1. Introduction
Work related injuries, illnesses, and deaths are critical public health problems that result in important social and economic costs. In the European Union, the cost related to these problems is 3.3% of its gross domestic product (GPD), roughly reaching up to 3.9% of the worldwide GDP [
1]. Musculoskeletal disorders (MSDs) are the most frequent problems and the leading cause of work disability, sickness, and absence from work [
2,
3]. For example, the prevalence of work related MSDs in Great Britain in 2017/18 was 469,000 out of a total of 1,358,000 for all work-related illnesses (35% of the total) [
4]. It is difficult to measure the real economic burden related to MSDs [
2,
5]. Apart from direct costs, such as medical expenses or compensation, and indirect costs related to absenteeism or productivity decline, intangible costs due to the social consequences of MSDs must be considered [
6]. Sixty-seven percent of those affected state that their quality of life has been significantly reduced [
7] due to chronic pain, chronic fatigue, and economic reasons such as decreased incomes. Forty-nine percent of them declare that they are unable to perform their work normally, and 30% of them are worried about discrimination or losing their job [
8].
Governments and public organizations encourage enterprises to adopt strategies to diminish the prevalence of MSDs. Physical, organizational, and cognitive ergonomics interventions are focused on reducing the risk factors for MSDs [
9] through physical workplace redesigns, variations of task times and contents, implementing training programs, improving cognitive processes to reduce mental workload, and involving workers in developing and implementing changes [
10]. Out of these interventions, currently, public occupational safety and health agencies and institutions are especially interested in promoting participatory ergonomic training programs. Ergonomic training programs are intended to transfer knowledge-relating ergonomics issues about work to the employees, but also to involve them in participating in the recognition and resolution of the problems [
11].
There is very little research about the effectiveness of ergonomics training. In an effective ergonomics training program, the acquired knowledge must lead to a positive change in the trained workers’ behavior. The training is transferred to the workplace, achieving the goal of the training program, for example, a reduction of MSDs. However, there is some controversy about this. Some previous studies [
12,
13,
14,
15,
16] support the effectiveness of occupational health and safety training. Educational interventions increase the safety knowledge of the workers, have a positive effect on attitude and beliefs toward prevention behaviors, and reduce negative safety and health outcomes like musculoskeletal pains and symptoms. On the other hand, some works and systematic reviews found that ergonomics training does not always lead to the expected workers’ behavioral change [
17,
18,
19,
20,
21]. However, there is consensus that training methods and learning materials are important factors that affect the effectiveness of ergonomic training programs [
14,
22]. Findings from previous works revealed that as the method of training becomes more engaging, the effect of training is greater [
12,
13] and that the duration of outcome may be influenced by the style of training delivery. The perceived quality and usefulness of the training methods are positively correlated with learning transfer [
23]. Furthermore, learning materials that are too theoretical prevent the transfer of training [
24] and their effectiveness to change workers’ behavior is low [
17,
18]. Although moving from passive information-based methods (lectures, pamphlets, classroom theory lessons…) to more engaging methods results in greater knowledge acquisition and more transfer of training to the work setting, the most common training method in occupational health and safety is classroom theory lessons [
14]. Currently, governments and public organizations promote the development of more engaging training methods and materials. Some examples are the series of occupational safety and health education toolkits (NAPO) devised by the European Agency for Safety and Health at Work, or projects like Train4work of the Federation of European Ergonomics Societies to identify training requirements and define learning objectives of the learning material in a participatory way.
The development of information and communication technologies now makes new learning methods possible in training programs. Until recently, the use of these techniques implied the need to wear complex and expensive devices. However, the advance of technology has made it possible to use very low-cost portable devices able to generate highly immersive experiences. Some virtual reality (VR) headsets are currently available in the market for prices from 250 euros and are becoming common consumer products. Furthermore, smartphones can be used now as VR systems, using devices that transform any smartphone into a VR device for prices below 5 euros. On the other hand, developing content to be used in these devices is now cheap and affordable. Content generation systems have also evolved enormously in recent times and, nowadays, it is possible to develop immersive virtual environments (3D environments, 360° video, etc.) using free development frameworks.
