
Precautionary Behaviors during the Second and Third Phases of the COVID-19 Pandemic: Comparative Study in the Latin American Population

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
- Information about COVID-19—five questions to establish the levels of information about COVID-19, satisfaction with public information, and primary sources of information (e. g. “public information about COVID-19 has been”, “my satisfaction with the information received from experts has been”). A 5-point Likert scale was used to answer, from “none” = 1 to “a lot” = 5. Additionally, when asked about their main source of information (“my main source of information has been”), participants could answer “internet”, “television”, “radio”, “family members”, “other, which one?”
- Concerns related to COVID-19—nine questions about the levels of concern caused by issues such as medical and institutional resources and training, the possibility of becoming ill or having family members become ill, the possibility of dying, and the loss of financial resources (e.g., “I am concerned about hospital’s resources to take care of the ill”, “I am concerned about the likelihood of getting infected during the current outbreak”, “I am concerned about the likelihood of being hospitalized”). A 5-point Likert scale was used to answer, from “none” = 1 to “a lot” = 5.
- Precautionary measures during COVID-19—seven questions on following the recommendations of authorities and experts, the use of masks, hand washing, and maintenance of social distancing, among others (e.g., “covering my mouth when coughing and sneezing”, “avoiding sharing utensils (e. g. fork)”, “washing my hands with soap and water”, “wearing mask regardless of the presence or absence of symptoms”). A 5-point Likert scale was used to answer, from “never” = 1 to “always” = 5.
- Maintenance of confinement—four questions on compliance with the home confinement established by the authorities (e.g., “maintenance of confinement”, “time spent in home confinement”, “I have had to go out to work and interact with other people”, “maintenance of activities”). A 5-point Likert scale was used to answer, from “I have been away from home all the time” = 1 to “I have not been out at all” = 5.
