Acute Effects of Self-Selected Music Intervention on Golf Performance and Anxiety Level in Collegiate Golfers: A Crossover Study



Abstract
1. Introduction
2. Materials and Methods
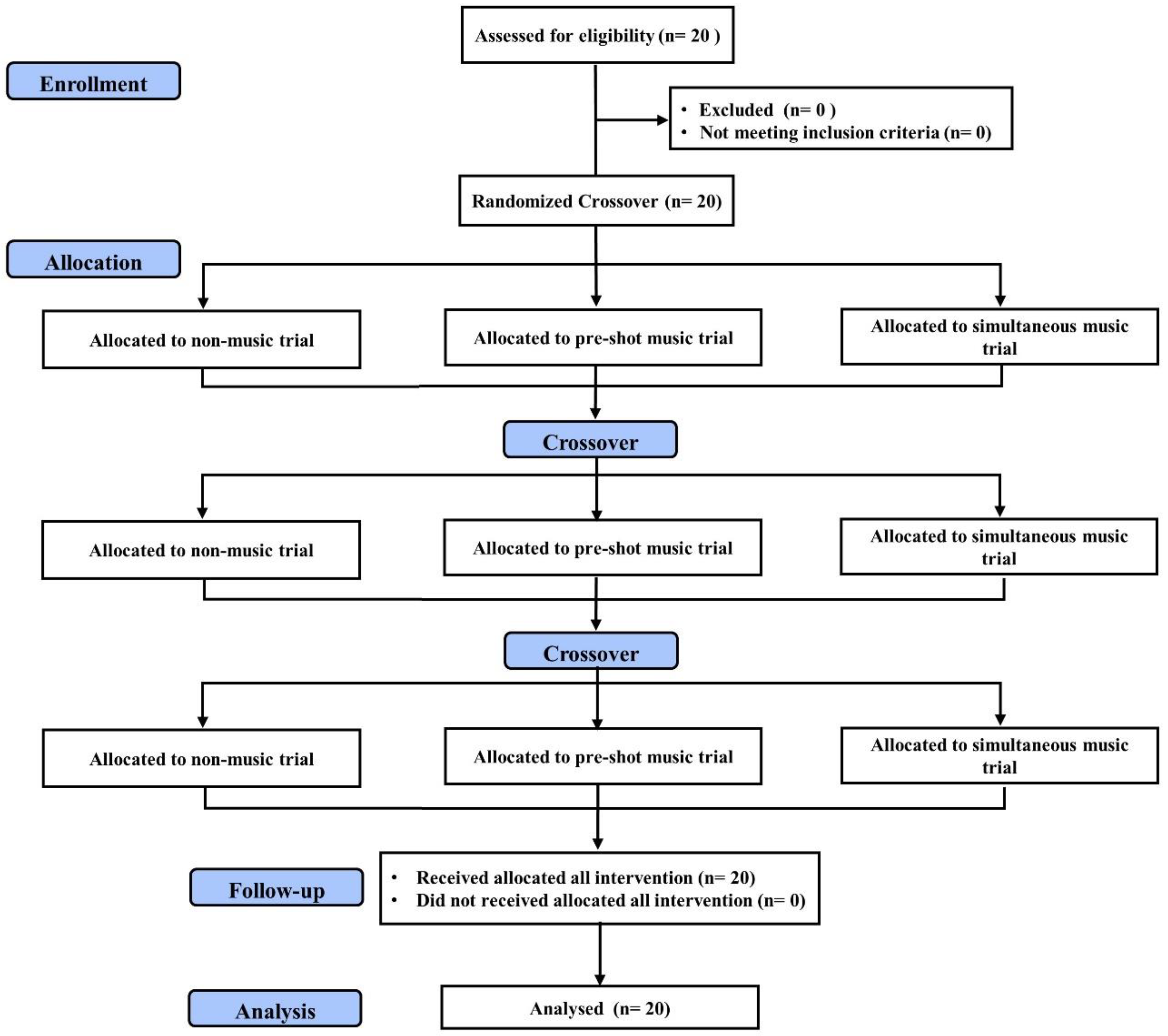
2.1. Experimental Approach to the Problem
2.2. Experimental Procedure
2.3. Participants
2.4. Music Intervention
2.5. Golf Performance
2.6. Heart Rate and Heart Rate Variability
2.7. State-Trait Anxiety Inventory-State
2.8. Statistical Analyses
3. Results
3.1. Physical Characterstics and Individual Self-Selected Music
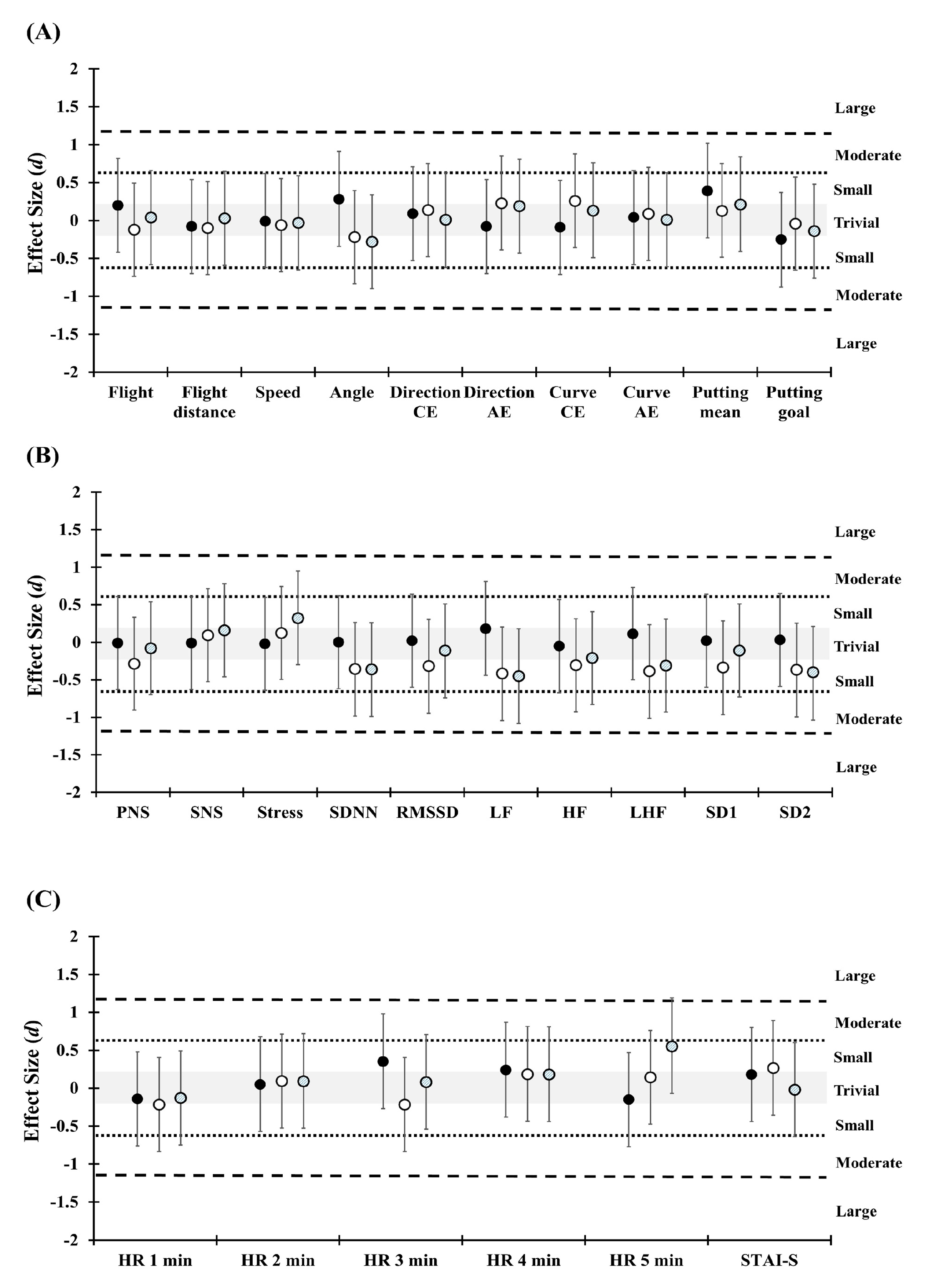
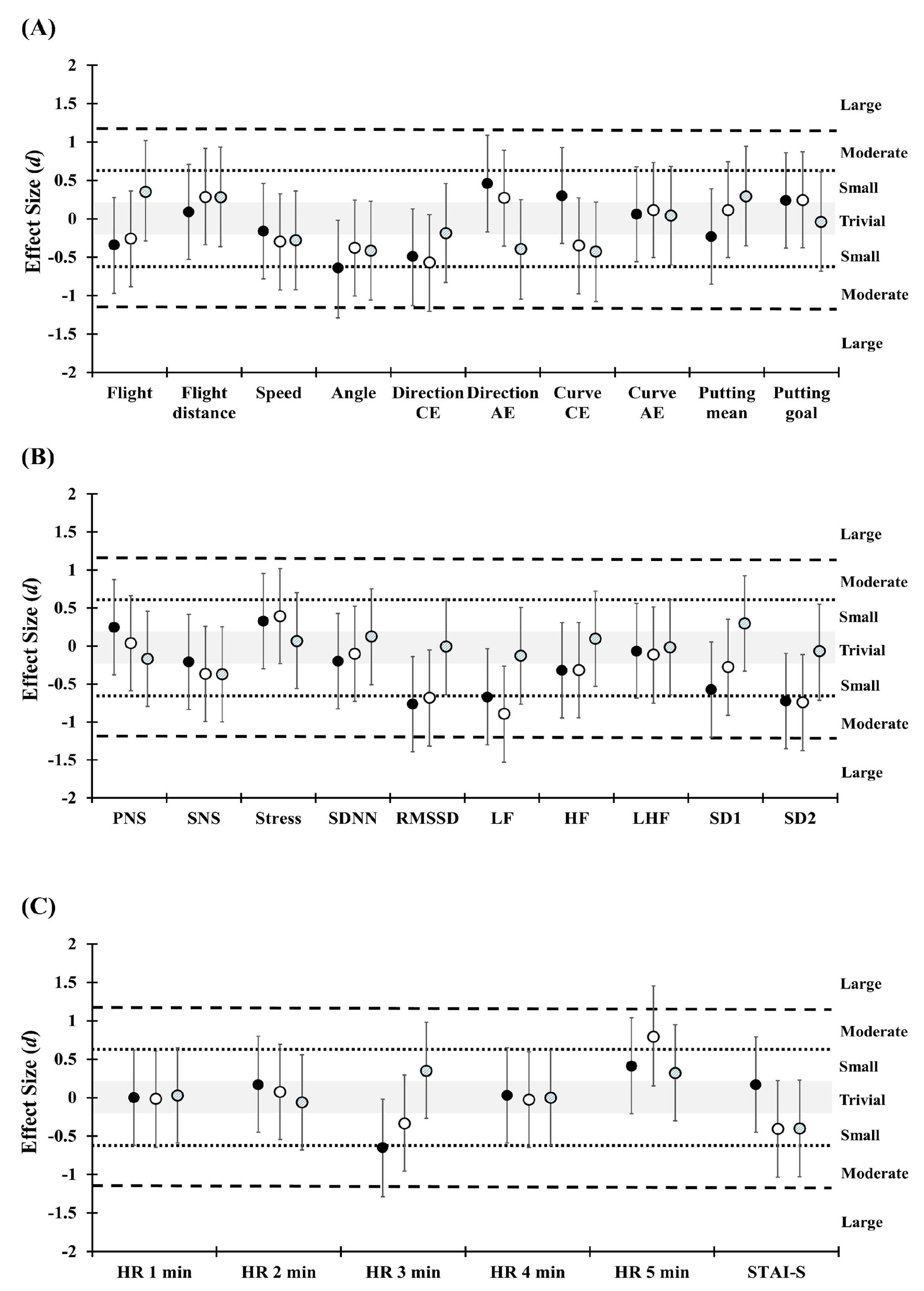
3.2. Golf Performance
3.3. State-Trait Anxiety Inventory-State
3.4. Heart Rate and Heart Rate Variability
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sheehan, W.B.; Watsford, M.L.; Pickering Rodriguez, E.C. Examination of the neuromechanical factors contributing to golf swing performance. J. Sports Sci. 2019, 37, 458–466. [Google Scholar] [CrossRef] [PubMed]
- Steele, K.M.; Roh, E.Y.; Mahtani, G.; Meister, D.W.; Ladd, A.L.; Rose, J. Golf swing rotational velocity: The essential follow-through. Ann. Rehabil. Med. 2018, 42, 713–721. [Google Scholar] [CrossRef] [PubMed]
- Richardson, A.K.; Mitchell, A.C.S.; Hughes, G. The effect of movement variability on putting proficiency during the golf putting stroke. Int. J. Sports Sci. Coach. 2018, 13, 590–597. [Google Scholar] [CrossRef]
- Bartolomei, S.; Michele, R.D.; Merni, F. Effects of self-selected music on maximal bench press strength and strength endurance. Percept. Mot. Ski. 2015, 120, 714–721. [Google Scholar] [CrossRef]
