Temperature Distribution of Selected Body Surfaces in Scoliosis Based on Static Infrared Thermography



Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
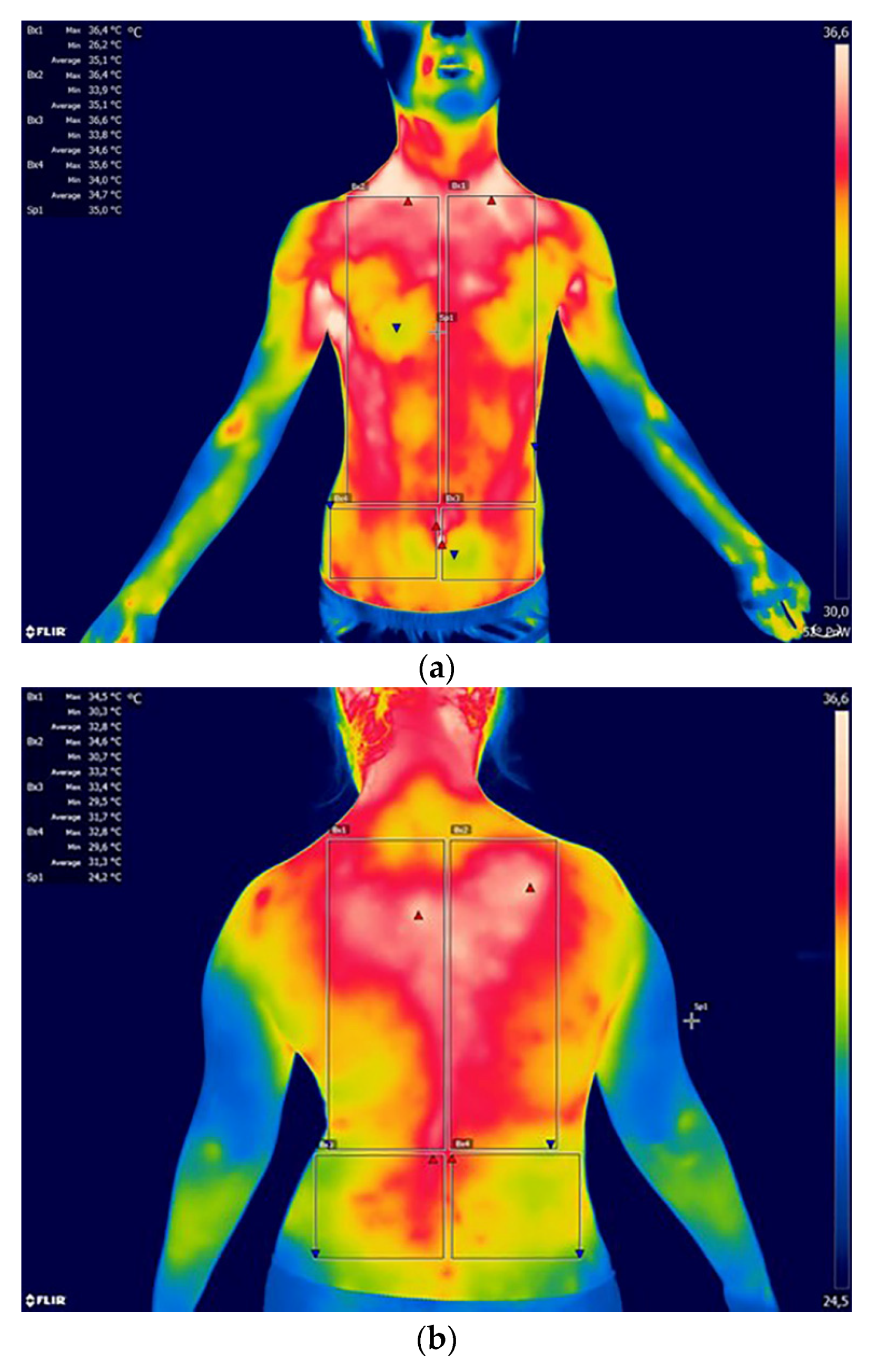
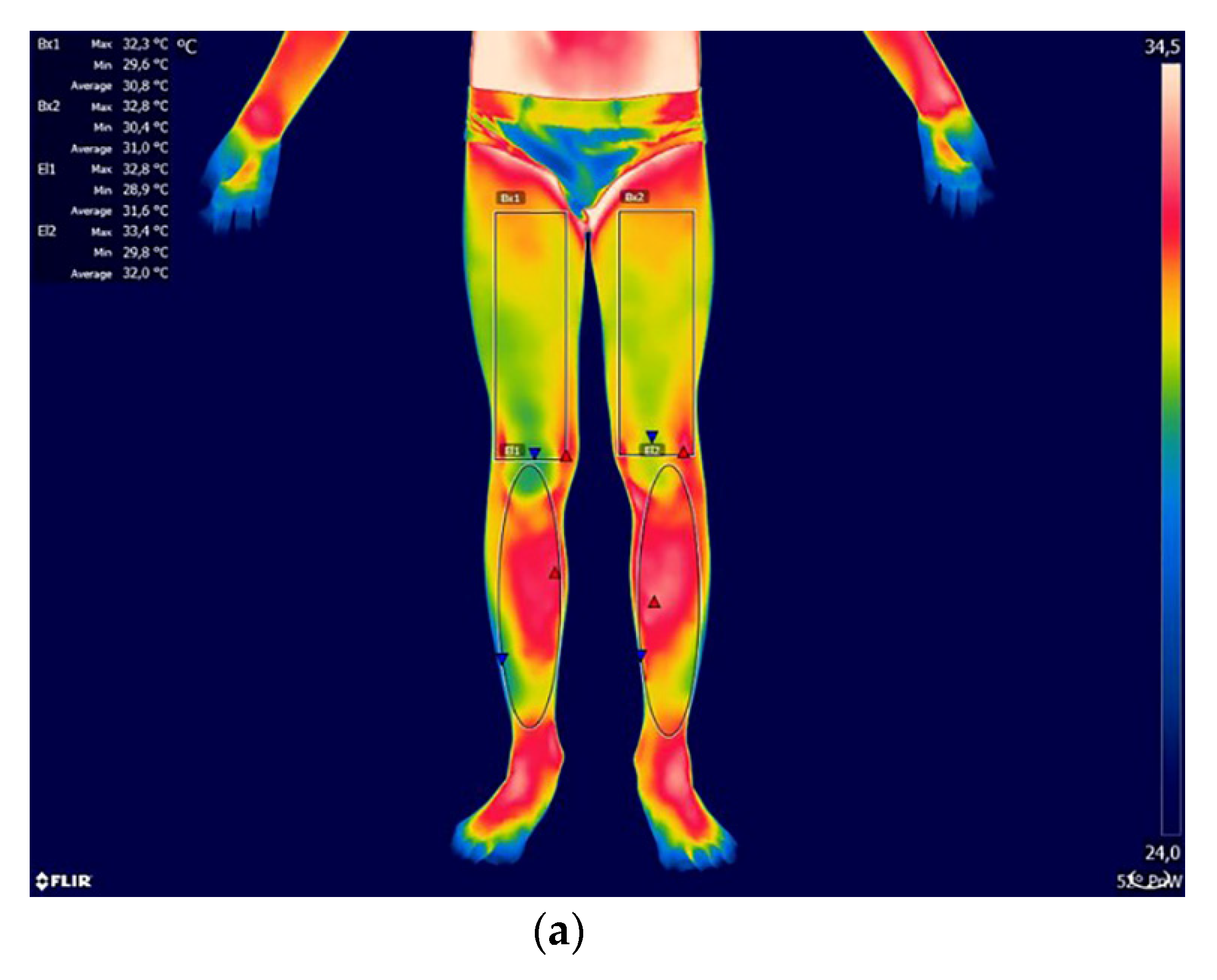
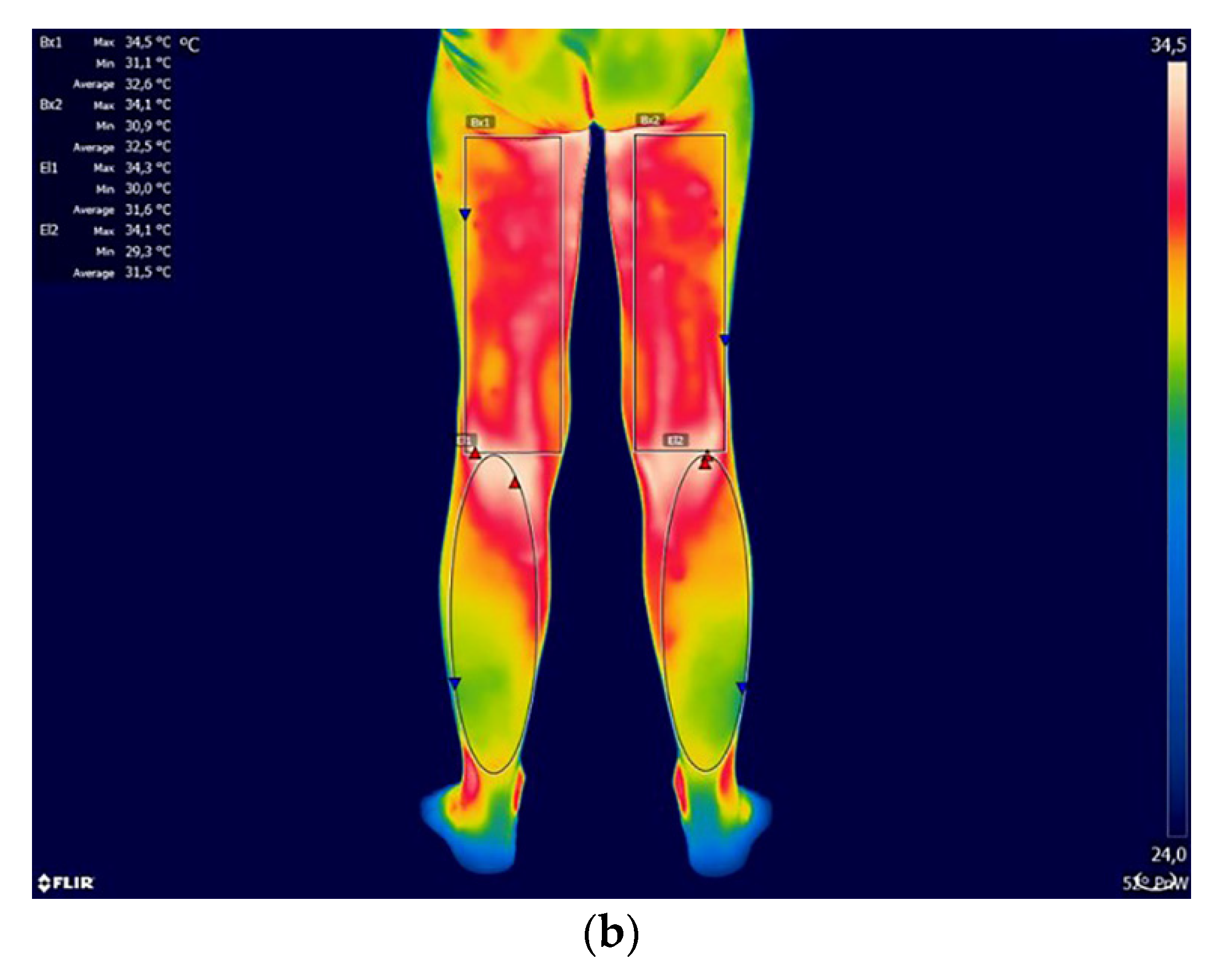
2.2. Thermographic Measurements
2.3. Statistical Analysis
3. Results
- UB—upper back; Ch—chest; Ab—abdominal; LB—lower back; TF—thigh front; TB—thigh back;
- SF—shank front; SB—shank back
- = no significant difference between areas
- → significant difference between the areas at p < 0.05
- →→ significant difference between the areas at p < 0.01
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bauer, J.; Dereń, E. Standardization of infrared thermal imaging in medicine and physiotherapy. Act. Bio-Opt. Inf. Med. 2014, 20, 11–20. [Google Scholar]
- Bogdan, A. Using Thermography for Assessment of Average Human Skin Temperature. Ciep. Og. Wen. 2011, 42, 481–483. [Google Scholar]
- Dębiec-Bąk, A.; Skrzek, A. The comparison of surface body temperature distribution between men and women by means of thermovision. Act. Bio-Opt. Inf. Med. 2012, 18, 25–30. [Google Scholar]
- Uematsu, S.; Jankel, W.; Edwin, D.; Kim, W.; Kozikowski, A.; Long, D.M. Quantification of thermal asymmetry. Part 2: Application in low-back pain and sciatica. J. Neursurg. 1988, 69, 556–561. [Google Scholar]
- Veldhuizen, A.G.; Wever, D.J.; Webb, P.J. The aetiology of idiopathic scoliosis: Biomechanical and neuromuscular factors. Eur. Spine J. 2000, 9, 178–184. [Google Scholar]
- Hildebrandt, C.; Raschner, C.; Ammer, K. An overview of Recent Application of Medical Infrared Thermography in Sports Medicine in Austria. Sensors 2010, 10, 4700–4715. [Google Scholar] [PubMed]
- Chudecka, M.; Lubkowska, A. Temperature changes of selected body’s surfaces of handball players in the course of training estimated by thermovision, and the study of the impact of physiological and morphological factors on the skin temperature. J. Therm. Biol. 2010, 35, 379–385. [Google Scholar]
- Chudecka, M.; Lubkowska, A. The use of thermal imaging to evaluate body temperature changes of athletes during training and a study on the impact of physiological and morphological factors on skin temperature. Hum. Mov. 2012, 13, 33–39. [Google Scholar]
