Selected Behavioural Factors Affecting Oral Health in Schoolchildren: Results from the Health Behaviour in School-Aged Children (HBSC) Slovak Study

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Design of the Study
2.2. Sample
2.3. Questionnaire
2.4. Data Collection
2.5. Analysed Variables
2.6. Statistical Analysis
3. Results
4. Discussion
Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Available online: https://www.who.int/health-topics/oral-health/ (accessed on 28 October 2019).
- Anil, S.; Anand, P.S. Early Childhood Caries: Prevalence, Risk Factors, and Prevention. Front. Pediatr. 2017, 5, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Jürgensen, N.; Petersen, P.E. Promoting oral health of children through schools—Results from a WHO global survey 2012. Community Dent. Health 2013, 30, 204–218. [Google Scholar] [PubMed]
- Petersen, P.E.; Bourgeois, D.; Ogawa, H.; Estupinan-Day, S.; Ndiaye, C. The global burden of oral diseases and risks to oral health. Bull World Health Organ. 2005, 83, 661–669. [Google Scholar] [PubMed]
- Tagliaferro, E.P.S.; Ambrosano, G.M.B.; Meneghim, M.C.; Pereira, A.C. Risk indicators and risk predictors of dental caries in schoolchildren. J. Appl. Oral Sci. 2008, 16, 408–413. [Google Scholar] [CrossRef]
- Hall-Scullin, E.; Whitehead, H.; Milsom, K.; Tickle, M.; Su, T.L.; Walsh, T. Longitudinal Study of caries Development from Childhood to Adolescence. J. Dent. Res. 2017, 96, 762–767. [Google Scholar] [CrossRef] [PubMed]
- Oral Health Platform. Available online: http://www.oralhealthplatform.eu/wp-content/uploads/2015/09/Report-the-State-of-Oral-Health-in-Europe.pdf (accessed on 10 September 2020).
- Petersen, P.E.; Baez, R.; Kwan, S.; Ogawa, H. Future Use of Materials for Dental Restoration: Report of the Meeting Convened at WHO HQ, Geneva, Switzerland 16th to 17th November 2009; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Attin, T.; Hornecker, E. Tooth brushing and oral health: How frequently and when should tooth brushing be performed. Oral Health Prev. Dent. 2005, 3, 135–140. [Google Scholar]
- Ndagire, B.; Kutesa, A.; Ssenyonga, R.; Mayanja Kiiza, H.; Nakanjako, D.; Mugisha Rwenyonyi, C. Prevalence, Severity and Factors Associated with Dental Caries Among School Adolescents in Uganda: A cross Sectional Study. Braz. Dent. J. 2020, 31, 171–178. [Google Scholar] [CrossRef]
- Obregón-Rodríguez, N.; Fernández-Riveiro, P.; Piñeiro-Lamas, M.; Smyth-Chamosa, E.; Montes-Martínez, A.; Suárez-Cunqueiro, M.M. Prevalence and caries-related risk factors in schoolchildren if 12- and 15-year-old: A cross-sectional study. BMC Oral Health 2019, 19, 120. [Google Scholar] [CrossRef]
- Peres, M.A.; Sheiham, A.; Liu, P.; Demarco, F.F.; Silva, A.E.R.; Assunção, M.C.; Menezes, A.M.; Barros, F.C.; Peres, K.G. Sugar Consumption and Changes in Dental Caries from Childhood to Adolescence. J. Dent. Res. 2016, 95, 388–394. [Google Scholar] [CrossRef]
- Moynihan, P.J.; Kelly, S.A. Effect on caries of restricting sugars intake: Systematic review to inform WHO guidelines. J. Dent. Res. 2014, 93, 8–18. [Google Scholar] [CrossRef]
- Da Silveira Moreira, R. Epidemiology of Dental Caries in the World. In Oral Health Care-Pediatric, Research, Epidemiology and Clinical Practices; Virdi, M., Ed.; IntechOpen: London, UK, 2012; pp. 149–168. [Google Scholar]
- Národné Centrum Zdravotníckych Informácií. Zubnolekárska starostlivosť v SR 2017. In Štatistické prehľady; Štatisticképrehľady: Bratislava, Slovakia, 2018; Volume 3, pp. 1–7. [Google Scholar]