- Medical symptoms—participants were asked about the presence of COVID-19-related symptoms in the 14 days prior to the survey, including: fever, cold, headache, muscle pain, cough, shortness of breath, dizziness, rhinitis, and sore throat. Presence of chronic illness, medical consultation in the past 14 days, quarantine in the past 14 days, and indirect contact with and individual with confirmed COVID-19 infection were collected as data.
2.1. Ethical Considerations
2.2. Statistical Analysis
3. Results
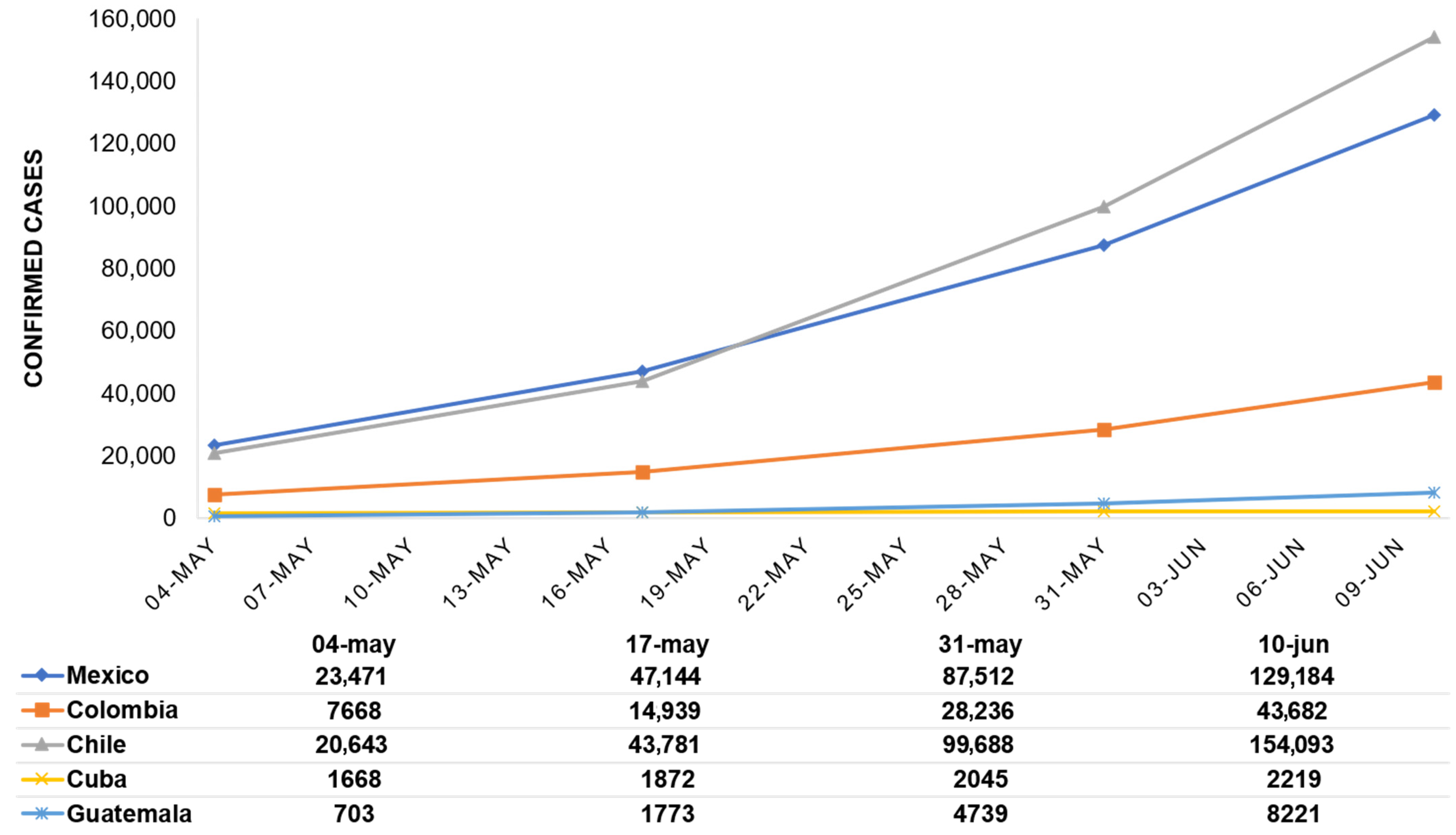
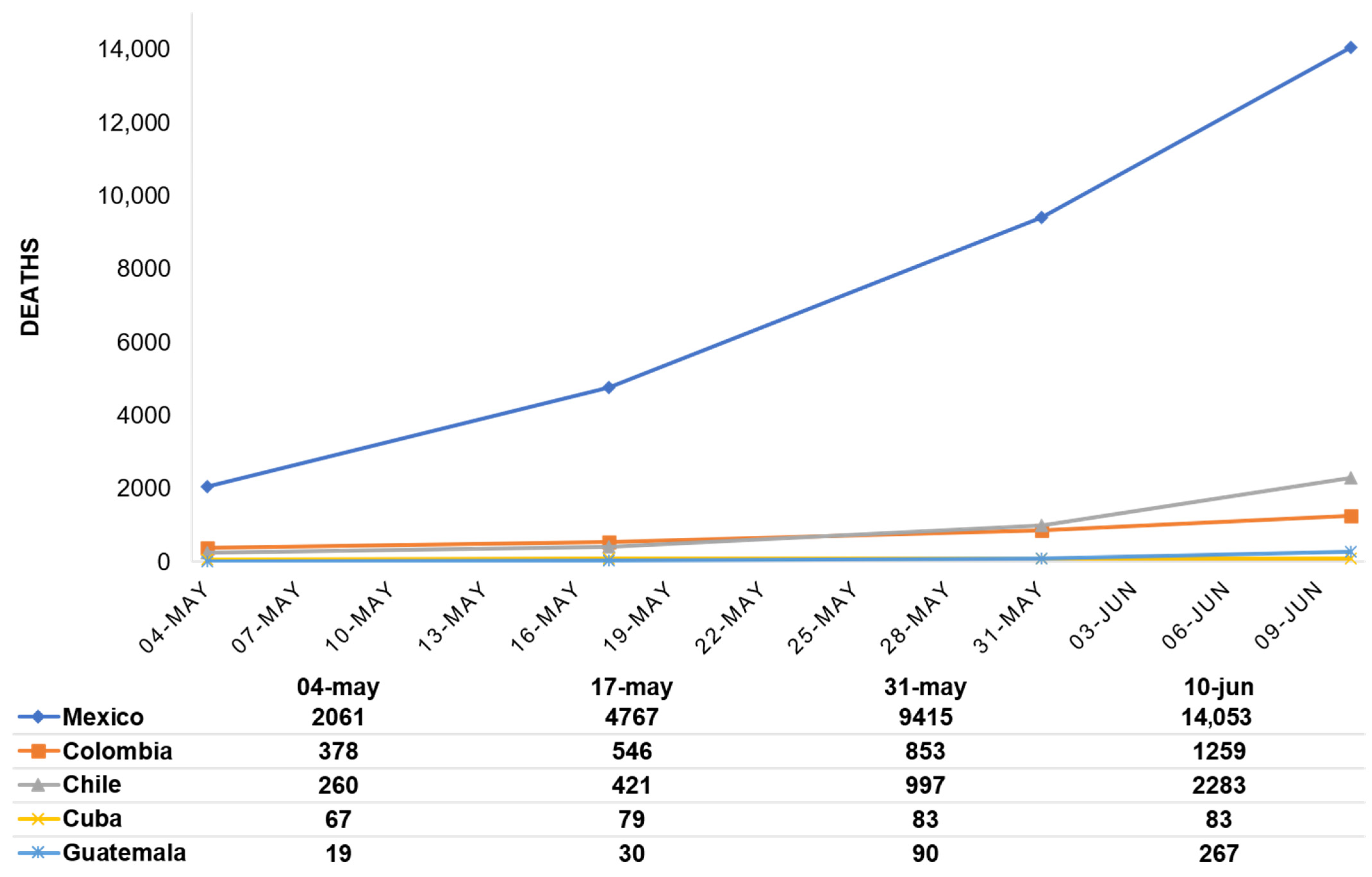
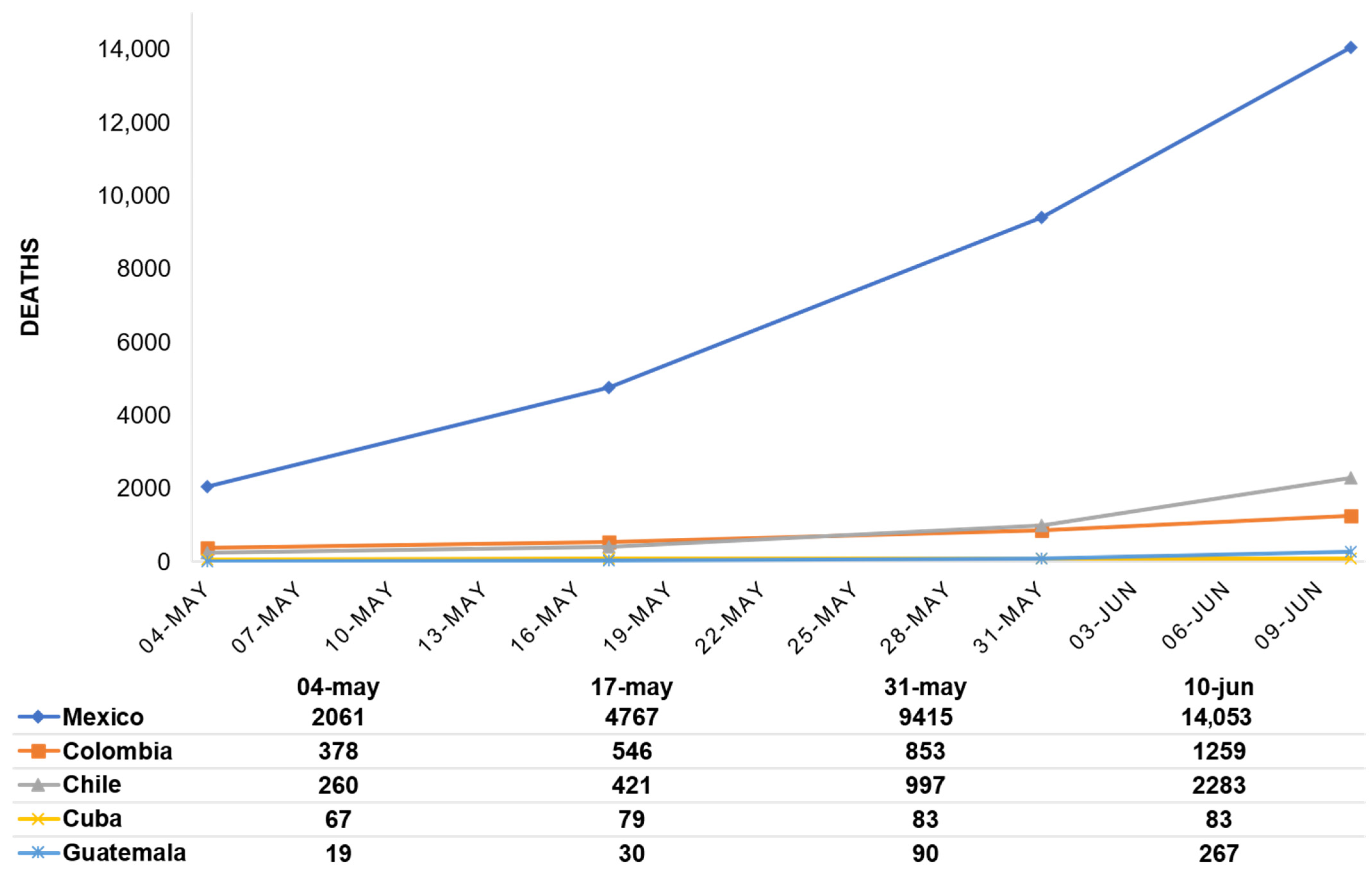
3.1. Development of the COVID-19 Pandemic in the five Latin American Countries during the Data Collection Period
3.2. Description of the Populations
3.3. Information about COVID-19
3.4. COVID-19-Related Concerns
3.5. Precautionary Behaviors
3.6. Maintenance of Confinement
3.7. Comparative Analysis by Medical Symptoms
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gámez, A.S. Resiliencia y Covid 19. Rev. Colomb. Obstet. Ginecol. 2020, 71, 7–8. [Google Scholar] [CrossRef]
- Pablos-Méndez, A.; Vega, J.; Aranguren, F.P.; Tabish, H.; Raviglione, M.C. Covid-19 in Latin America. BMJ 2020, 370. [Google Scholar] [CrossRef]
- St. Victor, G.S.; Ahmed, S. The importance of culture in managing mental health response to pandemics. In Psychiatry of Pandemics. A Mental Health Response to Infection Outbreak; Huremović, D., Ed.; Springer: Manhasset, NY, USA, 2019. [Google Scholar]
- Shinan-Altman, S.; Levkovich, I. COVID-19 precautionary behavior: The Israeli case in the initial stage of the outbreak. BMC Public Health 2020, 20, 1–7. [Google Scholar] [CrossRef]
- Clements, J.M. Knowledge and Behaviors Toward COVID-19 Among US Residents During the Early Days of the Pandemic: Cross-Sectional Online Questionnaire. JMIR Public Health Surveill. 2020, 6, e19161. [Google Scholar] [CrossRef]
- Bao, Y.; Sun, Y.; Meng, S.; Shi, J.; Lu, L. 2019-nCoV epidemic: Address mental health care to empower society. Lancet 2020, 395, e37–e38. [Google Scholar] [CrossRef] [Green Version]
- Pfattheicher, S.; Nockur, L.; Böhm, R.; Sassenrath, C.; Petersen, M.B. The Emotional Path to Action: Empathy Promotes Physical Distancing and Wearing of Face Masks During the COVID-19 Pandemic. Psychol. Sci. 2020, 31, 1363–1373. [Google Scholar] [CrossRef] [PubMed]
