Association of Health Utility Score with Physical Activity Outcomes in Stroke Survivors


 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
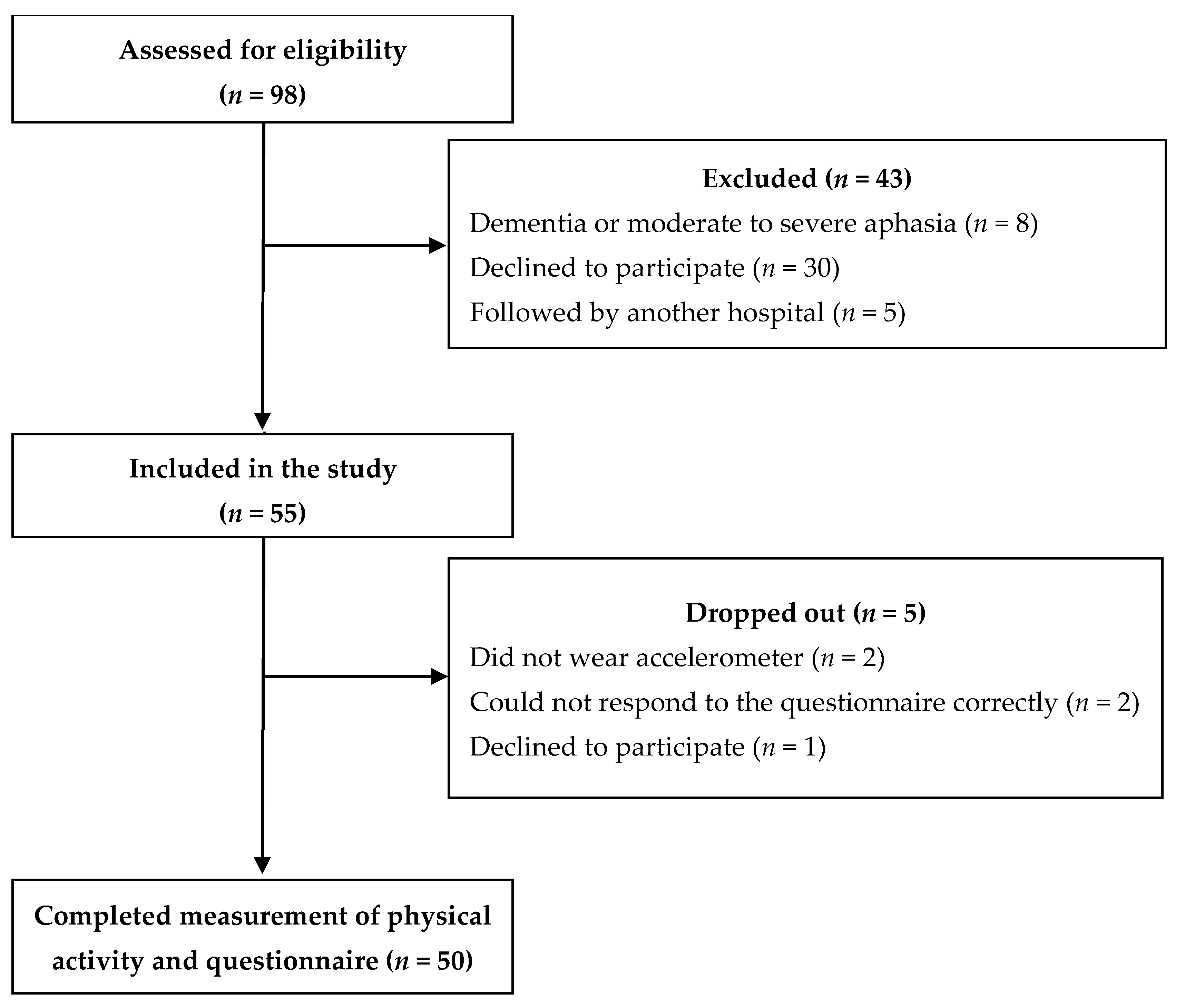
2.1. Study Design and Participant Recruitment
2.2. Clinical Characteristics
2.3. Assessment of Health Utility Score
2.4. Physical Activity Measurement
2.5. Statistical Analysis
3. Results
3.1. Participants and Clinical Characteristics
3.2. Health Utility and Physical Activity
4. Discussion
4.1. Key Findings
4.2. Association of Health Utility Score with Physical Activity Outcomes
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Powers, W.; Rabinstein, A.; Ackerson, T.; Adevoe, O.; Bambakidis, N.; Becker, K. 2018 Guidelines for the Early Management of Patients with Acute Ischemic Stroke: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. J. Vasc. Surg. 2018, 67, 1934. [Google Scholar] [CrossRef]
- Soto-Cámara, R.; González-Santos, J.; González-Bernal, J.; Martín-Santidrian, A.; Cubo, E.; Trejo-Gabriel-Galán, J.M. Factors Associated with shortening of prehospital delay among patients with acute ischemic stroke. J. Clin. Med. 2019, 17, 1712. [Google Scholar] [CrossRef] [PubMed]
- Carod-Artal, F.J.; Egido, J.A. Quality of life after stroke: The importance of a good recovery. Cerebrovasc. Dis. 2009, 27 (Suppl. 1), 204–214. [Google Scholar] [CrossRef]
- De Wit, L.; Theuns, P.; Dejaeger, E.; Devos, S.; Gantenbein, A.R.; Kerckhofs, E.; Schuback, B.; Schupp, W.; Putman, K. Long-term impact of stroke on patients’ health-related quality of life. Disabil. Rehabil. 2017, 39, 1435–1440. [Google Scholar] [CrossRef] [PubMed]
- Jeon, N.E.; Kwon, K.M.; Kim, Y.H.; Lee, J.S. The factors associated with health-related quality of life in stroke survivors age 40 and older. Ann. Rehabil. Med. 2017, 41, 743–752. [Google Scholar] [CrossRef] [PubMed]
- Kwon, S.; Park, J.H.; Kim, W.S.; Han, K.; Lee, Y.; Paik, N.J. Health-related quality of life and related factors in stroke survivors: Data from Korea National Health and Nutrition Examination Survey (KNHANES) 2008 to 2014. PLoS ONE 2018, 13, e0195713. [Google Scholar] [CrossRef]
- Ayis, S.; Wellwood, I.; Rudd, A.G.; McKevitt, C.; Parkin, D.; Wolfe, C.D. Variations in health-related quality of life (HRQoL) and survival 1 year after stroke: Five European population-based registers. BMJ Open 2015, 5, e007101. [Google Scholar] [CrossRef]
- Rand, D.; Eng, J.J.; Tang, P.F.; Hung, C.; Jeng, J.S. Daily physical activity and its contribution to the health-related quality of life of ambulatory individuals with chronic stroke. Health Qual. Life. Outcomes 2010, 8, 80. [Google Scholar] [CrossRef]
- White, J.; Magin, P.; Attia, J.; Sturm, J.; McElduff, P.; Carter, G. Predictors of health-related quality of life in community-dwelling stroke survivors: A cohort study. Fam. Pract. 2016, 33, 382–387. [Google Scholar] [CrossRef]
- Noto, S.; Yanagi, H.; Tomura, S. Measuring utilities for various functional outcomes after stroke. Comparison of rating scale and time trade-off methods. Jpn. J. Public Health 2002, 9, 1205–1216. [Google Scholar]
