Preschoolers’ Developmental Profiles and School-Readiness in a Low-Income Canadian City: A Cross-Sectional Survey

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
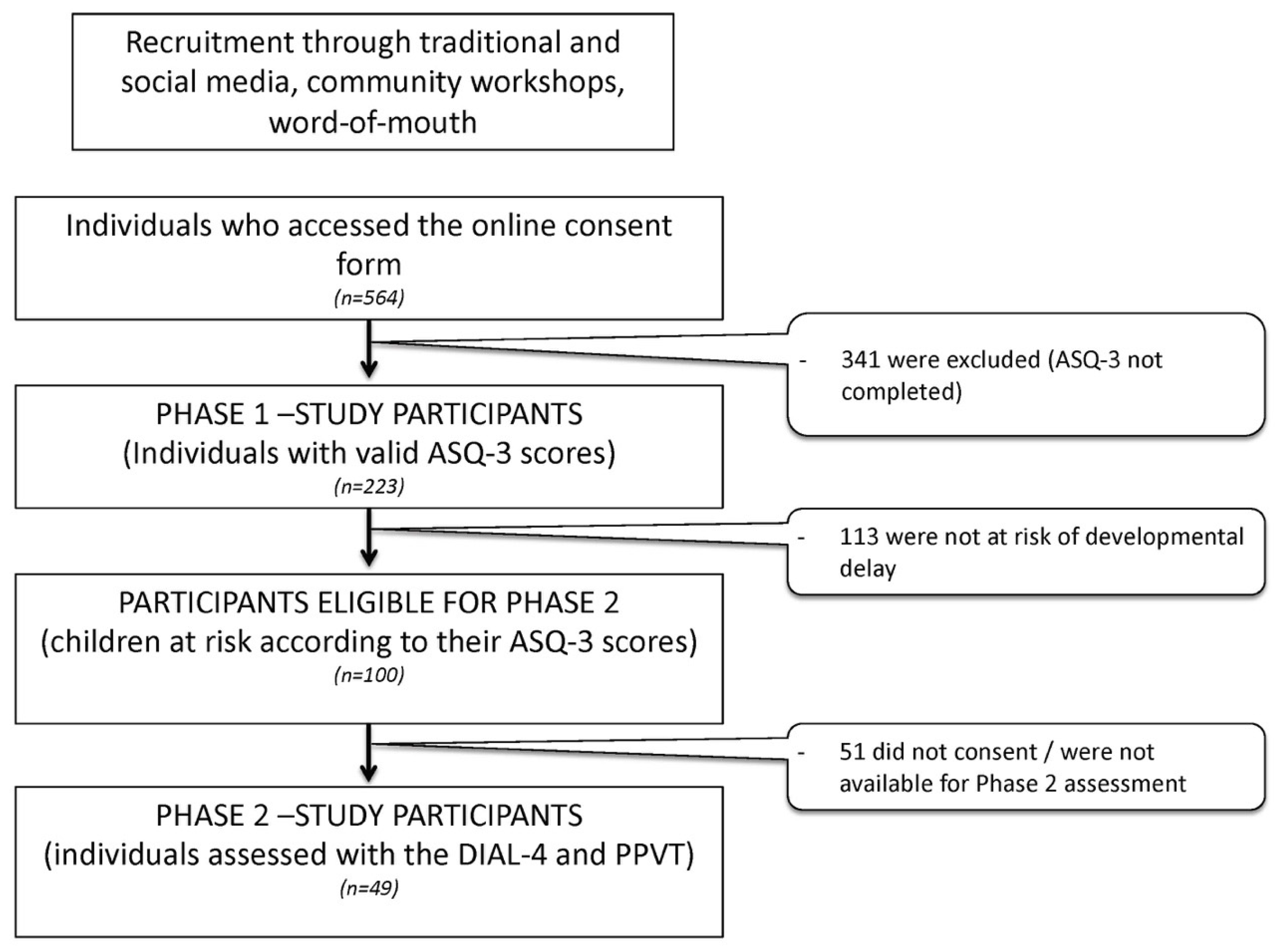
2.2. Participants and Recruitment Procedures
2.3. Data Collection Procedures and Instruments
2.3.1. Phase 1
2.3.2. Phase 2
2.4. Data Analysis
3. Results
3.1. Participants
3.2. Phase 1
3.3. Phase 2
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Britto, P.R.; Lye, S.J.; Proulx, K.; Yousafzai, A.K.; Matthews, S.G.; Vaivada, T.; Perez-Escamilla, F.; Rao, N.; Ip, P.; Fernald, L.; et al. Nurturing care: Promoting early childhood development. Lancet 2017, 389, 91–102. [Google Scholar] [CrossRef]
- Nurturing Care for Early Childhood Development: A Framework for Helping Children Survive and Thrive to Transform Health Human Potential; World Health Organization (WHO): Geneva, Switzerland, 2018.