- Ostberg, A.L.; Halling, A.; Lindblad, U. Gender differences in knowledge, attitude, behavior and perceived oral health among adolecents. Acta Odontol. Scand. 1999, 57, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Azodo, C.C.; Unamatokpa, B. Gender Differences in Oral Health Perception and Practices among Medical House Officers. Russ. Open Med. J. 2012, 1, 1–4. [Google Scholar] [CrossRef]
- Branch-Elliman, D.A. Gender-Based Approach to Oral Health Changes Across the Lifespan. Bachelor’s Thesis, University of Pennsylvania, Philadelphia, PA, USA, 2012. [Google Scholar]
- Cianetti, S.; Lombardo, G.; Lupatelli, E.; Rossi, G.; Abraha, I.; Pagano, S.; Paglia, L. Dental caries, parents educational level, family income and dental service attendance among children in Italy. Eur. J. Paediatr. Dent. 2017, 18, 15–18. [Google Scholar] [PubMed]
- Armfield, J.M.; Spencer, A.J.; Roberts-Thomson, K.F.; Plastow, K. Water Fluoridation and the association of sugar-sweetened beverage consumption and dental caries in Australian children. Am. J. Public Health 2013, 103, 494–500. [Google Scholar] [CrossRef] [PubMed]
- Asawa, K.; Sen, N.; Bhat, N.; Tak, M.; Sultane, P.; Patil, V. Association of sugary foods and drinks consumption with behavioral risk and oral health status of 12- and 15-year-old Indian school children. J. Educ. Health Promot. 2018, 7, 19. [Google Scholar]
- Bolt-Evensen, K.; Vik, F.N.; Stea, T.H.; Klepp, K.I.; Bere, E. Consumption of sugar-sweetened beverages and artificially sweetened beverages from childhood to adulthood in relation to socioeconomic status – 15 years follow-up in Norway. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 8. [Google Scholar] [CrossRef]
- Abiola Adeniyi, A.; Eyitope Ogunbodede, O.; Sonny Jeboda, O.; Morenike Folayan, O. Do maternal factors influence the dental health status of Nigerian pre-school children. Int. J. Paediatr. Dent. 2009, 19, 448–454. [Google Scholar] [CrossRef]
- Park, J.B.; Han, K.; Park, Y.G.; Ko, Y. Association between socioeconomic status and oral health behaviors: The 2008–2010 Korea national health and nutrition examination survey. Exp. Med. 2016, 12, 2657–2664. [Google Scholar] [CrossRef]
- Levin, K.A.; Currie, C. Adolescents toothbrushing and the home environment: Sociodemographic factors, family relationships and mealtime routines and disorganization. Community Dent. Oral Epidemiol. 2010, 38, 10–18. [Google Scholar] [CrossRef]
- Dukić, W.; Delija, B.; Dukić, O.L. Caries prevalence among schoolchildren in Zagreb, Croatia. Croat Medj. 2011, 52, 665–671. [Google Scholar] [CrossRef]
- Roberts, C.; Currie, C.; Samdal, O.; Currie, D.; Smith, R.; Maes, L. Measuring the health and health behaviours of adolescents through cross-national survey research: Recent developments in the Health Behaviour in School-Aged Children (HBSC) Study. J. Public Health 2007, 15, 179–186. [Google Scholar] [CrossRef]
- Tarvonen, P.-L.; Suominen, A.L.; Yang, G.S.; Ri, Y.S.; Sipilä, K. Association between oral health habits and dental caries among children in Pyongyang, Democratic People’s Republic of Korea. Int. J. Dent. Hyg. 2017, 15, 136–142. [Google Scholar] [CrossRef]
- Skadifa, V.; Chambers, S. Positive associations between sugar consumption and dental decay prevalence independent of oral hygiene in pre-school children: A longitudinal prospective study. J. Public Health 2018, 40, 275–283. [Google Scholar]
- STATdat Public Database. Available online: http://statdat.statistics.sk/cognosext/cgi-bin/cognos.cgi?b_action=xts.run&m=portal/cc.xts&gohome= (accessed on 22 October 2019).
