Computing and Oral Health: Mobile Solution for Collecting, Data Analysis, Managing and Reproducing Epidemiological Research in Population Groups

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
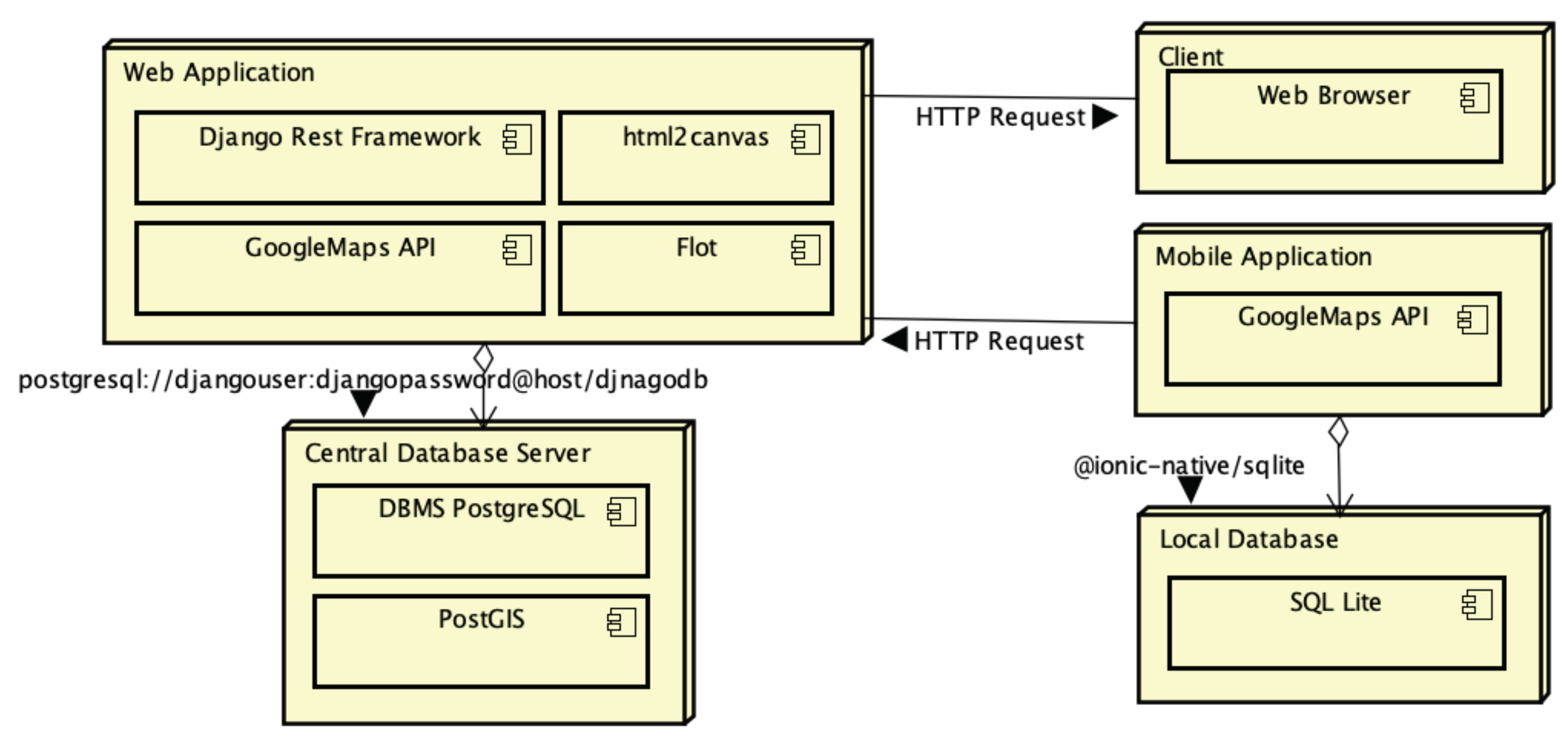
2.1. NutriOdonto Environment Architecture
- Portal module: containing the functions for recording information about project execution, such as news about the execution of epidemiological survey actions, documents, photos and videos.
- Data collection module: which concentrates the data collection functions on health actions, organized in the form of campaigns, characterization of school units, principals and students, as well as the application of questionnaires and oral examinations.
- Administration module: deals with security mechanisms of the computing environment, such as access control mechanisms and encryption of information stored in the database.
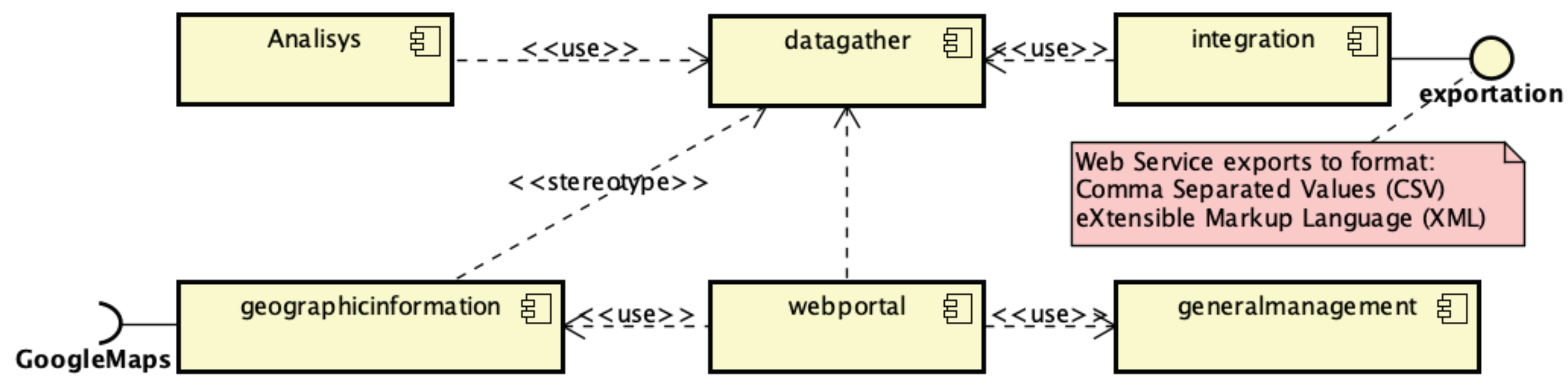
- Integration module: allows data export to external analysis tools in the CSV and XML formats.
