
Validation of the Psychometric Properties of the Practice Environment Scale of Nursing Work Index in Primary Health Care in Portugal


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Method
2.2.1. Data Collection and Procedure
2.2.2. Participants
2.3. Analysis
2.4. Ethical Considerations
3. Results
3.1. Exploratory Factor Analysis
3.2. Reliability Analysis
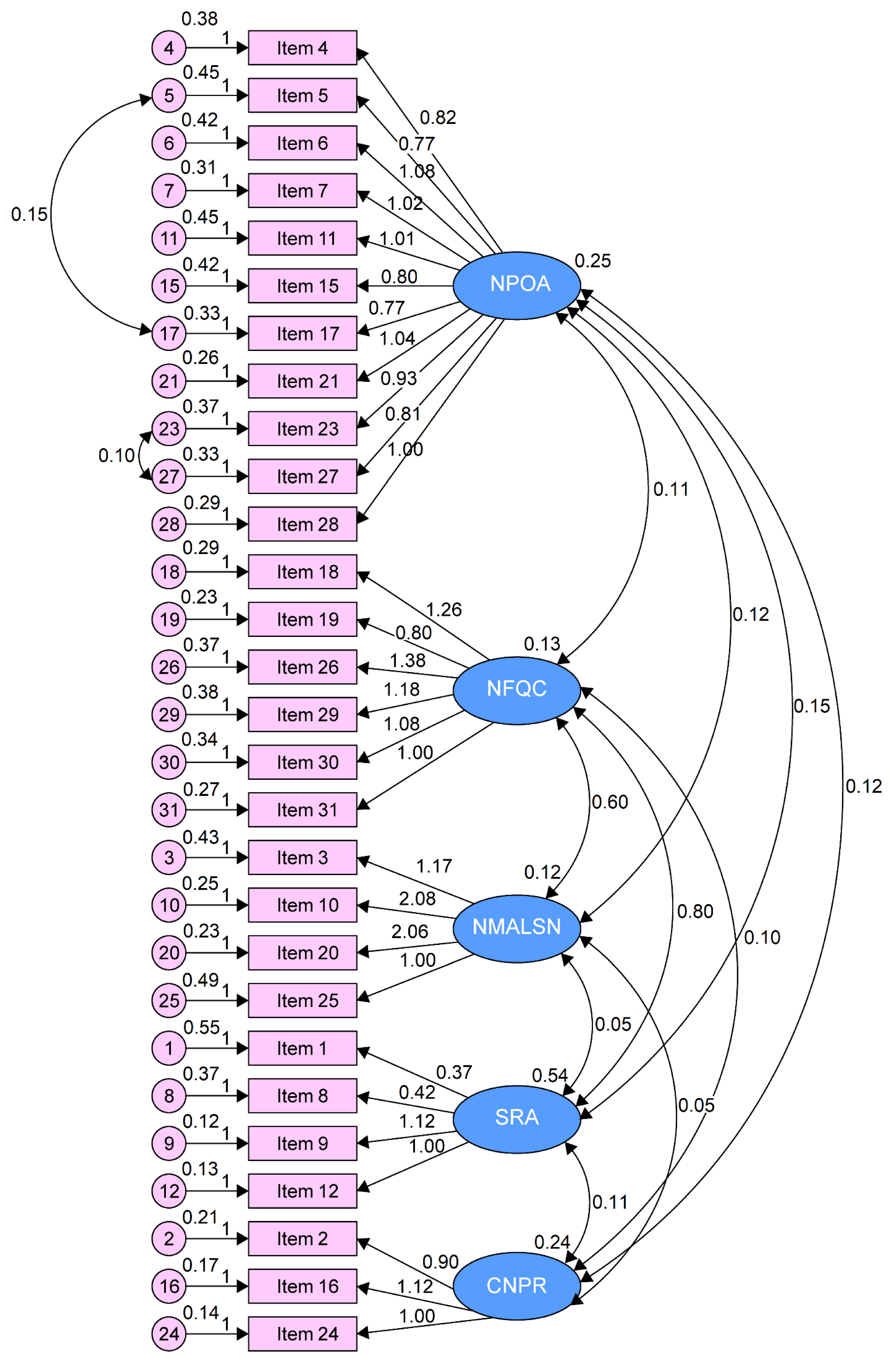
3.3. Confirmatory Factor Analysis
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lucas, P.R.M.B.; Nunes, E.M.G.T. Nursing practice environment in Primary Health Care: A scoping review. Rev. Bras. Enferm. 2020, 73, e20190479. [Google Scholar] [CrossRef] [PubMed]
- McSherry, R.; Pearce, P.; Grimwood, K.; McSherry, W. The pivotal role of nurse managers, leaders and educators in enabling excellence in nursing care. J. Nurs. Manag. 2012, 20, 7–19. [Google Scholar] [CrossRef] [PubMed]
- Parro-Moreno, A.; Serrano-Gallardo, P.; Ferrer-Arnedo, C.; Serrano-Molina, L.; Puerta-Calatayud, M.L.; Barberá-Martín, A.; De Pedro-Gómez, J. Influence of socio-demographic, labour and professional factors on nursing perception concerning practice environment in Primary Health Care. Aten. Primaria 2013, 45, 476–485. [Google Scholar] [CrossRef] [PubMed]
- Poghosyan, L.; Shang, J.; Liu, J.; Poghosyan, H.; Liu, N.; Berkowitz, B. Nurse practitioners as primary care providers: Creating favorable practice environments in New York State and Massachusetts. Health Care Manag. Rev. 2015, 40, 46–55. [Google Scholar] [CrossRef]
- Lake, E.T. Development of the practice environment scale of the nursing work index. Res. Nurs. Health 2002, 25, 176–188. [Google Scholar] [CrossRef]
- Almeida, S.; Nascimento, A.; Lucas, P.B.; Jesus, E.; Araújo, B. RN4CAST study in Portugal: Validation of the portuguese version of the Practice Environment Scale of the Nursing Work Index. Aquichan 2020, 20, 1–10. [Google Scholar] [CrossRef]
- Carvalho, M.C.; Lucas, P. The effectiveness of the clinical nurse leader practice—Systematic review. Millenium 2020, 2, 57–64. [Google Scholar] [CrossRef]
- De Sul, S.I.R.; Lucas, P.R.M.B. Translation and validation of the anticipated turnover scale for the Portuguese cultural context. Nurs. Open. 2020, 7, 1475–1481. [Google Scholar] [CrossRef]
- Tomaszewska, K.; Kłos, A.; Majchrowicz, B. Influence of work environment on the quality of benefits provided by primary health care nurses. J. Educ. Health Sport 2017, 7, 1191–1205. [Google Scholar]
- Leone, C.; Bruyneel, L.; Anderson, J.E.; Murrells, T.; Dussault, G.; Jesus, E.H.; Rafferty, A.M. Work environment issues and intention-to-leave in Portuguese nurses: A cross-sectional study. Health Polic. 2015, 119, 1584–1592. [Google Scholar] [CrossRef]