- Jamieson, L.M.; Thomson, W.M.; McGee, R. An assessment of the validity and reliability of dental self-report items used in a National Child Nutrition Survey. Community Dent. Oral Epidemiol. 2004, 32, 49–54. [Google Scholar] [CrossRef]
- McGrath, C.; Bedi, R. Gender variations in the social impact of oral health. J. Ir. Dent. Assoc. 2000, 46, 87–91. [Google Scholar]
- Maes, L.; Vereecken, C.; Vanobbergen, J.; Honkala, S. Tooth brushing and social characteristics of families in 32 countries. Int. Dentj. 2006, 56, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Hamasha, A.A.-H.; Alshehri, A.; Alshubaiki, A.; Alssafi, F.; Alamam, H.; Alshunaiber, R. Gender-specific oral health beliefs and behaviors among adult patients attending King Abdulaziz Medical City in Riyadh. Saudi Dent. J. 2018, 30, 226–231. [Google Scholar] [CrossRef] [PubMed]
- Poche, C.; McCubbrey, H.M.; Munn, T. The development of correct toothbrushing technique in preschool children. J. Appl. Behav. Anal. 1982, 15, 315–320. [Google Scholar] [CrossRef]
- Damle, S.G.; Patil, A.; Jain, S.; Damle, D.; Chopal, N. Effectiveness of supervised toothbrushing and oral health education in improving oral hygiene status and practices of urban and rural school children: A comparative study. J. Int. Soc. Prev. Community Dent. 2014, 4, 175–181. [Google Scholar] [CrossRef]
- Ahad, M.; Sukumaran, G. Awareness of tooth brushing techniques and proper oral hygiene among school children. J. Pharm. Sci. Res. 2015, 7, 367–372. [Google Scholar]