- Adams, R.C.; Tapia, C. Council on children with disabilities. Early intervention, IDEA Part C services, and the medical home: Collaboration for best practice and best outcomes. Pediatrics 2013, 132, e1073–e1088. [Google Scholar] [CrossRef] [PubMed]
- Anderson, L.M.; Shinn, C.; Fullilove, M.T.; Scrimshaw, S.C.; Fielding, J.E.; Normand, J.; Carande-Kulis, V.; Task Force on Community Preventive Services. The effectiveness of early childhood development programs: A systematic review. Am. J. Prev. Med. 2003, 24, 32–46. [Google Scholar] [CrossRef]
- Blauw-Hospers, C.H.; Hadders-Algra, M. A systematic review of the effects of early intervention on motor development. Dev. Med. Child. Neurol. 2005, 47, 421–432. [Google Scholar] [CrossRef]
- Mackrides, P.S.; Ryherd, S.J. Screening for developmental delay. Am. Fam. Physician 2011, 84, 544–549. [Google Scholar]
- King, T.M.; Glascoe, F.P. Developmental surveillance of infants and young children in pediatric primary care. Curr. Opin. Pediatr. 2003, 15, 624–629. [Google Scholar] [CrossRef]
- Rydz, D.; Shevell, M.I.; Majnemer, A. Topical review: Developmental screening. J. Child. Neurol. 2005, 20, 4–21. [Google Scholar] [CrossRef]
- Committee on Children with Disabilities. Role of the paediatrician in family-centered early intervention services. Pediatrics 2001, 107, 1155–1157. [Google Scholar] [CrossRef]
- Garner, A.S.; Shonkoff, J.P.; Siegel, B.S.; Dobbins, M.T.; Earls, M.F.; McGuinn, L.; Pascoe, J.; Wood, D.L. Committee on Psychosocial Aspects of Child and Family Health; Committee on Early Childhood, Adoption, and Dependent Care. Early childhood adversity, toxic stress, and the role of the pediatrician: Translating developmental science into lifelong health. Pediatrics 2012, 129, e224–e231. [Google Scholar]
- Canadian Task Force on Preventive Health Care. Recommendations on screening for developmental delay. CMAJ 2016, 188, 579–587. [Google Scholar] [CrossRef]
- Dobrez, D.; Sasso, A.L.; Holl, J.; Shalowitz, M.; Leon, S.; Budetti, P. Estimating the cost of developmental and behavioral screening of preschool children in general pediatric practice. Pediatrics 2001, 108, 913–922. [Google Scholar] [CrossRef]
- Chung, C.Y.; Liu, W.Y.; Chang, C.J.; Chen, C.L.; Tang, S.F.; Wong, A.M. The relationship between parental concerns and final diagnosis in children with developmental delay. J. Child. Neurol. 2011, 26, 413–419. [Google Scholar] [CrossRef] [PubMed]
- Glascoe, F.P.; Marks, K.P. Detecting children with developmental-behavioral problems: The value of collaborating with parents. Psychol. Test. Assessm. Model. 2011, 53, 258–279. [Google Scholar]
- Piek, J.P.; Edwards, K. The identification of children with developmental coordination disorder by class and physical education teachers. Brit. J. Educ. Psychol. 2011, 67, 55–67. [Google Scholar] [CrossRef] [PubMed]