Currently, due to these new low-cost VR devices and content development frameworks, learning methods that use technological tools and immersive media, such as VR or augmented reality, are extensively employed in training programs. The effects of using immersive media and contents on the performance of training programs have been studied in several fields such as industry [
25,
26,
27], medicine and surgery [
28,
29,
30], rehabilitation [
31,
32], or construction [
33,
34,
35,
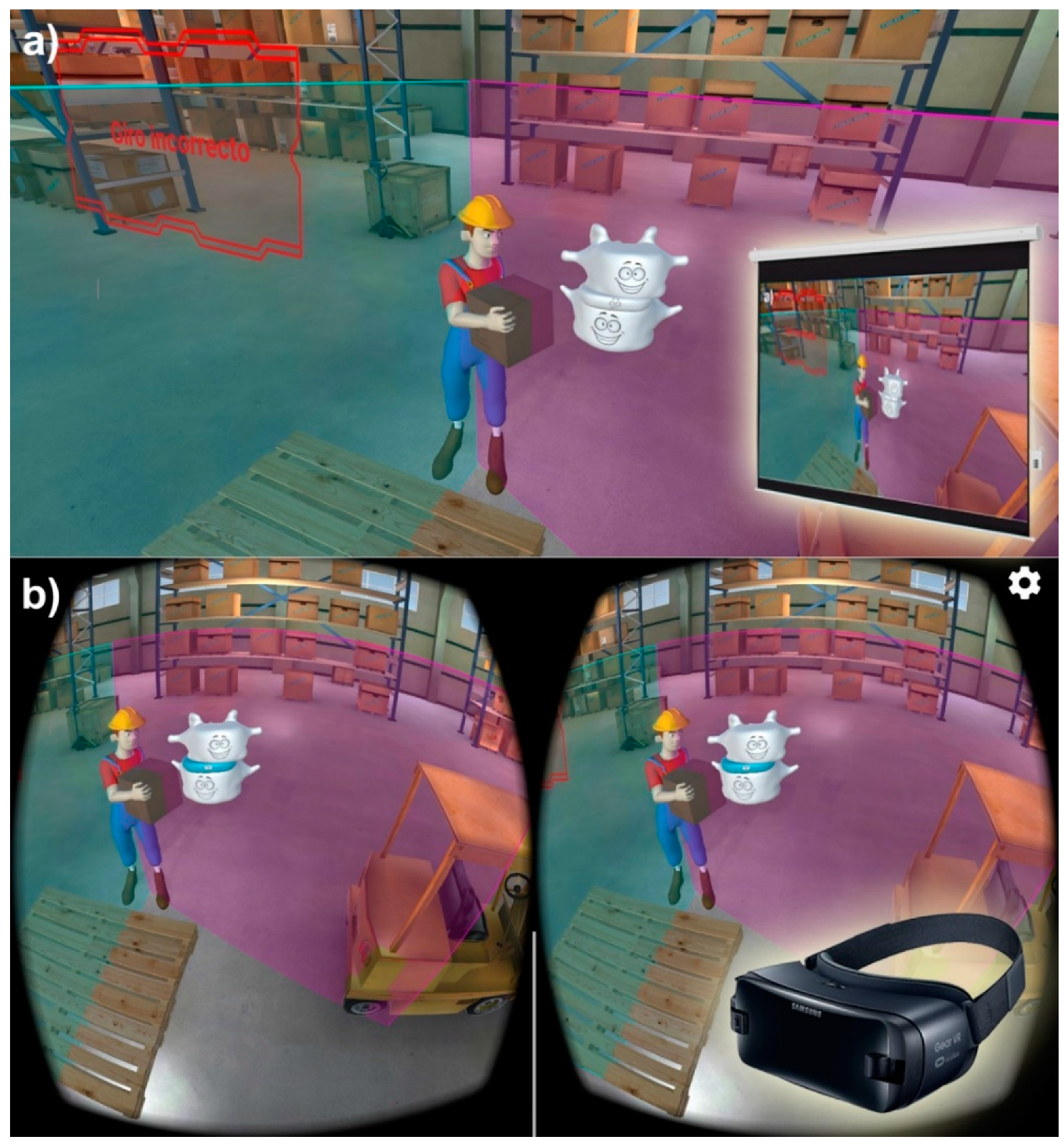
36]. However, there is very little research on the effects of using immersive media in training workers to avoid ergonomics risk factors. In this work, we used traditional (video presentations) and immersive media (virtual reality headsets) in a training program to avoid three common ergonomics risk factors in industrial environments: repetitive movements, improper postures, and handling loads. The differences in using both ways of delivering the learning contents in the workers’ knowledge, behavior, and attitudes were analyzed. The results of this study may assist trainers in developing more effective training programs to avoid ergonomics risk factors.
