
Trends in Suicide Mortality in 10 Years around the Great East Japan Earthquake: Analysis of Evacuation and Non-Evacuation Areas in Fukushima Prefecture




Abstract
1. Introduction
2. Materials and Methods
3. Results
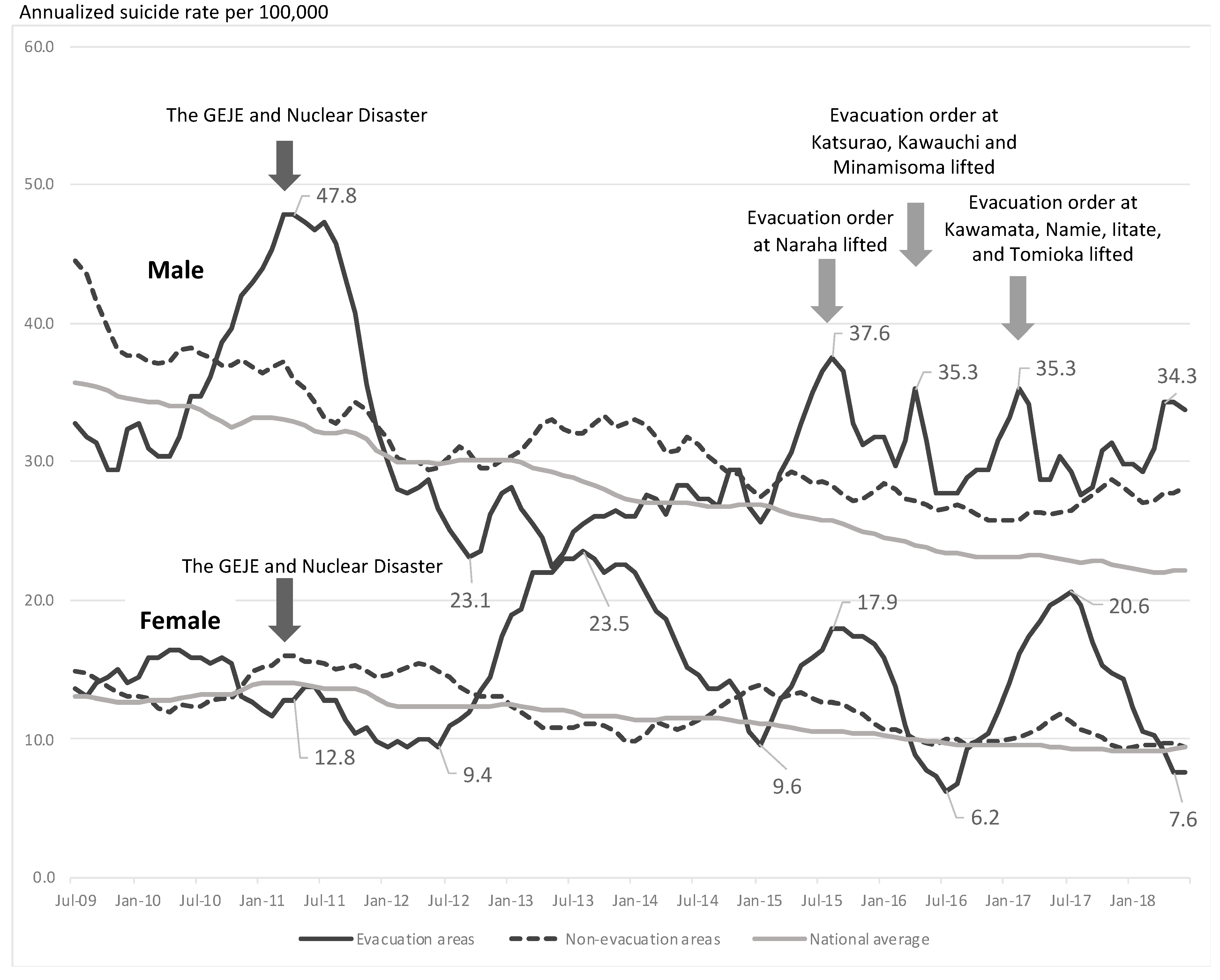
3.1. Changes in Suicide Rates in Evacuation and Non-Evacuation Areas by the Exponential Smoothing Time Series Model
3.2. Analysis of Suicide Rates by Age Categories in Evacuation and Non-Evacuation Areas
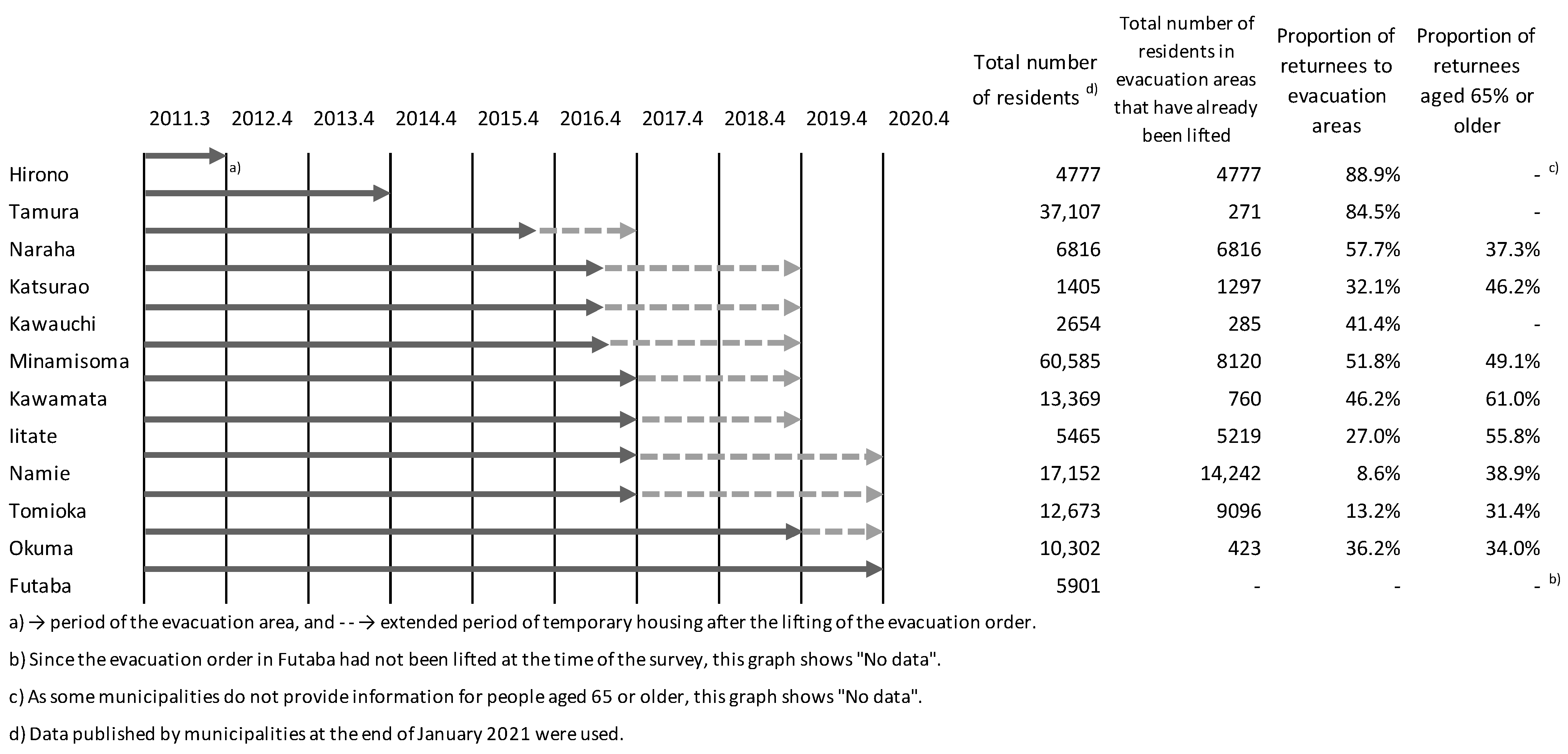
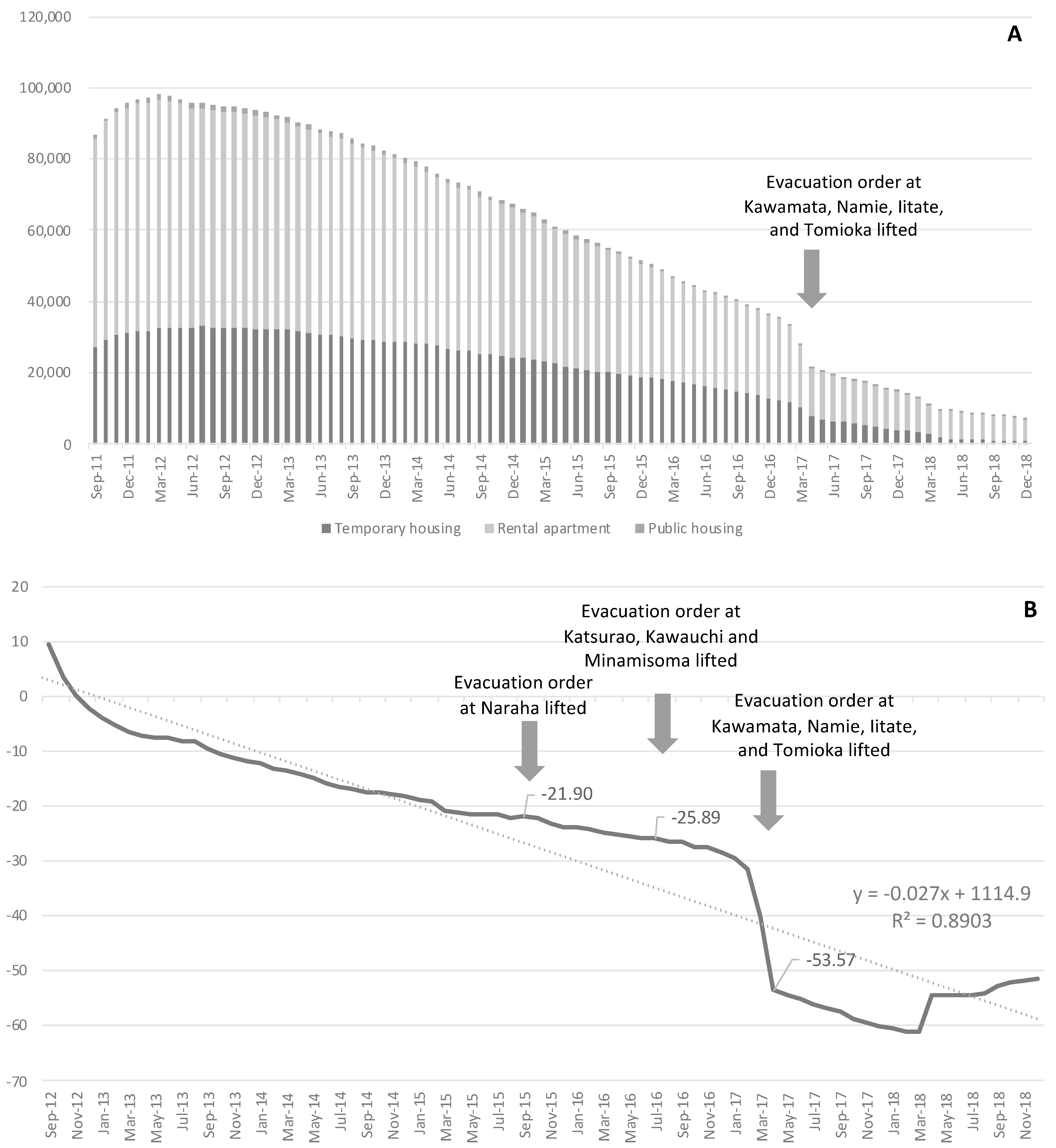
3.3. Trends in the Number of Residents in Temporary Housing, the Number of Returnees after the Lifting of the Evacuation Order
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ishikawa, T. Radiation Doses and Associated Risk From the Fukushima Nuclear Accident. Asia Pac. J. Public Health 2017, 29, 18S–28S. [Google Scholar] [CrossRef] [PubMed]
- Miyazaki, M. Using and Explaining Individual Dosimetry Data. Asia Pac. J. Public Health 2017, 29, 110S–119S. [Google Scholar] [CrossRef] [PubMed]
- Hyodo, K.; Nakamura, K.; Oyama, M.; Yamazaki, O.; Nakagawa, I.; Ishigami, K.; Tsuchiya, Y.; Yamamoto, M. Long-term suicide mortality rates decrease in men and increase in women after the Niigata-Chuetsu earthquake in Japan. Tohoku J. Exp. Med. 2010, 220, 149–155. [Google Scholar] [CrossRef]
- Suzuki, Y.; Tsutsumi, A.; Fukasawa, M.; Honma, H.; Someya, T.; Kim, Y. Prevalence of mental disorders and suicidal thoughts among community-dwelling elderly adults 3 years after the niigata-chuetsu earthquake. J. Epidemiol. 2011, 21, 144–150. [Google Scholar] [CrossRef]
- Wu, H.C.; Chou, P.; Chou, F.H.; Su, C.Y.; Tsai, K.Y.; Ou-Yang, W.C.; Su, T.T.; Chao, S.S.; Sun, W.J.; Chen, M.C. Survey of quality of life and related risk factors for a Taiwanese village population 3 years post-earthquake. Aust. N. Z. J. Psychiatry 2006, 40, 355–361. [Google Scholar] [CrossRef]