- van Eeden, M.; van Heugten, C.; van Mastrigt, G.A.; van Mierlo, M.; Visser-Meily, J.M.; Evers, S.M. The burden of stroke in The Netherlands: Estimating quality of life and costs for 1 year poststroke. BMJ Open 2015, 27, e008220. [Google Scholar] [CrossRef] [PubMed]
- Thilarajah, S.; Mentiplay, B.F.; Bower, K.J.; Tan, D.; Pua, Y.H.; Williams, G.; Koh, G.; Clark, R.A. Factors associated with post stroke physical activity: A systematic review and meta-analysis. Arch. Phys. Med. Rehabil. 2018, 99, 1876–1889. [Google Scholar] [CrossRef] [PubMed]
- Loprinzi, P.D.; Addoh, O. Accelerometer-determined physical activity and all-cause mortality in a national prospective cohort study of adults post-acute stroke. Am. J. Health Promot. 2018, 32, 24–27. [Google Scholar] [CrossRef]
- Kono, Y.; Yamada, S.; Yamaguchi, J.; Hagiwara, Y.; Iritani, N.; Ishida, S.; Araki, A.; Hasegawa, Y.; Sakakibara, H.; Koike, Y. Secondary prevention of new vascular events with lifestyle intervention in patients with noncardioembolic mild ischemic stroke: A single-center randomized controlled trial. Cerebrovasc. Dis. 2013, 36, 88–97. [Google Scholar] [CrossRef]
- Kono, Y.; Yamada, S.; Iwatsu, K.; Nitobe, S.; Tanaka, Y.; Shimizu, Y.; Shinoda, N.; Okumura, T.; Hirashiki, A.; Murohara, T. Predictive impact of daily physical activity on new vascular events in patients with mild ischemic stroke. Int. J. Stroke 2015, 10, 219–223. [Google Scholar] [CrossRef]
- Macko, R.F.; Benvenuti, F.; Stanhope, S.; Macellari, V.; Taviani, A.; Nesi, B.; Weinrich, M.; Stuart, M. Adaptive physical activity improves mobility function and quality of life in chronic hemiparesis. J. Rehabil. Res. Dev. 2008, 45, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Hou, L.; Du, X.; Chen, L.; Li, J.; Yan, P.; Zhou, M.; Zhu, C. Exercise and quality of life after first-ever ischaemic stroke: A two-year follow-up study. Int. J. Neurosci. 2018, 128, 540–548. [Google Scholar] [CrossRef]
- Sasaki, S.; Kanai, M.; Shinoda, T.; Morita, H.; Shimada, S.; Izawa, K.P. Relation between health utility score and physical activity in community-dwelling ambulatory patients with stroke: A preliminary cross-sectional study. Top. Stroke Rehabil. 2018, 25, 475–479. [Google Scholar] [CrossRef]
- van Swieten, J.C.; Koudstaal, P.J.; Visser, M.C.; Schouten, H.J.; van Gijn, J. Interobserver agreement for the assessment of handicap in stroke patients. Stroke 1988, 19, 604–607. [Google Scholar] [CrossRef]
- Lyden, P.; Brott, T.; Tilley, B.; Welch, K.M.; Mascha, E.J.; Levine, S.; Haley, E.C.; Grotta, J.; Marler, J. Improved reliability of the NIH Stroke Scale using video training. NINDS TPA Stroke Study Group. Stroke 1994, 25, 2220–2226. [Google Scholar] [CrossRef]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A short physical performance battery assessing lower extremity function: Association with self-reported disability and prediction of mortality and nursing home admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef] [PubMed]