- Escamilla-Galindo, V.L.; Estal-Martínez, A.; Adamczyk, A.G.; Brito, C.J.; Arnaiz-Lastras, J.; Sillero-Quintana, M. Skin temperature response to unilateral training measured with infrared thermography. J. Exerc. Rehabil. 2017, 13, 526–534. [Google Scholar]
- Chudecka, M.; Lubkowska, A.; Leźnicka, K.; Krupecki, K. The use of thermal imaging in the evaluation of the symmetry of muscle activity in various types of training (symmetrical and asymmetrical). J. Hum. Kinet. 2015, 49, 141–147. [Google Scholar]
- Rodríguez-Sanz, D.; Losa-Iglesias, M.E.; López-López, D.; Calvo-Lobo, C.; Palomo-López, P.; Becerro-de-Bengoa-Vallejo, R. Infrared thermography applied to lower limb muscles in elite soccer players with functional ankle equinus and non-equinus condition. PeerJ 2017, 5, e3388. [Google Scholar] [PubMed]
- Rodriguez-Sanz, D.; Losa-Iglesias, M.E.; Becerro de Bengoa-Vallejo, R.; Palomo-Lopez, P.; Beltran-Alacreu, H.; Calvo-Lobo, C.; Navarro-Flores, E.; Lopez-Lopez, D. Skin temperature in youth soccer players with functional equinus and non-equinus condition after running. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 2020–2024. [Google Scholar] [PubMed]
- Benito-de-Pedro, M.; Becerro-de-Bengoa-Vallejo, R.; Losa-Iglesias, M.E.; Rodríguez-Sanz, D.; López-López, D.; Cosín-Matamoros, J.; Martínez-Jiménez, E.M.; Calvo-Lobo, C. Effectiveness between Dry Needling and Ischemic Compression in the Triceps Surae Latent Myofascial Trigger Points of Triathletes on Pressure Pain Threshold and Thermography: A Single Blinded Randomized Clinical Trial. J. Clin. Med. 2019, 8, 1632. [Google Scholar]
- Tkacova, M.; Hudak, R.; Foffova, P.; Zicak, J. An importantance of camera—subject distance and angle in musculoskeletal applications of medical thermography. Act. Electrotech. Inform. 2010, 10, 57–60. [Google Scholar]
- Cibulka, M.C.; Strube, M.J.; Meier, D.; Selsor, M.; Wheatley, C.; Wilson, N.G.; Irrgang, J.J. Symmetrical and asymmetrical hip rotation and its relationship to hip rotator muscle strength. Clin. Biomech. 2010, 25, 56–62. [Google Scholar]