- Kiliç, C.; Ulusoy, M. Psychological effects of the November 1999 earthquake in Turkey: An epidemiological study. Acta Psychiatr. Scand. 2003, 108, 232–238. [Google Scholar] [CrossRef]
- Kuroda, Y.; Koyama, Y. Relationship between Psychological Factors and Social Support after Lifting of Evacuation Order in Fukushima Prefecture, Japan. Behav. Sci. 2020, 10, 149. [Google Scholar] [CrossRef]
- Nomura, S.; Murakami, M. Public Health Preparedness for and Response to Nuclear Disasters: An Editorial. Int. J. Environ. Res. Public Health 2018, 15, 2489. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, S. Radiation Medical Science Center for the Fukushima Health Management Survey. Comprehensive Health Risk Management after the Fukushima Nuclear Power Plant Accident. Clin. Oncol. (R. Coll. Radiol.) 2016, 28, 255–262. [Google Scholar] [CrossRef]
- Sonoda, Y.; Ozaki, A.; Hori, A.; Higuchi, A.; Shimada, Y.; Yamamoto, K.; Morita, T.; Sawano, T.; Leppold, C.; Tsubokura, M. Premature Death of a Schizophrenic Patient due to Evacuation after a Nuclear Disaster in Fukushima. Case Rep. Psychiatry 2019, 2019, 3284153. [Google Scholar] [CrossRef]
- Maeda, M.; Oe, M. Mental Health Consequences and Social Issues After the Fukushima Disaster. Asia Pac. J. Public Health 2017, 29, 36S–46S. [Google Scholar] [CrossRef]
- Maeda, M.; Oe, M.; Bromet, E.; Yasumura, S.; Ohto, H. Fukushima, mental health and suicide. J. Epidemiol. Community Health 2016, 9, 843–844. [Google Scholar] [CrossRef]
- Hori, A.; Hoshino, H.; Miura, I.; Hisamura, M.; Wada, A.; Itagaki, S.; Kunii, Y.; Matsumoto, J.; Mashiko, H.; Katz, C.L.; et al. Psychiatric Outpatients After the 3.11 Complex Disaster in Fukushima, Japan. Ann. Glob. Health 2016, 82, 798–805. [Google Scholar] [CrossRef]
- Schneider, T.; Maitre, M.; Lochard, J.J.; Charron, S.; Lecomte, J.; Kanai, Y.; Kuroda, Y.; Naito, W.; Takamura, N.; Orita, M.; et al. The role of radiological protection experts in stakeholder involvement in the recovery phase of post-nuclear accident situations: Some lessons from the Fukushima-Daïchi NPP accident. Radioprotection 2019, 54, 259–270. [Google Scholar] [CrossRef]