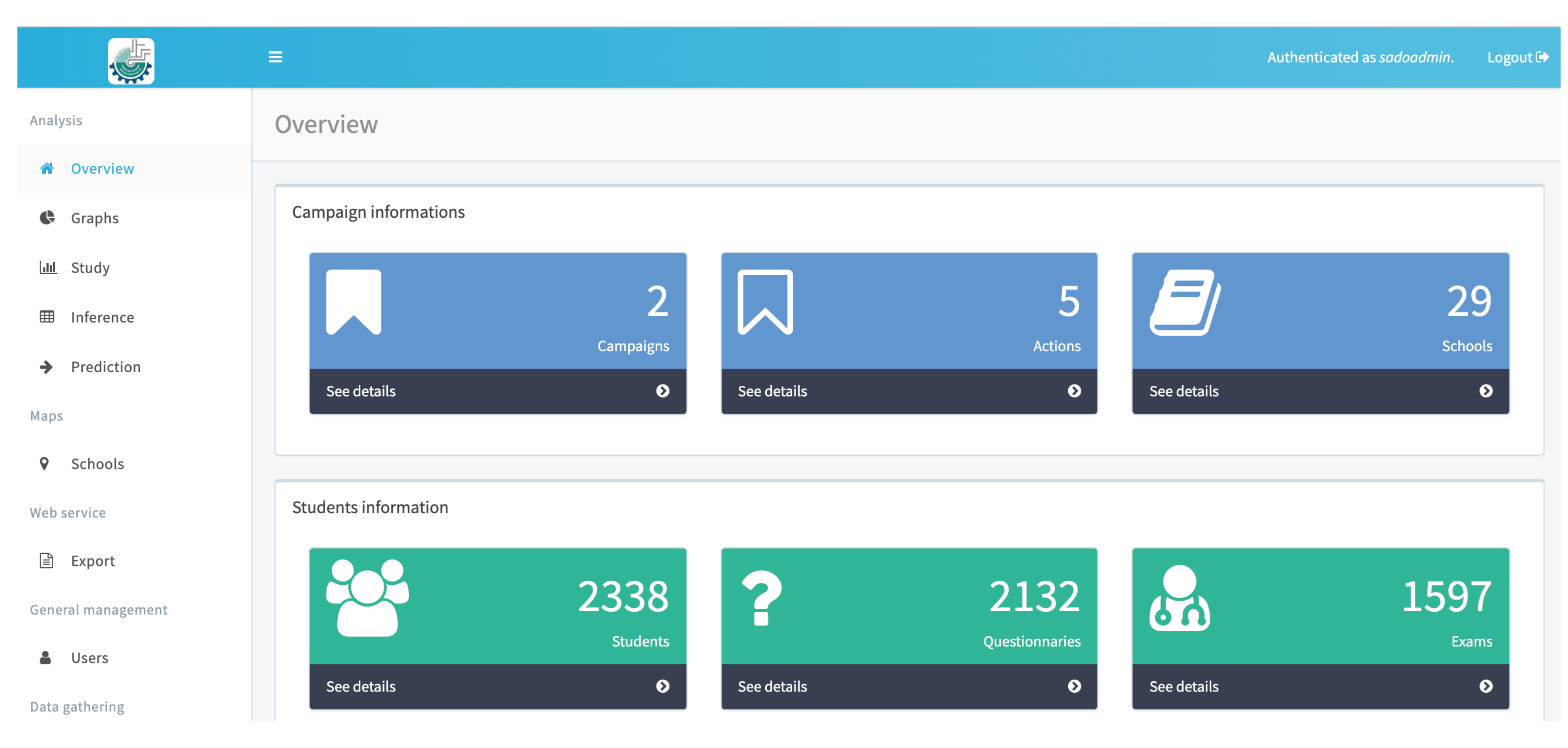
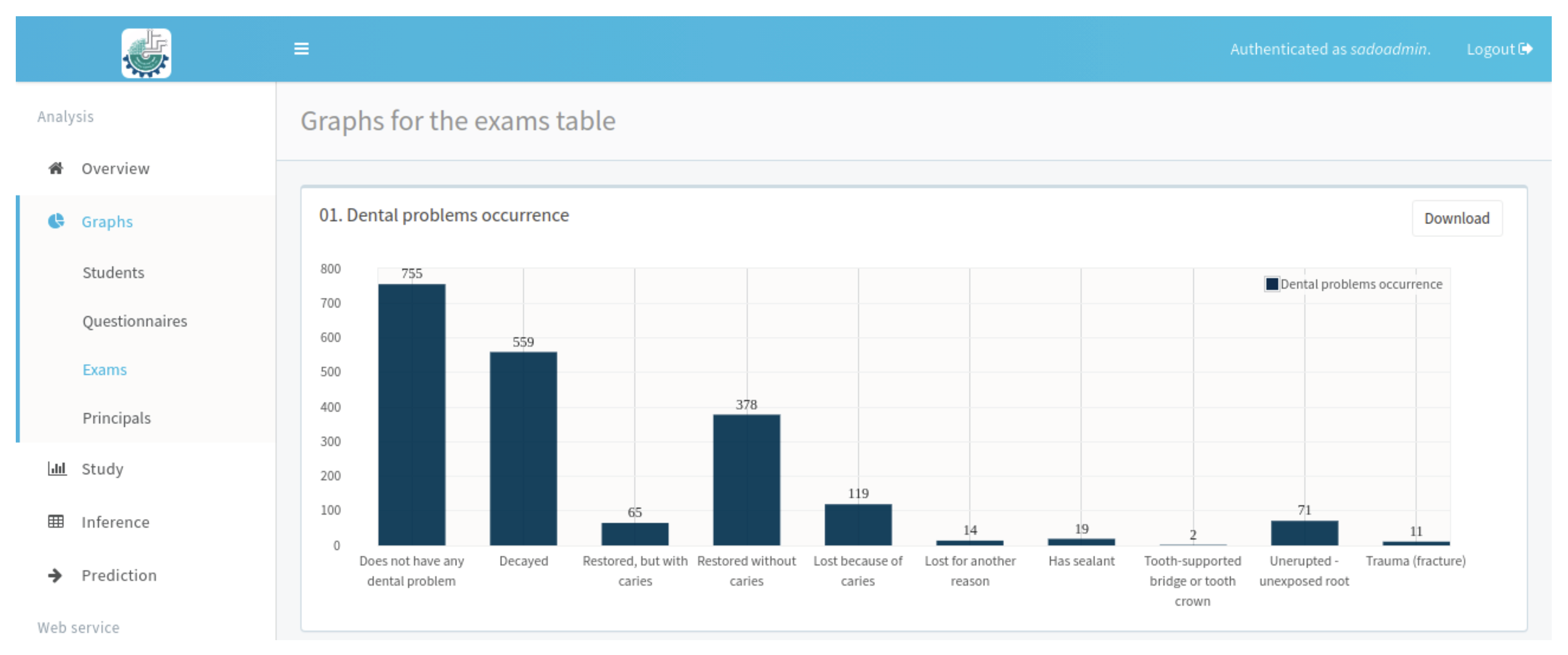
- Analysis module: implements the information analysis mechanisms.
- Geographic module: performs data management through a geographic information system.