- Kamo, T.; Suzuki, R.; Ito, K.; Sugimoto, T.; Murakoshi, T.; Nishida, Y. Prevalence of sarcopenia and its relation to body composition, physiological function, and nutritional status in community-dwelling frai1 elderly people [Japanese with English abstract]. J. Jpn. Phys. Ther. Assoc. 2013, 40, 414–420. [Google Scholar]
- Tsuchiya, A.; Ikeda, S.; Ikegami, N.; Nishimura, S.; Sakai, I.; Fukuda, T.; Hamashima, C.; Hisashige, A.; Tamura, M. Estimating an EQ-5D population value set: The case of Japan. Health Econ. 2002, 11, 341–353. [Google Scholar] [CrossRef] [PubMed]
- Kanai, M.; Izawa, K.P.; Kubo, H.; Nozoe, M.; Mase, K.; Koohsari, M.J.; Oka, K.; Shimada, S. Association of perceived built environment attributes with objectively measured physical activity in community-dwelling ambulatory patients with stroke. Int. J. Environ. Res. Public Health 2019, 16, 3908. [Google Scholar] [CrossRef]
- Kanai, M.; Izawa, K.P.; Nozoe, M.; Kubo, H.; Kobayashi, M.; Onishi, A.; Mase, K.; Shimada, S. Long-term effect of promoting in-hospital physical activity on postdischarge patients with mild ischemic stroke. J. Stroke Cerebrovasc. Dis. 2019, 28, 1048–1055. [Google Scholar] [CrossRef]
- Fitbit Dashboard. Available online: https://accounts.fitbit.com/login (accessed on 21 December 2020).
- Kharroubi, S.A.; Brazier, J.E.; Roberts, J.; O’Hagan, A. Modelling SF-6D health state preference data using a nonparametric Bayesian method. J. Health Econ. 2007, 26, 597–612. [Google Scholar] [CrossRef]
- Haacke, C.; Althaus, A.; Spottke, A.; Siebert, U.; Back, T.; Dodel, R. Long-term outcome after stroke: Evaluating health-related quality of life using utility measurements. Stroke 2006, 37, 193–198. [Google Scholar] [CrossRef]
- Post, P.N.; Stiggelbout, A.M.; Wakker, P.P. The utility of health states after stroke: A systematic review of the literature. Stroke 2001, 32, 1425–1429. [Google Scholar] [CrossRef]
- Grau-Pellicer, M.; Chamarro-Lusar, A.; Medina-Casanovas, J.; Serdà Ferrer, B.C. Walking speed as a predictor of community mobility and quality of life after stroke. Top. Stroke Rehabil. 2019, 26, 349–358. [Google Scholar] [CrossRef]
- Fulk, G.D.; He, Y.; Boyne, P.; Dunning, K. Predicting home and community walking activity poststroke. Stroke 2017, 48, 406–411. [Google Scholar] [CrossRef]
- Tse, T.; Binte Yusoff, S.Z.; Churilov, L.; Ma, H.; Davis, S.; Donnan, G.A.; Carey, L.M.; START Research Team. Increased work and social engagement is associated with increased stroke specific quality of life in stroke survivors at 3 months and 12 months post-stroke: A longitudinal study of an Australian stroke cohort. Top. Stroke Rehabil. 2017, 24, 405–414. [Google Scholar] [CrossRef] [PubMed]
- Hokstad, A.; Indredavik, B.; Bernhardt, J.; Ihle-Hansen, H.; Salvesen, Ø.; Seljeseth, Y.M.; Schüler, S.; Engstad, T.; Askim, T. Hospital differences in motor activity early after stroke: A comparison of 11 Norwegian stroke units. J. Stroke Cerebrovasc. Dis. 2015, 24, 1333–1340. [Google Scholar] [CrossRef] [PubMed]