- Ulrike, H.; Mitchell, U.H.; Johnson, A.W.; Adamson, A.B. Relationship between functional movementScreen scores, core strength, posture, and Body Mass Index in school children in Moldova. J. Strength Cond. Res. 2015, 29, 1172–1179. [Google Scholar]
- Horn, P. Scoliosis Early Identification of Affected Patients. Clin. Rev. 2012, 22, 16–22. [Google Scholar]
- Fernandez, S. A Method of Treating Scoliosis, Kyphosis and Lordosis, 1st ed.; Markmed Rehabilitacja S.C.: Ostrowiec Świętokrzyski, Poland, 2009. [Google Scholar]
- Gaudreault, N.; Arsenault, A.B.; Larivière, C.; DeSerres, S.J.; Rivard, C.H. Assessment of the paraspinal muscles of subjects presenting an idiopathic scoliosis: An EMG pilot study. BMC Musculoskelet Disord. 2005, 6, 14. [Google Scholar]
- Karski, T. Etiology of the so-called “idiopathic scoliosis”. Biomechanical explanation of spine deformity. Two groups of development of scoliosis. New rehabilitation treatment; possibility of prophylactics. Stud. Health Technol. Inf. 2002, 91, 37–46. [Google Scholar]
- Horne, J.P.; Flannery, R.; Usman, S. Adolescent Idiopathic Scoliosis: Diagnosis and Management. Am. Fam. Physician. 2014, 89, 193–198. [Google Scholar]
- Vutan, A.M.; Lovasz, E.C.; Amarandei, M.; Ciupe, V. The methods used for the diagnosis and evaluation of scoliosis. Timis. Phys. Educ. Rehabil. J. 2016, 9, 36–41. [Google Scholar] [CrossRef][Green Version]
- Kwok, G.; Yip, J.; Yick, K.L.; Cheung, M.C.; Tse, C.Y.; Ng, S.P.; Luximon, A. Postural Screening for Adolescent Idiopathic Scoliosis with Infrared Thermography. Sci. Rep. 2017, 7, 14431. [Google Scholar] [CrossRef] [PubMed]
- Adams, W. Lectures on the Pathology and Treatment of Lateral and Other Forms of Curvature of the Spine; Churchill: London, UK, 1865. [Google Scholar]
- Coelho, D.M.; Bonagamba, G.H.; Oliveira, A.S. Scoliometer measurements of patients with idiopathic scoliosis. Braz. J. Phys. Ther. 2013, 17, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Uematsu, S. Thermographic imaging of cutaneous sensory segment in patients with peripheral nerve injury skin-temperature stability between sides of the body. J. Neurosurg. 1985, 62, 716–720. [Google Scholar] [CrossRef] [PubMed]
