Abstract
Intimate partner violence (IPV) is a pervasive form of gender-based violence that exacerbates in humanitarian settings. This systematic review examined the myriad IPV impacts and the quality of existing evidence of IPV in humanitarian settings. Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) procedures, a total of 51 articles were included from the 3924 screened. We identified the impact of IPV across two levels of the ecological framework: individual and microsystem. Our findings corroborated previous evidence that indicated IPV to be associated with adverse physical and mental health for survivors. Our findings also uniquely synthesized the intergenerational impact of IPV in humanitarian settings. However, findings highlighted a glaring gap in evidence examining the non-health impact of IPV for survivors in humanitarian settings and across levels of the ecological framework. Without enhanced research of women and girls and the violence they experience, humanitarian responses will continue to underachieve, and the needs of women and girls will continue to be relegated as secondary interests. Investment should prioritize addressing the range of both health and non-health impacts of IPV among individuals, families, and communities, as well as consider how the humanitarian environment influences these linkages.
1. Introduction
Intimate Partner Violence (IPV) is a critically concerning form of gender-based violence in humanitarian settings. IPV includes violence that occurs within an intimate relationship of romantic partners or ex-partners, whether cohabitating or not [1]. Moreover, IPV can be exhibited through physical, sexual, or psychological harm and includes physical aggression, sexual coercion, psychological abuse, and controlling behaviors [2]. Violence perpetrated by intimate partners within the private sphere of the home continues to be an insidious form of gender-based violence during periods of acute crisis as well as protracted emergencies and post-conflict settings [3,4,5,6,7]. In humanitarian settings, known predictors of interpersonal violence within the household, including IPV, include conflict exposure, substance use, low economic status, adverse mental health, and limited social support [8], and many known determinants of IPV are exacerbated in emergency settings [9].
While less is known regarding the widespread impacts of IPV in humanitarian settings specifically, several reviews have synthesized evidence examining the global impacts of IPV on survivors. One review, not specific to low- and middle-income countries (LMICs) nor humanitarian settings, identified consistent evidence that IPV affected sexual risk-taking behaviors, risk of lifetime sexually transmitted infections (STIs), unwanted pregnancy or induced abortion, and sexual dysfunction [10]. Another review examining both physical and mental health consequences found that IPV survivors were more likely to exhibit physical injury, chronic pain, gastrointestinal issues, gynecological disorders, depression, and post-traumatic stress disorder (PTSD) [11]. Systematic reviews of violence against women and girls in LMICs found that IPV was associated with composite measures of adverse mental health, suicidal ideation and behavior, and symptoms of depression, posttraumatic stress, and disordered eating [12], as well as STIs, unwanted pregnancy or induced abortion, and number of sexual partners [13]. While these four reviews bolster our understanding of the consequences of experiencing IPV, they have three notable gaps: (1) these reviews did not consider IPV in humanitarian settings, (2) these reviews did not include non-health correlates with IPV, and (3) these reviews did not examine the impacts of IPV beyond the survivor. The importance of addressing each of these gaps is described below.
Humanitarian crises are associated with periods of extreme chronic stress, loss of health and social service infrastructure, and strained social support networks; all can serve to exacerbate the impacts of IPV [14,15]. Moreover, this fundamental breakdown within humanitarian settings could contribute to unique consequences of IPV when compared to non-humanitarian settings. For example, the socioeconomic precarity within humanitarian settings may not only contribute to elevated prevalence of IPV but may also limit survivors’ abilities to return to or search for employment after experiencing IPV. Data collection of IPV in humanitarian settings is also difficult due to the instability inherent to natural disasters, infectious disease outbreaks, mass displacement, and civil unrest [6,16,17]. These measurement challenges have contributed to a paucity of IPV research in humanitarian settings; thus, little is known about how IPV impacts compare to those encountered in non-humanitarian settings.
Survivors in humanitarian settings may experience different types and severity of health impacts given the contextual variances between humanitarian and non-humanitarian settings. For example, women who would have otherwise accessed healthcare facilities for physical injuries from IPV may be unable to do so during a natural disaster, thus, increasing their risk for secondary infection or long-term disability. Moreover, research has yet to synthesize the non-health related impacts of IPV for survivors despite a growing body of evidence that has highlighted adverse economic outcomes for IPV survivors [18,19,20,21]. Other potential non-health impacts of IPV for survivors include loss of education and opportunity, productivity loss at work and home, stigma and shame, as well as diminished social capital, autonomy, and decision making.
Given the burden of violence placed on survivors, individual-level consequences of IPV are important to identify; however, IPV also has implications for the family unit and society. For example, witnessing IPV as a child has been linked to adverse mental health as well as an increased likelihood of perpetrating and experiencing IPV later in life [22,23,24]. IPV can also have harder-to-measure consequences at the community and societal levels. Women and girls who have experienced IPV may become further embedded in a cycle of victimization that perpetuates the feminization of poverty and the wider erosion of women’s sexual and reproductive agency. Gender-based violence, including IPV, has also been demonstrated to have harmful macroeconomic impacts in non-humanitarian settings [25,26,27,28,29,30]. Other potential impacts across the ecological framework include intra-household tensions and poverty, increased service needs and strains (health, legal, housing, justice, etc.), as well as perpetuation of harmful social norms, structural violence, and gender inequities.
