org/10.3390/ijerph18147266
Chicago/Turabian StyleGonzález-Estevez, Guillermo, Francisco Javier Turrubiates-Hernández, Laura Elena Herrera-Jiménez, Gabriela Athziri Sánchez-Zuno, Melva Guadalupe Herrera-Godina, and José Francisco Muñoz-Valle. 2021. "Association of Food Intake Quality with Vitamin D in SARS-CoV-2 Positive Patients from Mexico: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 18, no. 14: 7266. https://doi.org/10.3390/ijerph18147266
APA StyleGonzález-Estevez, G., Turrubiates-Hernández, F. J., Herrera-Jiménez, L. E., Sánchez-Zuno, G. A., Herrera-Godina, M. G., & Muñoz-Valle, J. F. (2021). Association of Food Intake Quality with Vitamin D in SARS-CoV-2 Positive Patients from Mexico: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 18(14), 7266. https://doi.org/10.3390/ijerph18147266