- Biagini, M.S.; Brown, L.E.; Coburn, J.W.; Judelson, D.A.; Statler, T.A.; Bottaro, M.; Tran, T.T.; Longo, N.A. Effects of self-selected music on strength, explosiveness, and mood. J. Strength Cond. Res. 2012, 26, 1934–1938. [Google Scholar] [CrossRef]
- Bigliassi, M.; Karageorghis, C.I.; Bishop, D.T.; Nowicky, A.V.; Wright, M.J. Cerebral effects of music during isometric exercise: An fMRI study. Int. J. Psychophysiol. 2018, 133, 131–139. [Google Scholar] [CrossRef]
- Karageorghis, C.I.; Hutchinson, J.C.; Jones, L.; Farmer, H.L.; Ayhan, M.S.; Wilson, R.C.; Rance, J.; Hepworth, C.J.; Bailey, S.G. Psychological, psychophysical, and ergogenic effects of music in swimming. Psychol. Sports Exerc. 2013, 14, 560–568. [Google Scholar] [CrossRef]
- Smirmaul, B.; Dos Santos, R.; Da Silva Neto, L. Pre-task music improves swimming performance. J. Sports. Med. Phys. Fit. 2015, 55, 1445–1451. [Google Scholar]
- Atkinson, G.; Wilson, D.; Eubank, M. Effects of music on work-rate distribution during a cycling time trial. Int. J. Sports Med. 2004, 25, 611–615. [Google Scholar] [CrossRef]
- Bigliassi, M.; Karageorghis, C.I.; Wright, M.J.; Orgs, G.; Nowicky, A.V. Effects of auditory stimuli on electrical activity in the brain during cycle ergometry. Physiol. Behav. 2017, 177, 135–147. [Google Scholar] [CrossRef]
- Nakamura, P.M.; Pereira, G.; Papini, C.B.; Nakamura, F.Y.; Kokubun, E. Effects of preferred and nonpreferred music on continuous cycling exercise performance. Percept. Mot. Ski. 2010, 110, 257–264. [Google Scholar] [CrossRef]
- Bigliassi, M.; León-Domínguez, U.; Buzzachera, C.F.; Barreto-Silva, V.; Altimari, L.R. How does music aid 5 km of running? J. Strength Cond. Res. 2015, 29, 305–314. [Google Scholar] [CrossRef] [PubMed]