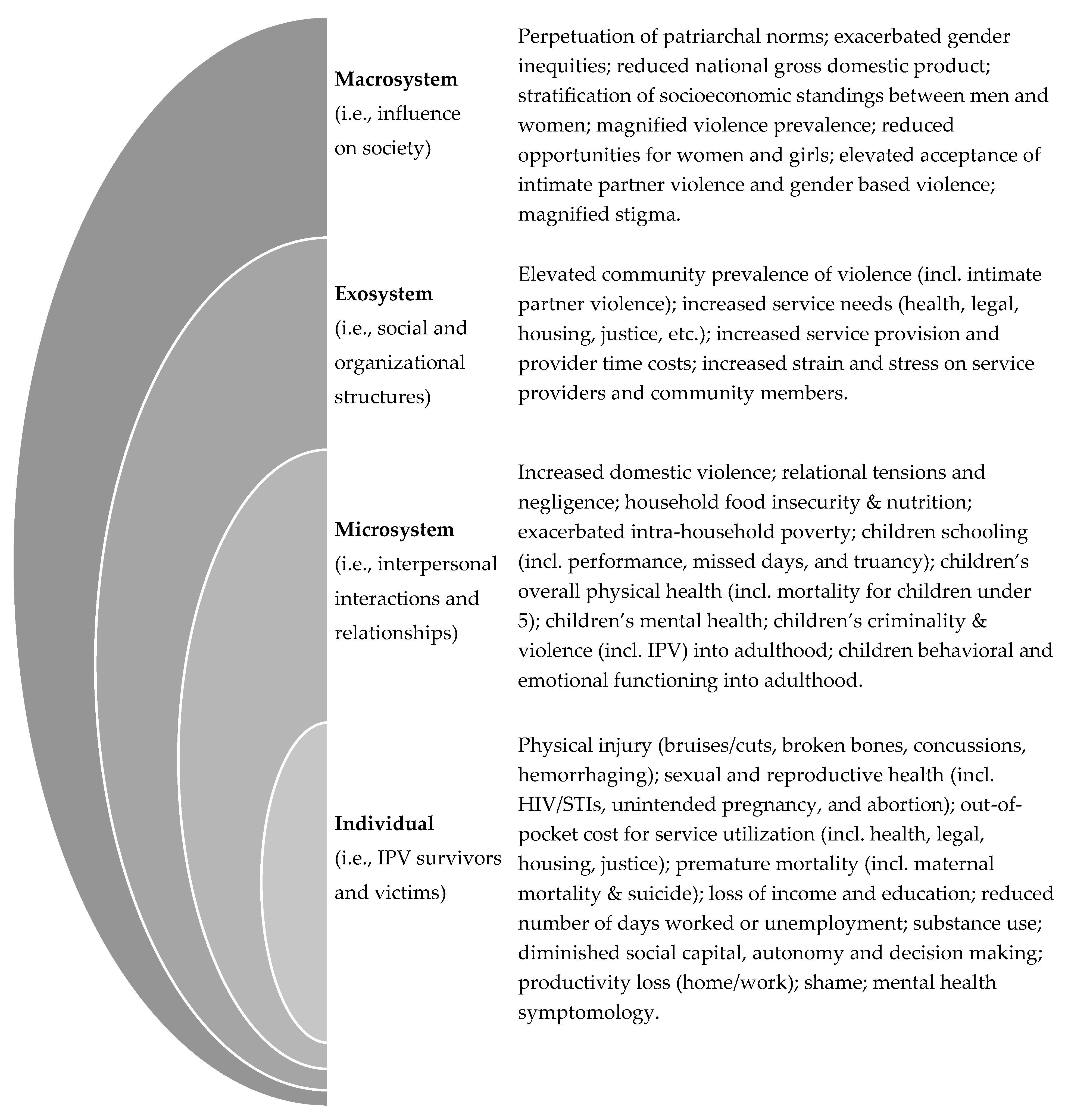
Thus, it is critically important to examine the breadth of IPV impacts in humanitarian settings to understand the complexity of IPV and inform response efforts. Comprehensively examining IPV can enable the critical examination across and between all levels of society. Heise’s [31] seminal ecological framework illustrated the synergies between personal, situational, and sociocultural risk factors of male-perpetrated IPV across four levels: individual (i.e., IPV survivors and victims), microsystem (i.e., interpersonal interactions and relationships), exosystem (i.e., social and organizational structures), and macrosystem (i.e., influence on society). This risk framework has been adapted to humanitarian settings [9] and integrated for program design [32]; however, it has not been adapted as an impact framework. Building from the IPV and humanitarian literature, we adapted Heise’s ecological framework to hypothesize the myriad impacts of IPV in humanitarian settings. The adapted framework in Figure 1 guided the expansive interest of this systematic review by mapping potential impacts of IPV in humanitarian settings at the individual, microsystem, exosystem, and macrosystem levels.
Figure 1.
Impacts of intimate partner violence in humanitarian settings using an amended ecological framework.
Using the adapted ecological framework, this systematic review endeavored to examine the impact of IPV for survivors, families, communities, and society. Given the methodological challenges of collecting data in humanitarian settings, this review also examined the quality of studies from which the evidence was drawn. Understanding the full range of impacts that IPV has in humanitarian settings can simultaneously support critical programming for survivors and address the needs of families and communities affected by IPV.
2. Methods
2.1. Search Strategy
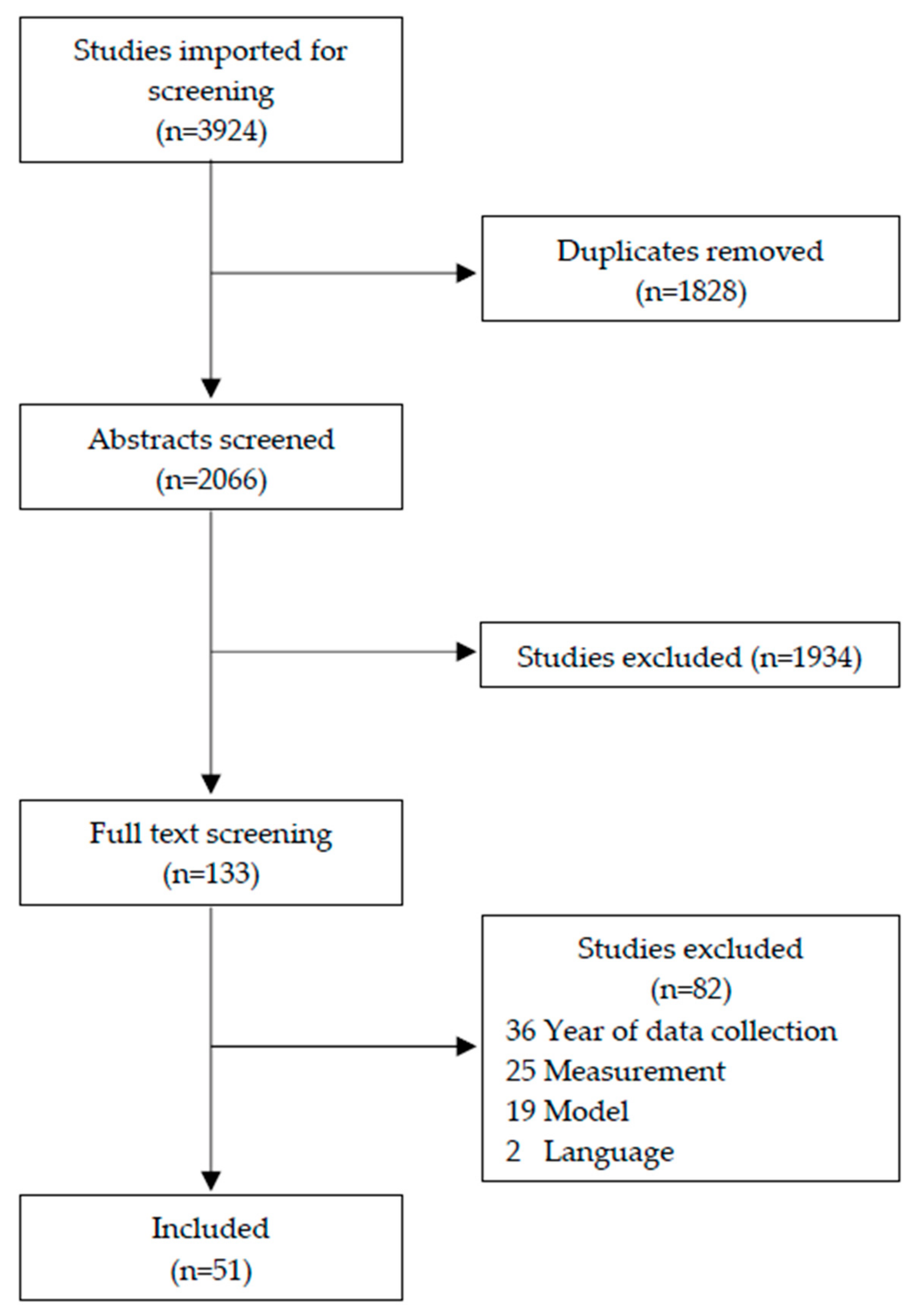
We conducted a systematic review of peer-reviewed articles that examined the impacts of IPV in humanitarian settings using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [33]. Aligning with standardized violence definitions brokered by the WHO Multi-Country Study in 2005 on Women’s Health and Domestic Violence against Women [34], the search included articles published between 2005 and 2020. Our search terms strategy was applied to four databases: Embase through Elsevier, Medline via EBSCO, PsycInfo through Ebscohost, and Scopus via Scopus. Abstracts from the identified articles (N = 3924) were imported into Covidence for duplication removal, abstract review, and full-text review. All abstracts and full texts were reviewed by the authors to determine if they met review criteria at each stage. Conflicts at both the abstract and full-text review stages were reread and discussed by the authors for the final decision. A visual representation of the review process is available in Figure 2.