- Żyłka, W.; Gala-Błądzińska, A. The role of thermovision in the diagnostics of vascular diseases in hemodialysis patients. Act. Bio-Opt. Inf. Med. 2016, 22, 121–129. [Google Scholar]
- Awrejcewicz, J.; Byczek, S.; Zagrodny, B. Influence of the asymmetric loading of the body during the walk on the temperature distribution. Act. Bio-Opt. Inf. Med. 2012, 2, 74–79. [Google Scholar]
- Dębiec-Bąk, A.; Kuligowski, T.; Skrzek, A. Analyzing thermoregulation processes in early school-age girls and boys through thermography. J. Anal. Calorim. 2020, 140, 243–251. [Google Scholar] [CrossRef]
- Dyszkiewicz, J.; Kuna, J. Simplified analisi of spine thermovision picture in diagnosticsa of scolioses. Acta Bioeng. Biomech. 2001, 3, 93–99. [Google Scholar]
- Dyszkiewicz, J.; Kuna, J. Application of thermography in diagnostics and prognostication of scoliosis treatment. Acta Bioeng. Biomech. 2002, 4, 63–70. [Google Scholar]
- Weinstein, S.L.; Dolan, L.A.; Wright, J.G.; Dobbs, M.B. Efects of bracing in adolescents with idiopathic scoliosis. N. Engl. J. Med. 2013, 369, 1512–1521. [Google Scholar] [CrossRef]
- Negrini, S.; Donzelli, S.; Aulisa, A.G.; Czaprowski, D.; Schreiber, S.; de Mauroy, J.C.; Diers, H.; Grivas, T.B.; Knott, P.; Kotwicki, T.; et al. 2016 SOSORT guidelines: Orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis Spinal Disord. 2018, 13, 1–48. [Google Scholar] [CrossRef] [PubMed]
- Fong, D.Y.; Lee, C.F.; Cheung, K.M.; Cheng, J.C.; Ng, B.K.; Lam, T.P.; Mak, K.H.; Yip, P.S.; Luk, K.D. A meta-analysis of the clinical effectiveness of school scoliosis screening. Spine 2010, 35, 1061–1071. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Study Group | Control Group | |||||||
|---|---|---|---|---|---|---|---|---|
| ♀ | ♂ | ♀ | ♂ | |||||
| X | Min | X | Min | X | Min | X | Min | |
| ±SD | Max | ±SD | Max | ±SD | Max | ±SD | Max | |
| Age | 12 | 7 | 9.7 | 7 | 11.3 | 7 | 10.9 | 6 |
| [years] | ± 2.5 | 16 | ± 3.3 | 15 | ± 2.9 | 15 | ± 2.8 | 15 |
| Body mass [kg] | 42.2 | 20 | 33 | 24 | 46 | 38 | 43.3 | 22 |
| ± 11.6 | 63 | ±9.9 | 48 | ± 12.5 | 68 | ± 19.9 | 73 | |
| Body height [m] | 1.5 | 1.3 | 1.4 | 1.3 | 1.5 | 1.4 | 1.6 | 1.4 |