- Simard, M.; Lavoie, A.; Audet, N. Enquête Québécoise sur le Développement des Enfants à la Maternelle: Portrait Statistique Pour le Québec et ses Régions Administratives; Institut de la statistique du Québec: Quebec City, QC, Canada, 2018. [Google Scholar]
- Porterfield, S.L.; McBride, T.D. The effect of poverty and caregiver education on perceived need and access to health services among children with special health care needs. Am. J. Public Health 2007, 97, 323–329. [Google Scholar] [CrossRef]
- Magnusson, D.; Palta, M.; McManus, B.; Benedict, R.E.; Durkin, M.S. Capturing unmet therapy need among young children with developmental delay using national survey data. Acad. Pediatr. 2016, 16, 145–153. [Google Scholar] [CrossRef]
- Frohlich, K.L.; Potvin, L. Transcending the known in public health practice: The inequality paradox: The population approach and vulnerable populations. Am. J. Public Health 2008, 98, 216–221. [Google Scholar] [CrossRef]
- Baron, G.; Roy, M.; Stronach, N.; Roy, M.-A.; Généreux, M. Mieux répondre aux besoins des communautés linguistiques et culturelles de l’Estrie; Direction de santé publique de l’Estrie: Sherbrooke, QC, Canada, 2016. [Google Scholar]
- Statistic Canada. 2016 Canadian Census; Statistic Canada: Ontario, ON, Canada, 2016. [Google Scholar]
- Reason, P.; Bradbury, H. Handbook of Action Research: Participative Inquiry and Practice; SAGE Publications: London, UK, 2001. [Google Scholar]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef]
- Squires, J.; Bricker, D. Ages & Stages Questionnaires: A Parent-Completed System, 3rd ed.; Brookes Publishing: Baltimore, MD, USA, 2009. [Google Scholar]
- Mardell, C.; Goldenberg, D.S. Developmental Indicators for the Assessment of Learning Manual, 2nd ed.; Pearson: Bloomington, MN, USA, 2011. [Google Scholar]
- Dunn, L.M.; Theriault-Whalen, C. Échelle de Vocabulaire en Images Peabody: EVIP; PSYCAN: Toronto, ON, Canada, 1993. [Google Scholar]
- Mitchell, S. Comprehensive Assessment Systems in Preschool Development and Expansion Grant States; Preschool Development and Expansion Grant Technical Assistance (PDG TA): Washington, DC, USA, 2016. [Google Scholar]
- Coughlan, K.A. Test review: Developmental Indicators for the Assessment of Learning, Fourth Edition (DIAL-4), by C. Mardell-Czudnowski & D.S. Goldenberg. J. Psychoeduc Assess. 2015, 33, 291–295. [Google Scholar]
- Campbell, J. Book review: Peabody Picture Vocabulary Test, third edition. J. Psychoeduc. Assess 1998, 16, 334–338. [Google Scholar] [CrossRef]
- Rosenberg, S.A.; Zhang, D.; Robinson, C.C. Prevalence of developmental delays and participation in early intervention services for young children. Pediatrics 2008, 121, e1503–e1509. [Google Scholar] [CrossRef]
- Phoenix, M.; Rosenbaum, P. Presenting the model of risk, disability and hard-to-reach families to inform early intervention services. Disabil. Rehabil. 2019, 41, 244–249. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Phase 1 Only n = 174 (%) | Phases 1 + 2 n = 49 (%) |