2.2. NutriOdonto Functional and Non-Functional Requirements
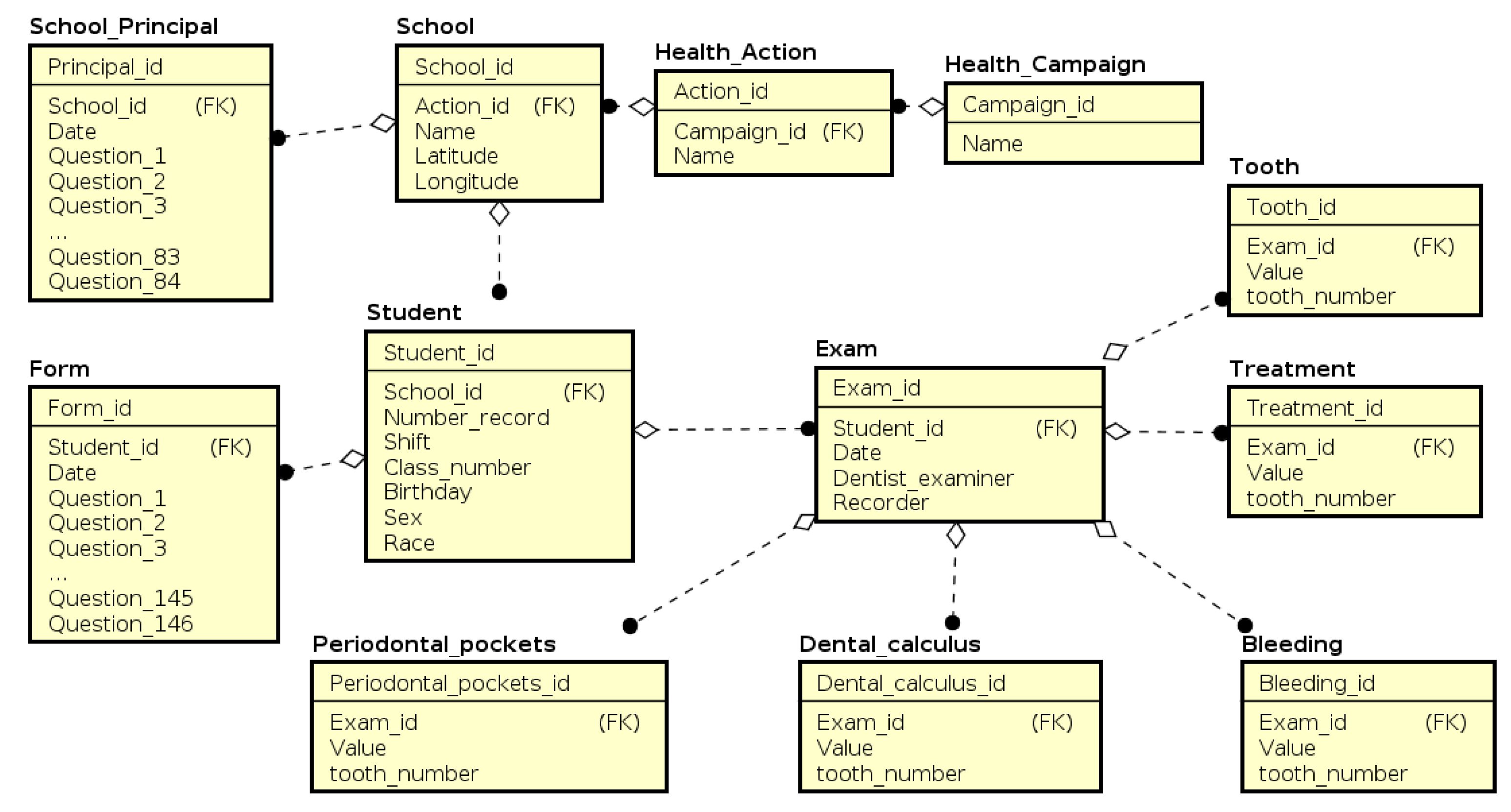
2.3. NutriOdonto Data Structure
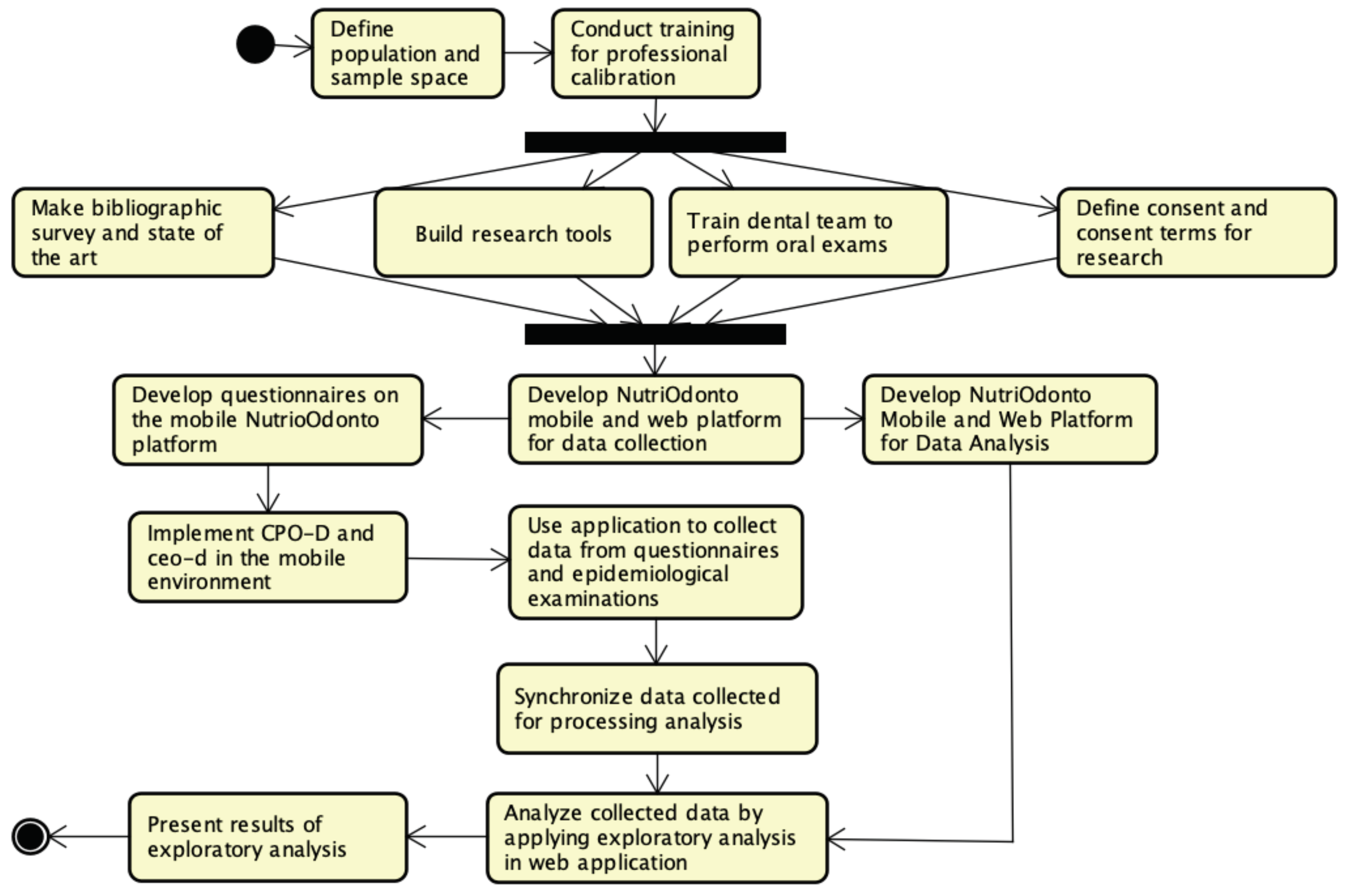
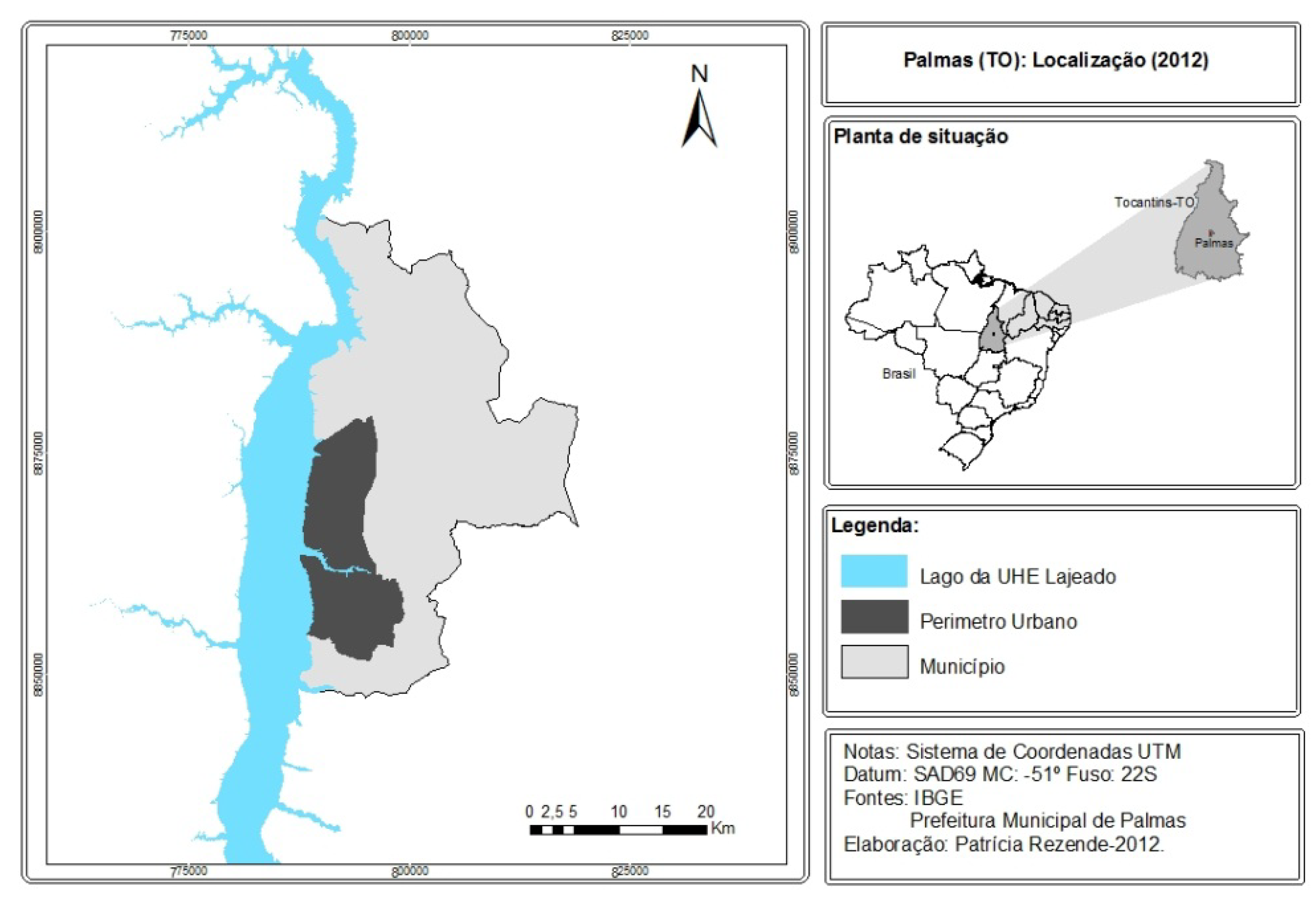
2.4. Research Execution
- The last year of elementary school was considered a coherent parameter for evaluation of the reflexes of exposure to public policies focused on adolescents, and the Brazilian educational system predicts a grade-school adjustment in which ideally, students between the ages of 13 and 15 should attend the 9th grade of elementary school [17];
- The study of dental caries in adolescents is not very common, both in Brazil and in other countries (including developed ones), leaving a gap in the oral health knowledge of this population segment [19];
- Although the age of 12 is recommended by the WHO and its CPO-D is used as an international standard for the evaluation of dental caries, our study privileged the age of 15, as it is also important since its supposed increase in relation to the age of 12 indicates the degree of severity of the disease [20];
- The 9th graders have a level of education that allows them better reading and comprehension for use of self-administered questionnaire [17].