| ± 0.1 | 1.7 | ±0.1 | 1.7 | ± 0.1 | 1.6 | ±0.2 | 1.8 | |
| BMI [kg/m2] | 18.2 | 12.2 | 15.7 | 13.5 | 20 | 13.6 | 16.9 | 11.6 |
| ± 3.7 | 23.6 | ± 1.8 | 18.9 | ± 3.3 | 24.9 | ± 3.4 | 21.4 | |
| ♀ Study Group | ♀ Control Group | ♂ Study Group | ♂ Control Group | |||||
|---|---|---|---|---|---|---|---|---|
| X | Min | X | Min | X | Min | X | Min | |
| ± SD | Max | ± SD | Max | ±SD | Max | ± SD | Max | |
| [°C] | [°C] | [°C] | [°C] | [°C] | [°C] | [°C] | [°C] | |
| UBR | 34.6 | 32.9 | 34.3 | 33.9 | 35.1 | 34.8 | 34.6 | 33.5 |
| ±1.0 | 36.1 | ±0.4 | 35.5 | ±0.3 | 35.7 | ±0.9 | 36.2 | |
| UBL | 34.2 | 32.6 | 34.2 | 33.8 | 34.8 | 34.3 | 34.7 | 33.5 |
| ±1.0 | 35.8 | ±0.5 | 35.5 | ±0.4 | 35.6 | ±0.8 | 36 | |
| LBR | 33.4 | 31.7 | 32.9 | 32.2 | 34 | 33 | 35.8 | 32 |
| ±1.2 | 35 | ±0.8 | 34.8 | ±0.6 | 34.8 | ±1.2 | 35.7 | |
| LBL | 33.4 | 31.5 | 32.8 | 32.1 | 33.7 | 32.8 | 33.5 | 31.8 |
| ±1.3 | 35.9 | ±0.8 | 34.7 | ±0.6 | 34.5 | ±1.2 | 35.6 | |
| ChR | 34.6 | 32.9 | 33.6 | 32.9 | 34.6 | 34.4 | 34.2 | 33 |
| ±0.9 | 35.7 | ±0.7 | 35.5 | ±0.2 | 35 | ±0.9 | 35.5 | |
| ChL | 34.6 | 32.9 | 33.7 | 32.9 | 34.7 | 34.5 | 34.2 | 33 |
| ±1.0 | 35.7 | ±0.7 | 35.5 | ±0.2 | 35.1 | ±0.9 | 35.5 | |
| AbR | 34 | 31.7 | 32.7 | 31.5 | 34.1 | 33.6 | 33.7 | 32.2 |
| ±1.2 | 35.4 | ±1.2 | 35.7 | ±0.5 | 34.6 | ±1.3 | 35.7 | |
| AbL | 34 | 31.9 | 32.6 | 31.4 | 34.1 | 33.6 | 33.7 | 32.3 |
| ±1.1 | 35.5 | ±1.3 | 35.7 | ±0.5 | 34.6 | ±1.3 | 35.7 | |
| TFR | 30.6 | 28.4 | 29.9 | 27.6 | 30.7 | 30.1 | 30.2 | 28.3 |
| ±1.3 | 33.4 | ±1.6 | 32.3 | ±0.4 | 31.2 | ±1.6 | 32.3 | |
| TFL | 30.4 | 28.1 | 29.9 | 27.7 | 31.2 | 30.8 | 30.1 | 27.7 |
| ±1.5 | 33 | ±1.6 | 32.5 | ±0.3 | 31.5 | ±1.9 | 32.5 | |
| TBR | 30.9 | 29.1 | 30.2 | 28 | 31.6 | 31.1 | 30.8 | 28.5 |
| ±1.3 | 32.9 | ±1.7 | 33.5 | ±0.3 | 32 | ±2.1 | 33.5 | |
| TBL | 30.9 | 29.4 | 30.3 | 27.9 | 31.7 | 31.7 | 30.8 | 28.6 |
| ±1.3 | 33.4 | ±1.7 | 33.3 | ±0.1 | 31.8 | ±2.0 | 33.3 | |
| SFR | 30.9 | 29.4 | 30.9 | 28.6 | 31.6 | 31.4 | 31.1 | 29.8 |
| ±1 | 32.4 | ±1.4 | 32.8 | ±0.2 | 31.9 | ±1.3 | 32.8 | |
| SFL | 30.9 | 29.3 | 30.6 | 28.5 | 31.5 | 30.9 | 31.1 | 29.6 |
| ±1.1 | 32.4 | ±1.4 | 33.1 | ±0.4 | 32 | ±1.4 | 33.1 | |