- Alves, D.F.S.; Guirardello, E.B. Ambiente de trabalho da enfermagem, segurança do paciente e qualidade do cuidado pediátrico. Rev. Gaúcha Enferm. 2016, 37, 1–7. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Copanitsanou, P.; Fotos, N.; Brokalaki, H. Effects of work environment on patient and nurse outcomes. Br. J. Nurs. 2017, 26, 172–176. [Google Scholar] [CrossRef]
- Gea-Caballero, V.; Castro-Sánchez, E.; Júarez-Vela, R.; Díaz-Herrera, M.Á.; Miguel-Montoya, I.; Martínez-Riera, J.R. Elementos esenciales de los entornos profesionales enfermeros en Atención Primaria y su influencia en la calidad del cuidado. Enferm. Clin. 2018, 28, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Weber, E.; Ward, J.; Walsh, T. Nurse leader competencies: A toolkit for success. Nurs. Manag. 2015, 46, 47–50. [Google Scholar] [CrossRef]
- Nunes, E.; Gaspar, M. A liderança em enfermagem e a satisfação dos pacientes em contexto hospitalar. Rev. Gaucha Enferm. 2016, 37. [Google Scholar] [CrossRef][Green Version]
- Lake, E.T. Measurement and Evidence. Med. Care Res. Rev. 2007, 64, 104S–122S. [Google Scholar] [CrossRef]
- Neves, T.M.A.; Parreira, P.M.S.D.; Graveto, J.M.G.N.; Rodrigues, V.J.L.; Marôco, J.P. Practice environment scale of the nursing work index: Portuguese version and psychometric properties. J. Nurs. Manag. 2018, 1–9. [Google Scholar] [CrossRef]
- Swiger, P.A.; Raju, D.; Breckenridge-Sproat, S.; Patrician, P.A. Adaptation of the Practice Environment Scale for military nurses: A psychometric analysis. J. Adv. Nurs. 2017, 73, 2219–2236. [Google Scholar] [CrossRef] [PubMed]
- Amaral, A.F.S.; Ferreira, P.L.; Lake, E. Validation of the Practice Environment Scale of the Nursing Work Index (PES-NWI) for the Portuguese nurse population. Int. J. Caring Sci. 2012, 5, 280–288. [Google Scholar]
- Amaral, A.F.S.; Ferreira, P. Influência do ambiente da prática nos resultados dos cuidados de enfermagem. Rev. Investig. Enferm. 2013, 5, 66–74. [Google Scholar]
- Ferreira, M.R.S.C.F.; Amendoeira, J. Study of adaptation and validation of the Practice environment scale of the nursing work index for the Portuguese reality. Rev. Esc Enferm. USP 2014, 48, 690–697. [Google Scholar] [CrossRef] [PubMed]
- Jesus, E.H.; Roque, S.M.B.; Amaral, A.F.S. Estudo RN4CAST em Portugal: Ambientes da prática de enfermagem. Rev. Investig. Enferm. 2015, 13, 26–44. [Google Scholar]
- Pinto, A.; Jesus, E.; Mendes, A.; Fronteira, I. Estudo RN4CAST em Portugal: Work Engagement dos Enfermeiros. Rev Investig. Enferm. 2015, 10, 26–37. [Google Scholar]