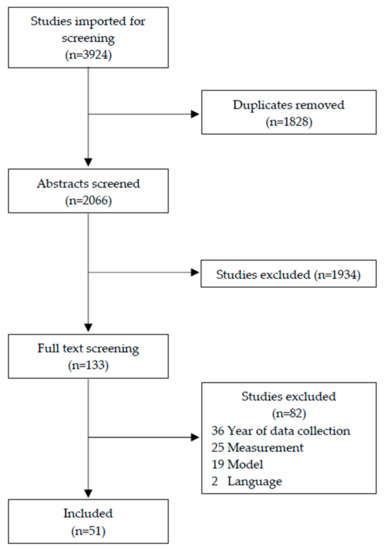
Figure 2.
PRISMA flow diagram.
2.2. Inclusion and Exclusion Criteria
Using systematic review software (Covidence), abstracts were reviewed per inclusion criteria. Criteria included abstracts that utilized quantitative methods and abstracts that included at least one form of IPV as an independent variable. Examples of eligible IPV variables included experiencing physical IPV during adulthood, mean community rates of IPV, and witnessing intra-parental violence during childhood. Using the United Nation’s Financial Tracking System (FTS) [35], articles were considered eligible if their abstract mentioned that data were collected during at least one year when the country received humanitarian funding through either the Consolidated Appeals Process (CAP) or Humanitarian Response Planning (HRP). If the year of data collection was unclear, abstracts were flagged but included in the full-text review (n = 54). Countries that received flash and regional appeals were only included if they also received either direct CAP or HRP funding. Systematic reviews and dissertations were not included, but their reference lists were reviewed to identify potentially relevant articles.
The 133 articles that met the criteria for full-text review were closely examined to determine if the article met exclusion criteria. First, the authors checked to see if each article was available in English. Articles were then re-reviewed to ensure data collection overlapped at some point during receipt of CAP and HRP funding between 2005 and 2020. Articles that did not make explicit note of when data were collected were excluded. However, articles were included if there was any data collection during a CAP or HRP year; thus, some articles may include data that were collected during CAP/HRP and non-CAP/HRP years. Similarly, included articles may include some degree of data collection before 2005 if simultaneous data collection coincided with a CAP/HRP year. Articles were also more rigorously examined based on if their definition of IPV aligned with the Inter-Agency Standing Committee (IASC) guidelines definition [1]. For example, articles needed to either include the explicit IPV terminology or describe how their measure of violence—particularly interpersonal and domestic violence—was restricted to intimate partners. Finally, analytical models that did not disaggregate by country were excluded.
2.3. Data Extraction and Quality Assessment
Each article that met inclusion and exclusion criteria was re-reviewed in full (n = 51). Data extracted from each article related to the study’s sampling framework, variable creation, and analysis methods. Using the Appraisal tool for Cross-Sectional Studies (AXIS tool) [36], all included articles were individually scored based on 20 quality assessment criteria.
3. Findings
3.1. Overview of Included Articles
The majority of included articles collected data in sub-Saharan Africa (n = 33). The remaining articles, including those with data from multiple regions, included data from Central and Southeast Asia (n = 7), the Middle East (n = 7), or the Caribbean (n = 5). It is worth noting that all articles from the Caribbean were from Haiti and no articles were published from Central nor South America. Further, while 48 countries received CAP or HRP funding between 2005 and 2020, only 18 had at least one article that met inclusion criteria. While articles that included data collection from 2020 to 2018 were limited, the years of data collection were roughly equal across the remaining years 2005–2017 with an average of six articles including data collected from each of these years.
All of the articles included women and/or girls within the sample and five also included men and/or boys. The vast majority of articles utilized cross-sectional data either from a cross-sectional (72.55%, n = 37) or longitudinal study (17.65%, n = 9). Only 9.80% (n = 5) articles included analysis using longitudinal data. With 19.61% (n = 10) of articles using data from interventions, most of the remaining articles utilized population-based designs (41.18%, n = 21) or non-population-based designs (35.29%, n = 18). One article included data from an intervention study in Afghanistan and a non-population-based study design from Palestine. The final type of study design, a retrospective case review, was only used in one article that examined homicides in Maputo Province, Mozambique between 2016 and 2017.
The most common primary analysis model was multivariable logistic regression (60.78%, n = 31). Ten articles (19.61%) utilized other types of multivariable inferential modeling, including multivariable linear regression (9.80%, n = 5). One article included both multivariable linear and logistic regressions and another article utilized multivariable hierarchical regression. The primary models for the remaining nine articles that did not incorporate multivariable inferential modeling used either bivariate (13.73%, n = 7) or descriptive (3.92%, n = 2) analysis. See Table 1 for a comprehensive overview of the included articles.

Table 1.
Overview of included studies.
3.2. Impacts of IPV
Consequences of IPV were identified across two primary levels: individual/survivor and microsystem/relationship (see Table 2). While all but six inferential articles demonstrated significant associations between at least one form of IPV and adverse individual-level impacts, these findings were often related to the ill-health of the survivor. Only two articles examined how direct IPV experience was associated with future IPV victimization (n = 1) or perpetration (n = 1), while five articles included variables related to healthcare access, healthcare adherence, or health status disclosure.
Table 2.
Associations with intimate partner violence, per study.
Except for one article that examined IPV perpetration and one article that examined IPV revictimization, all of the individual-level associations with IPV were directly related to ill-health (n = 41). The most common associations were in the mental health category (n = 11). Each of the 11 mental health studies included significant associations between IPV experience and worse mental health, with mental health variables ranging from aggregate wellness measures (including poor mental health and mental component summary) to specific conditions (including PTSD, substance abuse, and depression) or suicide variables (including ideation, thoughts, and attempts). The most common mental health variable was depression, which was included in six-articles and included perinatal depression, major depressive disorder, and past one-week, two-week, or four-week depression symptoms.
Other health categories at the individual level included the groupings of reproductive health (n = 8), HIV and other sexually transmitted infections (n = 7), pregnancy, birth, and infancy (n = 7), healthcare access, adherence, or disclosure (n = 5), overall health (n = 2), substance use (2.17% n = 1), and fatal injuries (n = 1). Significant findings were consistent across groupings, linking IPV with adverse physical health and mental health. Only seven of the articles included no significant results concerning individual-level impacts of IPV; moreover, there were two descriptive articles (n = 2) that were excluded when reviewing significance.
Fewer articles included impacts of IPV at the microsystem level (23.53%, n = 12). The 10 articles that examined the intergenerational impact of IPV between parents or caregivers often focused on IPV perpetration (n = 3) or victimization (n = 4) during adulthood. Other categories, each examined by one article, included physical health conditions during childhood, emotional and behavioral problems during childhood, and accepting attitudes of IPV during adulthood. All of these articles included significant associations with at least one of the IPV variable(s) and an adverse outcome, except one article that did not find a significant association between childhood exposure and perpetration during adulthood. Moreover, one article examined the significant association between IPV and marital disruption. The final article, examining the associations of IPV with relationships, identified that women who experienced physical violence in the past year were more likely to report a female relative being killed in the name of honor by another family member. While community-level IPV (i.e., societal level violence) was included as an independent variable in three articles, no articles examined societal-level impacts of IPV.