|---|---|---|
| Child sociodemographic information | ||
| Child’s age (years) | ||
| 2 | 37 (21.3) | 18 (36.7) |
| 3 | 74 (42.5) | 13 (26.5) |
| 4 | 43 (24.7) | 12 (24.5) |
| 5 | 20 (11.5) | 6 (12.2) |
| Child sex | ||
| Male | 78 (52.3) | 33 (67.3) |
| Female | 71 (47.7) | 16 (32.7) |
| Child’s birth country | ||
| Canada | 156 (91.8) | 37 (84.1) |
| Other country | 14 (8.2) | 7 (15.9) |
| Parents and families’ sociodemographic information | ||
| Number of children in the family | ||
| 1 | 36 (21.1) | 8 (16.3) |
| 2 | 98 (57.3) | 32 (65.3) |
| 3 or more | 37 (21.6) | 9 (18.4) |
| Number of children between 2 and 5 years old in the family | ||
| 1 | 130 (74.7) | 34 (69.4) |
| 2 | 44 (25.3) | 15 (30.6) |
| Residence in 1 of the 4 low socioeconomic neighbourhoods | ||
| Yes | 21 (12.5) | 6 (12.2) |
| No | 147 (87.5) | 43 (87.8) |
| Relation to the child | ||
| Mother | 152 (87.4) | 43 (87.8) |
| Father | 22 (12.6) | 6 (12.2) |
| Parent age (years) | ||
| 18–30 | 48 (28.1) | 11 (22.9) |
| 31–40 | 109 (63.7) | 33 (68.8) |
| 41 or more | 14 (8.2) | 4 (8.3) |
| Ethnicity | ||
| Caucasian | 161 (94.2) | 42 (87.5) |
| Other | 10 (5.8) | 6 (12.5) |
| Civil status | ||
| Common law union | 94 (55.0) | 26 (54.2) |
| Married | 56 (32.7) | 15 (31.3) |
| Other | 21 (12.3) | 7 (14.5) |
| Language | ||
| French | 160 (93.6) | 44 (91.7) |
| English | 8 (4.7) | 2 (4.2) |
| Other | 3 (1.8) | 2 (4.2) |
| Education of the parent | ||
| Elementary school | 5 (2.9) | 0 (0.0) |
| High school | 29 (17.0) | 10 (20.8) |
| College | 33 (19.3) | 9 (18.8) |
| University | 104 (60.8) | 29 (60.4) |
| Family income ($) | ||
| <10,000 | 3 (1.8) | 1 (2.1) |
| 10,000 to 29,999 | 17 (9.9) | 2 (4.2) |
| 30,000 to 59,999 | 24 (14.0) | 8 (16.7) |
| 60,000 to 79,999 | 25 (14.6) | 10 (20.8) |
| 80,000 to 99,999 | 29 (16.7) | 8 (16.7) |
| 100,000 to 149,999 | 56 (32.7) | 15 (31.3) |
| >150,000 | 14 (8.2) | 4 (8.3) |
| Parent occupation | ||
| Working full time—salary | 84 (48.3) | 30 (61.2) |
| Working part time—salary | 21 (12.1) | 3 (6.1) |
| Independent worker | 17 (9.8) | 2 (4.1) |
| At home | 16 (9.2) | 2 (4.1) |
| Searching for a job | 2 (1.1) | 0 (0.0) |
| On family leave | 15 (8.6) | 5 (10.2) |
| Social welfare | 5 (2.9) | 1 (2.0) |
| Studying | 15 (8.6) | 4 (8.2) |
| Variables | Phase 1 Only n = 174 (%) | Phases 1 + 2 n = 49 (%) |
|---|---|---|
| Parents’ developmental concerns | ||
| Parental concerns on the ASQ-3 | ||
| Yes | 80 (46.2) | 38 (77.6) |
| No | 93 (53.8) | 11 (22.4) |
| Parents’ reported use of programs and services | ||
| Kindergarten type | ||
| Publicly-funded | 113 (65.7) | 30 (61.2) |
| Other | 59 (34.3) | 19 (38.8) |
| Most frequent health care professional accessed | ||
| Doctor | 158 (91.3) | 44 (93.6) |
| Speech therapist | 31 (17.8) | 14 (28.6) |