- Hori, A.; Morita, T.; Yoshida, I.; Tsubokura, M. Enhancement of PTSD treatment through social support in Idobata-Nagaya community housing after Fukushima’s triple disaster. BMJ Case Rep. 2018, 2018, bcr2018224935. [Google Scholar] [CrossRef] [PubMed]
- Orui, M.; Harada, S.; Hayashi, M. Disaster Mental Health Team of the Sendai City Mental Health and Welfare Center. Practical Report on Long-term Disaster Mental Health Services Following the Great East Japan Earthquake: Psychological and Social Background of Evacuees in Sendai City in the Mid- to Long-term Post-disaster Period. Disaster Med. Public Health Prep. 2017, 11, 439–450. [Google Scholar] [PubMed]
- Orui, M.; Suzuki, Y.; Maeda, M.; Yasumura, S. Suicide Rates in Evacuation Areas After the Fukushima Daiichi Nuclear Disaster. Crisis 2018, 39, 353–363. [Google Scholar] [CrossRef]
- Takebayashi, Y.; Hoshino, H.; Kunii, Y.; Niwa, S.I.; Maeda, M. Characteristics of Disaster-Related Suicide in Fukushima Prefecture After the Nuclear Accident. Crisis 2020, 41, 475–482. [Google Scholar] [CrossRef]
- Kuroda, Y.; Koyama, Y.; Noriko, S. Farming as a purpose of life as well as a business: Rethinking the reconstruction of food and agriculture in Fukushima after the nuclear accident. In Proceedings of the IAEA Consultancy Meeting, IAEA, Vienna, Austria, 7–11 October 2019. [Google Scholar]
- Orui, M.; Nakayama, C.; Moriyama, N.; Tsubokura, M.; Watanabe, K.; Nakayama, T.; Sugita, M.; Yasumura, S. Current Psychological Distress, Post-traumatic Stress, and Radiation Health Anxiety Remain High for Those Who Have Rebuilt Permanent Homes Following the Fukushima Nuclear Disaster. Int. J. Environ. Res. Public Health 2020, 17, 9532. [Google Scholar] [CrossRef]
- Orui, M.; Fukasawa, M.; Horikoshi, N.; Suzuki, Y.; Kawakami, N. Development and Evaluation of a Gatekeeper Training Program Regarding Anxiety about Radiation Health Effects Following a Nuclear Power Plant Accident: A Single-Arm Intervention Pilot Trial. Int. J. Environ. Res. Public Health 2020, 17, 4594. [Google Scholar] [CrossRef]