- Dong, L.; Bouey, J. Public Mental Health Crisis during COVID-19 Pandemic, China. Emerg. Infect. Dis. 2020, 26, 1616–1618. [Google Scholar] [CrossRef] [PubMed]
- Jovančević, A.; Milićević, N. Optimism-pessimism, conspiracy theories and general trust as factors contributing to COVID-19 related behavior—A cross-cultural study. Pers. Individ. Differ. 2020, 167, 110216. [Google Scholar] [CrossRef]
- Wood, M.J. Propagating and Debunking Conspiracy Theories on Twitter during the 2015–2016 Zika Virus Outbreak. Cyberpsychol. Behav. Soc. Netw. 2018, 21, 485–490. [Google Scholar] [CrossRef] [PubMed]
- Han, Q.; Curtis, D.R. Suspicious minds: Cinematic depiction of distrust during epidemic disease outbreaks. Med. Humanit. 2020. [Google Scholar] [CrossRef]
- Wilder-Smith, A.; Freedman, D.O. Isolation, quarantine, social distancing and community containment: Pivotal role for old-style public health measures in the novel coronavirus (2019-nCoV) outbreak. J. Travel Med. 2020, 27. [Google Scholar] [CrossRef] [PubMed]
- Lima, C.K.T.; Carvalho, P.M.D.M.; Lima, I.D.A.A.S.; Nunes, J.V.A.D.O.; Saraiva, J.S.; de Souza, R.I.; da Silva, C.G.L.; Neto, M.L.R. The emotional impact of Coronavirus 2019-nCoV (new Coronavirus disease). Psychiatry Res. 2020, 287, 112915. [Google Scholar] [CrossRef]
- Xin, M.; Luo, S.; She, R.; Yu, Y.; Li, L.; Wang, S.; Ma, L.; Tao, F.; Zhang, J.; Zhao, J.; et al. Negative cognitive and psychological correlates of mandatory quarantine during the initial COVID-19 outbreak in China. Am. Psychol. 2020, 75, 607–617. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Acosta, L.D. Capacidad de respuesta frente a la pandemia de COVID-19 en América Latina y el Caribe [Response capacity to the COVID-19 pandemic in Latin America and the Caribbean]. Rev. Panam. Salud Pública 2020, 44, 109. [Google Scholar] [CrossRef]
- Secretaria de Salud. Medidas de Seguridad Sanitaria. Available online: https://www.gob.mx/salud/documentos/medidas-de-seguridad-sanitaria-239275 (accessed on 31 March 2020).
- Secretaria de Salud. Nuevo Coronavirus en el mundo COVID-19. Comunicado Técnico Diario. Available online: https://www.gob.mx/salud/prensa/nuevo-coronavirus-en-el-mundo-covid-19-comunicado-tecnico-diario-244654 (accessed on 10 June 2020).
- MINSAL, Chilean Ministry of Health. Cifras Oficiales COVID-19. Available online: https://s3.amazonaws.com/gobcl-prod/public_files/Campa%C3%B1as/Corona-Virus/Reportes/10.06.2020_Reporte_Covid19 (accessed on 10 June 2020).