- Terry, P.C.; Karageorghis, C.I.; Saha, A.M.; D’Auria, S. Effects of synchronous music on treadmill running among elite triathletes. J. Sci. Med. Sports 2012, 15, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Arazi, H.; Asadi, A.; Purabed, M. Physiological and psychophysical responses to listening to music during warm-up and circuit-type resistance exercise in strength trained men. J. Sports Med. 2015, 2015, 389831. [Google Scholar] [CrossRef] [PubMed]
- Karageorghis, C.I.; Priest, D.L.; Williams, L.S.; Hirani, R.M.; Lannon, K.M.; Bates, B.J. Ergogenic and psychological effects of synchronous music during circuit-type exercise. Psychol. Sports Exerc. 2010, 11, 551–559. [Google Scholar] [CrossRef]
- Ballmann, C.G.; Maynard, D.J.; Lafoon, Z.N.; Marshall, M.R.; Williams, T.D.; Rogers, R.R. Effects of listening to preferred versus non-preferred music on repeated wingate anaerobic test performance. Sports 2019, 7, 185. [Google Scholar] [CrossRef]
- Castañeda-Babarro, A.; Marqués-Jiménez, D.; Calleja-González, J.; Viribay, A.; León-Guereño, P.; Mielgo-Ayuso, J. Effect of listening to music on Wingate anaerobic test performance. A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2020, 17, 4564. [Google Scholar] [CrossRef]
- Chtourou, H.; Jarraya, M.; Aloui, A.; Hammouda, O.; Souissi, N. The effects of music during warm-up on anaerobic performances of young sprinters. Sci. Sports 2012, 27, e85–e88. [Google Scholar] [CrossRef]
- Stork, M.; MY, K.; Gibala, M.; Martin, G.K. Music enhances performance and perceived enjoyment of sprint interval exercise. Med. Sci. Sport. Exer. 2015, 47, 1052–1060. [Google Scholar] [CrossRef]
