Correlation of COVID-19 Pandemic with Healthcare System Response and Prevention Measures in Saudi Arabia

 ,
,  and
and 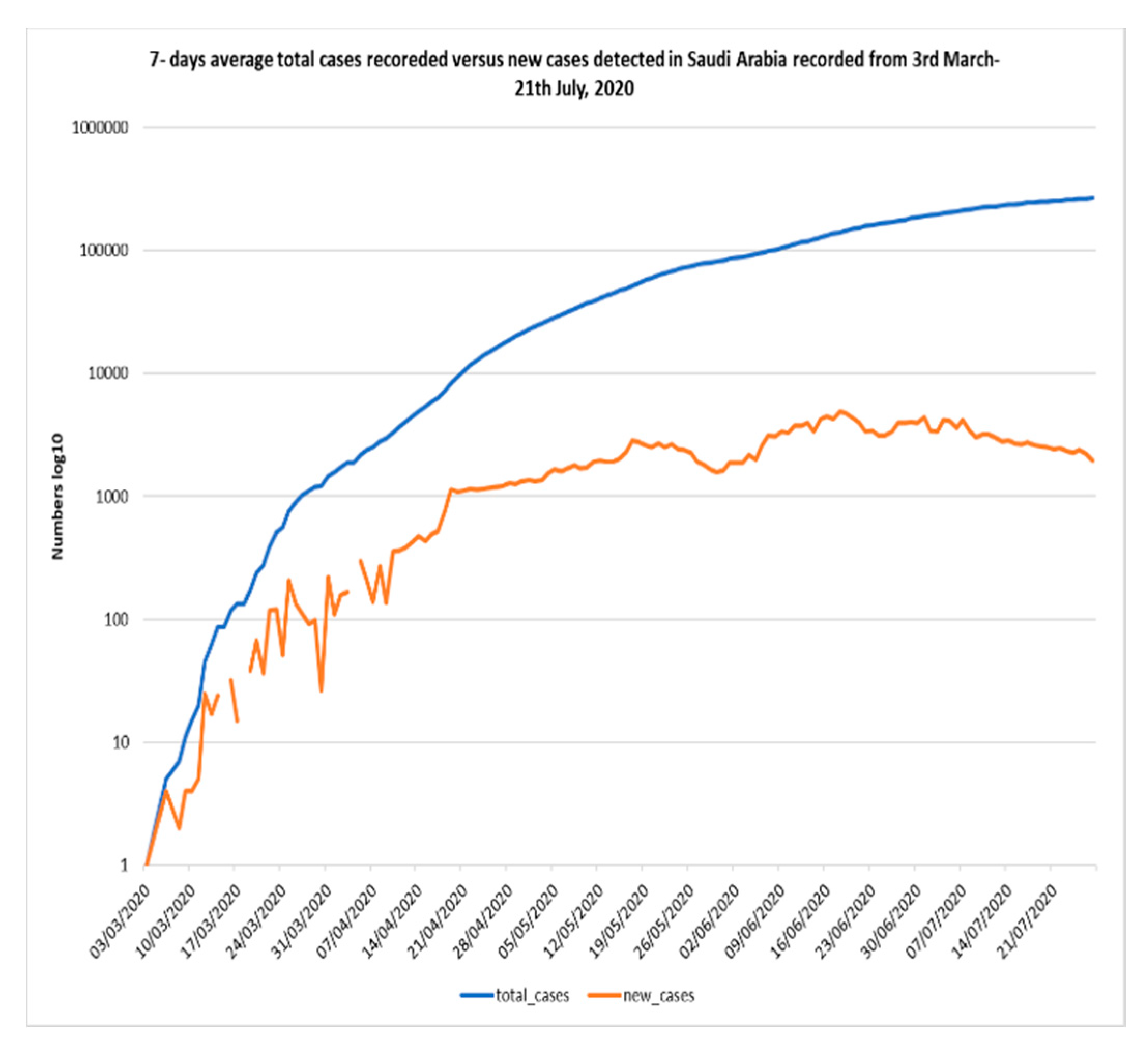{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
1.1. Demographics and COVID-19 Cases
1.2. Healthcare Availability and COVID-19 Scattering
1.3. COVID-19 Epidemiology
1.4. Prevention Measures and COVID-19
2. Materials and Methods
2.1. Demography and Patterns of Contact across Saudi Arabia
2.2. Community Prevention Program
2.3. Study Limitations
2.4. Statistical Analysis
3. Results and Discussion
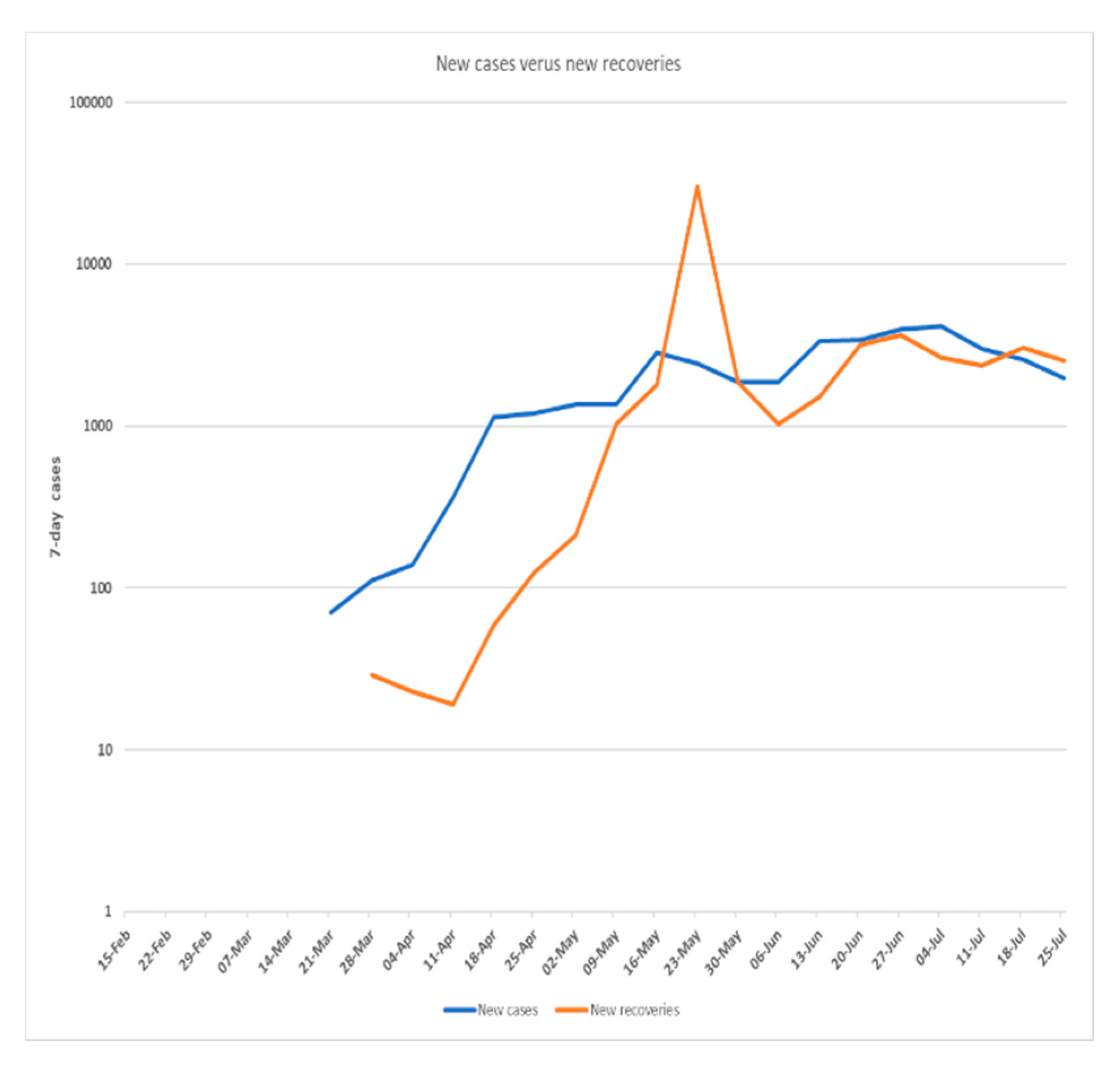