3.3. IPV Variables
The measurement of IPV varied across articles (See Table 3), with a little less than half including more than one measure of IPV (43.14%, n = 22). However, there were some notable themes in measurement, including the tendency to focus on direct victimization of violence (86.27%, n = 44). When measuring direct victimization of IPV, articles often included the timeframe of lifetime exposure for at least one of the violence variables (n = 29). The most common form of IPV was multiple or any form (n = 28), and most measures of direct victimization of IPV were binary (n = 37).
Table 3.
Classification of intimate partner violence as independent variable(s), per study.
Fewer articles included variables that identified whether respondents witnessed IPV between their parents or primary caregivers during childhood (19.61%, n = 10). However, all of those articles included binary measurement of all forms of violence. Each of the articles (n = 3) that included a variable of community rates of IPV included multiple or any form of IPV; one article also included community rates of sexual violence. The timeframe used to determine community rates was either the past five-year reporting from secondary data (n = 1) or the aggregate lifetime experience of respondents in the sample (n = 2). The two measurement typologies for community violence were ordinal (n = 1) or ratio (n = 2).
3.4. Quality Assessment
As there are no formal AXIS scoring criteria, the authors ranked articles into four categories whereby scores of 15–20 were classified as the upper category, 10–14 as the upper-middle category, 5–9, as the lower-middle category, and 0–4 as the lowest category. Table 1 includes the quality assessment classification of each article and Table 4 includes the aggregate AXIS results per item. Nearly all articles met the criteria for the top 31.37% (n = 16) or upper-middle 62.75%% (n = 32) categories, with only three (5.88%) articles meeting the criteria for the lower-middle category and none meeting the criteria for the lowest category. The low overall scoring of items 13 and 14, both of which pertained to non-response rates, was not surprising given that only 45.10% (n = 23) of articles described measures taken to categorize non-responders (item 7). The other low score was related to the measurement of risk factors and dependent variables (item 9), whereby only 25.49% (n = 13) of the articles fully described how the primary variables were derived from instruments or measurements that had been trialed, piloted, or previously published.
Table 4.
AXIS quality assessment of included articles, frequency per item, and quartile distribution of final score.
The averages of the first four domains in the AXIS tool—introduction, methods, results, discussion—were relatively similar; however, the final domain of “other” included two items with low averages. The first item of the “other” domain asked about funding sources or conflicts of interest that may affect the authors’ interpretation of the results, whereby only half of the articles (n = 28) did not have overt conflicts. It is important to note that the “don’t know” option was selected whenever funding information was not provided; thus, those votes did not contribute to the final count. Similarly, only 68.63% (n = 35) of the articles reported ethical approval; however, this only reflects ethical approval reported within the articles. Some studies may have acquired ethical approval, but the authors did not report it. In both instances, these findings are important in regard to flagging the inconsistent reporting of ethical information.
4. Discussion
This review endeavored to identify the common and unique impacts of IPV in humanitarian settings across the entire ecological framework; however, no included article examined the impacts of IPV at the exosystem or macrosystem levels. Thus, we synthesized the existing empirical evidence at the individual and microsystem levels. Our synthesis corroborated previous reviews that indicated IPV to be associated with adverse physical and mental health outcomes for survivors at the individual level [10,11,12,13] and identified that IPV in humanitarian settings has detrimental impacts on family members at the microsystem level. Critically, the included articles for this review did not elucidate humanitarian-unique impacts of IPV. This is concerning, as there are many characteristics germane to humanitarian settings that could both exacerbate the prevalence of IPV [6] and magnify the impact of IPV [9,88]. Without a comprehensive understanding of IPV’s influence across the ecological framework, important considerations for programming and policy may be overlooked and funding may continue to underserve women and girls in humanitarian settings [89]. As the evidence-base expands, we advocate for future efforts to consider how the ecological framework proposed in Figure 1 may be refined to comprehensively reflect the impacts of IPV in humanitarian settings. Few of the hypothesized impacts of IPV from Figure 1 were explored in the included articles and no novel impacts were included within the study designs of the reviewed literature, thus, highlighting huge and important data gaps.
A striking challenge with examining the included research to ascertain the impacts of IPV during humanitarian crises was the reliance on lifetime experience of IPV as a single binary variable. In addition to reflecting an oversimplification or potential measurement issue, this lifetime experience of IPV could have occurred outside the period when a context would be considered a humanitarian setting. Only ten articles included IPV experienced within the past 1 to 12 months, but it is important to flag that all of them reported a significant association between IPV and the impacts of IPV. The number of selected articles was too small to rigorously compare but this finding highlights that IPV experienced during a humanitarian crisis may be more consistently associated with adverse IPV impacts than lifetime exposure. Future research should include explicit consideration regarding how different experiences of violence before, during, and after a humanitarian crisis may uniquely influence survivors, families, and communities. Research should also explore the interactions of IPV impacts between levels of ecological framework. Such research would begin to elucidate how and to what extent various levels of the ecological framework have interactive and reinforcing influence on the impacts of IPV (also known as reciprocal determinism). This type of interconnected thinking could bolster program efficiency by supporting more targeted programming to address the most acutely influential impacts of IPV [90,91].
When examining the quality assessment results, the AXIS tool yielded favorable scores for the included articles; however, there are still important gaps regarding the broader scientific evidence available. The choice of the AXIS tool was, in part, due to the cross-sectional nature of most articles. Only five of included articles analyzed longitudinal data, aligning with other reviews in non-humanitarian settings with a similar dearth in longitudinal data [12,13]. Longitudinal studies from humanitarian settings are needed to temporally understand the interplay of IPV experience, humanitarian conflict/emergency, and outcomes across the ecological model. Moreover, humanitarian IPV research is geographically stymied. Of the 48 countries that received either CAP or HRP funding between 2005 and 2020, data from only 18 countries (37.50%) were included within a publication that met our inclusion criteria. The vast majority of data were collected within the African continent, and there were no articles from South and Central America. The included studies were also limited in their ability to consider the temporal and geographical severity of humanitarian crises. Emergency designation (Level 1—Level 3) is available for current and recent crises [92], but there is no open-source designation of crisis severity between settings and across time. The INFORM Global Crisis Severity Index (GCSI) provides as an emerging initiative that may support examination of humanitarian crisis designation and IPV impacts for future research [93]. By integrating multi-level modeling techniques of GCSI designations or other secondary data sources like Armed Conflict Location and Event Data Project (ACLED) or Uppsala Conflict Data Program (UCDP) [4,54], researchers could examine the influence of various forms of IPV between crisis severity. In the meantime, researchers should consider operationalizing humanitarian stressors, such as self-reported conflict exposure and forced migration. Researchers and donors, alike, need to consider how to more inclusively and comprehensively fix these data gaps as they impede the ability to address the impacts of IPV in humanitarian settings.