3. Results
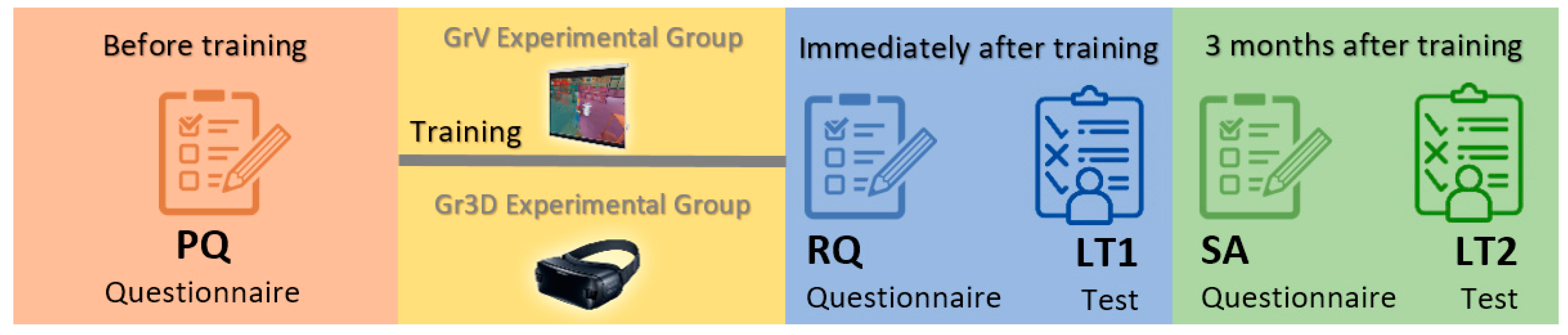
Initially, 70 workers took part in the training and answered the PQ and RQ questionnaires and the LT knowledge test. One of the participants of the GrV group (GrV26 in
Table A3) did not complete the LT test and the SA questionnaire in the second round because he no longer worked in the company.