- Burki, T. COVID-19 in Latin America. Lancet Infect. Dis. 2020, 20, 547–548. [Google Scholar] [CrossRef]
- Shadmi, E.; Chen, Y.; Dourado, I.; Faran-Perach, I.; Furler, J.; Hangoma, P.; Hanvoravongchai, P.; Obando, C.; Petrosyan, V.; Rao, K.D.; et al. Health equity and COVID-19: Global perspectives. Int. J. Equity Health 2020, 19, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Salud Pública y Asistencia Social. Situación de COVID-10 en Guatemala. Available online: https://tablerocovid.mspas.gob.gt/ (accessed on 10 June 2020).
- Ministerio de Salud Colombia. Colombia Confirma su Primer Caso. Available online: https://www.minsalud.gov.co/Paginas/Colombia-confirma-su-primer-caso-de-COVID-19.aspx (accessed on 10 June 2020).
- Pérez Riverol, A. The Cuban Strategy for Combatting the COVID-19 Pandemic. MEDICC Rev. 2020, 22, 64–68. [Google Scholar]
- Eysenbach, G. Improving the quality of Web surveys: The Checklist for reporting results of internet E-Surveys (CHERRIES). J. Med. Internet Res. 2004, 6, e34. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, R.; Flint, J. Accessing Hidden and Hard-to-reach Populations: Snowball Research Strategies. Soc. Res. Update 2001, 33, 1–4. [Google Scholar]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [Green Version]
- Leung, G.; Lam, T.-H.; Ho, L.-M.; Ho, S.-Y.; Chan, B.H.Y.; Wong, I.O.L.; Hedley, A.J. The impact of community psychological responses on outbreak control for severe acute respiratory syndrome in Hong Kong. J. Epidemiol. Community Health 2003, 57, 857–863. [Google Scholar] [CrossRef] [Green Version]
- Mak, W.W.; Law, R.W.; Woo, J.; Cheung, F.M.; Lee, D. Social support and psychological adjustment to SARS: The mediating role of self-care self-efficacy. Psychol. Health 2009, 24, 161–174. [Google Scholar] [CrossRef] [PubMed]
- Rubin, G.J.; Potts, H.W.W.; Michie, S. The impact of communications about swine flu (influenza A H1N1v) on public responses to the outbreak: Results from 36 national telephone surveys in the UK. Health Technol. Assess. 2010, 14, 183–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum: Hillsdale, MI, USA; Hove, UK, 1988. [Google Scholar]
- WHO coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/table (accessed on 24 June 2021).