- Naseem, S.; Fatima, S.H.; Ghazanfar, H.; Haq, S.; Khan, N.A.; Mehmood, M.; Ghazanfar, A. Oral Hygiene Practices and Teeth Cleaning Techniques Among Medical Students. Cureus 2017, 9, 1487. [Google Scholar] [CrossRef] [PubMed]
- Melo, P.; Fine, C.; Malone, S.; Frencken, J.E.; Horn, V. The effectiveness of the Brush Day and Night programme in improving children’s toothbrushing knowledge and behaviour. Int. Dentj. 2018, 68, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Al-Omiri, M.K.; Al-Wahadni, A.M.; Saeed, K.N. Oral health attitudes, knowledge, and behaviour among school children in North Jordan. J. Dent. Educ. 2006, 70, 179–187. [Google Scholar] [CrossRef]
- Shaghaghian, S.; Zeraatkar, M. Factors Affecting Oral Hygiene and Tooth Brushing in Preschool Children, Shiraz/Iran. J. Dent. Biomater. 2017, 4, 394–402. [Google Scholar]
- Tromp, K.; Zwaan, C.M.; van de Varthorst, S. Motivations of children and their parents to participate in drug research: A systematic review. Eur. J. Pediatr. 2016, 175, 599–612. [Google Scholar] [CrossRef] [PubMed]
- Javed, F.; Feng, C.; Kopycka-Kedzierawski, D.T. Incidence of early childhood caries: A systematic review and meta-analysis. J. Investig. Clin. Dent. 2017, 8, 12238. [Google Scholar] [CrossRef]
- Frencken, J.E.; Sharma, P.; Stenhouse, L.; Green, D.; Laverty, D.; Dietrich, T. Global epidemiology of dental caries and severe periodontitis—A comprehensive review. J. Clin. Periodontol. 2017, 44, 94–105. [Google Scholar] [CrossRef]
- Kostičová, M. Ústne zdravie. In Sociálne determinanty zdravia školákov; Madarasová Gecková, A., Ed.; Equilibria, s.r.o.: Košice, Slovakia, 2019; pp. 49–57. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| School Year | Number of Schools Involved in the Survey | Total Number of Respondents | Number of 11 to 13-Year-Old Respondents (Boys; Girls) | Response Rate (%) |