- Bishop, D.T.; Wright, M.J.; Karageorghis, C.I. Tempo and intensity of pre-task music modulate neural activity during reactive task performance. Psychol. Music 2014, 42, 714–727. [Google Scholar] [CrossRef]
- Kuan, G.; Morris, T.; Terry, P. Effects of music on arousal during imagery in elite shooters: A pilot study. PLoS ONE 2017, 12, e0175022. [Google Scholar] [CrossRef] [PubMed]
- Karageorghis, C.I.; Priest, D.-L. Music in the exercise domain: A review and synthesis (Part II). Int. Rev. Sports Exerc. Psychol. 2012, 5, 67–84. [Google Scholar] [CrossRef] [PubMed]
- Bigliassi, M.; Karageorghis, C.I.; Nowicky, A.V.; Orgs, G.; Wright, M.J. Cerebral mechanisms underlying the effects of music during a fatiguing isometric ankle-dorsiflexion task. Psychophysiology 2016, 53, 1472–1483. [Google Scholar] [CrossRef] [PubMed]
- Koelsch, S. Toward a neural basis of music perception—A review and updated model. Front. Psychol. 2011, 2. [Google Scholar] [CrossRef] [PubMed]
- Karageorghis, C.I.; Priest, D.-L. Music in the exercise domain: A review and synthesis (Part I). Int. Rev. Sports Exerc. Psychol. 2012, 5, 44–66. [Google Scholar] [CrossRef]
- Pineschi, G.; Di Pietro, A. Anxiety management through psychophysiological techniques: Relaxation and psyching-up in sport. J. Sports Psychol. Action 2013, 4, 181–190. [Google Scholar] [CrossRef]
- Smirmaul, B. Effect of pre-task music on sports or exercise performance. J. Sports Med. Phys. Fit. 2017, 57, 976–984. [Google Scholar]
- Simpson, S.D.; Karageorghis, C.I. The effects of synchronous music on 400-m sprint performance. J. Sports Sci. 2006, 24, 1095–1102. [Google Scholar] [CrossRef]