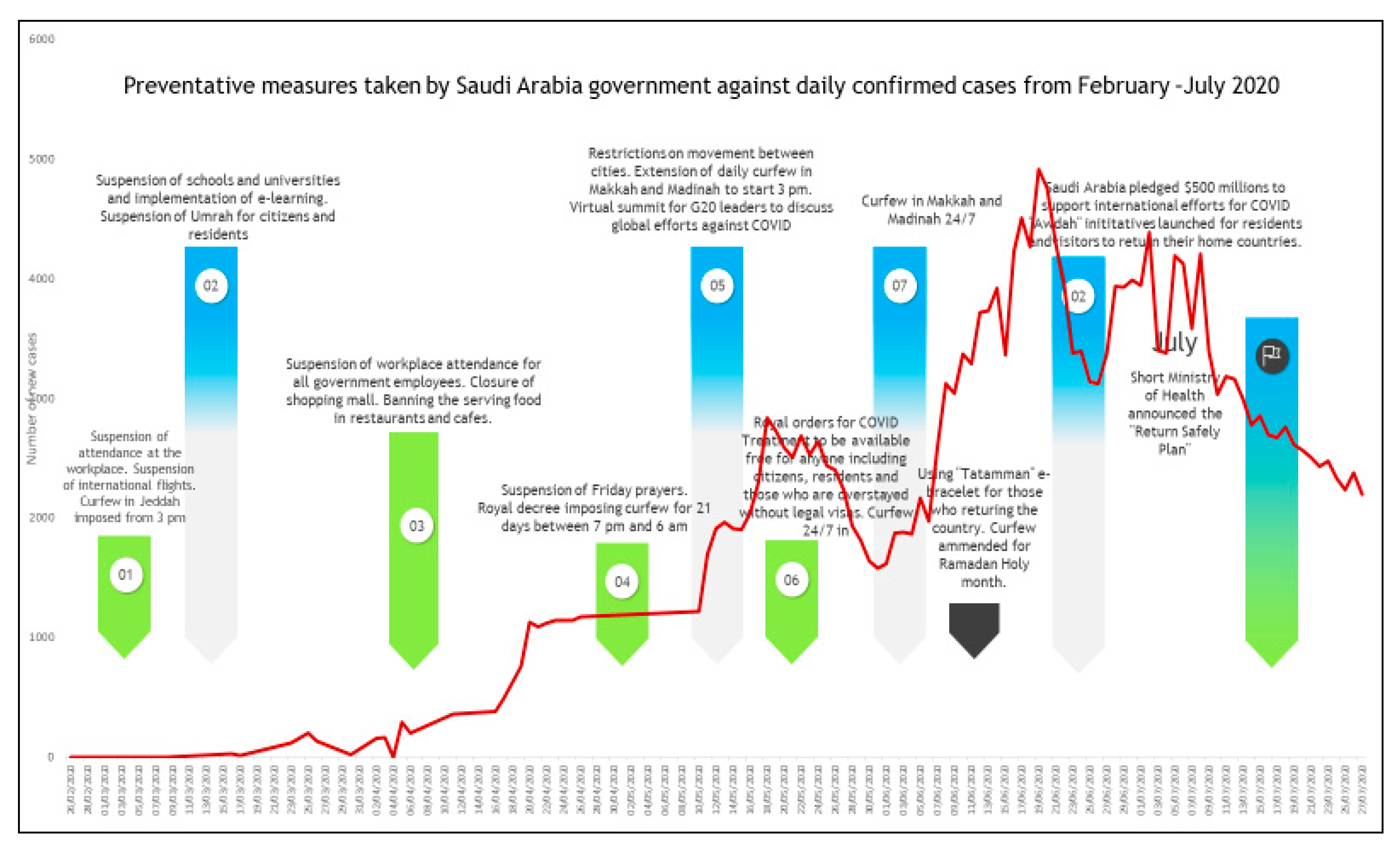
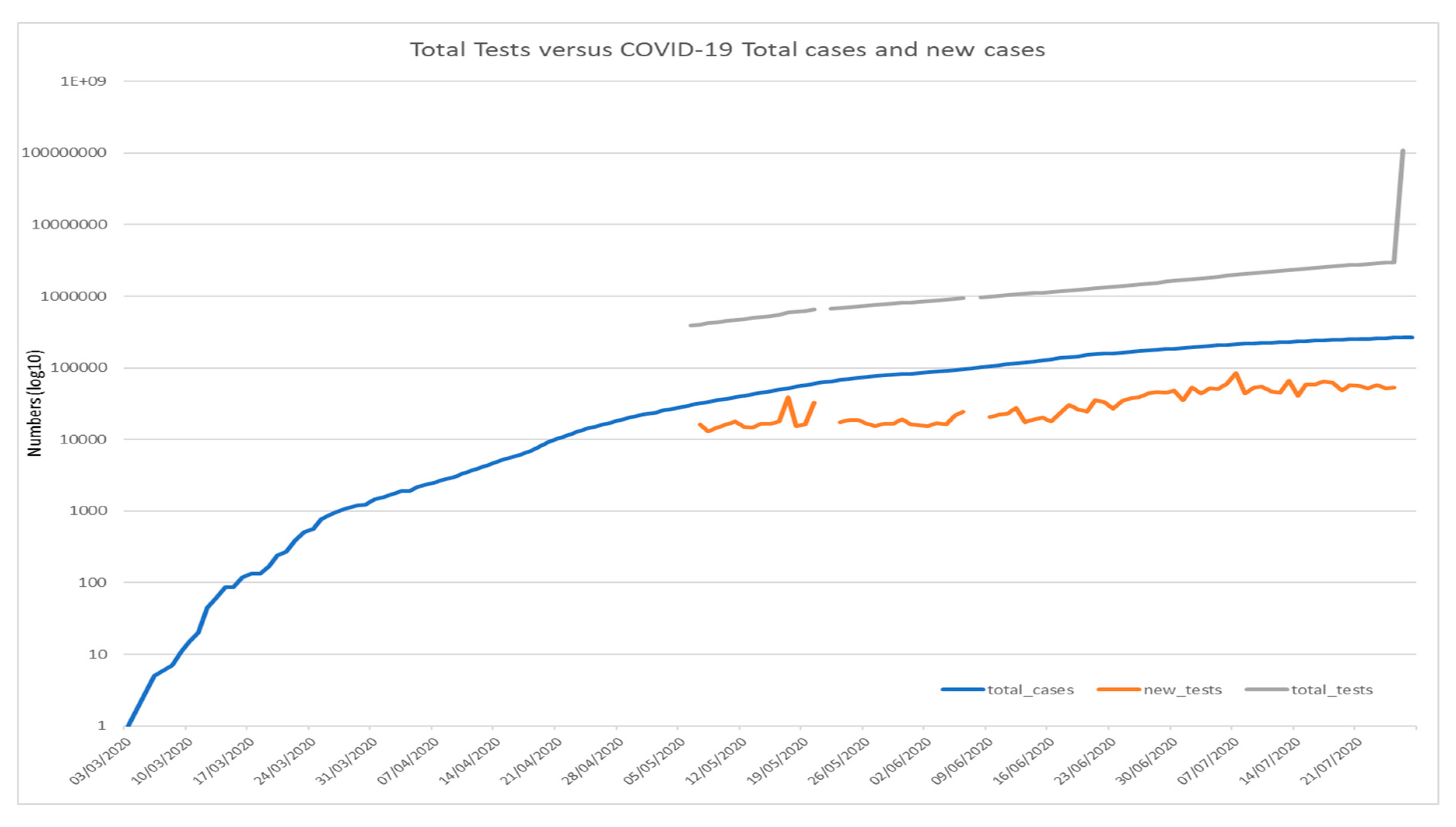
3.1. Correlations between Prevention Measures and Number of Cases
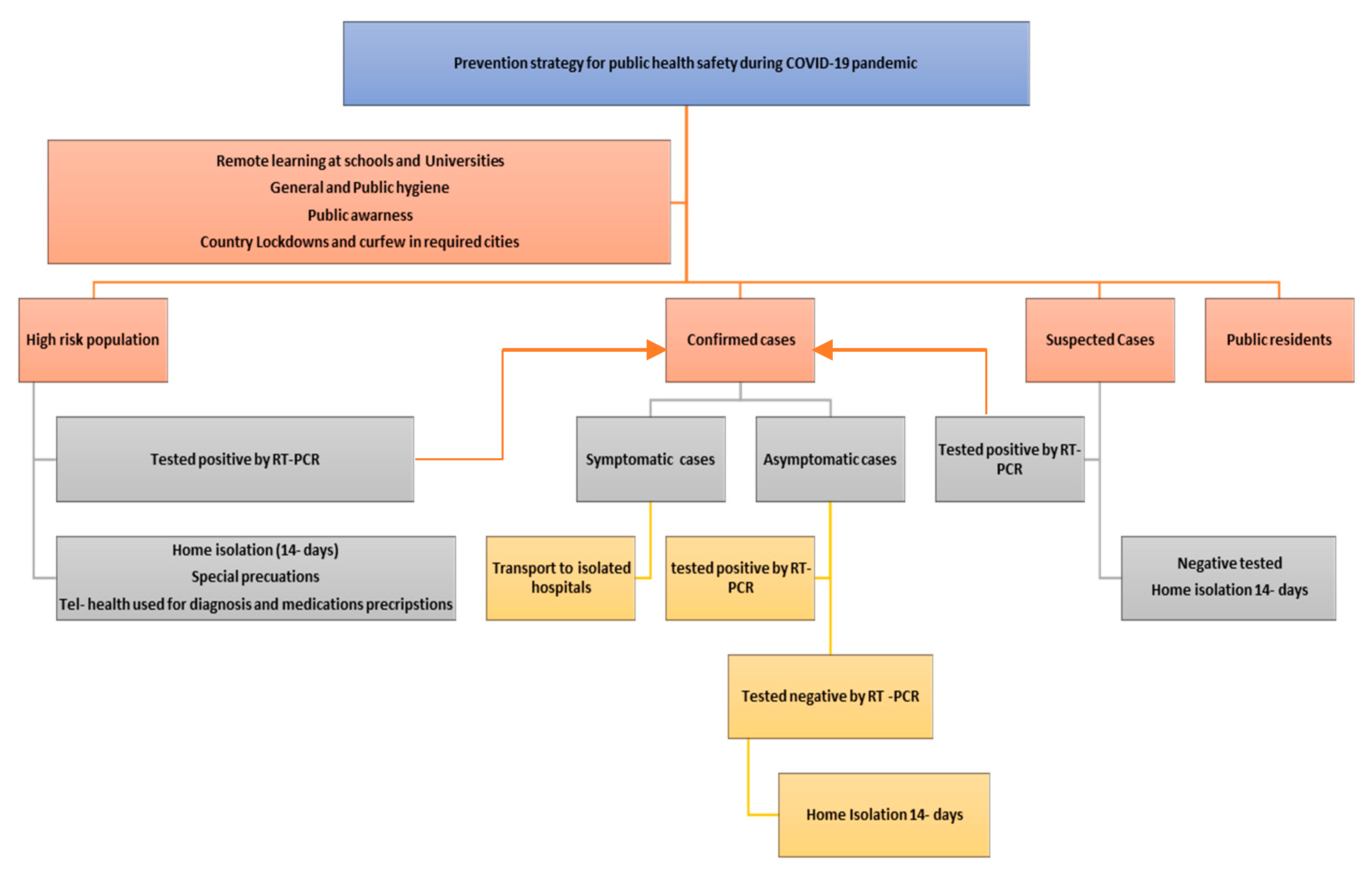
3.2. Suggested COVID-19 Prevention Measures Strategy for the Saudi Arabian Community
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- WHO. Novel Coronavirus—China; WHO: Geneva, Switzerland, 2020; Available online: http://www.who.int/csr/don/12-January-2020-novel-coronavirus-china/en/ (accessed on 19 January 2020).
- WHO. Coronavirus Situation Report-184; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Saudi Center