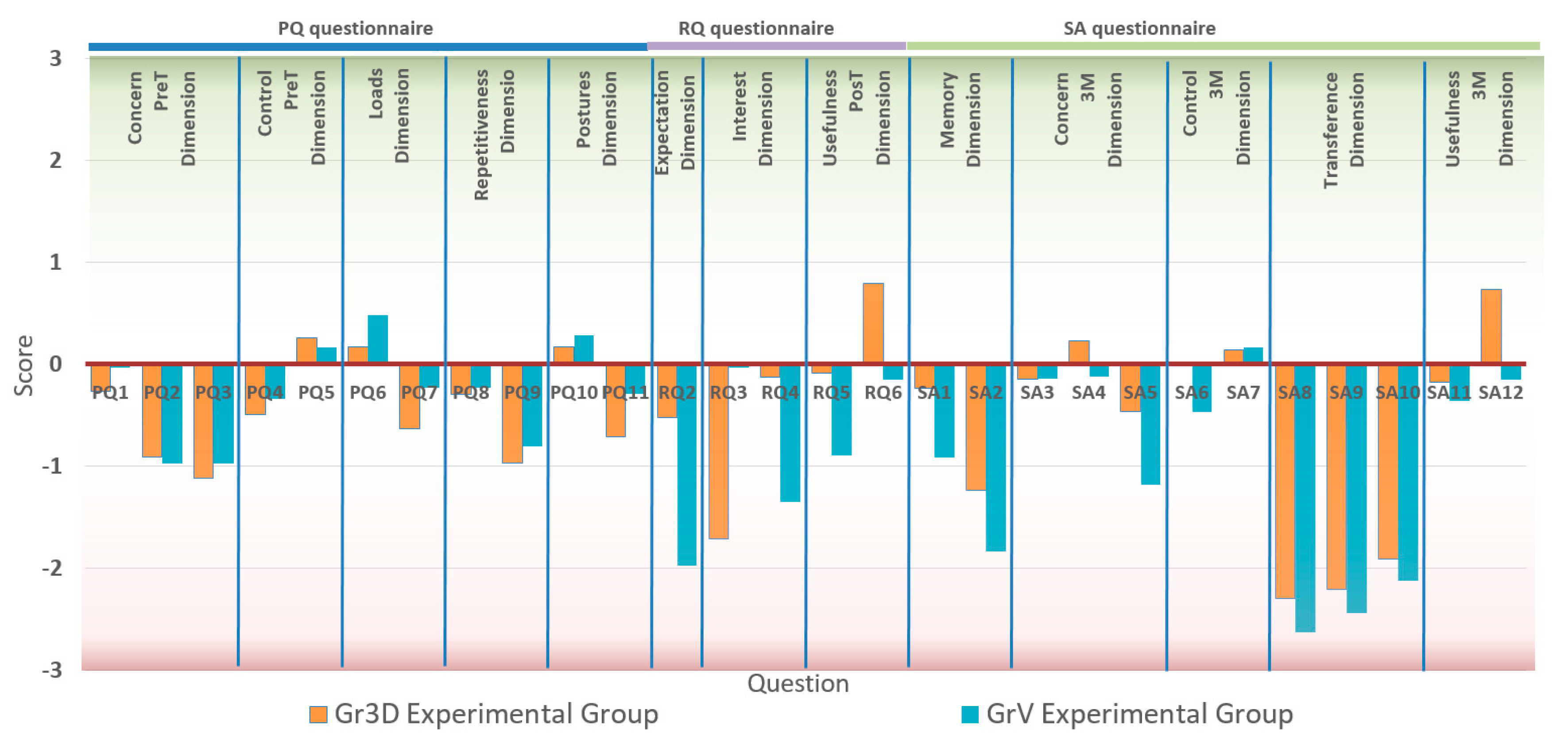
Figure 5 shows the average response to each question by experimental group. To elaborate this figure, a score was given to each answer of the scales ranging from −3 for the lowest level of the scales (strongly disagree, never, and not important at all) to +3 for the highest level (strongly agree, very frequently, and very important).
A different score system was used to statistically analyze the data. For the lowest level of the scales, 1 was used, and for the highest level of the scales, 7 was used. The complete set of responses to the questionnaires PQ and RQ are shown in
Table A1 and
Table A2 in the
Appendix A using this score system. The results for the questionnaire SA and for the LT knowledge tests are given in
Table A2 and
Table A3. In these tables, the LT1 column shows the number of correct answers given to the LT test in the first round, and the LT2 column shows the difference between the number of correct answers given to the LT test in the first round and in the second round three months after the training.