3. Results
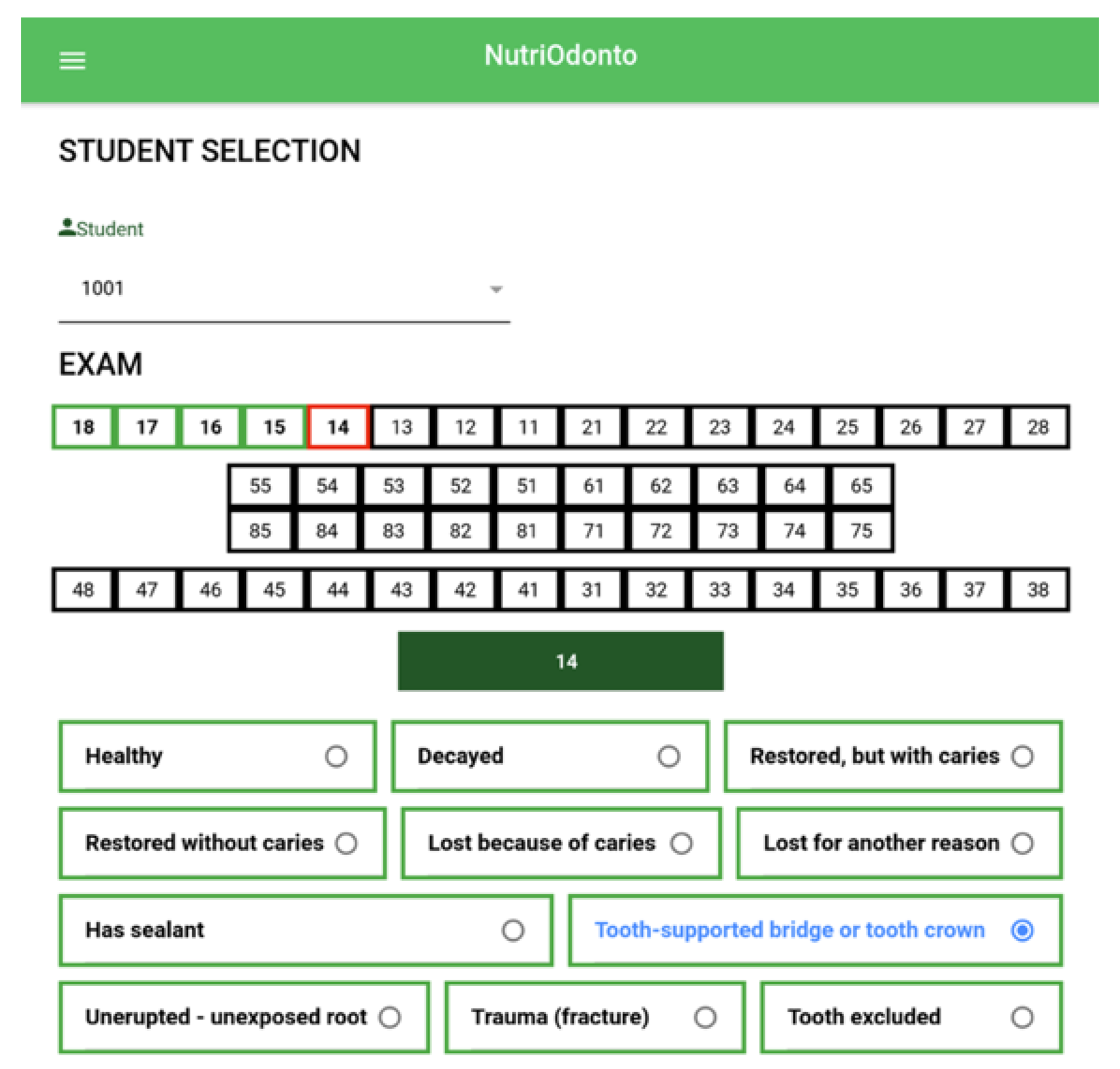
3.1. NutriOdonto Mobile App
3.2. Data Collection Application
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Teixeira, D.S.d.C.; Frazao, P.; Alencar, G.P.; Baquero, O.S.; Narvai, P.C.; Lebrao, M.L.; de Oliviera Duarte, Y.A. Estudo prospectivo da perda dentária em uma coortede idosos dentados. Cadernos de Saúde Pública 2016, 32, e00017215. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Petersen, P.E. World Health Organization global policy for improvement of oral health-World Health Assembly 2007. Int. Dental J. 2008, 58, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Cypriano, S.; Sousa, M.d.L.R.d.; Wada, R. Avaliação de índices CÓD. simplificados em levantamentos epidemiológicos de cárie dentária. Revista de Saúde Pública 2005, 39, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Pinto, V.G. Programação em saúde bucal. In Saúde Bucal Coletiva; Santos: São Paulo, Brazil, 2011. [Google Scholar]
- World Health Organization. Calibration of Examiners for Oral Health Epidemiology Surveys; World Health Organization: Geneva, Switzerland, 1993. [Google Scholar]
- Queiroz, C.J.P.; Calmon, N.S.S.; da Costa, A.S. O Papel do Gestor Educacional no uso das Tecnologias da Informação e Comunicação: Possibilidades e Limites. Encontro Internacional de Formação de Professores e Fórum Permanente de Inovação Educacional, v. 9, n. 1. 2016. Available online: https://eventos.set.edu.br/index.php/enfope/article/view/2072 (accessed on 20 November 2019).
- Turchi, L.M.; Morais, J.M. Políticas de Apoio à Inovação Tecnológica no Brasil: Avanços Recentes, Limitações e Propostas de Ações. 2017. Available online: http://www.ipea.gov.br/portal/images/stories/PDFs/livros/livros/171103_politicas_de_apoio_a_inovacao.pdf (accessed on 20 November 2019).