- De Pedro-Gómez, J.; Morales-Asencio, J.M.; Sesé-Abad, S.; Bennasar-Veny, M.; Artigues-Vives, G.; Campaner, C.P. Entorno de práctica de los profesionales de enfermería y competencia para la incorporación de la evidencia a las decisiones: Situación en las Islas Baleares. Gac Sanit 2011, 25, 191–197. [Google Scholar] [CrossRef][Green Version]
- De Pedro-Gómez, J.; Morales-Asencio, J.M.; Sesé-Abad, A.; Bennasar-Veny, M.; Pericas-Beltran, J.; Miguélez-Chamorro, A. Psychometric testing of the Spanish version of the Practice Environment Scale of the Nursing Work Index in a primary healthcare context. J. Adv. Nurs. 2011, 68, 212–221. [Google Scholar] [CrossRef]
- Parro-Moreno, A.; Serrano-Gallardo, P.; Díaz-Holgado, A.; Aréjula-Torres, J.L.; Abraira, V.; Santiago-Pérez, I.M.; Morales-Asencio, J.M. Impact of primary care nursing workforce characteristics on the control of high-blood pressure: A multilevel analysis. BMJ Open 2015, 5, e009126. [Google Scholar] [CrossRef][Green Version]
- Pérez-Campos, M.A.; Sánchez-García, I.; Pancorbo-Hidalgo, P.L. Knowledge, Attitude and Use of Evidence-Based Practice among nurses active on the Internet. Investig. Educ. Enferm. 2014, 32, 451–460. [Google Scholar] [CrossRef]
- Rabie, T.; Coetzee, S.K.; Klopper, H.C. The nature of community health care centre practice environments in a province in South Africa. Afr. J. Nurs. Midwifery 2016, 18, 27–41. [Google Scholar] [CrossRef]
- Wang, Y.; Dong, W.; Mauk, K.; Li, P.; Wan, J.; Yang, G.; Hao, M. Nurses’ practice environment and their job satisfaction: A study on nurses caring for older adults in Shanghai. PLoS ONE 2015, 10, e0138035. [Google Scholar] [CrossRef]
- Warshawsky, N.E.; Havens, D.S. Global use of the Practice Environment Scale of the Nursing Work Index. Nurs. Res. 2011, 60, 17–31. [Google Scholar] [CrossRef]
- Gasparino, R.C.; Guirardello, E.B. Validation of the Practice Environment Scale to the Brazilian culture. J. Nurs. Manag. 2017, 25, 375–383. [Google Scholar] [CrossRef]
- Fuentelsaz-Gallego, C.; Moreno-Casbas, M.T.; González-Maria, E. Validation of the Spanish version of the questionnaire Practice Environment Scale of the Nursing Work Index. Int. J. Nurs. Stud. 2013, 50, 274–280. [Google Scholar] [CrossRef] [PubMed]
- McCusker, J.; Dendukuri, N.; Cardinal, L.; Laplante, J.; Bambonye, L. Nursing work environment and quality of care: Differences between units at the same hospital. Int. J. Health Care Qual. 2004, 17, 313–322. [Google Scholar] [CrossRef]
- Bruyneel, L.; Li, B.; Squires, A.; Spotbeen, S.; Meuleman, B.; Lesaffre, E.; Sermeus, W. Bayesian Multilevel MIMIC Modeling for Studying Measurement Invariance in Cross-group Comparisons. Med. Care 2017, 55(4), e25–e35. [Google Scholar] [CrossRef]