| SBR | 30.3 | 28.6 | 30.1 | 27.7 | 31.5 | 30.9 | 30.3 | 28.3 |
| ±0.9 * | 31.6 | ±1.6 | 32.4 | ±0.6 | 32.5 | ±1,7 | 32.4 | |
| SBL | 30.6 | 29 | 30 | 27.9 | 31.5 | 30.4 | 30.3 | 28.2 |
| ±0.9 * | 31.9 | ±1.5 | 32.4 | ±0.5 | 31.9 | ±1.7 | 32.4 | |
| UBL | UBR | LBR | LBL | ChR | ChL | AbR | AbL | TFR | TFL | TBR | TBL | SFR | SFL | SBR | SBL | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| UBL | - | 0.97 | 0.82 | 0.76 | 0.72 | 0.76 | 0.65 | 0.62 | 0.16 | 0.3 | 0.27 | 0.34 | 0.45 | 0.39 | 0.35 | 0.45 |
| UBR | 0.97 | - | 0.82 | 0.77 | 0.75 | 0.79 | 0.7 | 0.67 | 0.2 | 0.33 | 0.26 | 0.37 | 0.47 | 0.42 | 0.33 | 0.45 |
| LBR | 0.82 | 0.82 | - | 0.96 | 0.76 | 0.78 | 0.67 | 0.65 | 0.44 | 0.54 | 0.55 | 0.64 | 0.49 | 0.48 | 0.57 | 0.74 |
| LBL | 0.76 | 0.77 | 0.96 | - | 0.77 | 0.76 | 0.67 | 0.66 | 0.5 | 0.54 | 0.53 | 0.64 | 0.47 | 0.45 | 0.49 | 0.67 |
| ChR | 0.72 | 0.75 | 0.76 | 0.77 | - | 0.98 | 0.92 | 0.87 | 0.47 | 0.46 | 0.42 | 0.49 | 0.44 | 0.38 | 0.24 | 0.47 |
| ChL | 0.76 | 0.79 | 0.78 | 0.76 | 0.98 | - | 0.91 | 0.86 | 0.48 | 0.49 | 0.43 | 0.5 | 0.53 | 0.46 | 0.28 | 0.5 |
| AbR | 0.65 | 0.7 | 0.67 | 0.67 | 0.92 | 0.91 | - | 0.97 | 0.54 | 0.5 | 0.37 | 0.51 | 0.52 | 0.45 | 0.38 | 0.5 |
| AbL | 0.62 | 0.67 | 0.65 | 0.66 | 0.87 | 0.86 | 0.97 | - | 0.57 | 0.55 | 0.41 | 0.54 | 0.57 | 0.51 | 0.42 | 0.51 |
| TFR | 0.16 | 0.2 | 0.44 | 0.5 | 0.47 | 0.48 | 0.54 | 0.57 | - | 0.93 | 0.78 | 0.84 | 0.81 | 0.79 | 0.63 | 0.61 |
| TFL | 0.3 | 0.33 | 0.54 | 0.54 | 0.46 | 0.49 | 0.5 | 0.55 | 0.93 | - | 0.89 | 0.89 | 0.86 | 0.85 | 0.74 | 0.76 |
| TBR | 0.27 | 0.26 | 0.55 | 0.53 | 0.42 | 0.43 | 0.37 | 0.41 | 0.78 | 0.89 | - | 0.92 | 0.68 | 0.67 | 0.7 | 0.756 |
| TBL | 0.34 | 0.37 | 0.64 | 0.64 | 0.49 | 0.5 | 0.51 | 0.54 | 0.84 | 0.89 | 0.92 | - | 0.76 | 0.76 | 0.78 | 0.77 |
| SFR | 0.45 | 0.47 | 0.49 | 0.47 | 0.44 | 0.53 | 0.52 | 0.57 | 0.81 | 0.86 | 0.68 | 0.76 | - | 0.97 | 0.68 | 0.59 |
| SFL | 0.39 | 0.42 | 0.48 | 0.45 | 0.38 | 0.46 | 0.45 | 0.51 | 0.79 | 0.85 | 0.67 | 0.76 | 0.97 | - | 0.63 | 0.57 |
| SBR | 0.35 | 0.33 | 0.57 | 0.49 | 0.24 | 0.28 | 0.38 | 0.42 | 0.63 | 0.74 | 0.7 | 0.78 | 0.68 | 0.63 | - | 0.86 |
| SBL | 0.45 | 0.45 | 0.74 | 0.67 | 0.47 | 0.5 | 0.5 | 0.51 | 0.61 | 0.76 | 0.75 | 0.77 | 0.59 | 0.57 | 0.86 | - |