- Schmeil, M.A. Saúde e Tecnologia da Informação e Comunicação. Fisioterapia em Movimento 2013, 26, 477–478. [Google Scholar] [CrossRef][Green Version]
- Rocha, T.A.H.; Fachini, L.A.; Thume, E.; da Silva, N.C.; Barbosa, A.C.Q.; do Carmo, M.; Rodrigues, J.M. Saúde Móvel: Novas perspectivas para a oferta de serviços em saúde. Epidemiologia e Serviços de Saúde 2016, 25, 159–170. [Google Scholar] [PubMed]
- Tibes, C.M.S.; Dias, J.D.; Zem-Mascarenhas, S.H. Aplicativos móveis desenvolvidos para a área da saúde no Brasil: Revisão integrativa da literatura. Revista Mineira de Enfermagem 2014, 18, 471–486. [Google Scholar]
- Barra, D.C.C.; Paim, S.M.S.; Dal Sasso, G.T.M.; Colla, G.W. Métodos para desenvolvimento de aplicativos móveis em saúde: Revisão integrativa da literatura. Texto Contexto-Enfermagem 2017, 26. [Google Scholar] [CrossRef][Green Version]
- Ferreira, A.; Pauferro, B.C.S.; da Cruz, G.M.; Trezena, S.; Batisat, R.W.C. O Uso das Tecnologias de Informação e Comunicação no Ensino e em Odontologia. Revista da AcBO 2018, 8. [Google Scholar]
- Brasil. Constituição da República Federativa do Brasil: Promulgada em 5 de Outubro de 1988, 4th ed.; Constituição (1988); Saraiva: São Paulo, Brazil, 1990. [Google Scholar]
- Pamas-TO. Secretaria Municipal de Saúde. Coordenação de Saúde Bucal. Semus Palmas. Available online: https://saude.palmas.to.gov.br/ (accessed on 20 December 2019).
- Brasil Ministério da Saúde. Secretaria de Atenção à Saúde. Secretaria de Vigilância em Saúde. SB Brasil 2010: Pesquisa Nacional de Saúde Bucal: Resultados principais/Ministério da Saúde. Secretaria de Atenção à Saúde. Secretaria de Vigilância em Saúde. Brasília: Ministério da Saúde, Palmas. 2012. Available online: http://bvsms.saude.gov.br/bvs/publicacoes/pesquisa_nacional_saude_bucal.pdf (accessed on 20 December 2019).
- Palmas-TO. Secretaria Municipal de Educação. Available online: https://www.palmas.to.gov.br/secretaria/educacao/noticia/1507385/rede-municipal-de-ensino-avanca-na-oferta-de-matriculas/ (accessed on 5 May 2018).
- Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa Nacional de Saúde Escolar (PeNSE)—2015. Rio de Janeiro (RJ), IBGE; 2016. Available online: https://biblioteca.ibge.gov.br/visualizacao/livros/liv97870.pdf (accessed on 16 October 2017).
- Instituto Brasileiro de Geografia e Estatística (IBGE). Panorama Palmas-Tocantins. 2018. Available online: https://cidades.ibge.gov.br/brasil/to/palmas/panorama (accessed on 10 December 2019).
- Gushi, L.L.; Soares, M.d.C.; Forni, T.I.B.; Vieira, V.; Wada, R.S.; de Sousa, M.d.L.R. Cárie dentária em adolescentes de 15 a 19 anos de idade no Estado de São Paulo, Brasil, 2002. Cadernos Saúde Pública 2005, 21, 1383–1391. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, A.G.R.C.; Unfer, B.; Costa, I.d.C.C.; Arcieri, R.M.; Guimaraes, L.O.C.; Saliba, N.A. Levantamentos epidemiológicos em saúde bucal: Análise da metodologia proposta pela Organização Mundial da Saúde. Revista Brasileira de Epidemiologia 1998, 1, 177–189. [Google Scholar] [CrossRef]
- Bazolli, J.A. Os desafios da democracia participativa e a complementariedade na democracia representativa: O Plano de Regularização Fundiária Sustentável e Participativo de Palmas/TO. in Poder político e políticas públicas: Desafios e dimensões contemporâneas do desenvolvimento. Eduft 2017. [Google Scholar]
- Antunes, J.L.F.; Narvai, P.C. Políticas de saúde bucal no Brasil e seu impacto sobre as desigualdades em saúde. Revista de Saúde Pública 2010, 44, 360–365. [Google Scholar] [CrossRef] [PubMed]
- Narvai, P.C. Está ocorrendo um declínio de cárie no Brasil. J. Aboprev 1996, 6. [Google Scholar]
- SPSS Inc. SPSS Complex Samples 15.0; SPSS: Chicago, IL, USA, 2006. [Google Scholar]
- PORTARIA INST Nº 518, de 14 de junho de 2016. Diário Oficial do Estado do Tocantins Nº 1.533, SEMUS/GAB, Palmas, Brazil, 28 Jun 2016. Available online: https://docero.com.br/doc/1css5c (accessed on 25 November 2019).
- Palmas-TO. Secretaria Municipal de Saúde. Palmenses já Podem Encontrar Todos os Serviços Oferecidos Pelo SUS com o app Saúde Palmas. Available online: http://www.palmas.to.gov.br/secretaria/saude/noticia/1505902/palmenses-ja-podem-encontrar-todos-os-servicos-oferecidos-pelo-sus-com-o-app-saude-palmas/617 (accessed on 31 October 2017).
- Lopes, J.E.; Heimann, C. Uso das Tecnologias da Informação e Comunicação nas Ações Médicas a Distância: Um Caminho Promissor a ser Investido na Saúde Pública. J. Health Inf. 2016, 8. [Google Scholar]
- Singhal, S.; Jain, S.; Rathi, M.; Sinha, A. Smart technologies to build healthcare models for vision impairment. In Advanced Classification Techniques for Healthcare Analysis; IGI Global: Hershey, PA, USA, 2019; pp. 259–285. Available online: https://www.igi-global.com/chapter/smart-technologies-to-build-healthcare-modelsfor-vision-impairment/222150 (accessed on 10 November 2019).
- Detsomboonrat, P.; Pisarnturakit, P.P. Development and Evaluation: The Satisfaction of Using an Oral Health Survey Mobile Application. Telemed. e-Health 2019, 25, 55–59. [Google Scholar] [CrossRef] [PubMed]
- De Barros Lima, A.M.E.; Rodrigues, C.A.Q.; Haikal, D.S.A.; Silveira, M.F.; Mendes, D.C.; Oliviera, P.M.; Andrade, A.F.; de Feritas, C.V.; Pordeus, I.A. Desenvolvimento de um programa de computador para levantamentos epidemiológicos sobre condições de saúde bucal. Unimontes Científica 2012, 14, 30–42. Available online: http://rucunimontesbr/indexphp/unicientifica/article/view/115 (accessed on 15 November 2019).
- Da Silva Bonome, K.; di Santo, C.C.; Prado, C.S.; Sousa, F.S.; Pisa, I.T. Disseminação do uso de Aplicativos Móveis na Atenção à Saúde. In Anais do XIII Congresso Brasileiro em Informática em Saúde CBIS. 2012. Available online: https://www.researchgate.net/conference-event/CBIS_Congresso-Brasileiro-de-Informatica-em-Saude_2012/11685 (accessed on 21 November 2019).
- Qari, A.H. Assessing the Quality of Mobile Apps for Oral Health: Content Analysis and Usability. 2019. Available online: https://hdl.handle.net/2144/37387 (accessed on 20 November 2019).