Table 4 shows the mean and the standard deviation of the responses to each question by experimental group, and the results of the
t-tests conducted to check whether there are statistically significant differences between the two groups (at significance level of 0.05). The scores for each dimension (Concern, Control, Loads, Repetitiveness, Postures, Expectation, Interest, Usefulness, Memory, and Transference) were calculated, summing up the scores of the correspondents’ questions for each participant. Questions PQ5 and RQ3 were negatively worded with respect to the rest of the questions of their dimensions, therefore, the scores of these questions were reversed. Cronbach’s alpha (α) was used to calculate the internal reliability of the dimensions. The Cronbach’s alpha is commonly used to test for internal consistency and reliability of a questionnaire consisting of multiple Likert scales and items [
49]. Although there is no clear consensus on the value of α that indicates an acceptable reliability, a value over 0.7 is usually considered to indicate a moderate consistency [
50]. The Cronbach’s alphas in this study (
Table 4) showed that all the dimensions had a moderate internal reliability.
The results of the PQ questionnaire (
Table 4) showed that there were not significant differences between the workers of the two experimental groups before the training. No significant differences were found (
t (68) = −0.37,
p = 0.714) in the level of the workers’ concern about ergonomics risks in their tasks (Concern dimension) between the workers selected to receive the training using a video projection (GrV: M = 10.03) and the workers selected to receive the training using a VR headset (Gr3D: M = 9.71). Differences between the groups were not found in any of the questions of this dimension either. The scores of the questions PQ1 (GrV: M = 3.97, Gr3D: M = 3.74), PQ2 (GrV: M = 3.03, Gr3D: M = 3.09), and PQ3 (GrV: M = 3.03, Gr3D: M = 2.89) show, in general terms, a low workers’ level of concern about ergonomics risks and the consequences on their long-term health. In the same way, no differences were found between experimental groups in the Control dimension (
t (68) = −0.40,
p = 0.687) before the training. The answers to the questions PQ4 (GrV: M = 3.66, Gr3D: M = 3.51) and PQ5 (GrV: M = 3.83, Gr3D: M = 3.74) showed that workers believed that ergonomics risks were controlled to the same extent by the managers of health and safety of the plant and by themselves. Improperly handling loads (GrV: M = 4.48, Gr3D: M = 4.17) and adopting awkward postures (GrV: M = 4.29, Gr3D: M = 4.17) were considered more important risk factors than performing excessive repetitive movements (GrV: M = 3.77, Gr3D: M = 3.71), with no differences between the experimental groups. Nonetheless, the answers to the questions PQ7 (GrV: M = 3.77, Gr3D: M = 3.37), PQ9 (GrV: M = 3.20, Gr3D: M = 3.03), and PQ11 (GrV: M = 3.71, Gr3D: M = 3.19) showed that they did not feel that they needed training to avoid any of the risk factors.
Conversely, the answers to the RQ questionnaire, filled out just after the training, showed significant differences between the two experimental groups. From the results of the RQ2 question, the participants of the Gr3D group were significantly (
t (68) = 5.03,
p < 0.001) more keen on receiving the training than those of the GrV group (GrV: M = 2.03, Gr3D: M = 3.48). In the same way, significant differences (
t (68) = 7.53,
p < 0.001) between the experimental groups were found in the level of engagement of the participants during the training sessions (Interest dimension). The participants of the GrV group felt more tired or bored during the training (question RQ3) than those of the Gr3D group (GrV: M = 4.03, Gr3D: M = 5.71). Similarly, judging from the RQ4 question’s answers, the participants who used the VR headset found the learning materials more interesting (GrV: M = 2.66, Gr3D: M = 3.88). Finally, the perceived usefulness of the training (Usefulness PosT dimension) showed significant differences (
t (68) = 5.40,
p < 0.001) between the groups. The questions RQ5 and RQ6 indicate that the workers who used the VR headset found the training more useful (GrV: M = 3.11, Gr3D: M = 3.91) and better than previous similar trainings (GrV: M = 3.85, Gr3D: M = 4.80). The scores of the LT knowledge test (LT1 column in the
Table A3 and
Table A4) were a bit higher for the participants of the GrV experimental group (GrV: M = 23.37, Gr3D: M = 22.06), but this difference was not significant (
t (68) = 1.68,
p < 0.397).