for Disease Control and Prevention (CDC). Saudi Arabia Fact Sheet; Saudi Center for Disease Control and Prevention (CDC): Riyadh, Saudi Arabia, October 2019.
- Verity, R.; Okell, L.C.; Dorigatti, I.; Winskill, P.; Whittaker, C.; Imai, N.; Dighe, A. Estimates of the severity of COVID-19 disease. Lancet Infect. Dis. 2020, in press. [Google Scholar]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Guan, L. Articles Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1–9. [Google Scholar] [CrossRef]
- WHO. Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19); WHO: Geneva, Switzerland, 2020; Available online: https://www.who.int/publications-detail/report-of-the-who-china-joint-mission-on-coronavirus-disease-2019-(covid-19) (accessed on 22 March 2020).
- Saudi Ministry of Health. Annual Statistics Books; Saudi Ministry of Health: Riyadh, Saudi Arabia, 2019.
- Ministry of Health, National Health Laboratory. The Minister of Health to Launch the National Health Laboratory in Riyadh Next Sunday. Available online: https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2015-03-25-002.aspx (accessed on 25 March 2020).
- Ferguson, N.; Laydon, D.; Nedjati Gilani, G.; Imai, N.; Ainslie, K.; Baguelin, M.; Dighe, A. Impact of Non-Pharmaceutical Interventions (NPIs) to Reduce COVID-19 Mortality and Healthcare Demand; Springer: Berlin, Germany, 2020. [Google Scholar] [CrossRef]
- Walker, P.; Whittaker, C.; Watson, O.; Baguelin, M.; Ainslie, K.; Bhatia, S.; Cucunuba Perez, Z. The Global Impact of COVID-19 and Strategies for Mitigation and Suppression; Imperial College London: London, UK, 2020. [Google Scholar] [CrossRef]
- Saudi Center for Disease Prevention and Control (SCDC). (Covid-19) Disease Interactive Dashboard. Available online: https://covid19.cdc.gov.sa/daily-updates/ (accessed on 25 March 2020).