|---|---|---|---|---|
| 2005/2006 | 87 | 3877 | 2525 (1203; 1322) | 86 |
| 2009/2010 | 106 | 4308 | 2740 (1302; 1438) | 80 |
| 2013/2014 | 130 | 5245 | 3696 (1811; 1885) | 79 |
| 2017/2018 | 109 | 8902 | 5260 (2651; 2609) | 60 |
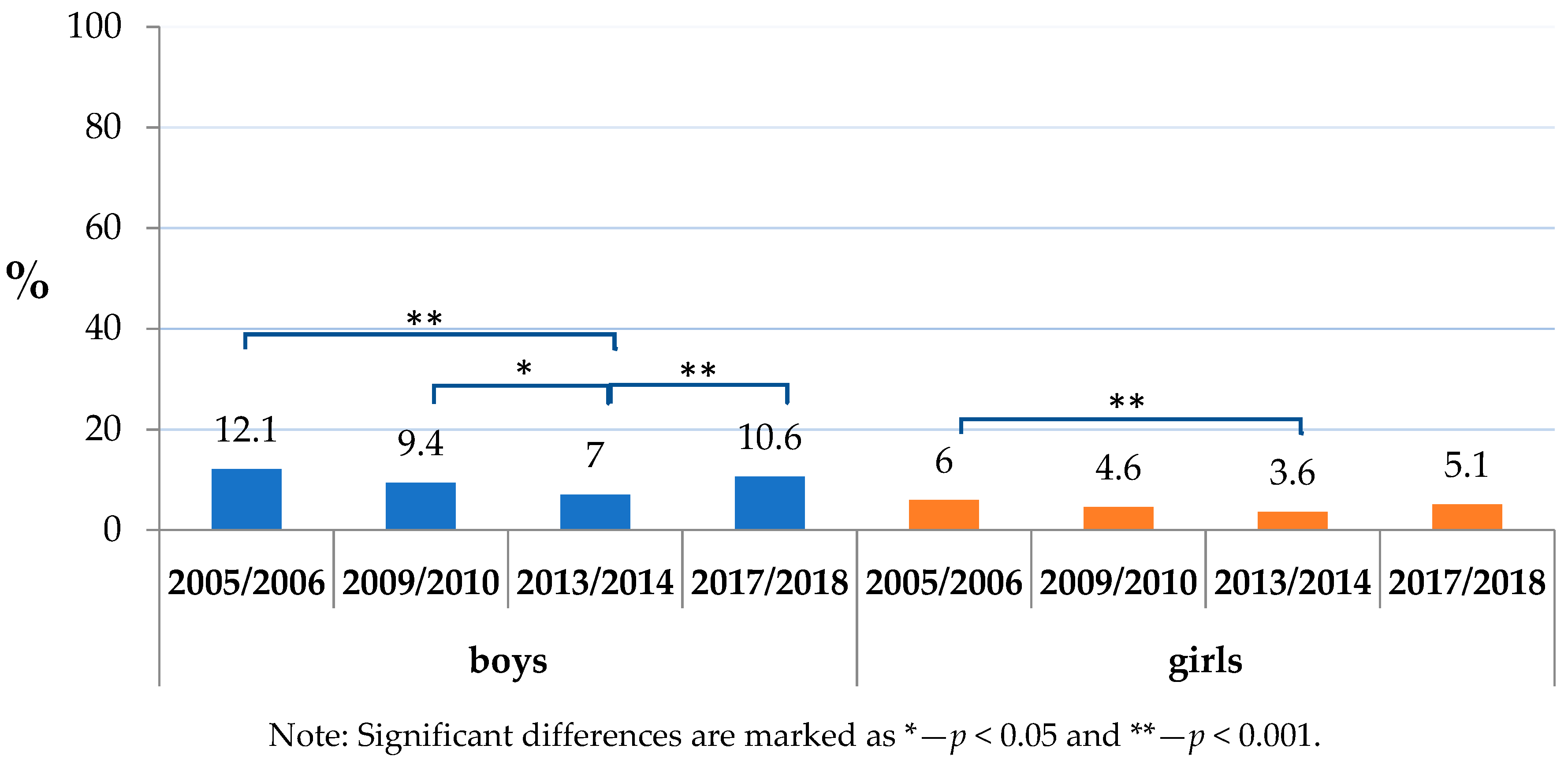
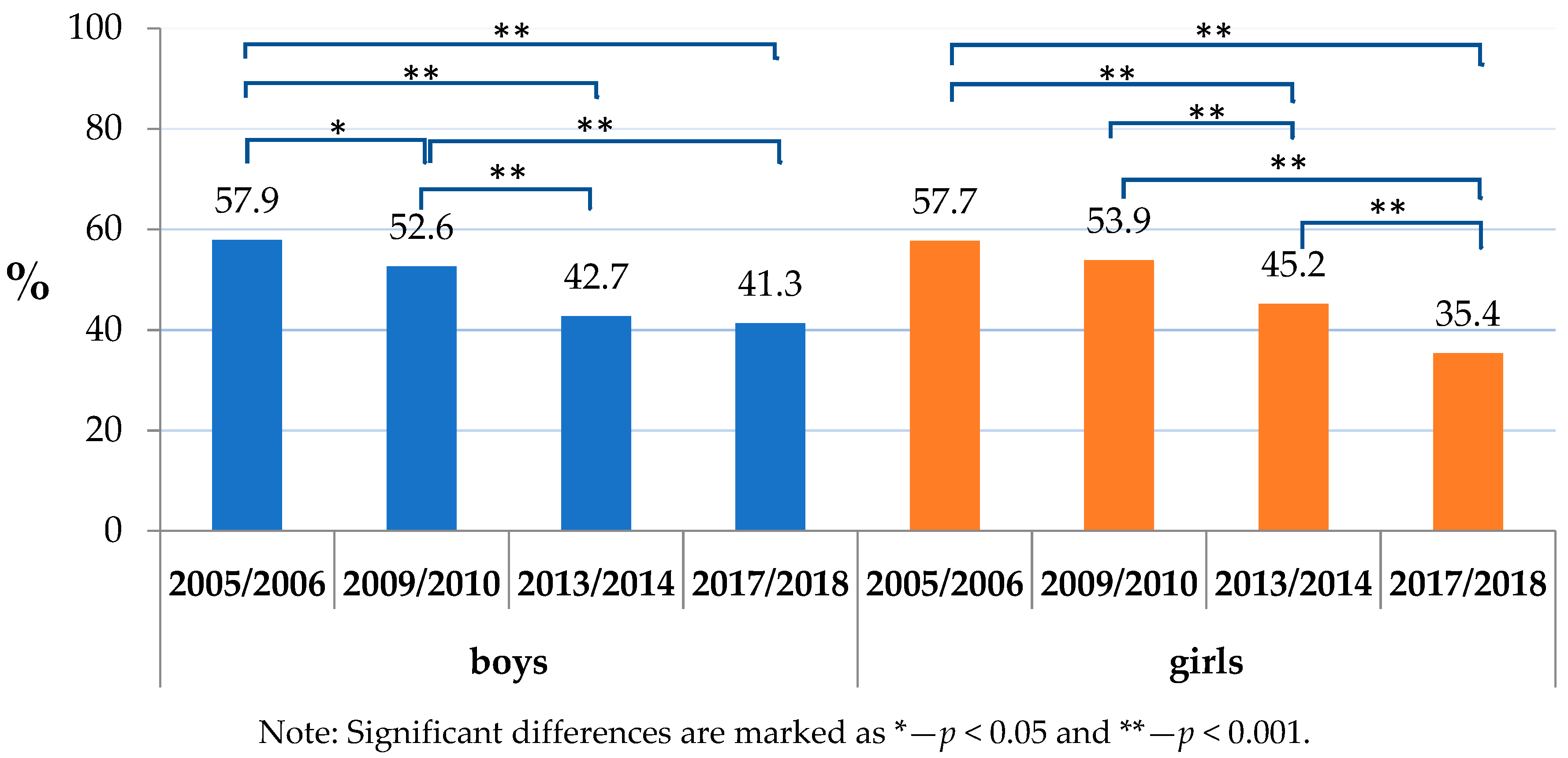
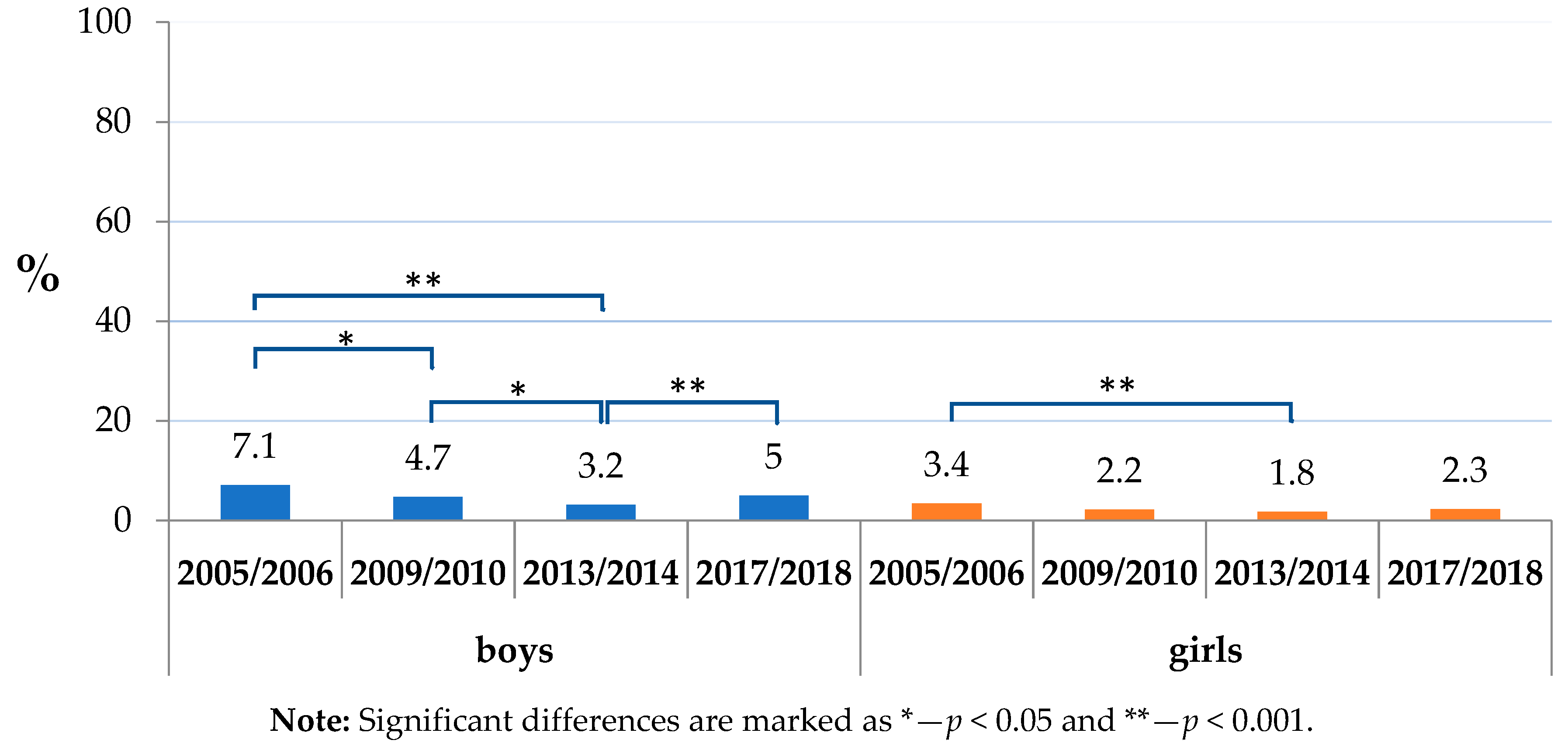
| School Year | Sex | Absence of Daily Toothbrushing | Daily Consumption of Sweets and/or Sweetened Soft Drinks | Co-occurring of Daily Toothbrushing Absence with Consumption of Sweets and/or Sweetened Soft Drinks | |||
|---|---|---|---|---|---|---|---|
| Absolute Number (Abs.) (%) | Difference (Diff.) (p-Value) | Abs. (%) | Diff. (p-Value) | Abs. (%) | Diff. (p-Value) | ||
| 2005/2006 | Boys | 145 (12.1) | <0.001 | 696 (57.9) | 0.951 | 85 (7.1) | <0.001 |
| Girls | 86 (6.0) | 821 (57.7) | 49 (3.4) | ||||
| 2009/2010 | Boys | 203 (9.4) | <0.001 | 1141 (52.6) | 0.399 | 102 (4.7) | <0.001 |
| Girls | 108 (4.6) | 1278 (53.9) | 53 (2.2) | ||||
| 2013/2014 | Boys | 187 (7.0) | <0.001 | 1142 (42.7) | 0.071 | 85 (3.2) | <0.001 |
| Girls | 98 (3.6) | 1229 (45.2) | 49 (1.8) | ||||
| 2017/2018 | Boys | 280 (10.6) | <0.001 | 1096 (41.3) | 0.196 | 133 (5.0) | <0.001 |
| Girls | 132 (5.1) | 1033 (39.6) | 61 (2.3) | ||||
| School Year | FAS | Absence of Daily Toothbrushing | Daily Consumption of Sweets and/or Sweetened Soft Drinks | Co-occurring of Daily Toothbrushing Absence with Consumption of Sweets and/or Sweetened Soft Drinks | |||