- Tapps, T.; Baghurst, T.; Boolani, A.; Jacobson, B. The influence of musical genres on putting accuracy in golf: An exploratory study. J. Athl Enhanc. 3 2014, 5, 2. [Google Scholar] [CrossRef]
- Gabana, N.T.; Hutchinson, J.; Beauchemin, J.; Powless, M.; Cawthra, J.; Halterman, A.; Steinfeldt, J. A qualitative investigation of music use among amateur and semi-professional golfers. Sports 2019, 7, 60. [Google Scholar] [CrossRef]
- Priest, D.; Karageorghis, C.; Sharp, N. The characteristics and effects of motivational music in exercise settings: The possible influence of gender, age, frequency of attendance, and time of attendance. J. Sports Med. Phys. Fit. 2004, 44, 77–86. [Google Scholar]
- Koelsch, S.; Jäncke, L. Music and the heart. Eur. Heart J. 2015, 36, 3043–3049. [Google Scholar] [CrossRef] [PubMed]
- Karageorghis, C.I.; Terry, P.C.; Lane, A.M. Development and initial validation of an instrument to assess the motivational qualities of music in exercise and sport: The Brunel music rating inventory. J. Sports Sci. 1999, 17, 713–724. [Google Scholar] [CrossRef] [PubMed]
- Tarvainen, M.P.; Niskanen, J.-P.; Lipponen, J.A.; Ranta-aho, P.O.; Karjalainen, P.A. Kubios HRV—Heart rate variability analysis software. Comput. Meth. Prog. Biomed. 2014, 113, 210–220. [Google Scholar] [CrossRef]
- Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Heart rate variability: Standards of measurement, physiological interpretation, and clinical use. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef]
- Tarvainen, M.P.; Lipponen, J.; Niskanen, J.-P.; Ranta-aho, P.O. Kubios HRV User’s Guide Version 3.3. Available online: https://www.kubios.com/downloads/Kubios_HRV_Users_Guide.pdf (accessed on 10 August 2020).