- Donnelly, S.C. COVID-19 and mental health: Lessons to be learnt from the Fukushima disaster. QJM 2020, 113, 777. [Google Scholar] [CrossRef]
- Bromet, E.J.; Havenaar, J.M.; Guey, L.T. A 25 year retrospective review of the psychological consequences of the Chernobyl accident. Clin. Oncol. (R. Coll. Radiol.) 2011, 23, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Nishio, A.; Akazawa, K.; Shibuya, F.; Abe, R.; Nushida, H.; Ueno, Y.; Nishimura, A.; Shioiri, T. Influence on the suicide rate two years after a devastating disaster: A report from the 1995 Great Hanshin-Awaji Earthquake. Psychiatry Clin. Neurosci. 2009, 63, 247–250. [Google Scholar] [CrossRef] [PubMed]
- Ohto, H.; Maeda, M.; Yabe, H.; Yasumura, S.; Bromet, E.E. Suicide rates in the aftermath of the 2011 earthquake in Japan. Lancet 2015, 385, 727. [Google Scholar] [CrossRef]
- Orui, M.; Sato, Y.; Tazaki, K.; Kawamura, I.; Harada, S.; Hayashi, M. Delayed increase in male suicide rates in tsunami disaster-stricken areas following the great east japan earthquake: A three-year follow-up study in Miyagi Prefecture. Tohoku J. Exp. Med. 2015, 235, 215–222. [Google Scholar] [CrossRef][Green Version]
- Orui, M.; Harada, S.; Saeki, S.; Sato, K.; Kozakai, Y. Trend in the suicide rate following the Great East Japan Earthquake: An eight-year follow-up study in Miyagi prefecture. Psychiatr. Neurol. Jpn. 2020, 122, 573–584. [Google Scholar]
- Orui, M.; Nakajima, S.; Takebayashi, Y.; Ito, A.; Momoi, M.; Maeda, M.; Yasumura, S.; Ohto, H. Mental Health Recovery of Evacuees and Residents from the Fukushima Daiichi Nuclear Power Plant Accident after Seven Years-Contribution of Social Network and a Desirable Lifestyle. Int. J. Environ. Res. Public Health 2018, 15, 2381. [Google Scholar] [CrossRef]
- Shinfuku, N. Disaster mental health: Lessons learned from the Hanshin Awaji earthquake. World Psychiatry 2002, 1, 158–159. [Google Scholar] [PubMed]