| UBL | UBR | LBR | LBL | ChR | ChL | AbR | AbL | TFR | TFL | TBR | TBL | SFR | SFL | SBR | SBL | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| UBL | - | 0.97 | 0.92 | 0.96 | 0.9 | 0.89 | 0.83 | 0.83 | 0.3 | 0.25 | 0.43 | 0.41 | 0.4 | 0.39 | 0.28 | 0.25 |
| UBR | 0.97 | - | 0.94 | 0.96 | 0.91 | 0.91 | 0.85 | 0.85 | 0.38 | 0.36 | 0.521 | 0.5 | 0.46 | 0.46 | 0.37 | 0.34 |
| LBR | 0.92 | 0.94 | - | 0.98 | 0.96 | 0.95 | 0.94 | 0.93 | 0.53 | 0.48 | 0.64 | 0.63 | 0.58 | 0.57 | 0.5 | 0.46 |
| LBL | 0.96 | 0.96 | 0.98 | - | 0.94 | 0.93 | 0.9 | 0.89 | 0.44 | 0.39 | 0.57 | 0.55 | 0.51 | 0.5 | 0.41 | 0.38 |
| ChR | 0.9 | 0.91 | 0.96 | 0.94 | - | 0.99 | 0.98 | 0.98 | 0.6 | 0.56 | 0.7 | 0.69 | 0.64 | 0.65 | 0.57 | 0.56 |
| ChL | 0.89 | 0.91 | 0.95 | 0.93 | 0.99 | - | 0.97 | 0.96 | 0.65 | 0.61 | 0.74 | 0.73 | 0.69 | 0.69 | 0.62 | 0.6 |
| AbR | 0.83 | 0.85 | 0.94 | 0.9 | 0.98 | 0.97 | - | 0.99 | 0.68 | 0.65 | 0.7 | 0.76 | 0.69 | 0.71 | 0.65 | 0.64 |
| AbL | 0.83 | 0.85 | 0.93 | 0.899 | 0.98 | 0.96 | 0.99 | - | 0.64 | 0.6 | 0.74 | 0.71 | 0.65 | 0.67 | 0.6 | 0.59 |
| TFR | 0.3 | 0.38 | 0.53 | 0.443 | 0.6 | 0.65 | 0.68 | 0.64 | - | 0.98 | 0.97 | 0.97 | 0.95 | 0.96 | 0.99 | 0.98 |
| TFL | 0.25 | 0.36 | 0.48 | 0.39 | 0.56 | 0.61 | 0.65 | 0.6 | 0.98 | - | 0.96 | 0.96 | 0.92 | 0.93 | 0.98 | 0.99 |
| TBR | 0.43 | 0.52 | 0.64 | 0.57 | 0.7 | 0.74 | 0.79 | 0.74 | 0.97 | 0.96 | - | 0.99 | 0.94 | 0.96 | 0.97 | 0.96 |
| TBL | 0.41 | 0.5 | 0.63 | 0.55 | 0.69 | 0.73 | 0.76 | 0.71 | 0.97 | 0.96 | 0.99 | - | 0.95 | 0.96 | 0.97 | 0.97 |
| SFR | 0.4 | 0.46 | 0.58 | 0.51 | 0.64 | 0.69 | 0.69 | 0.65 | 0.95 | 0.92 | 0.94 | 0.95 | - | 0.99 | 0.96 | 0.94 |
| SFL | 0.39 | 0.46 | 0.57 | 0.5 | 0.65 | 0.69 | 0.71 | 0.67 | 0.96 | 0.93 | 0.96 | 0.96 | 0.99 | - | 0.96 | 0.95 |
| SBR | 0.28 | 0.37 | 0.5 | 0.41 | 0.57 | 0.62 | 0.65 | 0.6 | 0.99 | 0.98 | 0.97 | 0.97 | 0.96 | 0.96 | - | 0.99 |
| SBL | 0.25 | 0.34 | 0.46 | 0.38 | 0.56 | 0.6 | 0.64 | 0.59 | 0.98 | 0.99 | 0.96 | 0.97 | 0.94 | 0.95 | 0.99 | - |
| ∆TR/L | ||||
|---|---|---|---|---|
| ♀ Study Group | ♀ Control Group | ♂ Study Group | ♂ Control Group | |