5. Limitations
Limitations of this systematic review should be carefully considered. The overwhelmingly significant associations demonstrated in the findings may be a result of publication biases for articles that demonstrate significant findings. Thus, we cannot exhaustively state that other dependent variables have not been examined, only that other dependent variables were not available in the published peer-reviewed literature. Future research should examine and report on a range of outcomes that have been theorized to have associations with IPV. When including common impact variables, future research should build upon existing modelling to support comparability as the misalignment in measurement across studies hindered the possibility of meta-analysis for this systematic review. Finally, this systematic review utilized the AXIS tool for quality assessment despite not all articles using cross-sectional data. While the AXIS tool was developed for cross-sectional studies, each item within the AXIS tool was relevant for longitudinal research and the authors felt it was important to apply the same criteria for each article to enable comparability.
6. Conclusions
IPV in humanitarian settings is pervasive, and findings from this review indicated that its impacts are far-reaching. We demonstrated that IPV was significantly associated with a range of adverse health and non-health impacts for individuals and family members. However, there remains a paucity of inclusive research examining the novel impacts of IPV in humanitarian settings across the ecological framework. An understanding of the health and non-health impacts of IPV among survivors and, importantly, their families and communities, is critical for programming to thwart the widespread harms of IPV. With any hopes of achieving the Sustainable Development Goal of Gender Equality by 2030 [94], research and investment needs to prioritize the unique experiences of IPV by survivors in humanitarian settings and the impacts across the ecological framework.
Author Contributions
The manuscript was conceptualized by L.S. and M.M. Article review and data extraction was conducted by K.T., M.M. and S.M. and supported by C.P., I.S., L.S. and L.V. Initial literature review was conducted by K.T., L.V., M.M. and S.M., M.M., C.P., I.S., K.T., L.S., L.V. and S.M. were involved in original draft writing, editing, and final approval. All authors have read and agreed to the published version of the manuscript.
Funding
This study is made possible by the support of the American People through the US State Department Bureau of Population, Refugees and Migration. The findings of this study are the sole responsibility of the contributing authors and do not necessarily reflect the views of the United States Government.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- IASC. Guidelines for Integrating Gender-Based Violence Interventions in Humanitarian Action; IASC: Geneva, Switzerland, 2015. [Google Scholar]
- UNFPA. Managing Gender-based Violence Programmes in Emergencies. Available online: https://extranet.unfpa.org/Apps/GBVinEmergencies/index.html (accessed on 17 December 2020).
- Catani, C. War in the Home- an Overview of the Connection between War Traumatization and Domestic Violence. Behav. Ther. 2010, 20, 19–27. [Google Scholar] [CrossRef]
- Kelly, J.T.D.; Colantuoni, E.; Robinson, C.; Decker, M.R. From the Battlefield to the Bedroom: A Multilevel Analysis of the Links between Political Conflict and Intimate Partner Violence in Liberia. BMJ Glob. Health 2018, 3, 668. [Google Scholar] [CrossRef]
- Parcesepe, A.; Stark, L.; Roberts, L.; Boothby, N. Measuring Physical Violence and Rape against Somali Women Using the Neighborhood Method. Violence Women 2016, 22, 798–816. [Google Scholar] [CrossRef]
- Stark, L.; Ager, A. A Systematic Review of Prevalence Studies of Gender-Based Violence in Complex Emergencies. Trauma Violence Abus. 2011, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Stark, L.; Warner, A.; Lehmann, H.; Boothby, N.; Ager, A. Measuring the Incidence and Reporting of Violence against Women and Girls in Liberia Using the “Neighborhood Method”. Confl. Health 2013, 7, 20. [Google Scholar] [CrossRef] [Green Version]
- Rubenstein, B.L.; Lu, L.Z.N.; MacFarlane, M.; Stark, L. Predictors of Interpersonal Violence in the Household in Humanitarian Settings: A Systematic Review. Trauma Violence Abus. 2020, 31–44. [Google Scholar] [CrossRef]
- Stark, L.; Seff, I.; Reis, C. Gender-Based Violence against Adolescent Girls in Humanitarian Settings: A Review of the Evidence. Lancet Child Adolesc. Health 2020, 5, 210–222. [Google Scholar] [CrossRef]
- Coker, A.L.; Davis, K.E.; Arias, I.; Desai, S.; Sanderson, M.; Brandt, H.M.; Smith, P.H. Physical and Mental Health Effects of Intimate Partner Violence for Men and Women. Am. J. Prev. Med. 2002, 23, 260–268. [Google Scholar] [CrossRef]
- Campbell, J.C. Health Consequences of Intimate Partner Violence. Lancet 2002, 359, 1331–1336. [Google Scholar] [CrossRef]
- Grose, R.G.; Roof, K.A.; Semenza, D.C.; Leroux, X.; Yount, K.M. Mental Health, Empowerment, and Violence against Young Women in Lower-Income Countries: A Review of Reviews. Aggress. Violent Behav. 2019, 46, 25–36. [Google Scholar] [CrossRef]
- Grose, R.G.; Chen, J.S.; Roof, K.A.; Rachel, S.; Yount, K.M. Sexual and Reproductive Health Outcomes of Violence Against Women and Girls in Lower-Income Countries: A Review of Reviews. J. Sex Res. 2020, 1–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Classen, C.C.; Palesh, O.G.; Aggarwal, R. Sexual Revictimization. Trauma Violence Abus. 2005, 6, 103–129. [Google Scholar] [CrossRef]
- Logie, C.H.; Okumu, M.; Mwima, S.; Hakiza, R.; Irungi, K.P.; Kyambadde, P.; Kironde, E.; Narasimhan, M. Social Ecological Factors Associated with Experiencing Violence among Urban Refugee and Displaced Adolescent Girls and Young Women in Informal Settlements in Kampala, Uganda: A Cross-Sectional Study. Confl. Health 2019, 13, 60. [Google Scholar] [CrossRef]
- Kohli, A.; Perrin, N.; Mpanano, R.M.; Banywesize, L.; Mirindi, A.B.; Banywesize, J.H.; Mitima, C.M.; Binkurhorhwa, A.K.; Bufole, N.M.; Glass, N. Family and Community Driven Response to Intimate Partner Violence in Post-Conflict Settings. Soc. Sci. Med. 2015, 146, 276–284. [Google Scholar] [CrossRef] [Green Version]