Significant differences were found between the groups (t (67) = 2.24, p = 0.029) in the Memory dimension of the SA questionnaire, filled out three months after the training. The Memory dimension measured if the trainees remembered the learning contents after the training, when they were undertaking their tasks (SA1 question), and if they analyzed these tasks considering the learning of the training (SA2 question). The results showed that the workers who received the training using the VR headset remembered the training more than those in the GrV group (GrV: M = 5.26, Gr3D: M = 6.54).
The Concern dimension was assessed again in the SA questionnaire (Concern 3M in
Table 4). Three months after the training, significant differences (
t (67) = 2.04,
p = 0.045) were found between groups in this dimension. The workers of the Gr3D group showed a higher level of concern about ergonomics risks and the consequences on their long-term health (GrV: M = 9.91, Gr3D: M = 11.69). An analysis of covariance (ANCOVA) was performed on the Concern 3M scores, using the scores of Concern PT as the covariate, to check if the media used to deliver the training significantly affected the concern of the workers about ergonomics risks. The ANCOVA indicated that the training method produced significant differences in the Concern dimension (
Table 5) at the 0.05 level of probability.
Conversely, no significant differences between the groups were found in the Control dimension three month after the training (t (67) = 0.83, p = 0.411) and neither were they found in the scores of the questions in this dimension (SA6 and SA7). An ANCOVA performed on the Control 3M scores, with the scores of Control PT as the covariate, found that the media used to deliver the training did not affect the workers perception of the ergonomics risks in their workplaces (F (1, 66) = 2.25, p = 0.138).
The results of the Transference dimension showed that little training was transferred to the work place, and no significant differences were found between the experimental groups (t (67) = 1.76, p = 0.083). The workers of the Gr3D group were able to identify risky activities among their tasks after the training to a greater extent than the participants in the GrV group (GrV: M = 1.38, Gr3D: M = 1.71). However, from the scores of questions SA9 and SA10, there were no differences between the groups in how the participants tried to improve the way in which they undertook their tasks to avoid ergonomics risks.
As occurred immediately after the training, three months later the perceived usefulness of the training (Usefulness 3M) showed significant differences (t (67) = 2.36, p = 0.021) between the experimental groups. However, the differences were, in this case, limited to only one out of the two questions in this dimension. Although the participants in the Gr3D group found the training significantly better than similar ones received previously (t (67) = 3.81, p < 0.001), no differences between the groups were found in the perceived usefulness of the training (t (67) = 0.60, p = 0.549).
As aforementioned, there were no significant differences between the groups in the scores of the LT knowledge test filled out just after the training. Therefore, it seems that the media used to deliver the training did not affect the level of knowledge or skills acquired by the participants. However, the results of the same test filled out three months after the training showed significant differences between the groups (
t (67) = 3.11,
p = 0.003). The LT2 column in
Table A3 and
Table A4 showed the difference between the number of correct answers given to the LT test in the first round and in the second round. Although the results were similar for the participants of the two groups in the first round, the scores in the second round (GrV: M = 18.47, Gr3D: M = 21.14) were better for the participants who used the VR headset during the training (
Figure 6). An ANCOVA was performed on the LT1 scores with the scores of LT2 as the covariate. The results (
F (1, 66) = 9.79,
p = 0.003) showed that the media used to deliver the training significantly affects how the knowledge acquired was retained over time.
4. Discussion
In this work, we studied the effects of using immersive media to deliver the learning contents in ergonomics training on the workers’ knowledge, behavior, and attitudes about ergonomics risk factors. The differences in using a traditional video projector and a VR headset were analyzed. The data were collected immediately after the training and three months later.