- Mainz, H.; Baernholdt, M.; Ramlau-Hansen, C.H.; Brink, O. Comparison of nurse practice environments in Denmark and the USA. Int. Nurs. Rev. 2015, 62, 479–488. [Google Scholar] [CrossRef]
- Brzyski, P.; Kózka, M.; Squires, A.; Brzostek, T. How factor analysis results may change due to country context. J. Nurs. Scholarsh 2016, 48, 598–607. [Google Scholar] [CrossRef]
- Gunnarsdottir, S.; Clarke, S.P.; Rafferty, A.M.; Nutbeam, D. Front-line management, staffing and nursedoctor relationships as predictors of nurse and patient outcomes. A survey of Icelandic hospital nurses. Int. J. Nurs. Stud. 2009, 46, 920–927. [Google Scholar] [CrossRef]
- Efstathiou, G.; Andreou, C.; Tsangari, H.; Dimitriadou, M.; Papastavrou, E. Adaptation and validation of the Cyprus version of the Practice Environment Scale of the Nursing Work Index: A methodological study. BMC Res. Notes 2018, 11, 791–797. [Google Scholar] [CrossRef] [PubMed]
- Chiang, H.Y.; Lin, S.Y. Psychometric testing of the Chinese version of nursing practice environment scale. J. Clin. Nurs. 2009, 18, 919–929. [Google Scholar] [CrossRef]
- Cho, E.; Choi, M.; Kim, E.Y.; Yoo, I.Y.; Lee, N.J. Construct validity and reliability of the Korean version of the practice environment scale of nursing work index for Korean nurses. J. Korean Acad. Nurs. Adm. 2011, 41, 325–332. [Google Scholar] [CrossRef] [PubMed]
- Parker, D.; Tuckett, A.; Eley, R.; Hegney, D. Construct validity and reliability of the Practice Environment Scale of the Nursing Work Index for Queensland nurses. Int. J. Nurs. Pract. 2010, 16, 352–358. [Google Scholar] [CrossRef]
- Alzate, L.C.; Bayer, G.L.; Squires, A. Validation of a Spanish version of the practice environment scale of the nursing work index in the Colombian context. Hisp Health Care Int. 2014, 12, 34–42. [Google Scholar] [CrossRef]
- Ogata, Y.; Nagano, M.; Akanuma, T. Translating “The Practice Environment Scale of the Nursing Work Index (PES-NWI)” in to Japanese. J. Sch. Nurs. 2008, 30, 19–24. [Google Scholar] [CrossRef]
- Almeida, S. Análise em Componentes Principais. In Estatística Aplicada à Investigação em Ciências da Saúde—Um Guia Com o SPSS; Lusodidacta: Loures, Portugal, 2017; pp. 141–153. [Google Scholar]
- Marôco, J. Análise Fatorial. In Análise de Equações Estruturais: Fundamentos teóricos, Software e Aplicações, 2nd ed.; ReportNumber: Pêro Pinheiro, Portugal, 2014; pp. 179–243. [Google Scholar]
- Stevens, J.P. Applied Multivariate Statistics for the Social Sciences, 5th ed.; Routledge Academic: Mahwah, NJ, USA, 2009. [Google Scholar]