|---|---|---|---|---|---|---|---|
| Abs. (%) | Diff. (p-Value) | Abs. (%) | Diff. (p-Value) | Abs. (%) | Diff. (p-Value) | ||
| 2005/2006 | Low FAS | 85 (13.9) | 0.034 | 365 (59.8) | 0.265 | 49 (8.0) | 0.130 |
| High FAS | 48 (9.8) | 278 (56.5) | 28 (5.7) | ||||
| 2009/2010 | Low FAS | 105 (10.6) | 0.028 | 507 (51.0) | 0.113 | 52 (5.2) | 0.161 |
| High FAS | 67 (7.6) | 480 (54.7) | 34 (3.9) | ||||
| 2013/2014 | Low FAS | 95 (7.9) | 0.008 | 500 (41.7) | 0.556 | 45 (3.8) | 0.053 |
| High FAS | 55 (5.2) | 458 (42.9) | 25 (2.3) | ||||
| 2017/2018 | Low FAS | 128 (11.7) | 0.008 | 452 (41.3) | 0.540 | 66 (6.0) | 0.002 |
| High FAS | 60 (7.9) | 302 (39.9) | 22 (2.9) | ||||
| School Year | FAS | Absence of Daily Toothbrushing | Daily Consumption of Sweets or Sweetened Soft Drinks | Absence of Toothbrushing Combined with Daily Consumption of Sweets or Sweetened Soft Drinks | |||
|---|---|---|---|---|---|---|---|
| Abs. (%) | Diff. (p-Value) | Abs. (%) | Diff. (p-Value) | Abs. (%) | Diff. (p-Value) | ||
| 2005/2006 | Low FAS | 60 (7.0) | 0.007 | 507 (58.7) | 0.223 | 36 (4.2) | 0.015 |
| High FAS | 16 (3.4) | 261 (55.3) | 8 (1.7) | ||||
| 2009/2010 | Low FAS | 74 (5.8) | 0.002 | 689 (53.7) | 0.808 | 37 (2.9) | 0.054 |
| High FAS | 25 (2.9) | 474 (54.2) | 14 (1.6) | ||||
| 2013/2014 | Low FAS | 58 (4.3) | 0.014 | 644 (47.7) | 0.006 | 28 (2.1) | 0.189 |
| High FAS | 27 (2.5) | 461 (42.1) | 15 (1.4) | ||||
| 2017/2018 | Low FAS | 67 (5.6) | 0.037 | 493 (40.9) | 0.369 | 33 (2.7) | 0.005 |