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R.E. Manual for the State-Trait Anxiety Inventory; Consulting Psychologists Press: Polo Alto, CA, USA, 1970. [Google Scholar]
- Chen, Y.-S.; Liao, C.-J.; Lu, W.-A.; Kuo, C.-D. Sympathetic enhancement in futsal players but not in football players after repeated sprint ability test. BMJ. Open Sport Exerc. Med. 2015, 1, e000049. [Google Scholar] [CrossRef]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 2009, 41, 3–12. [Google Scholar] [CrossRef]
- Maddigan, M.E.; Sullivan, K.M.; Halperin, I.; Basset, F.A.; Behm, D.G. High tempo music prolongs high intensity exercise. PeerJ 2019, 6, e6164. [Google Scholar] [CrossRef]
- Arbinaga, F.; Romero-Pérez, N.; Torres-Rosado, L.; Fernández-Ozcorta, E.J.; Mendoza-Sierra, M.I. Influence of music on closed motor skills: A controlled study with novice female dart-throwers. Int. J. Environ. Res. Public Health 2020, 17, 4146. [Google Scholar] [CrossRef]
- Krout, R.E. Music listening to facilitate relaxation and promote wellness: Integrated aspects of our neurophysiological responses to music. Arts Psychother. 2007, 34, 134–141. [Google Scholar] [CrossRef]
- Schaffert, N.; Janzen, T.B.; Mattes, K.; Thaut, M.H. A review on the relationship between sound and movement in sports and rehabilitation. Front. Psychol. 2019, 10. [Google Scholar] [CrossRef] [PubMed]
- Sommer, M.; Häger, C.; Rönnqvist, L. Synchronized metronome training induces changes in the kinematic properties of the golf swing. Sports Biomech. 2014, 13, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Sommer, M.; Rönnqvist, L. Improved motor-timing: Effects of synchronized metro-nome training on golf shot accuracy. J. Sports Sci. Med. 2009, 8, 648–656. [Google Scholar] [PubMed]
- Libkuman, T.M.; Otani, H.; Steger, N. Training in timing improves accuracy in golf. J. Gen. Psychol. 2002, 129, 77–96. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Mean ± SD |
|---|---|
| Gender (male/female, n) | 15/5 |
| Age (years) | 20.2 ± 1.4 |
| Height (cm) | 171.7 ± 8.0 |
| Weight (kg) | 69.5 ± 14.6 |
| Golf experience (years) | 7.5 ± 2.1 |
| Music tempo (bpm, fast/slow) | 130.7 ± 5.2/113.8 ± 8.6 |
| Variables | Non-Music Trial (T1) | Pre-Excise Music Trial (T2) | Simultaneous Music Trial (T3) | T1 Phase One/Two % Difference | T2 Phase One/Two % Difference | T3 Phase One/Two % Difference | |||
|---|---|---|---|---|---|---|---|---|---|
| Phase One | Phase Two | Phase One | Phase Two | Phase One | Phase Two | ||||
