No Difference in Weight Loss, Glucose, Lipids and Vitamin D of Eggs for Breakfast Compared with Cereal for Breakfast during Energy Restriction



Abstract
1. Introduction
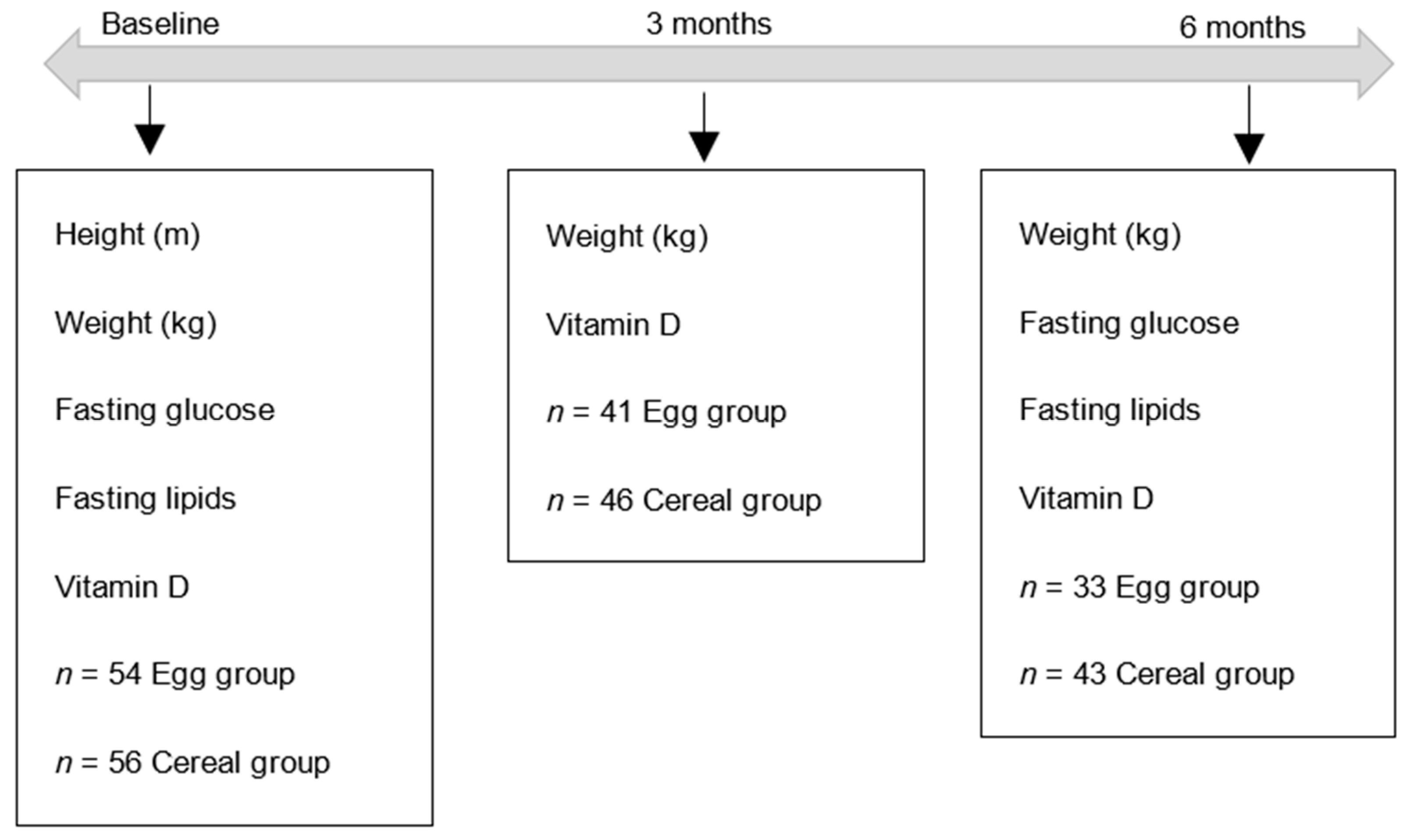
2. Materials and Methods
3. Results
3.1. Weight and Vitamin D at 3 Months
3.2. Outcomes at 6 Months
3.3. Fasting Glucose and Lipids
3.4. Vitamin D
3.5. Compliance
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- AIHW. Overweight and Obesity: An Interactive Insight; Australian Institute of Health and Welfare: Bruce, Australia, 2019. [Google Scholar]
- Santos, I.; Sniehotta, F.F.; Marques, M.M.; Carraca, E.V.; Teixeira, P.J. Prevalence of personal weight control attempts in adults: A systematic review and meta-analysis. Obes. Rev. 2017, 18, 32–50. [Google Scholar] [CrossRef] [PubMed]
- Megson, M.; Wing, R.; Leahey, T.M. Effects of breakfast eating and eating frequency on body mass index and weight loss outcomes in adults enrolled in an obesity treatment program. J. Behav. Med. 2017, 40, 595–601. [Google Scholar] [CrossRef] [PubMed]
- Paixao, C.; Dias, C.M.; Jorge, R.; Carraca, E.V.; Yannakoulia, M.; de Zwaan, M.; Soini, S.; Hill, J.O.; Teixeira, P.J.; Santos, I. Successful weight loss maintenance: A systematic review of weight control registries. Obes. Rev. 2020, 21, e13003. [Google Scholar] [CrossRef] [PubMed]
- AIHW. Australian Health Survey: Nutrition First Results-Foods and Nutrients; Australian Institute of Health and Welfare: Bruce, Australia, 2014. [Google Scholar]
- ABS. National Nutrition Survey: Foods Eaten, Australia, 1995; Australian Bureau of Statistics: Canberra, Australia, 1999. [Google Scholar]
- Vander Wal, J.S.; Gupta, A.; Khosla, P.; Dhurandhar, N.V. Egg breakfast enhances weight loss. Int. J. Obes. 2008, 32, 1545–1551. [Google Scholar]
- Keogh, J.; Clifton, P. Energy intake and satiety responses of eggs for breakfast in overweight and obese adults-a crossover study. Int. J. Environ. Res. Public Health 2020, 17, 5583. [Google Scholar] [CrossRef] [PubMed]
- Vranić, L.; Mikolašević, I.; Milić, S. Vitamin D deficiency: Consequence or cause of obesity? Medicina 2019, 55. [Google Scholar] [CrossRef] [PubMed]
- Malacova, E.; Cheang, P.R.; Dunlop, E.; Sherriff, J.L.; Lucas, R.M.; Daly, R.M.; Nowson, C.A.; Black, L.J. Prevalence and predictors of Vitamin D deficiency in a nationally representative sample of adults participating in the 2011-2013 australian health survey. Br. J. Nutr. 2019, 121, 894–904. [Google Scholar] [CrossRef]