- Ian, A. Kingdom of Saudi Arabia Healthcare overview. In The Pulse, 8th ed.; Colliers International MENA: Toronto, Canada, 2018. [Google Scholar]
- WHO. Coronavirus Disease 2019 (COVID-19); Situation Report; WHO: Geneva, Switzerland, 2020; p. 24. [Google Scholar]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef]
- Zhonghua, L.; Xing, B.; Xue, Z.Z. The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China. Chin. J. Epidemiol. 2020, 41, 145–151. [Google Scholar]
- Watson, O.J.; FitzJohn, R.; Eaton, J.W. rdhs: An R package to interact with The Demographic and Health Surveys (DHS) Program datasets. Wellcome Open Res. 2019, 4, 103. [Google Scholar] [CrossRef]
- Zhang, L.; Tao, Y.; Shen, M.; Fairley, C.K.; Guo, Y. Can self-imposed prevention measures mitigate the COVID-19 epidemic? PLoS Med. 2020, 17, e1003240. [Google Scholar] [CrossRef]
- Alsofayan, Y.M.; Althunayyan, S.M.; Khan, A.A.; Hakawi, A.M.; Assiri, A.M. Clinical characteristics of COVID-19 in Saudi Arabia: A national retrospective study. J. Infect. Public Health 2020. [Google Scholar] [CrossRef]
- Li, L.; Wong, J.Y.; Wu, P.; Bond, H.S.; Lau, E.H.; Sullivan, S.G.; Cowling, B.J. Heterogeneity in estimates of the impact of influenza on population mortality: A systematic review. Am. J. Epidemiol. 2018, 187, 378–388. [Google Scholar] [CrossRef]
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Xing, X. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- Lipsitch, M. Will COVID-19 Go Away on Its Own in Warmer Weather? Center for Communicable Disease Dynamics (CCDD) at the Harvard, T.H. Chan School of Public Health: Boston, MA, USA, 2020; Available online: https://ccdd.hsph.harvard.edu/will-covid-19-go-away-on-its-own-in-warmer-weather/ (accessed on 5 March 2020).
- Boëlle, P.Y.; Ansart, S.; Cori, A.; Valleron, A.J. Transmission parameters of the A/H1N1 (2009) influenza virus pandemic: A review. Influenza Other Respir. Viruses 2011, 5, 306–316. [Google Scholar] [CrossRef]
- Anderson, R.M.; Heesterbeek, H.; Klinkenberg, D.; Hollingsworth, D.T. How Will Country-Based Mitigation Measures Influence the Course of the COVID-19 Epidemic? Lancet 2020. [Google Scholar] [CrossRef]
- The Novel Coronavirus Pneumonia Emergency Response Epidemiology Team. The Epidemiological Characteristics of an Outbreak of 2019 Novel Coronavirus Disease (COVD-19). China CDC Wkly. 2020, 2, 113–122. [Google Scholar]
- Elston, J.W.; Cartwright, C.; Ndumbi, P.; Wright, J. The health impact of the 2014–15 Ebola outbreak. Public Health 2017, 143, 60–70. [Google Scholar] [CrossRef] [PubMed]
- Ives, A.R.; Bozzuto, C. State-by-State estimates of R0 at the start of COVID-19 outbreaks in the USA; preprint. medRxiv 2020. [Google Scholar] [CrossRef]
- National Bureau of Statistics of China. Preliminary Results of Gross Domestic Product (GDP) for the First Quarter of 2020. Available online: http://www.stats.gov.cn/tjsj/zxfb/202004/t20200417_1739602.html (accessed on 10 May 2020).
- WHO. COVID-19: Surveilllance, case investigation and epidemiological protocols. In Surveillance Strategies For COVID-19 Human Infection; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Abdelhafiz, A.S.; Mohammed, Z.; Ibrahim, M.E.; Ziady, H.H.; Alorabi, M.; Ayyad, M.; Sultan, E.A. Knowledge, Perceptions, and Attitude of Egyptians Towards the Novel Coronavirus Disease (COVID-19). J. Community Health 2020, 45, 881–890. [Google Scholar] [CrossRef] [PubMed]
- Wolf, M.S.; Serper, M.; Opsasnick, L.; O’Conor, R.M.; Curtis, L.M.; Benavente, J.Y.; Russell, A. Awareness, Attitudes, and Actions Related to COVID-19 Among Adults With Chronic Conditions at the Onset of the US Outbreak: A Cross-sectional Survey. Ann. Intern Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Garg, S.; Kim, L.; Whitaker, M. Hospitalization Rates and Characteristics of Patients Hospitalized with Laboratory-Confirmed Coronavirus Disease 2019—COVID-NET, 14 States, March 1–30, 2020; MMWR Morbility and Mortality Weekly Report; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2020; Volume 69, pp. 458–464.