- Panter-Brick, C. Conflict, Violence, and Health: Setting a New Interdisciplinary Agenda. Soc. Sci. Med. 2010, 1–6. [Google Scholar] [CrossRef]
- Rios-Avila, F.; Canavire-Bacarreza, G.J. The Effect of Intimate Partner Violence on Labor Market Decisions: Evidence from a Multi-Ethnic Country. Int. J. Soc. Econ. 2017, 44, 75–92. [Google Scholar] [CrossRef]
- Swanberg, J.E.; Logan, T.K.; Macke, C. Intimate Partner Violence, Employment, and The Workplace: Consequences and Future Directions. Trauma Violence Abus. 2005, 6, 286–312. [Google Scholar] [CrossRef]
- Dalal, K.; Dawad, S. Economic Costs of Domestic Violence: A Community Study in South Africa. HealthMED 2011, 5, 1931–1940. [Google Scholar]
- Lince-Deroche, N.; Berry, K.M.; Hendrickson, C.; Sineke, T.; Kgowedi, S.; Mulongo, M. Women’s Costs for Accessing Comprehensive Sexual and Reproductive Health Services: Findings from an Observational Study in Johannesburg, South Africa. Reprod. Health 2019, 16, 179. [Google Scholar] [CrossRef]
- Abramsky, T.; Watts, C.H.; Garcia-Moreno, C.; Devries, K.; Kiss, L.; Ellsberg, M.; Jansen, H.A.; Heise, L. What Factors Are Associated with Recent Intimate Partner Violence? Findings from the WHO Multi-Country Study on Women’s Health and Domestic Violence. BMC Public Health 2011, 11, 109. [Google Scholar] [CrossRef] [Green Version]
- Fulu, E.; Miedema, S.; Roselli, T.; McCook, S.; Chan, K.L.; Haardörfer, R.; Jewkes, R.; Fulu, E.; Jewkes, R.; Warner, X.; et al. Pathways between Childhood Trauma, Intimate Partner Violence, and Harsh Parenting: Findings from the UN Multi-Country Study on Men and Violence in Asia and the Pacific. Lancet Glob. Health 2017, 5, e512–e522. [Google Scholar] [CrossRef] [Green Version]
- Jewkes, R. Intimate Partner Violence: Causes and Prevention. Lancet Lond. Engl. 2002, 359, 1423–1429. [Google Scholar] [CrossRef]
- Krug, E.G.; Mercy, J.A.; Dahlberg, L.L.; Zwi, A.B. The World Report on Violence and Health. Lancet 2002, 360, 1083–1088. [Google Scholar] [CrossRef] [Green Version]
- United Nations. United Nations Security Council Resolution 1325 on Women, Peace and Security Understanding the Implications, Fulfilling the Obligations; United Nations: New York, NY, USA, 2000. [Google Scholar]
- Pinheiro, P.S. World Report on Violence against Children; UN: Geneva, Switzerland, 2009. [Google Scholar]
- Bundhamcharoen, K.; Odton, P.; Mugem, S.; Phulkerd, S.; Dhisayathikom, K.; Brown, D.W.; Tangcharoensathien, V. Costs of Injuries Due to Interpersonal and Self-Directed Violence in Thailand. J. Med. Assoc. Thai. 2005, 91, S110–S118. [Google Scholar]
- Raghavendra, S.; Duvvury, N.; Ashe, S. The Macroeconomic Loss Due to Violence against Women: The Case of Vietnam. Fem. Econ. 2017, 23, 62–89. [Google Scholar] [CrossRef]
- Roldós, M.I.; Corso, P. The Economic Burden of Intimate Partner Violence in Ecuador: Setting the Agenda for Future Research and Violence Prevention Policies. West. J. Emerg. Med. 2013, 14, 347–353. [Google Scholar] [CrossRef]
- Heise, L.L. Violence against Women: An Integrated, Ecological Framework. Violence Woman 1998, 4, 262–290. [Google Scholar] [CrossRef]
- Cislaghi, B.; Heise, L. Using Social Norms Theory for Health Promotion in Low-Income Countries. Health Promot. Int. 2019, 34, 616–623. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. BMJ 2009, 332–336. [Google Scholar] [CrossRef] [Green Version]
- WHO. WHO Multi-Country Study on Women’s Health and Domestic Violence against Women; World Health Organization: Geneva, Switzerland, 2005. [Google Scholar]
- United Nations Office for the Coordination of Humanitarian Affairs. Financial Tracking System. Available online: https://fts.unocha.org/ (accessed on 17 December 2020).
- Downes, M.J.; Brennan, M.L.; Williams, H.C.; Dean, R.S. Development of a Critical Appraisal Tool to Assess the Quality of Cross-Sectional Studies (AXIS). BMJ Open 2016, 6, e011458. [Google Scholar] [CrossRef] [Green Version]
- Goessmann, K.; Ibrahim, H.; Neuner, F. Association of War-Related and Gender-Based Violence With Mental Health States of Yazidi Women. JAMA Netw. Open 2020, 3, e2013418. [Google Scholar] [CrossRef] [PubMed]
- Al-Atrushi, H.H.; Al-Tawil, N.G.; Shabila, N.P.; Al-Hadithi, T.S. Intimate Partner Violence against Women in the Erbil City of the Kurdistan Region, Iraq. BMC Womens Health 2013, 13, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zakar, R.; Zakar, M.Z.; Mikolajczyk, R.; Krämer, A. Intimate Partner Violence and Its Association with Women’s Reproductive Health in Pakistan. Int. J. Gynaecol. Obstet. 2012, 117, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Zakar, R.; Zakar, M.Z.; Mikolajczyk, R.; Kraemer, A. Spousal Violence against Women and Its Association with Women’s Mental Health in Pakistan. Health Care Women Int. 2013, 34, 795–813. [Google Scholar] [CrossRef]
- Sousa, C.; Yacoubian, K.; Flaherty Fischette, P.; Haj-Yahia, M.M. The Co-Occurrence and Unique Mental Health Effects of Political Violence and Intimate Partner Violence. J. Interpers. Violence 2018, 33, 268–292. [Google Scholar] [CrossRef]
- Falb, K.L.; Blackwell, A.; Stennes, J.; Hussein, M.; Annan, J. Depressive Symptoms among Women in Raqqa Governorate, Syria: Associations with Intimate Partner Violence, Food Insecurity, and Perceived Needs. Glob. Ment. Health Camb. Engl. 2019, 6, e22. [Google Scholar] [CrossRef] [Green Version]
- Fiorentino, M.; Sagaon-Teyssier, L.; Ndiaye, K.; Suzan-Monti, M.; Mengue, M.-T.; Vidal, L.; Kuaban, C.; March, L.; Laurent, C.; Spire, B.; et al. Intimate Partner Violence against HIV-Positive Cameroonian Women: Prevalence, Associated Factors and Relationship with Antiretroviral Therapy Discontinuity—Results from the ANRS-12288 EVOLCam Survey. Womens Health 2019, 15, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Peltzer, K.; Pengpid, S. Female Genital Mutilation and Intimate Partner Violence in the Ivory Coast. BMC Womens Health 2014, 14, 13. [Google Scholar] [CrossRef] [Green Version]
- Alenko, A.; Girma, S.; Abera, M.; Workicho, A. Children Emotional and Behavioural Problems and Its Association with Maternal Depression in Jimma Town, Southwest Ethiopia. Gen. Psychiatry 2020, 33. [Google Scholar] [CrossRef]
- Gebreslasie, K.Z.; Weldemariam, S.; Gebre, G.; Mehari, M.-A. Intimate Partner Violence during Pregnancy and Risk of Still Birth in Hospitals of Tigray Region Ethiopia. Ital. J. Pediatr. 2020, 46, 107. [Google Scholar] [CrossRef]