| X± SD [°C] | X ± SD [°C] | |||
| UBR | 0.4 ± 0.1 | 0.0 ± 0.1 *** | 0.4 ± 0.1 | 0.1 ± 0.1 *** |
| UBL | ||||
| LBR | 0.2 ± 0.2 | 0.1 ± 0.1 | 0.2 ± 0.1 | 0.1 ± 0.1 * |
| LBL | ||||
| ChR | 0.1 ± 0.14 | 0.1 ± 0.11 | 0.1 ± 0.1 | 0.02 ± 0.0 ** |
| ChL | ||||
| AbR | 0.2 ± 0.1 | 0.1 ± 0.1 | 0.025 ± 0.0 | 0.1 ± 0.1 ** |
| AbL | ||||
| TFR | 0.4 ± 0.1 | 0.19 ± 0.1 ** | 0.5 ± 0.1 | 0.3 ± 0.2 |
| TFL | ||||
| TBR | 0.3 ± 0.1 | 0.15 ± 0.1 *** | 0.4 ± 0.1 | 0.1 ± 0.1 *** |
| TBL | ||||
| SFR | 0.2 ± 0.1 | 0.16 ± 0.1 | 0.22 ± 0.1 | 0.2 ± 0.1 |
| SFL | ||||
| SBR | 0.5 ± 0.2 | 0.22 ± 0.1 ** | 0.5 ± 0.1 | 0.1 ± 0.1 *** |
| SBL | ||||
| ∆TR/L | ||
|---|---|---|
| ♀ + ♂ Study Group | ♀ + ♂ Control Group | |
| N = 20 | N = 20 | |
| X ± SD [°C] | X ± SD [°C] | |
| UBR | 0.4 ± 0.1 *** | 0.1 ± 0.1 |
| UBL | ||
| LBR | 0.2 ± 0.2 | 0.1 ± 0.1 |
| LBL | ||
| ChR | 0.1 ± 0.1 | 0.0 ± 0.1 |
| ChL | ||
| AbR | 0.1 ± 0.1 | 0.1 ± 0.1 |
| AbL | ||
| TFR | 0.4 ± 0.1 ** | 0.2 ± 0.1 |
| TFL | ||
| TBR | 0.3 ± 0.1 ** | 0.1 ± 0.1 |
| TBL | ||
| SFR | 0.2 ± 0.1 | 0.2 ± 0.1 |
| SFL | ||
| SBR | 0.5 ± 0.2 *** | 0.2 ± 0.1 |
| SBL | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lubkowska, A.; Gajewska, E. Temperature Distribution of Selected Body Surfaces in Scoliosis Based on Static Infrared Thermography. Int. J. Environ. Res. Public Health 2020, 17, 8913. https://doi.org/10.3390/ijerph17238913
Lubkowska A, Gajewska E. Temperature Distribution of Selected Body Surfaces in Scoliosis Based on Static Infrared Thermography. International Journal of Environmental Research and Public Health. 2020; 17(23):8913. https://doi.org/10.3390/ijerph17238913
Chicago/Turabian StyleLubkowska, Anna, and Ewa Gajewska. 2020. "Temperature Distribution of Selected Body Surfaces in Scoliosis Based on Static Infrared Thermography" International Journal of Environmental Research and Public Health 17, no. 23: 8913. https://doi.org/10.3390/ijerph17238913
APA StyleLubkowska, A., & Gajewska, E. (2020). Temperature Distribution of Selected Body Surfaces in Scoliosis Based on Static Infrared Thermography. International Journal of Environmental Research and Public Health, 17(23), 8913. https://doi.org/10.3390/ijerph17238913