- Alavi, M.; Visentin, D.C.; Thapa, D.K.; Hunt, G.E.; Watson, R.; Cleary, M. Exploratory factor analysis and principal component analysis in clinical studies: Which one should you use? J. Adv. Nurs. 2020, 76, 1886–1889. [Google Scholar] [CrossRef] [PubMed]
- Cutillo, L. Parametric and multivariate methods. In Encyclopedia of Bioinformatics and Computational Biology; Ranganathan, M., Gribskov, K., Nakai, S.C., Eds.; Elsevier: Cambridge, UK, 2019; pp. 738–746. [Google Scholar]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis, 8th ed.; Cengage Learning EMEA: Hampshire, UK, 2019. [Google Scholar]
- De Pedro-Gómez, J.; Morales-Asencio, J.M.; Sesé-Abad, S.; Bennasar-Veny, M.; Artigues-Vives, G.; Pericàs-Beltrán, J. Validación y adaptación al español de la escala del entorno de práctica enfermera del Nursing Work Index. Metas Enferm. 2009, 12, 65–73. [Google Scholar]
- Anzai, E.; Douglas, C.; Bonner, A. Nursing practice environment, quality of care and morale of hospital nurses in Japan. Nurs. Health Sci. 2014, 16, 171–178. [Google Scholar] [CrossRef]
- Liou, S.R.; Cheng, C.Y. Using the Practice Environment Scale of the Nursing Work Index on Asian nurses. Nurs. Res. 2009, 58, 218–225. [Google Scholar] [CrossRef]
- Middleton, S.; Griffiths, R.; Fernandez, R.; Smith, B. Nursing practice environment: How does one Australian hospital compare with magnet hospitals? Int. J. Nurs. Pract. 2008, 14, 366–372. [Google Scholar] [CrossRef]
- Ogata, Y.; Sasaki, M.; Yumoto, Y.; Yonekura, Y.; Nagano, M.; Kanda, K. Reliability and validity of the practice environment scale of the nursing work index for Japanese hospital nurses. Nurs. Open 2018, 5, 362–369. [Google Scholar] [CrossRef] [PubMed]
- Patrician, P.; Shang, J.; Lake, E. Organizational determinants of work outcomes and quality care ratings among Army Medical Department registered nurses. Res. Nurs. Health 2010, 33, 99–110. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| N | % | Mean | SD | |
|---|---|---|---|---|
| Gender | - | - | - | - |
| Female | 909 | 85.8 | - | - |
| Male | 150 | 14.2 | - | - |
| Academic Degree | - | - | - | - |
| Graduates | 1.047 | 98.9 | - | - |
| Bachelor’s | 12 | 1.1 | - | - |
| Specialists | - | - | - | - |
| Specialist nurses | 579 | 54.7 | - | - |
| Age | - | - | 43.5 | 7.9 |
| Years of nursing | - | - | 20.5 | 7.8 |
| ITEMS | COMPONENTS | ||||
|---|---|---|---|---|---|
| Nurse Participation in Organization Affairs | Nursing Foundations for Quality of Care | Nurse Manager Ability, Leadership, and Support of Nurses | Staffing and Resource Adequacy | Collegial Nurse–Physician Relations | |
| Item 4 | 0.51 | - | - | - | - |
| Item 5 | 0.67 | - | - | - | - |