- Pereira, I.M.; Bonfim, D.; Peres, H.H.C.; Goes, R.F.; Gaidzinski, R.R. Tecnologia móvel para coleta de dados de pesquisas em saúde. Acta Paulista de Enfermagem 2017, 30, 479–488. [Google Scholar] [CrossRef][Green Version]
- Sundefeld, M.L.M.M.; Gotlieb, S.L.D. Sistema computacional para índices de cárie dentária: Banco de dados e análise estatística. Revista de Saúde Pública 1996, 30, 421–432. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Dehling, T.; Gao, F.; Schneider, S.; Sunyaev, A. Exploring the far side of mobile health: Information security and privacy of mobile health apps on iOS and Android. JMIR mHealth uHealth 2015, 3, e8. [Google Scholar] [CrossRef] [PubMed]
- De Andrade, F.R.; Narvai, P.C.; Montagner, M.Â. Dificuldades Éticas na Realização da Pesquisa Nacional de Saúde Bucal 2010. 2018. Available online: https://repositorio.unb.br/handle/10482/33674 (accessed on 20 November 2019).
- Mattos, G.C.M.; Ferreira, E.F.; Leite, I.C.G.; Greco, R.M. A inclusão da equipe de saúde bucal na Estratégia Saúde da Família: Entraves, avanços e desafios. Ciência Saúde Coletiva 2014, 19, 373–382. [Google Scholar] [CrossRef] [PubMed]
- Roncalli, A.G. Projeto SB Brasil 2010: Elemento Estratégico na Construção de um Modelo de Vigilância em Saúde Bucal. 2010. Available online: https://www.scielosp.org/scielo.php?pid=S0102-311X2010000300001&script=sci_arttext&tlng=pt (accessed on 30 November 2019).













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Module: Portal |
| RF0001: Record Registration Information: Registration, update and exclusion of news, photos and movies record of epidemiological survey of actions undertaken during the campaigns to document the field activities. It is a set of mechanisms that help to share information about the actions taken by the epidemiological survey team. |
| Module: Administration |
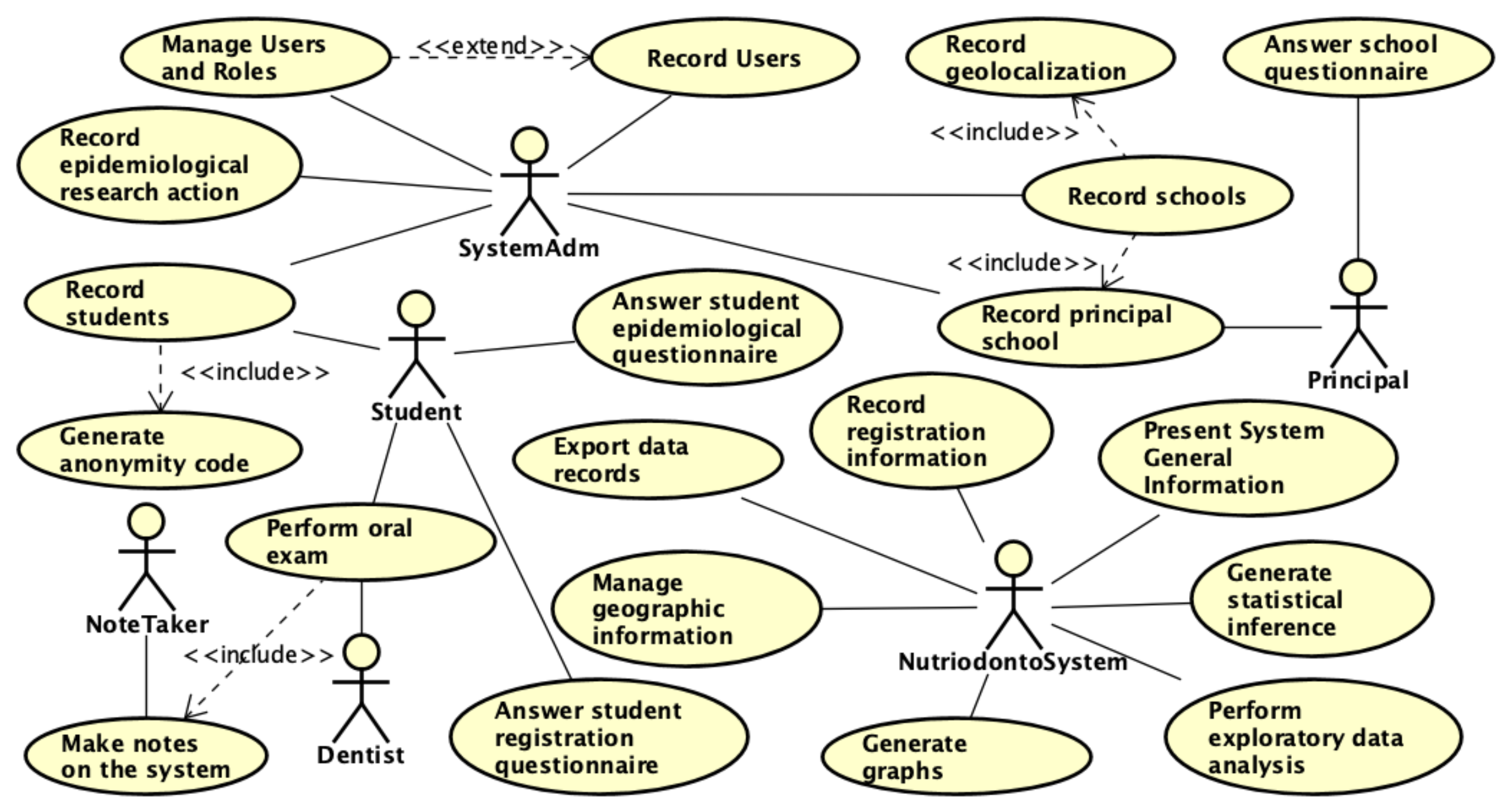
| RF0010: Record Users: Registration, update and exclusion of system users. Includes queries by name present a list of users registered. |
| RF0011: Manage Users and Roles: Registration, update and exclusion of system users roles defining user access rules to the environment and data stored in the system database Includes queries by role name present a list of roles registered in the system. |
| Module: Integration |
| RF0012: Export Data Records: This module is responsible for exporting database data to external systems through web services. The export is done through XML or JSON files allowing the manipulation of the data by other external tools. |
| Module: Data Gather |
| RF0002: Manage campaign (Record epidemiological research action): Registration, update and exclusion of campaign data in the system. Includes queries by name present a list of registered campaign. A campaign is a way of classifying major events for epidemiological survey, for example, held annually. |
| RF0003: Manage actions (Record epidemiological research action): Registration, update and exclusion of actions data in the system. Includes queries by name present a list of registered actions. It is a way of classifying small events within an epidemiological survey campaign |
| RF0004: Record schools: Registration, update and exclusion of school data in the system through the management of school name and geolocation information. The schools are included in a previously registered action and are plotted on a thematic map of the locations served in an epidemiological survey campaign. Includes queries by school name present a list of registered schools. |
| RF0005: Record principal school: Registration, update and exclusion of school data characterization in the system by completing the director’s questionnaire. Includes queries by school name present a list of registered actions. In this case the principal should answer the questionnaire based on the characteristics of the school. The principal questionnaire has 84 questions. |
| RF0006: Record student: Registration, update and exclusion of student registration data in the system through information on gender, date of birth and race. The student reports secret registration code, school and class. Includes queries by secret registration code present a list of students associated with their respective school. |
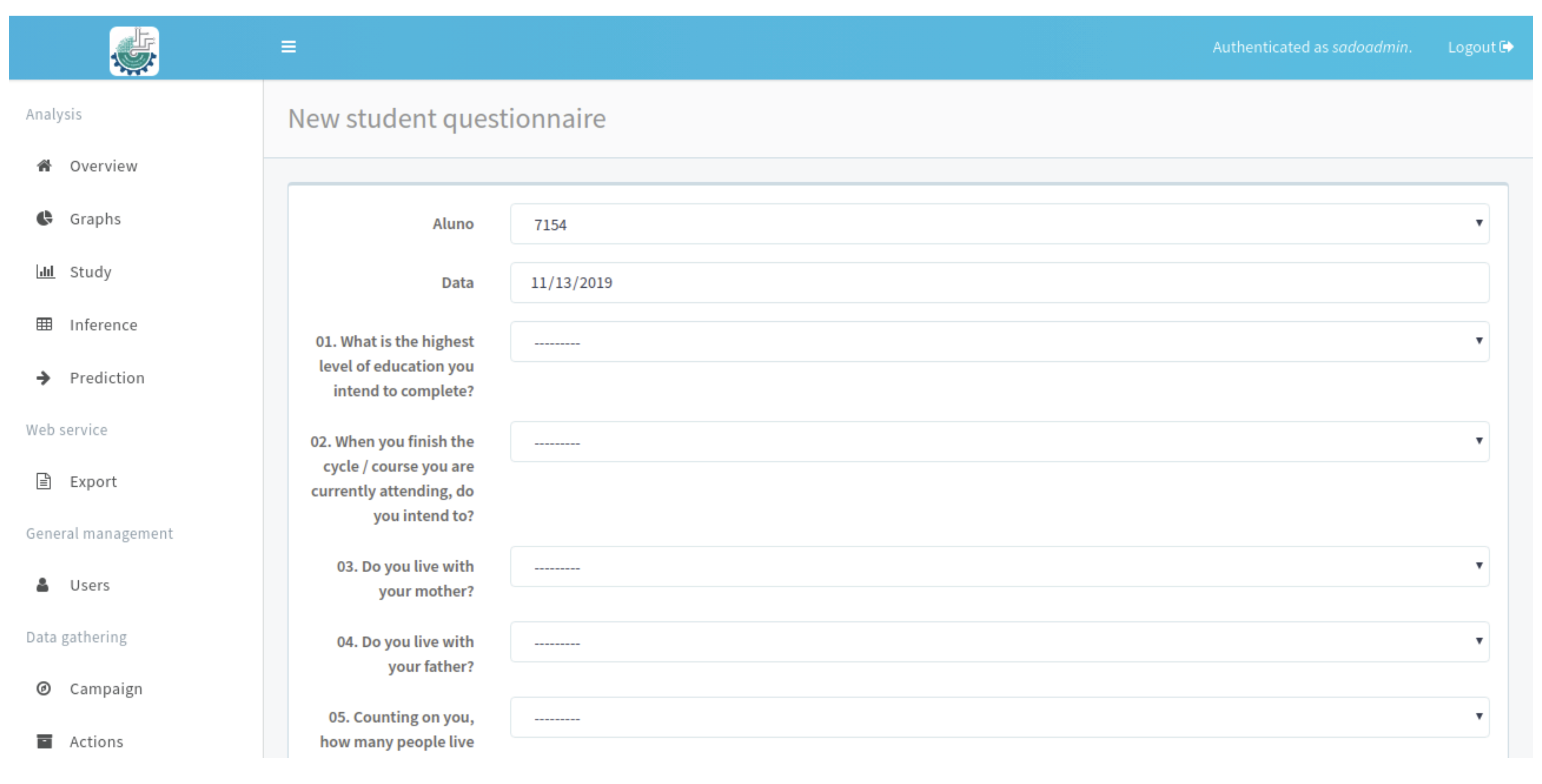