- Sipsma, H.; Callands, T.A.; Bradley, E.; Harris, B.; Johnson, B.; Hansen, N.B. Healthcare Utilisation and Empowerment among Women in Liberia. J. Epidemiol. Community Health 2013, 67, 953–959. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sobkoviak, R.M.; Yount, K.M.; Halim, N. Domestic Violence and Child Nutrition in Liberia. Soc. Sci. Med. 2012, 74, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Hayes, B.; van Baak, C. Risk Factors of Physical and Sexual Abuse for Women in Mali: Findings from a Nationally Representative Sample. Violence Women 2017, 23, 1361–1381. [Google Scholar] [CrossRef] [PubMed]
- DeLong, S.M.; Brooks, M.I.; Aliou, S.; Lundgren, R.; Corneliess, C.; Johns, N.E.; Challa, S.; Carter, N.; Lauro, G.; Silverman, J.G. Married Very Young Adolescent Girls in Niger at Greatest Risk of Lifetime Male Partner Reproductive Coercion and Sexual Violence. PLoS ONE 2020, 15, 30231392. [Google Scholar] [CrossRef]
- Silverman, J.G.; Challa, S.; Boyce, S.C.; Averbach, S.; Raj, A. Associations of Reproductive Coercion and Intimate Partner Violence with Overt and Covert Family Planning Use among Married Adolescent Girls in Niger. EClinicalMedicine 2020, 22, 100393. [Google Scholar] [CrossRef] [PubMed]
- Kana, M.A.; Safiyan, H.; Yusuf, H.E.; Musa, A.S.M.; Richards-Barber, M.; Harmon, Q.E.; London, S.J. Association of Intimate Partner Violence during Pregnancy and Birth Weight among Term Births: A Cross-Sectional Study in Kaduna, Northwestern Nigeria. BMJ Open 2020, 10. [Google Scholar] [CrossRef] [PubMed]
- Abiodun, O.; Sodeinde, K.; Bamidele, F.; Ojinni, Y.; Adekeye, J.; Ohiaogu, F.; Mbonu, F. Intimate Partner Violence among Women Accessing HIV-Care Services at Tertiary Hospitals in Ogun State, Nigeria: Implications for Policy and Practice. J. Interpers. Violence 2020, 1–21. [Google Scholar] [CrossRef]
- Kidman, R.; Palermo, T.; Bertrand, J. Intimate Partner Violence, Modern Contraceptive Use and Conflict in the Democratic Republic of the Congo. Soc. Sci. Med. 2015, 133, 2–10. [Google Scholar] [CrossRef]
- Fleming, P.J.; McCleary-Sills, J.; Morton, M.; Levtov, R.; Heilman, B.; Barker, G. Risk Factors for Men’s Lifetime Perpetration of Physical Violence against Intimate Partners: Results from the International Men and Gender Equality Survey (IMAGES) in Eight Countries. PLoS ONE 2015, 10, e0118639. [Google Scholar] [CrossRef]
- Johnson, K.; Scott, J.; Rughita, B.; Kisielewski, M.; Asher, J.; Ong, R.; Lawry, L. Association of Sexual Violence and Human Rights Violations with Physical and Mental Health in Territories of the Eastern Democratic Republic of the Congo. JAMA J. Am. Med. Assoc. 2010, 304, 553–562. [Google Scholar] [CrossRef] [Green Version]
- Gichane, M.W.; Moracco, K.E.; Thirumurthy, H.; Okitolonda, E.W.; Behets, F.; Yotebieng, M. Intimate Partner Violence and Prevention of Mother to Child Transmission of HIV: Evidence from Kinshasa, Democratic Republic of Congo. PLoS ONE 2018, 13, e0203471. [Google Scholar] [CrossRef]
- Tiruneh, F.N.; Chuang, K.Y.; Ntenda, P.A.M.; Chuang, Y.C. Unwanted Pregnancy, Pregnancy Loss, and Other Risk Factors for Intimate Partner Violence in the Democratic Republic of the Congo. Women Health 2018, 58, 983–1000. [Google Scholar] [CrossRef]
- Mpody, C.; Thompson, P.; Tabala, M.; Ravelomanana, N.L.R.; Malongo, F.; Kawende, B.; Behets, F.; Okitolonda, E.; Yotebieng, M. Hepatitis B Infection among Pregnant and Post-Partum Women Living with HIV and on Antiretroviral Therapy in Kinshasa, DR Congo: A Cross-Sectional Study. PLoS ONE 2019, 14, e0216293. [Google Scholar] [CrossRef] [Green Version]
- Onsomu, E.O.; Abuya, B.A.; Okech, I.N.; Rosen, D.L.; Duren-Winfield, V.; Simmons, A.C. Association between Domestic Violence and HIV Serostatus among Married and Formerly Married Women in Kenya. Health Care Women Int. 2015, 36, 205–228. [Google Scholar] [CrossRef] [Green Version]
- Shi, C.; Kouyoumdjian, F.G.; Dushoff, J. Intimate Partner Violence Is Associated with HIV Infection in Women in Kenya: A Cross-Sectional Analysis. BMC Public Health 2013, 13, 512. [Google Scholar] [CrossRef] [Green Version]
- Seff, I.; Stark, L. A Sex-Disaggregated Analysis of How Emotional Violence Relates to Suicide Ideation in Low- and Middle-Income Countries. Child Abus. Negl. 2019, 93, 222–227. [Google Scholar] [CrossRef]
- Phillips-Howard, P.A.; Otieno, G.; Burmen, B.; Otieno, F.; Odongo, F.; Odour, C.; Nyothach, E.; Amek, N.; Zielinski-Gutierrez, E.; Odhiambo, F.; et al. Menstrual Needs and Associations with Sexual and Reproductive Risks in Rural Kenyan Females: A Cross-Sectional Sehavioral Survey Linked with HIV Prevalence. J. Womens Health 2015, 24, 801–811. [Google Scholar] [CrossRef]
- Kinuthia, J.; Singa, B.; McGrath, C.J.; Odeny, B.; Langat, A.; Katana, A.; Ng’ang’a, L.; Pintye, J.; John-Stewart, G. Prevalence and Correlates of Non-Disclosure of Maternal HIV Status to Male Partners: A National Survey in Kenya. BMC Public Health 2018, 18, 671. [Google Scholar] [CrossRef] [PubMed]
- Goyette, M.; Mutiti, P.; Bukusi, D.; Wamuti, B.M.; Otieno, F.A.; Cherutich, P.; Golden, M.R.; Spiegel, H.; Richardson, B.A.; Ng’ang’a, A.; et al. HIV Assisted Partner Services among Those with and without a History of Intimate Partner Violence in Kenya. J. Acquir. Immune Defic. Syndr. 2018, 78, 16–19. [Google Scholar] [CrossRef] [PubMed]
- Wagman, J.A.; Charvat, B.; Thoma, M.E.; Ndyanabo, A.; Nalugoda, F.; Ssekasanvu, J.; Kigozi, G.; Serwadda, D.; Kagaayi, J.; Wawer, M.J.; et al. Intimate Partner Violence as a Predictor of Marital Disruption in Rural Rakai, Uganda: A Longitudinal Study. Int. J. Public Health 2016, 61, 961–970. [Google Scholar] [CrossRef] [PubMed]
- Kouyoumdjian, F.G.; Calzavara, L.M.; Bondy, S.J.; O’Campo, P.; Serwadda, D.; Nalugoda, F.; Kagaayi, J.; Kigozi, G.; Wawer, M.; Gray, R. Intimate Partner Violence Is Associated with Incident HIV Infection in Women in Uganda. AIDS Lond. Engl. 2013, 27, 1331–1338. [Google Scholar] [CrossRef] [PubMed]
- Speizer, I.S. Intimate Partner Violence Attitudes and Experience among Women and Men in Uganda. J. Interpers. Violence 2010, 25, 1224–1241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macucha, C.M.; Taunde, S.A. Domestic Homicide in Maputo Province, Mozambique. Forensic Sci. Int. Online 2020, 2, 157–161. [Google Scholar] [CrossRef]