- Espinosa, A.A.; Sarmiento-Ardila, J.A. COVID-19: Implicaciones en Colombia. Gac. Med. Mex. 2020, 156, 334–338. [Google Scholar] [CrossRef]
- Ríos-González, C.; Palacios, J.M. Trabajo de Investigación de la FCM—UNCA—Conocimientos, Actitudes y Prácticas sobre el COVID-19 de los Paraguayos. Facultad de Ciencias Médicas de la UNCA. Available online: https://cienciasdelsur.com/2020/04/30/covid-19-hay-mucha-ansiedad-y-depresion-segun-universidad-de-caaguazu-e-ins/ (accessed on 31 March 2020).
- Dagnino, P.; Anguita, V.; Escobar, K.; Cifuentes, S. Psychological Effects of Social Isolation Due to Quarantine in Chile: An Exploratory Study. Front. Psychiatry 2020, 11, 591142. [Google Scholar] [CrossRef]
- Garcia, P.J.; Alarcón, A.; Bayer, A.; Buss, P.; Guerra, G.; Ribeiro, H.; Rojas, K.; Saenz, R.; De Snyder, N.S.; Solimano, G.; et al. COVID-19 Response in Latin America. Am. J. Trop. Med. Hyg. 2020, 103, 1765–1772. [Google Scholar] [CrossRef] [PubMed]
- Haq, S.U.; Shahbaz, P.; Boz, I. Knowledge, behavior and precautionary measures related to COVID-19 pandemic among the general public of Punjab province, Pakistan. J. Infect. Dev. Ctries. 2020, 14, 823–835. [Google Scholar] [CrossRef]
- Alkhamees, A.A.; Alrashed, S.A.; Alzunaydi, A.A.; Almohimeed, A.S.; Aljohani, M.S. The psychological impact of COVID-19 pandemic on the general population of Saudi Arabia. Compr. Psychiatry 2020, 102, 152192. [Google Scholar] [CrossRef]
- Arafat, S.M.Y.; Kar, S.K.; Kabir, R. Editorial: Panic Buying: Human Psychology and Environmental Influence. Front. Public Health 2021, 9. [Google Scholar] [CrossRef]
- Arafat, S.Y.; Kar, S.K.; Menon, V.; Marthoenis, M.; Sharma, P.; Alradie-Mohamed, A.; Mukherjee, S.; Kaliamoorthy, C.; Kabir, R. Media portrayal of panic buying: A content analysis of online news portals. Glob. Psychiatry 2020, 1. [Google Scholar] [CrossRef]
- Urzua, A.; Vera-Villarroel, P.; Caqueo-Urízar, A.; Polanco-Carrasco, R. La psicología en la prevención y manejo del COVID-19. Aportes desde la Evid. Inicial. Ter. Psicológica 2020, 38, 103–118. [Google Scholar] [CrossRef]
- Basch, C.H.; Hillyer, G.C.; Erwin, Z.M.; Mohlman, J.; Cosgrove, A.; Quinones, N. News coverage of the COVID-19 pandemic: Missed opportunities to promote health sustaining behaviors. Infect. Dis. Health 2020, 25, 205–209. [Google Scholar] [CrossRef] [PubMed]
- Fernández, M.E.; McCurdy, S.A.; Arvey, S.R.; Tyson, S.K.; Morales-Campos, D.; Flores, B.; Useche, B.; Mitchell-Bennett, L.; Sanderson, M. HPV knowledge, attitudes, and cultural beliefs among Hispanic men and women living on the Texas–Mexico border. Ethn. Health 2009, 14, 607–624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pakpour, A.H.; Griffiths, M.D. The fear of COVID-19 and its role in preventive behaviors. J. Concurr. Disord. 2020, 2, 58–63. Available online: http://irep.ntu.ac.uk/id/eprint/39561/ (accessed on 31 March 2020).