| RF0007: Answer student registration questionnaire: Registration, update and exclusion of student questionnaire from secret registration code, school and class. The student reports their code in the mobile or web environment and completes the questionnaire. The environment preserves student anonymity through an encrypted key (secret code). |
| RF0008: Answer student epidemiological questionnaire: Registration, update and exclusion of student epidemiological data present in the questionnaire. The student enters the secret registration code and initiates the completion of the questionnaire by selecting the options presented that are most appropriate to his or her behavioral profile. The epidemiological questionnaire has 145 questions. Includes queries by secret registration code present a list of students associated with their respective school. |
| RF0009: Perform oral exam: Registration, update and exclusion of student epidemiological exam. The filling is performed by a note taker from the dentist information. In this case, the note taker requests the student’s secret code to be filled in and begins to fill in the forms from the dentist’s instructions. Two exams are performed: dental caries and need for treatment and periodontal condition. |
| Module: Analysis |
| RF0013: Generate Graphs: Function responsible for presenting a set of statistical analyzes from the data collected by the campaigns and epidemiological survey actions. It is a visualization mechanism that performs exploratory analyzes to characterize and summarize the data collected by the teams. The informations are classified based on campaigns, actions and time parameters. |
| Module: Geographical |
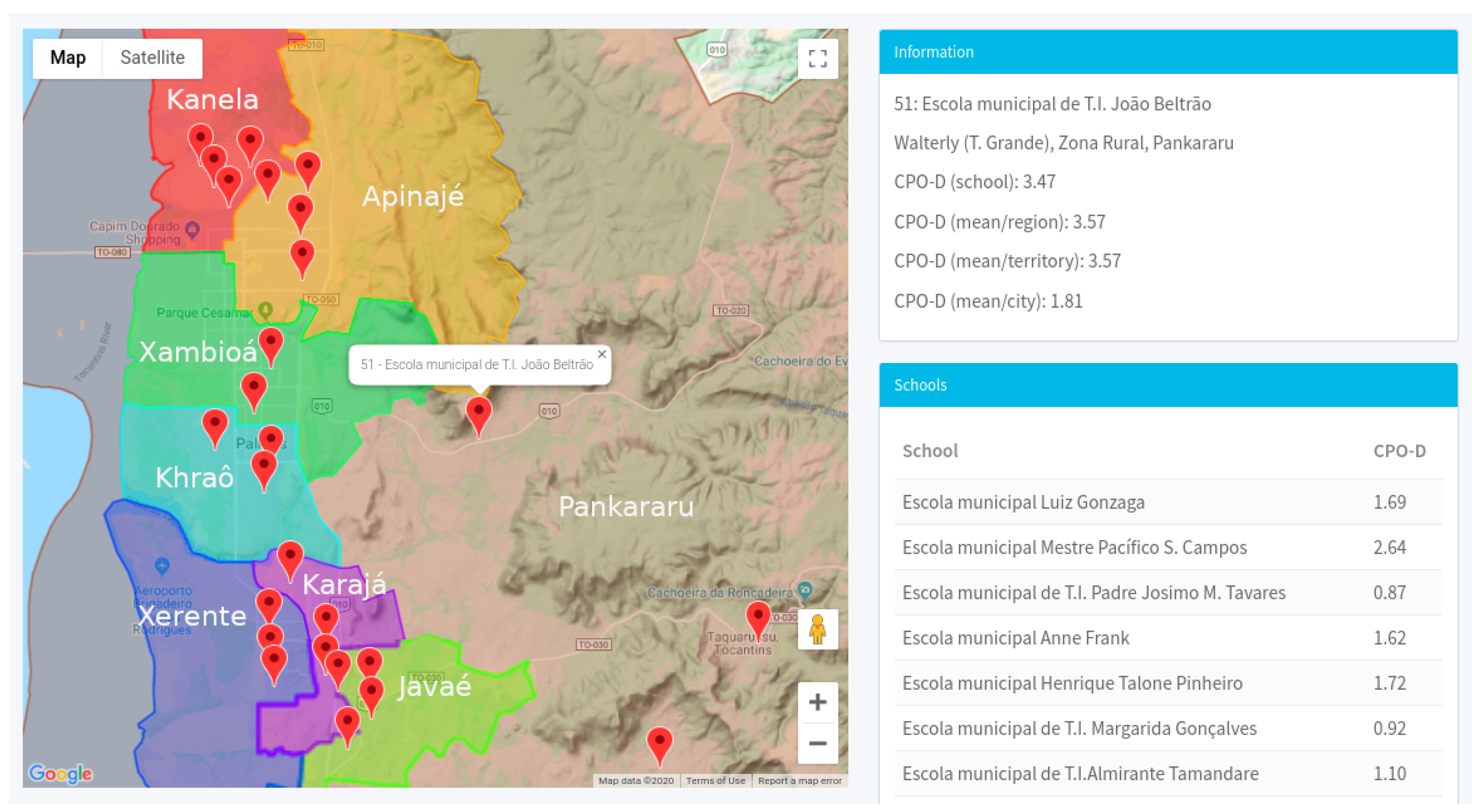
| RF0014: Manage Geographic Information: Function related to the management of information about geolocation of school units, campaigns and actions. It treats information under location parameters to assist visualization of statistical data on the spatial data layers relating health and education information. This module enhances the visualization of analyzes under a geographic component allowing to evaluate the data under the region in which the actions were performed. |
| Deciduous Dentition (Caries) | Permanent Dentition (Caries) | Treatment |
|---|---|---|
| A: Healthy | 0: Healthy | 0: None |
| B: Has Caries | 1: Has Caries | 1: Restoration of 1 surface |
| C: Restored, but with caries | 2: Restored, but with caries | 2: Restoration of 2 or more surfaces |
| D: Restored without caries | 3: Restored without caries | 3: Crown for any reason |
| E: Lost because of caries | 4: Lost because of caries | 4: Aesthetic facet |
| F: Lost for another reason | 5: Lost for another reason | 5: Pulp treatment and restoration |
| G: Has dental sealant | 6: Has dental sealant | 6: Extraction |
| H: Tooth-supported bridge | 7: Tooth-supported bridge | 7: White spot remineralisation |
| K: Unerupted/unexposed root | 8: Unerupted/unexposed root | 8: Sealant |
| T: Trauma (fracture) | T: Trauma (fracture) | 9: No information |
| L: Not considered | 9: Not considered | - |
| Healthy Territory | Schools | Total of Students | Total of Students in 9th Grade |
|---|---|---|---|
| Krahô | Escola Municipal Antonio Carlos Jobim | 599 | 99 |
| Xambioá | Escola Municipal AntonioG. De Carvalho Filho | 618 | 70 |
| Apinajé | Escola Municipal Anne Frank | 838 | 80 |
| Xambioá | Escola Municipal Darcy Ribeiro | 476 | 117 |
| Apinajé | Escola Municipal Henrique Talone Pinheiro | 794 | 80 |
| Xambioá | Escola Municipal de Tempo Integral Vinícius de Moraes | 483 | 81 |
| Kanela | Escola Municipal Beatriz Rodrigues da Silva | 897 | 157 |
| Kanela | Escola Municipal Mestre Pacifico S. Campos | 431 | 74 |
| Kanela | Escola Municipal Luiz Gonzaga | 264 | 65 |
| Kanela | Escola Municipal Tempo Integral Padre Josimo M. Tavares | 1087 | 116 |
| Apinajé | Escola Municipal Tempo Integral Daniel Batista | 386 | 29 |
| Apinajé | Escola Municipal Tempo Integral Monsenhor Pedro P. Piagem | 466 | 35 |
| Javaé | Escola Municipal Jorge Amado | 568 | 159 |
| Javaé | Escola Municipal Maria Rosa De Castro Sales | 703 | 79 |
| Krahô | Escola Municipal Professora Savia F. Jacome | 558 | 71 |
| Javaé | Escola Municipal de Tempo Integral Caroline C. C. Da Silva | 1187 | 72 |
| Karajá | Escola Municipal Aurelio Buarque De Holanda | 776 | 115 |