- Zhang, L.; Shen, M.; Ma, X.; Su, S.; Gong, W.; Wang, J.; Li, W. What is required to prevent a second major outbreak of SARS-CoV-2 upon lifting the quarantine of Wuhan city, China. Innovation 2020, 1, 100006. [Google Scholar] [CrossRef]
- Limaye, R.J.; Sauer, M.; Ali, J.; Bernstein, J.; Wahl, B.; Barnhill, A.; Labrique, A. Building trust while influencing online COVID-19 content in the social media world. Lancet Digit. Health 2020. [Google Scholar] [CrossRef]
- Offeddu, V.; Yung, C.F.; Low, M.S.F.; Tam, C.C. Effectiveness of Masks and Respirators Against Respiratory Infections in Healthcare Workers: A Systematic Review and Meta-Analysis. Clin. Infect Dis. 2017, 65, 1934–1942. [Google Scholar] [CrossRef]
- Wang, X.; Pan, Z.; Cheng, Z. Association between 2019-nCoV transmission and N95 respirator use. J. Hosp. Infect. 2020. [Google Scholar] [CrossRef]
- Kwok, Y.L.; Gralton, J.; McLaws, M.L. Face touching: A frequent habit that has implications for hand hygiene. Am. J. Infect. Control. 2015, 43, 112–114. [Google Scholar] [CrossRef] [PubMed]
- Shen, M.; Peng, Z.; Guo, Y.; Rong, L.; Li, Y.; Xiao, Y.; Zhang, L. Assessing the Effects of Metropolitan-Wide Quarantine on the Spread of COVID-19 in Public Space and Households. Int. J. Infect Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Cirrincione, L.; Plescia, F.; Ledda, C.; Rapisarda, V.; Martorana, D.; Moldovan, R.E.; Cannizzaro, E. COVID-19 Pandemic: Prevention and Protection Measures to Be Adopted at the Workplace. Sustainability 2020, 12, 3603. [Google Scholar] [CrossRef]
- Wang, X.; Pasco, R.F.; Du, Z.; Petty, M.; Fox, S.J.; Galvani, A.P.; Meyers, L.A. Impact of Social Distancing Measures on Coronavirus Disease Healthcare Demand, Central Texas, USA. Emerg. Infect. Dis. 2020, 26. [Google Scholar] [CrossRef] [PubMed]
- United Nations. World Population Prospects 2019; Department of Economic Social Population Affairs and Dynamic. Available online: https://population.un.org/wpp (accessed on 5 August 2020).
- Regional Social Development Council. Available online: http://github.com/sociolmix (accessed on 5 August 2020).
- Saudi Ministry of Health. Statistical Yearbook of 2018; Saudi Ministry of Health: Riyadh, Saudi Arabia, 2018.
- Saudi Ministry of Health. Hajj Statistics for 2019; Saudi Ministry of Health: Riyadh, Saudi Arabia, 2019.
- University of Oxford; Oxford Martin School. Our World Data. Available online: https://ourworldindata.org/coronavirus-source-data (accessed on 5 August 2020).