To achieve the training transfer to the workplace, the worker must be aware of the consequences of ergonomics risks on their health and quality of life. An adequate perception of the ergonomics risks is needed. The perceived risk is the subjective judgment that the worker makes about the frequency of a particular risk and the severity of the consequences [
51]. In general terms, the level of concern about ergonomics risks and the consequences on the long-term health of the workers who participated in the study was low. They did not feel that they needed training to avoid any of the risk factors selected for this study despite there being risks present in their tasks (more than 30% of the workstations had a medium or high level of each kind of risk). The results of this study found that the media used to deliver the training significantly affects the change in the workers’ level of concern about ergonomics risks. The workers of the experimental group that used a VR headset showed a higher level of concern about ergonomics risks and their consequences on their long-term health three months after the training. A low level of concern about ergonomics risks is a common situation because, overall, work-related musculoskeletal disorders are cumulative traumas. The injuries are caused by the accumulation of small traumas over a long period of time. Therefore, it is difficult for the worker to establish a direct cause–effect relationship between the ergonomics risk factors and their consequences for their health. Using immersive media in ergonomics training may lead to an increased ergonomics risks perception.
Although the workers of both experimental groups did not feel they needed the training, we found significant differences in the participants’ expectations about the training due to the different media used to deliver the learning contents (the only difference between the two experimental groups). The workers assigned to the training group that used the VR headset were significantly keener on receiving the training than those of the GrV group. This could have a significant influence on post-training attitudes and motivation to transfer learning [
47]. In the same way, significant differences in the level of engagement of the participants during the training sessions were found. During the training, the participants who used the VR headset found the learning materials more interesting, while the participants of the GrV group felt more tired or bored. The degree of novelty of the technology used in the training can affect the engagement of the trainees [
52], and the level of engagement of the participants during the training sessions affects the effectiveness of training programs [
12,
13,
14,
22]. Therefore, part of the effectiveness of the training can be attributed to the novelty of the device [
53]. Our intention was to measure if the different degrees of novelty of the VR headset among the workers of the Gr3D experimental group affected the effectiveness of the training. However, the answers to the question RQ1 of the RQ questionnaire (
Table 4) show that 88.57% of the workers of the Gr3D experimental group had never used a VR headset before the training, only 3 workers had used it once, and only 1 more than once. Therefore, there were not enough participants with experience in the use of VR headsets to perform a significant statistical analysis on the influence of novelty on training effectiveness.
Just after the training, the workers who used the VR headset found the training more useful and better than previous similar training. The perceived quality and usefulness of the training methods are positively correlated with learning transfer [
23]. Although three months later the differences were limited to training quality and no differences between the groups were found in the perceived usefulness of the training, overall, the scores of the Usefulness dimension were significantly higher in the Gr3D experimental group. On the other hand, although the media used in the training does not seem to have an effect on the level of knowledge or skills acquired by the participants, the learning was better retained over time by the workers who used the VR headset. This result is consistent with the findings of previous works that revealed that the duration of the outcome of the training may be influenced by the style of training delivery, lasting longer as the method of training becomes more engaging [
12,
13].
Despite the results in the other analyzed dimensions, the Transference dimension shows no significant differences between the experimental groups. Although the workers who used the VR headset were better able to identify risky activities among their tasks, they did not try to improve the way in which they undertook their tasks to avoid the perceived ergonomics risks. Therefore, from the responses of the participants of both groups, little training was transferred to the work place.
The low level of concern of the workers about ergonomics risks and their consequences may be a key aspect in the low level of transference found. The realization of the severity of the risks is essential so that the workers be motivated to learn about the risks and to transfer the knowledge to the work setting [
54] Using immersive media in the training program has been found to increase the workers’ risk perception to a greater extent than traditional procedures. However, the overall level of concern of the workers about ergonomics risks remains low after the training.
Finally, a limitation of this work must be pointed out. The participants in the study were assigned to each experimental group in a quasi-randomized way. Each participant was randomly assigned to one out of two experimental groups (GrV and Gr3D) in such a way that the workers of the same workstation (in different shifts) were assigned to different groups. In this way, both experimental groups were composed of workers developing the same tasks in different shifts. However, potential differences between the experimental groups can be of importance for the results obtained in this work.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}