| Xerente | Escola Municipal Maria Julia Amorim Rodrigues | 694 | 176 |
| Karajá | Escola Municipal Thiago Barbosa | 896 | 104 |
| Xerente | Escola Municipal de Tempo Integral Euridice F. De Mello | 1088 | 68 |
| Xerente | Escola Municipal de Tempo Integral Margarida Gonçalves | 1028 | 62 |
| Pankararu | Escola Municipal Crispim Pereira Alencar | 565 | 33 |
| Apinajé | Escola Municipal de Tempo Integral Aprigio T. De Matos | 235 | 15 |
| Pankararu | Escola Municipal de Tempo Integral Joao Beltrao | 217 | 21 |
| Pankararu | Escola Municipal de Tempo Integral Luiz Nunes De Oliveira | 249 | 22 |
| Pankararu | Escola Municipal de Tempo Integral Sueli Pereira A. Reche | 218 | 14 |
| 16.321 | 2.014 |
| Class | Question Description | Questions |
|---|---|---|
| Personal characteristics | General information about academics (preserving anonymity) | 1–18 |
| Nutritional data | Information on student behavior, frequency and eating habits. | 19–62 |
| Physical activities | Information about the physical activities performed, characteristics and frequency. | 63–72 |
| Smoking | Information on smoking by the student or a close person | 73–81 |
| Alcohol consumption | Information Alcohol consumption by the student or or a close person | 82–89 |
| Drug use | Information about illicit drug use by the student or close people | 90–95 |
| Personal relationships | Information on relationship with parents or guardians and with schoolmates. | 96–107 |
| Hygiene and oral health | Information on personal hygiene and oral health. | 108–113 |
| Security | Information on security that impedes attendance in the school unit and diverse assaults | 114–130 |
| Access to health services | Information on access, frequency, care, quality of use and health services. | 131–138 |
| Body image | Information about body image, overweight, medication or dietary supplements. | 139–145 |
| Your opinion | Students are asked to express their opinion by evaluating the questionnaire. | 146 |
| Group | Instrument | Objective | Author |
|---|---|---|---|
| Oral exam | CPO-D index | To evaluate the prevalence of dental caries in permanent dentition. | Klein and Palmer (1937) |
| ceo-d index | To evaluate the prevalence of dental caries in primary dentition. | Gruebbel (1944) | |
| Socioeconomic and Behavioral Characteristics of Students | Questionnaire of the Students | Describe the socioeconomic and behavioral characteristics of the students. | Adapted from IBGE (2016) |
| Structural and Demographic Characteristics Of Schools | Questionnaire of the school Principal | Describe the structural and sociodemographic characteristics of the schools surveyed. | Adapted from IBGE (2016) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cavalcante, N.V.; Oliveira, A.H.; Sá, B.V.C.d.; Botelho, G.; Moreira, T.R.; Costa, G.D.d.; Cotta, R.M.M. Computing and Oral Health: Mobile Solution for Collecting, Data Analysis, Managing and Reproducing Epidemiological Research in Population Groups. Int. J. Environ. Res. Public Health 2020, 17, 1076. https://doi.org/10.3390/ijerph17031076
Cavalcante NV, Oliveira AH, Sá BVCd, Botelho G, Moreira TR, Costa GDd, Cotta RMM. Computing and Oral Health: Mobile Solution for Collecting, Data Analysis, Managing and Reproducing Epidemiological Research in Population Groups. International Journal of Environmental Research and Public Health. 2020; 17(3):1076. https://doi.org/10.3390/ijerph17031076
Chicago/Turabian StyleCavalcante, Nilton Vale, Ary Henrique Oliveira, Bruno Vinícios Cunha de Sá, Glenda Botelho, Tiago Ricardo Moreira, Glauce Dias da Costa, and Rosangela Minardi Mitre Cotta. 2020. "Computing and Oral Health: Mobile Solution for Collecting, Data Analysis, Managing and Reproducing Epidemiological Research in Population Groups" International Journal of Environmental Research and Public Health 17, no. 3: 1076. https://doi.org/10.3390/ijerph17031076
APA StyleCavalcante, N. V., Oliveira, A. H., Sá, B. V. C. d., Botelho, G., Moreira, T. R., Costa, G. D. d., & Cotta, R. M. M. (2020). Computing and Oral Health: Mobile Solution for Collecting, Data Analysis, Managing and Reproducing Epidemiological Research in Population Groups. International Journal of Environmental Research and Public Health, 17(3), 1076. https://doi.org/10.3390/ijerph17031076