| Item 6 | 0.67 | - | - | - | - |
| Item 7 | 0.57 | - | - | - | - |
| Item 11 | 0.44 | - | - | - | - |
| Item 15 | 0.53 | - | - | - | - |
| Item 17 | 0.67 | - | - | - | - |
| Item 21 | 0.58 | - | - | - | - |
| Item 23 | 0.64 | - | - | - | - |
| Item 27 | 0.59 | - | - | - | - |
| Item 28 | 0.52 | - | - | - | - |
| Item 18 | - | 0.45 | - | - | - |
| Item 19 | - | 0.52 | - | - | - |
| Item 26 | - | 0.59 | - | - | - |
| Item 29 | - | 0.69 | - | - | - |
| Item 30 | - | 0.67 | - | - | - |
| Item 31 | - | 0.76 | - | - | - |
| Item 3 | - | - | 0.53 | - | - |
| Item 10 | - | - | 0.83 | - | - |
| Item 20 | - | - | 0.79 | - | - |
| Item 25 | - | - | 0.41 | - | - |
| Item 1 | - | - | - | 0.49 | - |
| Item 8 | - | - | - | 0.59 | - |
| Item 9 | - | - | - | 0.87 | - |
| Item 12 | - | - | - | 0.87 | - |
| Item 2 | - | - | - | - | 0.80 |
| Item 16 | - | - | - | - | 0.81 |
| Item 24 | - | - | - | - | 0.76 |
| Explained Variance | 28.9 | 6.7 | 8 | 5.2 | 4.7 |
| Cronbach’s alpha | 0.87 | 0.76 | 0.74 | 0.75 | 0.81 |
| Components | Alpha | AVE |
|---|---|---|
| 1. Nurse Participation in Organization Affairs | 0.87 | 0.88 |
| 2. Nursing Foundations for Quality of Care | 0.76 | 1.28 |
| 3. Nurse Manager Ability, Leadership, and Support of Nurses | 0.74 | 2.75 |
| 4. Staffing and Resource Adequacy | 0.75 | 0.59 |
| 5. Collegial Nurse–Physician Relations | 0.81 | 1.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lucas, P.; Jesus, E.; Almeida, S.; Araújo, B. Validation of the Psychometric Properties of the Practice Environment Scale of Nursing Work Index in Primary Health Care in Portugal. Int. J. Environ. Res. Public Health 2021, 18, 6422. https://doi.org/10.3390/ijerph18126422
Lucas P, Jesus E, Almeida S, Araújo B. Validation of the Psychometric Properties of the Practice Environment Scale of Nursing Work Index in Primary Health Care in Portugal. International Journal of Environmental Research and Public Health. 2021; 18(12):6422. https://doi.org/10.3390/ijerph18126422
Chicago/Turabian StyleLucas, Pedro, Elvio Jesus, Sofia Almeida, and Beatriz Araújo. 2021. "Validation of the Psychometric Properties of the Practice Environment Scale of Nursing Work Index in Primary Health Care in Portugal" International Journal of Environmental Research and Public Health 18, no. 12: 6422. https://doi.org/10.3390/ijerph18126422
APA StyleLucas, P., Jesus, E., Almeida, S., & Araújo, B. (2021). Validation of the Psychometric Properties of the Practice Environment Scale of Nursing Work Index in Primary Health Care in Portugal. International Journal of Environmental Research and Public Health, 18(12), 6422. https://doi.org/10.3390/ijerph18126422