- Taghrir, M.H.; Borazjani, R.; Shiraly, R. COVID-19 and Iranian Medical Students; A Survey on Their Related-Knowledge, Preventive Behaviors and Risk Perception. Arch. Iran. Med. 2020, 23, 249–254. [Google Scholar] [CrossRef] [Green Version]
- Muto, K.; Yamamoto, I.; Nagasu, M.; Tanaka, M.; Wada, K. Japanese citizens’ behavioral changes and preparedness against COVID-19: An online survey during the early phase of the pandemic. PLoS ONE 2020, 15, e0234292. [Google Scholar] [CrossRef]
- Idrovo, A.J. Long but Unreal Lockdowns in Latin America. Comment on Chen, Y.T.; Yen, Y.F.; Yu, S.H.; Su, E.C. An Examination on the Transmission of COVID-19 and the Effect of Response Strategies: A Comparative Analysis. Int. J. Environ. Res. Public Health 2020, 17, E5687. Int. J. Environ. Res. Public Health 2020, 17, 8064. [Google Scholar] [CrossRef]
- Elorrio, E.G.; Arrieta, J.; Arce, H.; Delgado, P.; Malik, A.M.; Villagran, C.O.; Rincon, S.; Sarabia, O.; Tono, T.; Hermida, J.; et al. The COVID-19 pandemic: A call to action for health systems in Latin America to strengthen quality of care. Int. J. Qual. Health Care 2021, 33. [Google Scholar] [CrossRef]
- Alonso-Galbán, P.; Alemañy-Castilla, C. Curbing Misinformation and Disinformation in the COVID-19 Era: A View from Cuba. MEDICC Rev. 2020, 22, 45–46. [Google Scholar]
- Hossain, M.A.; Jahid, I.K.; Hossain, K.M.A.; Walton, L.M.; Uddin, Z.; Haque, O.; Kabir, F.; Arafat, S.M.Y.; Sakel, M.; Faruqui, R.; et al. Knowledge, attitudes, and fear of COVID-19 during the Rapid Rise Period in Bangladesh. PLoS ONE 2020, 15, e0239646. [Google Scholar] [CrossRef] [PubMed]
- Iorfa, S.K.; Ottu, I.F.A.; Oguntayo, R.; Ayandele, O.; Kolawole, S.O.; Gandi, J.C.; Dangiwa, A.L.; Olapegba, P.O. COVID-19 Knowledge, Risk Perception, and Precautionary Behavior Among Nigerians: A Moderated Mediation Approach. Front. Psychol. 2020, 11, 566773. [Google Scholar] [CrossRef]
- MacKenzie, J.S.; Smith, D.W. COVID-19: A novel zoonotic disease caused by a coronavirus from China: What we know and what we don’t. Microbiol. Aust. 2020, 41, 45. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, D.B.; Aggleton, J.P.; Chakrabarti, B.; Cooper, C.; Creswell, C.; Dunsmuir, S.; Fiske, S.T.; Gathercole, S.; Gough, B.; Ireland, J.L.; et al. Research priorities for the COVID-19 pandemic and beyond: A call to action for psychological science. Br. J. Psychol. 2020, 111, 603–629. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Variable | Mexico (n = 680) | Colombia (n = 149) | Chile (n = 128) | Cuba (n = 106) | Guatemala (n = 120) | χ2 | V |
|---|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | n (%) | |||
| Gender | |||||||
| Women | 474 (69.70) | 120 (80.50) | 91 (71.10) | 61 (57.00) | 92 (76.70) | 19.06 *** | 0.127 |
| Men | 206 (30.30) | 29 (19.50) | 37 (28.90) | 46 (43.00) | 28 (23.30) | ||
| Relationships | |||||||
| In a stable relationship | 433 (63.68) | 73 (49.00) | 75 (58.60) | 62 (58.50) | 74 (61.67) | 23.80 ** | 0.100 |
| In an unstable relationship | 33 (4.85) | 7 (4.70) | 11 (8.60) | 8 (7.50) | 0 (0.00) | ||
| Single | 214 (31.47) | 69 (46.3) | 42 (32.80) | 36 (34.00) | 46 (38.33) | ||
| Family members older than 60 years | |||||||
| Yes | 537 (79.00) | 112 (75.20) | 96 (75.00) | 66 (61.70) | 99 (82.50) | 18.19 *** | 0.124 |
| No | 143 (21.00) | 37 (24.80) | 32 (25.00) | 41 (38.30) | 21 (17.50) | ||
| Children | |||||||
| Has children under 16 years | 192 (28.20) | 38 (26.00) | 42 (32.80) | 28 (26.20) | 45 (37.50) | 68.70 *** | 0.170 |
| Has children over 16 years | 162 (23.80) | 9 (6.00) | 23 (18.00) | 43 (40.20) | 39 (32.50) | ||
| No children | 326 (48.00) | 102 (68.00) | 63 (49.20) | 36 (33.60) | 36 (30.00) | ||
| Educational level | |||||||
| Basic education | 77 (11.30) | 80 (53.69) | 25 (21.09) | 54 (50.50) | 31 (25.80) | 332.45 *** | 0.265 |