- Council N.H.a.M.R. Vitamin D Nutrient Reference Values for Australia and New Zealand; National Health and Medical Research Council: Canberra, Australia, 2006. [Google Scholar]
- Zhong, V.W. Eggs, dietary cholesterol, and cardiovascular disease: The debate continues. J. Thorac. Dis. 2019, 11, E148–E150. [Google Scholar] [CrossRef]
- Fuller, N.R.; Sainsbury, A.; Caterson, I.D.; Denyer, G.; Fong, M.; Gerofi, J.; Leung, C.; Lau, N.S.; Williams, K.H.; Januszewski, A.S.; et al. Effect of a high-egg diet on cardiometabolic risk factors in people with type 2 diabetes: The diabetes and egg (diabegg) study-randomized weight-loss and follow-up phase. Am. J. Clin. Nutr. 2018, 107, 921–931. [Google Scholar] [CrossRef] [PubMed]
- Noakes, M.; Keogh, J.B.; Foster, P.R.; Clifton, P.M. Effect of an energy-restricted, high-protein, low-fat diet relative to a conventional high-carbohydrate, low-fat diet on weight loss, body composition, nutritional status, and markers of cardiovascular health in obese women. Am. J. Clin. Nutr. 2005, 81, 1298–1306. [Google Scholar] [CrossRef] [PubMed]
- Wycherley, T.P.; Buckley, J.D.; Noakes, M.; Clifton, P.M.; Brinkworth, G.D. Comparison of the effects of weight loss from a high-protein versus standard-protein energy-restricted diet on strength and aerobic capacity in overweight and obese men. Eur. J. Nutr. 2013, 52, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Berger, S.; Raman, G.; Vishwanathan, R.; Jacques, P.F.; Johnson, E.J. Dietary cholesterol and cardiovascular disease: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2015, 102, 276–294. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zhou, C.; Zhou, X.; Li, L. Egg consumption and risk of cardiovascular diseases and diabetes: A meta-analysis. Atherosclerosis 2013, 229, 524–530. [Google Scholar] [CrossRef] [PubMed]
- Zhong, V.W.; Van Horn, L.; Cornelis, M.C.; Wilkins, J.T.; Ning, H.; Carnethon, M.R.; Greenland, P.; Mentz, R.J.; Tucker, K.L.; Zhao, L.; et al. Associations of dietary cholesterol or egg consumption with incident cardiovascular disease and mortality. JAMA 2019, 321, 1081–1095. [Google Scholar] [CrossRef] [PubMed]
- Djousse, L.; Gaziano, J.M. Egg consumption in relation to cardiovascular disease and mortality: The physicians’ health study. Am. J. Clin. Nutr. 2008, 87, 964–969. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.Y.; Xun, P.; Nakamura, Y.; He, K. Egg consumption in relation to risk of cardiovascular disease and diabetes: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2013, 98, 146–159. [Google Scholar] [CrossRef] [PubMed]