- Szanto, K.; Dombrovski, A.Y.; Sahakian, B.J.; Mulsant, B.H.; Houck, P.R.; Reynolds, C.F., 3rd; Clark, L. Social emotion recognition, social functioning, and attempted suicide in late-life depression. Am. J. Geriatr. Psychiatry 2012, 20, 257–265. [Google Scholar] [CrossRef]
- Christensen, H.; Batterham, P.J.; Soubelet, A.; Mackinnon, A.J. A test of the Interpersonal Theory of Suicide in a large community-based cohort. J. Affect Disord. 2013, 144, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Van Orden, K.A.; Wiktorsson, S.; Duberstein, P.; Berg, A.I.; Fässberg, M.M.; Waern, M. Reasons for attempted suicide in later life. Am. J. Geriatr. Psychiatry 2015, 23, 536–544. [Google Scholar] [CrossRef]
- Hori, A.; Ozaki, A.; Murakami, M.; Tsubokura, M. Development of Behavior Abnormalities in a Patient Prevented From Returning Home After Evacuation Following the Fukushima Nuclear Disaster: Case Report. Disaster Med. Public Health Prep. 2020, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Gill, T. Radiation and Responsibility: What is the Right Thing for an Anthropologist to Do in Fukushima?(Practicing a Public Anthropology of the East Japan Disaster). Jpn. Rev. Cult. Anthropol. 2014, 15, 151–163. [Google Scholar]
- Aihara, H.; Iki, M. An ecological study of the relations between the recent high suicide rates and economic and demographic factors in Japan. J. Epidemiol. 2003, 13, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Yamasaki, A.; Araki, S.; Sakai, R.; Yokoyama, K.; Voorhees, A.S. Suicide mortality of young, middle-aged and elderly males and females in Japan for the years 1953-96: Time series analysis for the effects of unemployment, female labour force, young and aged population, primary industry and population density. Ind. Health 2008, 46, 541–549. [Google Scholar] [CrossRef]
- Kuroda, Y.; Koyama, Y.; Yoshida, H.; Naito, W. Preparation of an “information booklet for returnees”-Building trust through collaboration with local communities. Radioprotection 2020, 55, 4. [Google Scholar] [CrossRef]