| Bachelor´s degree | 320 (47.10) | 32 (22.82) | 72 (56.25) | 52 (48.60) | 51 (42.50) | ||
| Master´s degree or higher | 283 (41.60) | 33 (23.49) | 28 (22.66) | 1 (0.90) | 38 (31.70) | ||
| Occupation | |||||||
| Student | 134 (19.71) | 85 (57.05) | 50 (39.06) | 9 (8.49) | 11 (9.17) | 423.48 *** | 0.314 |
| Professor | 179 (26.32) | 23 (15.44) | 18 (14.06) | 9 (8.49) | 11 (9.17) | ||
| Administrative employee | 104 (15.30) | 27 (18.12) | 14 (10.94) | 14 (13.21) | 23 (19.16) | ||
| Other occupations | 234 (34.41) | 11 (7.38) | 40 (31.25) | 7 (6.60) | 35 (29.17) | ||
| Unemployed | 29 (4.26) | 3 (2.01) | 6 (4.69) | 0 (0.00) | 0 (0.00) | ||
| No answer | 0 (0.00) | 0 (0.00) | 0 (0.00) | 67 (63.21) | 40 (33.33) |
| Variable | Mexico | Colombia | Chile | Cuba | Guatemala | F | η2p |
|---|---|---|---|---|---|---|---|
| M ± DT | M ± DT | M ± DT | M ± DT | M ± DT | |||
| Level of information | 2.85 ± 0.90 | 2.68 ± 0.93 | 2.99 ± 0.95 | 3.84 ± 0.83 | 2.88 ± 0.89 | 31.21 ** | 0.096 |
| Search of information | 2.50 ± 1.09 | 2.52 ± 1.08 | 2.56 ± 1.24 | 3.38 ± 1.07 | 2.46 ± 1.13 | 15.44 ** | 0.050 |
| Public information | 2.72 ± 1.00 | 2.87 ± 0.90 | 2.71 ± 1.10 | 4.01 ± 0.92 | 2.59 ± 1.15 | 40.63 ** | 0.121 |
| Satisfaction with the information | 1.43 ± 0.99 | 1.41 ± 0.77 | 1.55 ± 1.04 | 2.69 ± 1.11 | 1.53 ± 1.10 | 6.66 ** | 0.022 |
| Variable | Mexico | Colombia | Chile | Cuba | Guatemala | F | η2p |
|---|---|---|---|---|---|---|---|
| M ± DT | M ± DT | M ± DT | M ± DT | M ± DT | |||
| Concerns about doctor´s resources to diagnose | 3.17 ± 0.91 | 2.87 ± 1.04 | 3.34 ± 0.71 | 2.33 ± 1.21 | 3.09 ± 0.95 | 22.63 ** | 0.071 |
| Concerns about hospital´s resources to take care of the ill | 3.34 ± 0.86 | 3.13 ± 1.01 | 3.54 ± 0.60 | 2.41 ± 1.25 | 3.46 ± 0.76 | 31.07 ** | 0.095 |
| Likelihood of getting infected during the current outbreak | 2.20 ± 0.93 | 2.17 ± 1.01 | 2.48 ± 0.93 | 2.42 ± 1.21 | 2.23 ± 0.92 | 3.30 * | 0.011 |
| Likelihood of being hospitalized | 1.98 ± 0.96 | 2.13 ± 1.01 | 2.23 ± 1.05 | 2.28 ± 1.22 | 2.21 ± 1.06 | 3.95 * | 0.013 |
| Likelihood of die because of COVID-19 infection | 1.81 ± 0.95 | 1.99 ± 1.03 | 2.00 ± 1.09 | 2.24 ± 1.28 | 1.80 ± 0.96 | 5.26 ** | 0.018 |
| Concerns about other family members getting COVID-19 infection | 2.80 ± 1.10 | 2.89 ± 1.03 | 3.09 ± 0.97 | 2.95 ± 1.14 | 2.75 ± 1.11 | 2.43 * | 0.008 |
| Concerns about older family members getting COVID-19 infection | 2.93 ± 1.12 | 2.93 ± 1.10 | 3.28 ± 0.94 | 2.83 ± 1.24 | 2.89 ± 1.09 | 6.46 * | 0.011 |
| Concerns about losing important economic resources | 2.20 ± 1.17 | 2.25 ± 1.16 | 2.16 ± 1.20 | 1.61 ± 1.13 | 2.21 ± 1.13 | 6.46 ** | 0.021 |
| Concerns about losing the job | 1.86 ± 1.17 | 1.98 ± 1.22 | 2.01 ± 1.21 | 1.37 ± 0.93 | 1.84 ± 1.10 | 5.57 ** | 0.019 |
| Variable | Mexico | Colombia | Chile | Cuba | Guatemala | F | η2p |
|---|---|---|---|---|---|---|---|
| M ± DT | M ± DT | M ± DT | M ± DT | M ± DT | |||
| Covering my mouth when coughing and sneezing | 3.64 ± 0.73 | 3.36 ± 0.88 | 3.48 ± 0.83 | 3.56 ± 0.84 | 3.59 ± 0.76 | 4.55 ** | 0.015 |
| Avoiding sharing of utensils (e.g., fork) | 3.19 ± 1.21 | 2.66 ± 1.45 | 3.14 ± 1.18 | 3.27 ± 1.31 | 3.31 ± 1.12 | 6.58 ** | 0.022 |
| Washing my hands with soap and water | 3.50 ± 0.83 | 3.21 ± 1.00 | 3.47 ± 0.76 | 3.42 ± 1.01 | 3.55 ± 0.84 | 3.93 * | 0.013 |
| Wearing mask regardless of the presence or absence of symptoms | 1.83 ± 1.47 | 2.85 ± 1.31 | 3.27 ± 1.05 | 3.70 ± 0.73 | 3.43 ± 1.01 | 93.18 ** | 0.241 |
| Wearing protection gloves | 0.75 ± 1.11 | 1.62 ± 1.43 | 1.48 ± 1.38 | 0.82 ± 1.44 | 1.08 ± 1.33 | 21.29 ** | 0.068 |
| Washing my hands immediately after touching contaminated objects | 3.44 ± 0.96 | 3.41 ± 0.95 | 3.56 ± 0.78 | 3.34 ± 1.04 | 3.68 ± 0.71 | 2.69 * | 0.009 |
| Keeping distance from other people | 3.33 ± 0.91 | 3.38 ± 0.86 | 3.62 ± 0.64 | 3.42 ± 0.88 | 3.61 ± 0.73 | 4.89 ** | 0.016 |