| Flight (m) | 162.1 ± 23.7 | 155.2 ± 41.9 | 164.4 ± 23.3 | 166.5 ± 22.6 | 162.8 ± 19.3 | 161.9 ± 23.1 | −4.0 ± 21.9 | 1.4 ± 4.3 | −0.8 ± 5.6 |
| Flight distance (m) | 147.5 ± 25.8 | 149.5 ± 24.9 | 151.6 ± 22.7 | 153.2 ± 22.5 | 149.4 ± 20.2 | 148.8 ± 24.3 | 1.8 ± 8.2 | 1.2 ± 4.1 | −0.8 ± 6.5 |
| Speed (m·s−1) | 76.7 ± 34.9 | 76.8 ± 34.3 | 87.7 ± 31.8 | 88.5 ± 31.9 | 81.4 ± 35.5 | 82.4 ± 34.7 | 0.6 ± 4.7 | 1.3 ± 4.5 | 3.5 ± 16.0 |
| Angle (degree) | 19.3 ± 5.1 | 18.1 ± 3.1 | 18.2 ± 3.3 | 18.9 ± 3.9 | 17.1 ± 4.9 | 18.2 ± 2.3 | −3.6 ± 14.2 | 3.6 ± 6.0 # | 152.7 ± 675.5 |
| Direction CE (degree) | 0.3 ± 2.1 | 0.1 ± 2.1 | 0.7 ± 2.7 | 0.2 ± 2.2 | 0.3 ± 2.1 | 0.3 ± 1.9 | −207.0 ± 499.6 | −21.0 ± 156.0 | −2.3 ± 236.1 |
| Direction AE (degree) | 2.0 ± 1.4 | 2.1 ± 1.2 | 2.3 ± 1.7 | 2.0 ± 1.1 | 2.1 ± 1.4 | 1.9 ± 1.0 | 68.3 ± 200.7 | 0.3 ± 49.0 | 18.4 ± 71.6 |
| Curve CE (bpm) | 75.4 ± 395.7 | 111.0 ± 358.8 | −144.3 ± 366.1 | −246.2 ± 313.3 | −62.3 ± 421.9 | −120.0 ± 424.2 | −95.2 ± 324.8 | −1374.2 ± 5830.9 | −10.1 ± 235.0 |
| Curve AE (bpm) | 428.0 ± 265.3 | 417.8 ± 210.8 | 448.2 ± 273.0 | 419.6 ± 191.1 | 425.8 ± 224.6 | 423.8 ± 236.7 | 29.1 ± 110.4 | 23.4 ± 88.4 | 13.9 ± 56.8 |
| Putting mean (yards) | 0.4 ± 0.2 | 0.3 ± 0.2 | 0.3 ± 0.2 | 0.3 ± 0.2 | 0.3 ± 0.2 | 0.3 ± 0.2 | −1.7 ± 84.7 | 23.3 ± 126.1 | −15.5 ± 71.4 |
| Putting goal (n) | 12.1 ± 3.0 | 13 ± 3.7 | 13.3 ± 3.7 | 13.4 ± 3.7 | 13.1 ± 2.8 | 13.6 ± 4.2 | 15.0 ± 42.8 | 5.7 ± 34.0 | 4.0 ± 27.0 |
| STAI-S | 34.4 ± 8.8 | 33 ± 6.8 | 35.2 ± 7.6 | 32.8 ± 7.6 * | 34.7 ± 9.6 | 34.9 ± 9.3 | −2.9 ± 8.7 | −5.5 ± 19.0 | 1.6 ± 16.0 † |
| Variables | Non-Music Trial (T1) | Pre-Excise Music Trial (T2) | Simultaneous Music Trial (T3) | T1 Phase One /Two % Difference | T2 Phase One /Two % Difference | T3 Phase One /Two % Difference | |||
|---|---|---|---|---|---|---|---|---|---|
| Phase One | Phase Two | Phase One | Phase Two | Phase One | Phase Two | ||||
| SDNN (log) | 3.6 ± 0.3 | 3.6 ± 0.4 | 3.5 ± 0.5 | 3.6 ± 0.5 * | 3.5 ± 0.4 | 3.7 ± 0.4 * | −0.1 ± 7.7 | 4.7 ± 5.2 # | 4.6 ± 7.9 |
| RMSSD (log) | 3.3 ± 0.5 | 3.3 ± 0.5 | 3.3 ± 0.6 | 3.4 ± 0.6 * | 3.3 ± 0.5 | 3.4 ± 0.6 | 0 ± 10.4 | 5.6 ± 9.7 | 2.1 ± 11.4 |
| LF (log) | 6.7 ± 0.7 | 6.6 ± 0.8 | 6.2 ± 0.9 # | 6.6 ± 1.1 * | 6.3 ± 0.9 | 6.7 ± 0.8 * | −1.7 ± 11.8 | 5.9 ± 11.6 # | 7.0 ± 9.2 # |
| HF (log) | 5.6 ± 0.9 | 5.7 ± 1.2 | 5.5 ± 1.2 | 5.8 ± 1.3 | 5.5 ± 1.0 | 5.7 ± 1.1 | 1.3 ± 16.6 | 7.1 ± 21.8 | 4.9 ± 14.2 |
| LHF (log) | 4.0 ± 3.6 | 3.6 ± 3.8 | 2.4 ± 1.4 | 3.2 ± 3.0 | 3.0 ± 2.1 | 4.1 ± 4.5 | 34 ± 136.8 | 38.7 ± 123.1 | 37.8 ± 84.3 |