- Yasutaka, T.; Kanai, Y.; Kurihara, M.; Kobayashi, T.; Kondoh, A.; Takahashi, T.; Kuroda, Y. Dialogue, radiation measurements and other collaborative practices by experts and residents in the former evacuation areas of Fukushima: A case study in Yamakiya District, Kawamata Town. Radioprotection 2020, 55, 215–224. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Region | Male | Female | ||||
|---|---|---|---|---|---|---|
| Median | Max | Min | Median | Max | Min | |
| Evacuation areas | ||||||
| Numbers of suicide deaths | 2 | 8 | 0 | 1 | 5 | 0 |
| Suicide rate | 29.8 | 47.8 | 22.4 | 14.1 | 23.5 | 6.2 |
| Non-evacuation areas | ||||||
| Numbers of suicide deaths | 23 | 46 | 11 | 9 | 23 | 3 |
| Suicide rate | 30.3 | 44.5 | 25.7 | 12.2 | 15.9 | 9.3 |
| National average | ||||||
| Numbers of suicide deaths | 1442 | 2180 | 979 | 628 | 1031 | 383 |
| Suicide rate | 27.8 | 42.1 | 18.8 | 11.5 | 7.0 | 18.9 |
| Variables | Male | Female | ||||||
|---|---|---|---|---|---|---|---|---|
| Suicide Mortality Rate (per 100,000) | ||||||||
| Area/Period | <30 | 30–49 | 50–69 | ≥70 | <30 | 30–49 | 50–69 | ≥70 |
| Evacuation areas | ||||||||
| 2009.3–2011.2 (pre-disaster) | 11.5 | 41.2 | 42.0 | 33.1 | 1.8 | 8.8 | 22.3 | 24.9 |
| 2010.3–2012.2 (peri-disaster) | 16.8 | 42.0 | 42.1 | 54.3 | 1.8 | 9.1 | 15.5 | 29.0 |
| 2011.3–2013.2 (post-disaster) | 17.8 | 32.7 | 40.9 | 54.5 | 0.0 | 4.8 | 19.2 | 21.6 |
| 2012.3–2014.2 | 14.7 | 22.1 | 36.1 | 39.2 | 3.9 | 4.8 | 22.7 | 35.2 |
| 2013.3–2015.2 | 18.9 | 20.2 | 32.9 | 41.9 | 10.1 | 4.9 | 15.8 | 40.9 |
| 2014.3–2016.2 | 17.5 | 33.9 | 29.8 | 56.3 | 8.3 | 12.5 | 16.0 | 25.2 |
| 2015.3–2017.2 | 18.1 | 31.9 | 33.0 | 56.5 | 4.3 | 10.2 | 19.6 | 17.5 |
| 2016.3–2018.2 | 16.6 | 20.7 | 36.3 | 36.0 | 6.6 | 5.2 | 21.4 | 15.8 |
| 2017.3–2018.12 | 12.9 | 21.1 | 31.9 | 55.9 | 4.6 | 5.3 | 12.7 | 19.8 |
| Non-evacuation area | ||||||||