- Headland, M.L.; Clifton, P.M.; Keogh, J.B. Effect of intermittent compared to continuous energy restriction on weight loss and weight maintenance after 12 months in healthy overweight or obese adults. Int. J. Obes. 2019, 43, 2028–2036. [Google Scholar] [CrossRef] [PubMed]
- Carter, S.; Clifton, P.M.; Keogh, J.B. The effects of intermittent compared to continuous energy restriction on glycaemic control in type 2 diabetes; a pragmatic pilot trial. Diabetes Res. Clin. Pract. 2016, 122, 106–112. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Commenced | Completed | |||
|---|---|---|---|---|
| Eggs (n = 54) | Cereal (n = 56) | Eggs (n = 33) | Cereal (n = 43) | |
| Age years | 54 ± 15 | 57 ± 15 | 57 ± 15 | 59 ± 15 |
| Weight kg | 94 ± 21 | 93 ± 18 | 90 ± 17 | 95 ± 16 |
| BMI kg/m2 | 34 ± 7 | 34 ± 6 | 32 ± 5 | 34 ± 5 |
| Glucose mmol/L | 5.0 ± 0.7 | 4.9 ± 0.5 | 5.1 ± 0.7 | 5.0 ± 0.5 |
| Total Cholesterol mmol/L | 5.3 ± 0.9 | 5.5 ± 0.9 | 5.4 ± 0.8 | 5.4 ± 0.8 |
| HDL-C mmol/L | 1.5 ± 0.3 | 1.5 ± 0.3 | 1.5 ± 0.3 | 1.5 ± 0.3 |
| LDL-C mmol/L | 3.2 ± 0.8 | 3.5 ± 0.8 | 3.4 ± 0.7 | 3.4 ± 0.8 |
| Triglycerides mmol/L | 1.1 ± 0.4 | 1.3 ± 0.7 | 1.2 ± 0.4 | 1.2 ± 0.5 |
| Vitamin D nmol/L | 54 ± 19 | 56 ± 17 | 53 ± 15 | 57 ± 17 |
| Non-Obese | Obese | |||
|---|---|---|---|---|
| Eggs (n = 9) | Cereal (n = 11) | Eggs (n = 24) | Cereal (n= 32) | |
| Age years | 63 ± 14 | 48.6 ± 21.5 | 54.8 ± 15.4 | 62.2 ± 9.5 1 |
| Weight kg | 75.4 ± 12.3 | 77.6 ± 12.1 | 95.8 ± 15.4 | 101.2 ± 12.9 |
| BMI kg/m2 | 27.6 ± 1.7 | 27.7 ± 1.6 | 34.1 ± 4.3 | 36.0 ± 4.3 |
| Glucose mmol/L | 5.0 ± 0.4 | 4.8 ± 0.4 | 5.1 ± 0.8 | 5.0 ± 0.5 |
| Total Cholesterol mmol/L | 5.7 ± 1.0 | 5.4 ± 1.0 | 5.3 ± 0.7 | 5.4 ± 0.8 |
| HDL-C mmol/L | 1.7 ± 0.2 | 1.5 ± 0.3 | 1.5 ± 0.3 | 1.4 ± 0.3 |
| LDL-C mmol/L | 3.5 ± 0.8 | 3.4 ± 0.9 | 3.3 ± 0.7 | 3.4 ± 0.7 |
| Triglycerides mmol/L | 1.1 ± 0.5 | 1.2 ± 0.5 | 1.2 ± 0.4 | 1.2 ± 0.6 |
| Vitamin D nmol/L | 55.8 ± 13.0 | 57.9 ± 14.0 | 51.3 ± 16.1 | 56.9 ± 18.3 |
| Baseline | 6 Months | |||
|---|---|---|---|---|
| Eggs | Cereal | Eggs | Cereal | |
| Glucose mmol/L | 5.1 ± 0.7 | 5.0 ± 0.8 | 5.1 ± 0.5 | 5.2 ± 0.7 |
| Total Cholesterol mmol/L | 5.4 ± 0.8 | 5.4 ± 0.8 | 5.4 ± 1.0 | 5.3 ± 0.9 |
| LDL- C mmol/L | 3.4 ± 0.7 | 3.4 ± 0.8 | 3.4 ± 0.7 | 3.3 ± 0.9 |
| HDL- C mmol/L | 1.5 ± 0.3 | 1.5 ± 0.3 | 1.5 ± 0.3 | 1.4 ± 0.3 |
| Triglyceride mmol/L | 1.2 ± 0.4 | 1.1 ± 0.4 | 1.2 ± 0.5 | 1.2± 0.5 |