| High FAS | 27 (3.5) | 299 (38.9) | 7 (0.9) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Štefanová, E.; Baška, T.; Holubčíková, J.; Timková, S.; Tatarková, M.; Sovičová, M.; Hudečková, H. Selected Behavioural Factors Affecting Oral Health in Schoolchildren: Results from the Health Behaviour in School-Aged Children (HBSC) Slovak Study. Int. J. Environ. Res. Public Health 2020, 17, 7516. https://doi.org/10.3390/ijerph17207516
Štefanová E, Baška T, Holubčíková J, Timková S, Tatarková M, Sovičová M, Hudečková H. Selected Behavioural Factors Affecting Oral Health in Schoolchildren: Results from the Health Behaviour in School-Aged Children (HBSC) Slovak Study. International Journal of Environmental Research and Public Health. 2020; 17(20):7516. https://doi.org/10.3390/ijerph17207516
Chicago/Turabian StyleŠtefanová, Eliška, Tibor Baška, Jana Holubčíková, Silvia Timková, Mária Tatarková, Miroslava Sovičová, and Henrieta Hudečková. 2020. "Selected Behavioural Factors Affecting Oral Health in Schoolchildren: Results from the Health Behaviour in School-Aged Children (HBSC) Slovak Study" International Journal of Environmental Research and Public Health 17, no. 20: 7516. https://doi.org/10.3390/ijerph17207516
APA StyleŠtefanová, E., Baška, T., Holubčíková, J., Timková, S., Tatarková, M., Sovičová, M., & Hudečková, H. (2020). Selected Behavioural Factors Affecting Oral Health in Schoolchildren: Results from the Health Behaviour in School-Aged Children (HBSC) Slovak Study. International Journal of Environmental Research and Public Health, 17(20), 7516. https://doi.org/10.3390/ijerph17207516