- Adjiwanou, V.; N’Bouke, A. Exploring the Paradox of Intimate Partner Violence and Increased Contraceptive Use in Sub-Saharan Africa. Stud. Fam. Plann. 2015, 46, 127–142. [Google Scholar] [CrossRef]
- Shamu, S.; Zarowsky, C.; Roelens, K.; Temmerman, M.; Abrahams, N. High-Frequency Intimate Partner Violence during Pregnancy, Postnatal Depression and Suicidal Tendencies in Harare, Zimbabwe. Gen. Hosp. Psychiatry 2016, 38, 109–114. [Google Scholar] [CrossRef] [Green Version]
- Shamu, S.; Munjanja, S.; Zarowsky, C.; Shamu, P.; Temmerman, M.; Abrahams, N. Intimate Partner Violence, Forced First Sex and Adverse Pregnancy Outcomes in a Sample of Zimbabwean Women Accessing Maternal and Child Health Care. BMC Public Health 2018, 18, 595. [Google Scholar] [CrossRef] [PubMed]
- Nyamukoho, E.; Mangezi, W.; Marimbe, B.; Verhey, R.; Chibanda, D. Depression among HIV Positive Pregnant Women in Zimbabwe: A Primary Health Care Based Cross-Sectional Study. BMC Pregnancy Childbirth 2019, 19, 53. [Google Scholar] [CrossRef]
- Kayibanda, J.F.; Alary, M. Trends and Risk Factors Associated with the Perpetration of Physical Intimate Partner Violence by Women in Haiti, 2000–2012. Women Health 2020, 60, 12–25. [Google Scholar] [CrossRef] [PubMed]
- Gage, A.J. Exposure to Spousal Violence in the Family, Attitudes and Dating Violence Perpetration among High School Students in Port-Au-Prince. J. Interpers. Violence 2016, 31, 2445–2474. [Google Scholar] [CrossRef]
- Saxena, A.; Deschamps, M.; Dorvil, N.; Christophe, I.; Rosenberg, R.; Jean-Gilles, M.; Koenig, S.; Pape, J.W.; Dévieux, J.G. Association between Intimate Partner Violence and HIV Status among Haitian Women. Glob. Public Health 2019, 14, 1557–1568. [Google Scholar] [CrossRef] [PubMed]
- Occean, J.R.; Thomas, N.; Lim, A.C.; Lovett, S.M.; Michael-Asalu, A.; Salinas-Miranda, A.A. Prevalence and Factors Associated with Intimate Partner Violence among Women in Haiti: Understanding Household, Individual, Partner, and Relationship Characteristics. J. Interpers. Violence 2020, 1–29. [Google Scholar] [CrossRef]
- Zalla, L.C.; Herce, M.E.; Edwards, J.K.; Michel, J.; Weir, S.S. The Burden of HIV among Female Sex Workers, Men Who Have Sex with Men and Transgender Women in Haiti: Results from the 2016 Priorities for Local AIDS Control Efforts (PLACE) Study. J. Int. AIDS Soc. 2019, 22, e25281. [Google Scholar] [CrossRef]
- Bellizzi, S.; Nivoli, A.; Salaris, P.; Ronzoni, A.R.; Pichierri, G.; Palestra, F.; Wazway, O.; Luque-Fernandez, M.A. Sexual Violence and Eclampsia: Analysis of Data from Demographic and Health Surveys from Seven Low-and Middle-Income Countries. J. Glob. Health 2019, 9, 020434. [Google Scholar] [CrossRef]
- Gibbs, A.; Corboz, J.; Jewkes, R. Factors Associated with Recent Intimate Partner Violence Experience amongst Currently Married Women in Afghanistan and Health Impacts of IPV: A Cross Sectional Study. BMC Public Health 2018, 18, 593. [Google Scholar] [CrossRef] [Green Version]
- Aye, W.T.; Lien, L.; Stigum, H.; Schei, B.; Sundby, J.; Bjertness, E. Domestic Violence Victimisation and Its Association with Mental Distress: A Cross-Sectional Study of the Yangon Region, Myanmar. BMJ Open 2020, 10, e037936. [Google Scholar] [CrossRef]
- Tsai, L.C.; Cappa, C.; Petrowski, N. The Relationship between Intimate Partner Violence and Family Planning among Girls and Young Women in the Philippines. Glob. J. Health Sci. 2016, 8, 121–131. [Google Scholar] [CrossRef]
- Falb, K.L.; McCormick, M.C.; Hemenway, D.; Anfinson, K.; Silverman, J.G. Symptoms Associated with Pregnancy Complications along the Thai-Burma Border: The Role of Conflict Violence and Intimate Partner Violence. Matern. Child Health J. 2014, 18, 29–37. [Google Scholar] [CrossRef]
- Fellmeth, G.; Plugge, E.; Fazel, M.; Oo, M.M.; Pimanpanarak, M.; Phichitpadungtham, Y.; Wai, K.; Charunwatthana, P.; Simpson, J.A.; Nosten, F.; et al. Prevalence and Determinants of Perinatal Depression among Labour Migrant and Refugee Women on the Thai-Myanmar Border: A Cohort Study. BMC Psychiatry 2020, 20, 168. [Google Scholar] [CrossRef] [Green Version]
- Gibbs, A.; Said, N.; Corboz, J.; Jewkes, R. Factors Associated with ‘Honour Killing’ in Afghanistan and the Occupied Palestinian Territories: Two Cross-Sectional Studies. PLoS ONE 2019, 14, e0219125. [Google Scholar] [CrossRef] [Green Version]
- Misch, E.S.; Yount, K.M. Intimate Partner Violence and Breastfeeding in Africa. Matern. Child Health J. 2014, 18, 688–697. [Google Scholar] [CrossRef]
- Gámez, A.M.; Speizer, I.S. Community-Level Intimate Partner Violence and the Circumstances of First Sex among Young Women from Five African Countries. Reprod. Health 2010, 7, 11. [Google Scholar] [CrossRef] [Green Version]
- Bermudez, L.G.; Stark, L.; Bennouna, C.; Jensen, C.; Potts, A.; Kaloga, I.F.; Tilus, R.; Buteau, J.E.; Marsh, M.; Hoover, A.; et al. Converging Drivers of Interpersonal Violence: Findings from a Qualitative Study in Post-Hurricane Haiti. Child Abuse Negl. 2019, 89, 178–191. [Google Scholar] [CrossRef]
- Marsh, M.; Blake, M. Where Is the Money? How the Humanitarian System Is Failing in Its Commitments to End Violence against Women and Girls; IRC. 2019. Available online: https://www.rescue.org/report/wheres-money-how-humanitarian-system-failing-fund-end-violence-against-women-and-girls (accessed on 10 June 2019).
- Schölmerich, V.L.N.; Kawachi, I. Translating the Socio-Ecological Perspective into Multilevel Interventions: Gaps between Theory and Practice. Health Educ. Behav. 2016, 43, 17–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Golden, S.D.; McLeroy, K.R.; Green, L.W.; Earp, J.A.L.; Lieberman, L.D. Upending the Social Ecological Model to Guide Health Promotion Efforts toward Policy and Environmental Change. Health Educ. Behav. 2015, 42 (Suppl. 1), 8S–14S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- IASC. IASC System-Wide Response Activations and Deactivations. Available online: https://interagencystandingcommittee.org/iasc-transformative-agenda/iasc-system-wide-response-activations-and-deactivations (accessed on 21 December 2020).
- ACAPS. INFORM Global Crisis Severity Index: Guidance Note; ACAPS: Geneva, Switzerland, 2020. [Google Scholar]
- UNGA. Transforming Our World: The 2030 Agenda for Sustainable Development; UNGA: New York, NY, USA, 2015. [Google Scholar]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).