| Variable | Mexico | Colombia | Chile | Cuba | Guatemala | F | η2p |
|---|---|---|---|---|---|---|---|
| M ± DT | M ± DT | M ± DT | M ± DT | M ± DT | |||
| Maintenance of confinement | 2.86 ± 0.62 | 3.02 ± 0.62 | 2.88 ± 0.66 | 2.97 ± 0.93 | 2.73 ± 0.73 | 3.92 * | 0.013 |
| Confinement time | 3.39 ± 0.64 | 3.68 ± 0.67 | 3.45 ± 0.67 | 3.26 ± 0.78 | 2.97 ± 0.95 | 18.17 ** | 0.058 |
| Restriction of interaction at work | 2.93 ± 0.85 | 3.15 ± 0.83 | 2.99 ± 0.87 | 2.24 ± 0.93 | 2.86 ± 0.84 | 19.42 ** | 0.062 |
| Restriction of exits | 3.13 ± 0.56 | 3.30 ± 0.55 | 3.17 ± 0.57 | 3.21 ± 0.63 | 3.03 ± 0.72 | 4.22 * | 0.014 |
| Variable | Mexico n (%) | Colombia n (%) | Chile n (%) | Cuba n (%) | Guatemala n (%) | χ2 | V |
|---|---|---|---|---|---|---|---|
| Medical symptoms | |||||||
| None | 385 (56.62) | 69 (46.31) | 48 (37.50) | 95 (88.79) | 83 (69.17) | 82.31 ** | 0.186 |
| 1–3 | 262 (38.53) | 71 (47.65) | 66 (51.56) | 12 (11.21) | 32 (26.67) | ||
| 4–7 | 33 (4.85) | 9 (6.04) | 14 (10.94) | 0 (0.00) | 5 (4.16) | ||
| Chronic illness | |||||||
| Yes | 141 (20.74) | 29 (19.46) | 37 (28.91) | 40 (37.38) | 27 (22.50) | 214.35 ** | 0.425 |
| No | 539 (79.26) | 120 (80.54) | 91 (71.19) | 67 (62.62) | 93 (77.50) | ||
| Medical consultation in the past 14 days | |||||||
| Yes | 93 (13.68) | 16 (10.74) | 14 (10.94) | 3 (2.80) | 11 (9.16) | 11.81 * | 0.100 |
| No | 587 (86.32) | 133 (89.26) | 114 (89.16) | 104 (97.20) | 109 (90.84) | ||
| Quarantine in the past 14 days | |||||||
| Yes | 136 (20.00) | 31 (20.81) | 21 (16.41) | 0 (0.00) | 5 (4.26) | 42.82 ** | 0.190 |
| No | 544 (80.00) | 118 (79.29) | 107 (83.59) | 107 (100.00) | 115 (95.84) | ||
| Indirect contact with an individual with confirmed COVID-19 infection. | |||||||
| Yes | 33 (4.85) | 2 (1.34) | 8 (6.25) | 0 (0.00) | 6 (5.00) | 10.09 * | 0.092 |
| No | 647 (95.15) | 147 (98.76) | 120 (93.75) | 107 (100.00) | 114 (95.00) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meda-Lara, R.M.; Juárez-Rodríguez, P.; Carrasco-Tapias, N.E.; Barrales-Díaz, C.R.; Palomera-Chávez, A.; González-Díaz, E.; Llantá-Abreu, M.d.C.; Lorenzana-Montenegro, L.; Herrero, M.; Moreno-Jiménez, B. Precautionary Behaviors during the Second and Third Phases of the COVID-19 Pandemic: Comparative Study in the Latin American Population. Int. J. Environ. Res. Public Health 2021, 18, 6882. https://doi.org/10.3390/ijerph18136882
Meda-Lara RM, Juárez-Rodríguez P, Carrasco-Tapias NE, Barrales-Díaz CR, Palomera-Chávez A, González-Díaz E, Llantá-Abreu MdC, Lorenzana-Montenegro L, Herrero M, Moreno-Jiménez B. Precautionary Behaviors during the Second and Third Phases of the COVID-19 Pandemic: Comparative Study in the Latin American Population. International Journal of Environmental Research and Public Health. 2021; 18(13):6882. https://doi.org/10.3390/ijerph18136882
Chicago/Turabian StyleMeda-Lara, Rosa Martha, Pedro Juárez-Rodríguez, Nayib Ester Carrasco-Tapias, Claudio Rodolfo Barrales-Díaz, Andrés Palomera-Chávez, Esteban González-Díaz, María del Carmen Llantá-Abreu, Lucia Lorenzana-Montenegro, Marta Herrero, and Bernardo Moreno-Jiménez. 2021. "Precautionary Behaviors during the Second and Third Phases of the COVID-19 Pandemic: Comparative Study in the Latin American Population" International Journal of Environmental Research and Public Health 18, no. 13: 6882. https://doi.org/10.3390/ijerph18136882
APA StyleMeda-Lara, R. M., Juárez-Rodríguez, P., Carrasco-Tapias, N. E., Barrales-Díaz, C. R., Palomera-Chávez, A., González-Díaz, E., Llantá-Abreu, M. d. C., Lorenzana-Montenegro, L., Herrero, M., & Moreno-Jiménez, B. (2021). Precautionary Behaviors during the Second and Third Phases of the COVID-19 Pandemic: Comparative Study in the Latin American Population. International Journal of Environmental Research and Public Health, 18(13), 6882. https://doi.org/10.3390/ijerph18136882