| Vitamin D (nmol/L) 1 | 52.9 ± 15.7 | 56.7 ± 17.0 | 58.3 ± 20.0 | 58.6 ± 1.4 |
| Baseline | 3 Months | |
|---|---|---|
| Egg group (n = 38) | 52.9 ± 15.7 | 64.5 ± 17.6 |
| Cereal group (n = 44) | 56.5 ± 17.2 | 64.9 ± 18.2 |
| Non-Obese | Obese | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | 3 Months | 6 Months | Baseline | 3 Months | 6 Months | |||||||
| Eggs | Cereal | Eggs | Cereal | Eggs | Cereal | Eggs | Cereal | Eggs | Cereal | Eggs | Cereal | |
| Glucose mmol/L | 5.0 ± 0.4 | 4.8 ± 0.4 | 5.0 ± 0.4 | 5.1 ± 0.5 | 5.1 ± 0.8 | 5.0 ± 0.8 | 5.2 ± 0.6 | 5.2 ± 0.7 | ||||
| Total Cholesterol mmol/L | 5.7 ± 1.0 | 5.4 ± 1.0 | 5.7 ± 1.2 | 5.1 ± 0.7 | 5.3 ± 0.7 | 5.4 ± 0.8 | 5.2 ± 0.8 | 5.4 ± 0.9 | ||||
| LDL- C mmol/L | 3.5 ± 0.8 | 3.4 ± 0.9 | 3.5 ± 1.0 | 3.1 ± 0.8 | 3.3 ± 0.7 | 3.4 ± 0.7 | 3.3 ± 0.7 | 3.4 ± 0.8 | ||||
| HDL- C mmol/L | 1.7 ± 0.2 | 1.5 ± 0.3 | 1.7 ± 0.2 | 1.4 ± 0.3 | 1.5 ± 0.3 | 1.5 ± 0.3 | 1.4 ± 0.3 | 1.5 ± 0.3 | ||||
| Triglyceride mmol/L | 1.1 ± 0.5 | 1.2 ± 0.5 | 1.1 ± 0.5 | 1.1 ± 0.4 | 1.2 ± 0.4 | 1.2 ± 0.6 | 1.1 ± 0.4 | 1.2 ± 0.6 | ||||
| Vitamin D nmol/L | 55.8 ± 13.0 | 57.9 ± 14.0 | 65.0 ± 12.1 | 64.6 ± 16.2 | 55.7 ± 13.3 | 63.7 ± 17.0 | 51.7 ± 16.8 | 56.2 ± 182 | 66.2 ±19.7 | 64.8 ± 17.6 | 59.3 ± 22.2 | 56.7 ± 17.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Keogh, J.B.; Clifton, P.M. No Difference in Weight Loss, Glucose, Lipids and Vitamin D of Eggs for Breakfast Compared with Cereal for Breakfast during Energy Restriction. Int. J. Environ. Res. Public Health 2020, 17, 8827. https://doi.org/10.3390/ijerph17238827
Keogh JB, Clifton PM. No Difference in Weight Loss, Glucose, Lipids and Vitamin D of Eggs for Breakfast Compared with Cereal for Breakfast during Energy Restriction. International Journal of Environmental Research and Public Health. 2020; 17(23):8827. https://doi.org/10.3390/ijerph17238827
Chicago/Turabian StyleKeogh, Jennifer B., and Peter M. Clifton. 2020. "No Difference in Weight Loss, Glucose, Lipids and Vitamin D of Eggs for Breakfast Compared with Cereal for Breakfast during Energy Restriction" International Journal of Environmental Research and Public Health 17, no. 23: 8827. https://doi.org/10.3390/ijerph17238827
APA StyleKeogh, J. B., & Clifton, P. M. (2020). No Difference in Weight Loss, Glucose, Lipids and Vitamin D of Eggs for Breakfast Compared with Cereal for Breakfast during Energy Restriction. International Journal of Environmental Research and Public Health, 17(23), 8827. https://doi.org/10.3390/ijerph17238827