| 2009.3–2011.2 (pre-disaster) | 16.3 | 48.7 | 56.8 | 43.1 | 5.7 | 13.2 | 18.1 | 20.0 |
| 2010.3–2012.2 (peri-disaster) | 16.2 | 41.0 | 48.1 | 39.1 | 5.5 | 13.6 | 17.7 | 20.3 |
| 2011.3–2013.2 (post-disaster) | 16.5 | 34.5 | 40.9 | 41.5 | 6.1 | 16.0 | 16.3 | 19.7 |
| 2012.3–2014.2 | 17.4 | 32.1 | 39.2 | 43.9 | 6.0 | 12.0 | 12.1 | 20.2 |
| 2013.3–2015.2 | 16.9 | 32.9 | 41.0 | 36.9 | 4.8 | 8.8 | 11.6 | 21.5 |
| 2014.3–2016.2 | 14.5 | 32.9 | 36.6 | 35.3 | 3.2 | 11.4 | 14.8 | 20.4 |
| 2015.3–2017.2 | 13.7 | 33.6 | 30.9 | 34.8 | 3.2 | 11.1 | 12.2 | 19.4 |
| 2016.3–2018.2 | 11.1 | 35.0 | 30.6 | 36.7 | 4.8 | 8.5 | 10.0 | 17.5 |
| 2017.3–2018.12 | 11.1 | 32.0 | 28.4 | 33.6 | 5.4 | 7.3 | 9.6 | 16.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuroda, Y.; Orui, M.; Hori, A. Trends in Suicide Mortality in 10 Years around the Great East Japan Earthquake: Analysis of Evacuation and Non-Evacuation Areas in Fukushima Prefecture. Int. J. Environ. Res. Public Health 2021, 18, 6005. https://doi.org/10.3390/ijerph18116005
Kuroda Y, Orui M, Hori A. Trends in Suicide Mortality in 10 Years around the Great East Japan Earthquake: Analysis of Evacuation and Non-Evacuation Areas in Fukushima Prefecture. International Journal of Environmental Research and Public Health. 2021; 18(11):6005. https://doi.org/10.3390/ijerph18116005
Chicago/Turabian StyleKuroda, Yujiro, Masatsugu Orui, and Arinobu Hori. 2021. "Trends in Suicide Mortality in 10 Years around the Great East Japan Earthquake: Analysis of Evacuation and Non-Evacuation Areas in Fukushima Prefecture" International Journal of Environmental Research and Public Health 18, no. 11: 6005. https://doi.org/10.3390/ijerph18116005
APA StyleKuroda, Y., Orui, M., & Hori, A. (2021). Trends in Suicide Mortality in 10 Years around the Great East Japan Earthquake: Analysis of Evacuation and Non-Evacuation Areas in Fukushima Prefecture. International Journal of Environmental Research and Public Health, 18(11), 6005. https://doi.org/10.3390/ijerph18116005