- Gray, L.J.; Sprigg, N.; Bath, P.M.; Boysen, G.; De Deyn, P.P.; Leys, D.; O’Neill, D.; Ringelstein, E.B.; TAIST Investigators. Sex differences in quality of life in stroke survivors: Data from the Tinzaparin in Acute Ischaemic Stroke Trial (TAIST). Stroke 2007, 38, 2960–2964. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.D.; McKevitt, C.; Lawrence, E.; Rudd, A.G.; Wolfe, C.D. Clinical determinants of long-term quality of life after stroke. Age Ageing 2007, 36, 316–322. [Google Scholar] [CrossRef]
- Baumann, M.; Lurbe, K.; Leandro, M.E.; Chau, N. Life satisfaction of two-year post-stroke survivors: Effects of socio-economic factors, motor impairment, Newcastle stroke-specific quality of life measure and World Health Organization quality of life: Bref of informal caregivers in Luxembourg and a rural area in Portugal. Cerebrovasc. Dis. 2012, 33, 219–230. [Google Scholar]


{kind=link}
| Characteristic | All Participants (n = 50) |
|---|---|
| Age (years) | 68.0 (53.8–77.0) |
| Sex (male), n (%) | 40 (80.0) |
| Body mass index (kg/m2) | 23.1 (21.8–24.8) |
| Subtypes, n (%) | |
| Ischemic | 32 (64.0) |
| Hemorrhage | 18 (36.0) |
| NIHSS (score) | 1.0 (1.0–2.0) |
| Time since stroke (months) | 4.2 (1.7–6.4) |
| Comorbidity, n (%) | |
| Hypertension | 44 (88.8) |
| Diabetes mellitus | 18 (36.0) |
| Dyslipidemia | 28 (56.0) |
| Handgrip strength (kgf) | 31.9 (24.3–37.6) |
| Walking speed (m/s) | 1.1 (0.9–1.3) |
| Age | Sex (0, Male; 1, Female) | BMI | NIHSS | Handgrip Strength | Walking Speed | Number of Steps | MVPA | |
|---|---|---|---|---|---|---|---|---|
| HU score | −0.204 | −0.438 | 0.465 | −0.326 | 0.396 | 0.429 | 0.454 | 0.497 |
| (0.154) | (0.001) | (0.001) | (0.021) | (0.004) | (0.002) | (0.001) | (<0.001) |
| Model 1 (Adjusted R2 = 0.383) | Model 2 (Adjusted R2 = 0.357) | |||
|---|---|---|---|---|
| β | p Value | β | p Value | |
| Sex | −0.366 | 0.026 | −0.354 | 0.035 |
| BMI | 0.210 | 0.109 | 0.218 | 0.106 |
| NIHSS | −0.124 | 0.365 | −0.142 | 0.309 |
| Handgrip strength | −0.158 | 0.382 | −0.082 | 0.641 |
| Walking speed | 0.188 | 0.182 | 0.171 | 0.257 |
| Number of steps | 0.304 | 0.035 | ||
| MVPA | 0.231 | 0.102 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kanai, M.; Izawa, K.P.; Kubo, H.; Nozoe, M.; Mase, K.; Shimada, S. Association of Health Utility Score with Physical Activity Outcomes in Stroke Survivors. Int. J. Environ. Res. Public Health 2021, 18, 251. https://doi.org/10.3390/ijerph18010251
Kanai M, Izawa KP, Kubo H, Nozoe M, Mase K, Shimada S. Association of Health Utility Score with Physical Activity Outcomes in Stroke Survivors. International Journal of Environmental Research and Public Health. 2021; 18(1):251. https://doi.org/10.3390/ijerph18010251
Chicago/Turabian StyleKanai, Masashi, Kazuhiro P. Izawa, Hiroki Kubo, Masafumi Nozoe, Kyoshi Mase, and Shinichi Shimada. 2021. "Association of Health Utility Score with Physical Activity Outcomes in Stroke Survivors" International Journal of Environmental Research and Public Health 18, no. 1: 251. https://doi.org/10.3390/ijerph18010251
APA StyleKanai, M., Izawa, K. P., Kubo, H., Nozoe, M., Mase, K., & Shimada, S. (2021). Association of Health Utility Score with Physical Activity Outcomes in Stroke Survivors. International Journal of Environmental Research and Public Health, 18(1), 251. https://doi.org/10.3390/ijerph18010251