| Physiotherapist | 17 (9.8) | 7 (14.3) |
| Occupational therapist | 13 (7.5) | 4 (8.2) |
| Psychoeducator | 10 (5.7) | 6 (12.2) |
| Social worker | 5 (2.9) | 6 (12.2) |
| Other | 8 (4.6) | 8 (16.4) |
| Number of health and community services known | ||
| One or no program | 13 (7.5) | 6 (12.2) |
| Two or more programs | 161 (92.5) | 43 (87.8) |
| Number of health and community services used | ||
| One or no program | 72 (41.4) | 29 (59.2) |
| Two or more programs | 102 (58.6) | 20 (40.8) |
| Risk of Developmental Delay Based on ASQ-3 Score | n (%) |
|---|---|
| Not at risk in any domain | 123 (55.2) |
| At risk in at least one domain | 100 (44.8) |
| In one domain | 50 (22.4) |
| In two domains | 21 (9.4) |
| In three or more domains | 29 (13.0) |
| Risk of developmental delay by ASQ-3 domain | n (%) |
| Fine motor skills | 59 (26.5) |
| Gross motor skills | 39 (17.5) |
| Communication | 36 (16.1) |
| Problem solving skills | 35 (15.7) |
| Personal social skills | 28 (12.6) |
| School-Readiness Risk Category | n (%) |
|---|---|
| Not at risk | 15 (30.6) |
| At risk in at least one domain | 34 (69.4) |
| One domain | 18 (36.7) |
| Two domains | 9 (18.4) |
| Three domains | 3 (6.1) |
| Four domains | 3 (6.1) |
| School-Readiness Risk by DIAL-4/PPVT domain | n (%) |
| DIAL-4 Motor Skills | 12 (24.5) |
| DIAL-4 Concepts | 8 (16.3) |
| DIAL-4 Self-help | 16 (32.7) |
| DIAL-4 Social | 18 (36.7) |
| PPVT Communication | 8 (16.3) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Camden, C.; Héguy, L.; Casoli, M.; Roy, M.; Rivard, L.; Berbari, J.; PPOP Research Team; Couture, M. Preschoolers’ Developmental Profiles and School-Readiness in a Low-Income Canadian City: A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2020, 17, 2529. https://doi.org/10.3390/ijerph17072529
Camden C, Héguy L, Casoli M, Roy M, Rivard L, Berbari J, PPOP Research Team, Couture M. Preschoolers’ Developmental Profiles and School-Readiness in a Low-Income Canadian City: A Cross-Sectional Survey. International Journal of Environmental Research and Public Health. 2020; 17(7):2529. https://doi.org/10.3390/ijerph17072529
Chicago/Turabian StyleCamden, Chantal, Léa Héguy, Megan Casoli, Mathieu Roy, Lisa Rivard, Jade Berbari, PPOP Research Team, and Mélanie Couture. 2020. "Preschoolers’ Developmental Profiles and School-Readiness in a Low-Income Canadian City: A Cross-Sectional Survey" International Journal of Environmental Research and Public Health 17, no. 7: 2529. https://doi.org/10.3390/ijerph17072529
APA StyleCamden, C., Héguy, L., Casoli, M., Roy, M., Rivard, L., Berbari, J., PPOP Research Team, & Couture, M. (2020). Preschoolers’ Developmental Profiles and School-Readiness in a Low-Income Canadian City: A Cross-Sectional Survey. International Journal of Environmental Research and Public Health, 17(7), 2529. https://doi.org/10.3390/ijerph17072529