| SD1 (log) | 3.0 ± 0.5 | 3.0 ± 0.5 | 2.9 ± 0.6 | 3.1 ± 0.6 * | 3.0 ± 0.5 | 3.0 ± 0.6 | 0 ± 11.6 | 6.3 ± 11.3 | 2.4 ± 12.9 |
| SD2 (log) | 3.9 ± 0.3 | 3.9 ± 0.4 | 3.7 ± 0.5 | 3.8 ± 0.5 * | 3.7 ± 0.4 | 3.9 ± 0.4 * | −0.1 ± 7.1 | 4.3 ± 5.4 | 4.6 ± 7.0 # |
| PNS index | −1.2 ± 0.8 | −1.2 ± 0.8 | −1.0 ± 1.0 | −0.8 ± 1.0 | −1.1 ± 0.9 | −1.0 ± 1.1 | −4.5 ± 95.1 | −27.6 ± 70.9 | −15.6 ± 92.9 |
| SNS index | 1.6 ± 1.2 | 1.6 ± 1.4 | 1.6 ± 1.5 | 1.3 ± 1.8 | 1.6 ± 1.3 | 1.4 ± 1.4 | −111.5 ± 447.3 | −52.5 ± 97.3 | −17.7 ± 104.6 |
| Stress index | 12.6 ± 3.7 | 12.6 ± 5 | 13.6 ± 5 | 12.6 ± 6.5 | 13.8 ± 5.1 | 12.2 ± 4.5 * | 1.7 ± 27.7 | −7.8 ± 25.4 | −10.0 ± 20.3 |
| HR1mn (log) | 4.4 ± 0.1 | 4.4 ± 0.1 | 4.4 ± 0.1 | 4.4 ± 0.2 | 4.4 ± 0.1 | 4.4 ± 0.1 | 0.5 ± 2.5 | 0.5 ± 2.3 | 0.5 ± 1.7 |
| HR2mn (log) | 4.4 ± 0.1 | 4.4 ± 0.1 | 4.4 ± 0.1 | 4.3 ± 0.2 | 4.4 ± 0.1 | 4.4 ± 0.2 | −0.1 ± 2.3 | −0.7 ± 3.0 | −0.5 ± 2.4 |
| HR3mn (log) | 4.4 ± 0.1 | 4.4 ± 0.1 * | 4.4 ± 0.1 | 4.4 ± 0.2 | 4.4 ± 0.1 | 4.4 ± 0.2 | −1.1 ± 2.2 | 0.5 ± 2.4 | −0.4 ± 2.5 |
| HR4mn (log) | 4.4 ± 0.1 | 4.4 ± 0.1 | 4.4 ± 0.1 | 4.4 ± 0.2 | 4.4 ± 0.1 | 4.3 ± 0.2 | −0.8 ± 2.8 | −0.8 ± 2.4 | −0.9 ± 2.5 |
| HR5mn (log) | 4.4 ± 0.1 | 4.4 ± 0.1 | 4.4 ± 0.1 | 4.3 ± 0.2 | 4.4 ± 0.1 | 4.3 ± 0.2 * | 0.5 ± 3.1 | −1.1 ± 4.1 | −1.9 ± 2.3 # |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, H.-T.; Tai, H.-L.; Yang, C.-C.; Chen, Y.-S. Acute Effects of Self-Selected Music Intervention on Golf Performance and Anxiety Level in Collegiate Golfers: A Crossover Study. Int. J. Environ. Res. Public Health 2020, 17, 7478. https://doi.org/10.3390/ijerph17207478
Wang H-T, Tai H-L, Yang C-C, Chen Y-S. Acute Effects of Self-Selected Music Intervention on Golf Performance and Anxiety Level in Collegiate Golfers: A Crossover Study. International Journal of Environmental Research and Public Health. 2020; 17(20):7478. https://doi.org/10.3390/ijerph17207478
Chicago/Turabian StyleWang, Hung-Tsung, Hsia-Ling Tai, Chia-Chen Yang, and Yung-Sheng Chen. 2020. "Acute Effects of Self-Selected Music Intervention on Golf Performance and Anxiety Level in Collegiate Golfers: A Crossover Study" International Journal of Environmental Research and Public Health 17, no. 20: 7478. https://doi.org/10.3390/ijerph17207478
APA StyleWang, H.-T., Tai, H.-L., Yang, C.-C., & Chen, Y.-S. (2020). Acute Effects of Self-Selected Music Intervention on Golf Performance and Anxiety Level in Collegiate Golfers: A Crossover Study. International Journal of Environmental Research and Public Health, 17(20), 7478. https://doi.org/10.3390/ijerph17207478