- Abdullah, A.; Algaissi, N.K.; Mazen, H.; Anwar, M. Preparedness and response to COVID-19 in Saudi Arabia: Building on MERS experience. J. Infect. Public Health 2020. [Google Scholar] [CrossRef]
- Kevin, S.; Thomas, V. Rt COVID-19. Probabilistic Programming in Python. Available online: https://rt.live/ (accessed on 5 August 2020).
- WHO. COVID-19 Preparedness and Response Progress Report; COVID-19: February–June Progress Report; WHO: Geneva, Switzerland, 2020. [Google Scholar]
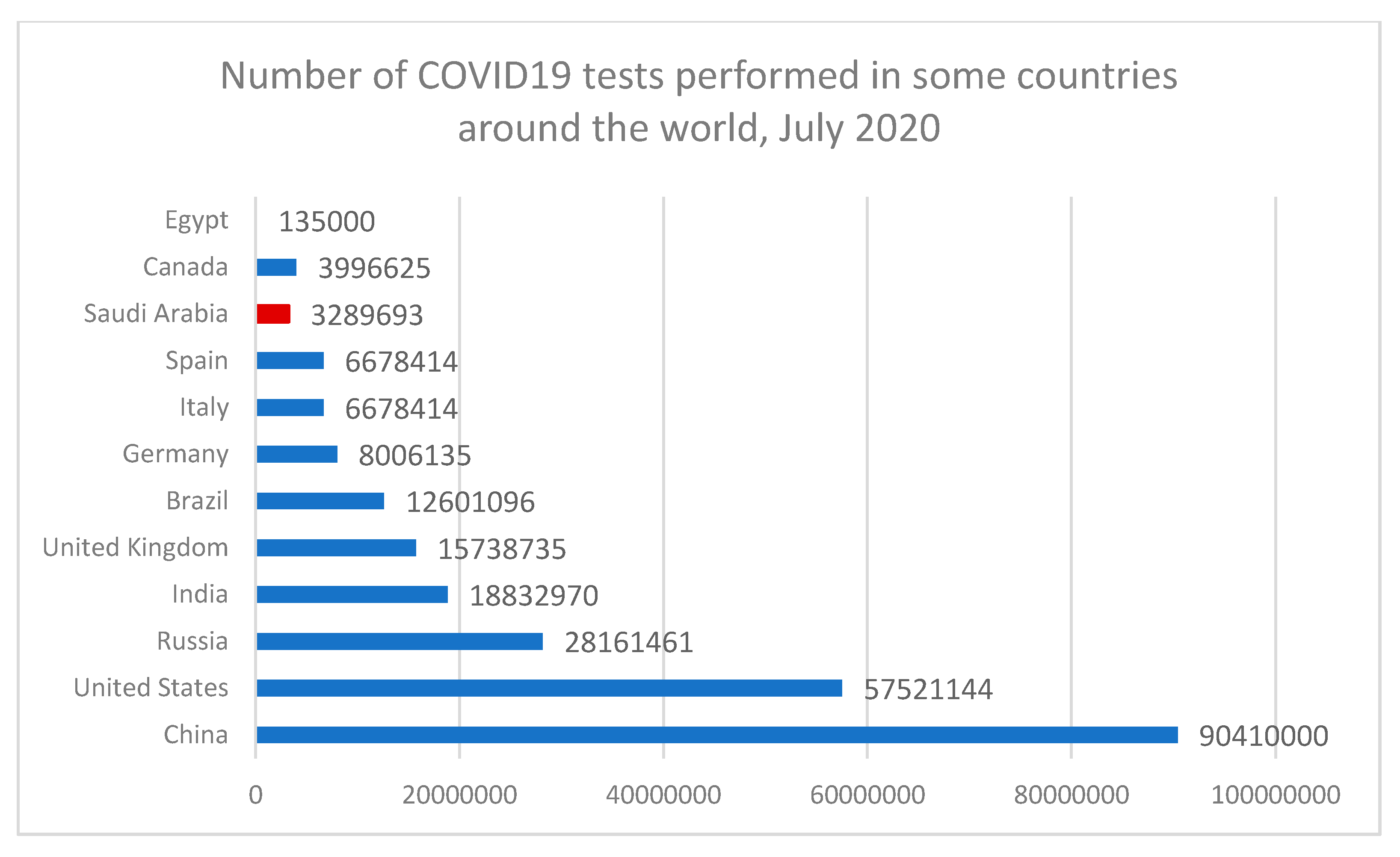
- John, E. Number of Tests for COVID-19 in Most Impacted Countries Worldwide as of July 31, 2020. Available online: https://www.statista.com/statistics/1028731/covid19-tests-select-countries-worldwide/ (accessed on 5 August 2020).
- Harpreet, S.; Tarun, P. Stopping the SARS-CoV-2 surge in the USA-CDC recommendations and ground realities. Adv. Respir. Med. 2020, 88, 173–175. [Google Scholar] [CrossRef]
- Zhang, X.M.; Zhou, H.E.; Zhang, W.W.; Dou, Q.L.; Li, Y.; Wei, J.; Cheng, A.S. Assessment of Coronavirus Disease 2019 Community Containment Strategies in Shenzhen, China. JAMA Netw. Open 2020, 3, e2012934. [Google Scholar] [CrossRef]
- Francesco Di, G.; Damiano, P.; Claudia, M.; Mario, A.; Vincenzo, R.; Nicola, V.; Lee, S. Coronavirus Diseases (COVID-19) Current Status and Future Perspectives: A Narrative Review. Int. J. Environ. Res. Public Health 2020, 17, 2690. [Google Scholar] [CrossRef]







© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adly, H.M.; AlJahdali, I.A.; Garout, M.A.; Khafagy, A.A.; Saati, A.A.; Saleh, S.A.K. Correlation of COVID-19 Pandemic with Healthcare System Response and Prevention Measures in Saudi Arabia. Int. J. Environ. Res. Public Health 2020, 17, 6666. https://doi.org/10.3390/ijerph17186666
Adly HM, AlJahdali IA, Garout MA, Khafagy AA, Saati AA, Saleh SAK. Correlation of COVID-19 Pandemic with Healthcare System Response and Prevention Measures in Saudi Arabia. International Journal of Environmental Research and Public Health. 2020; 17(18):6666. https://doi.org/10.3390/ijerph17186666
Chicago/Turabian StyleAdly, Heba M., Imad A. AlJahdali, Mohammed A. Garout, Abdullah A. Khafagy, Abdulla A. Saati, and Saleh A. K. Saleh. 2020. "Correlation of COVID-19 Pandemic with Healthcare System Response and Prevention Measures in Saudi Arabia" International Journal of Environmental Research and Public Health 17, no. 18: 6666. https://doi.org/10.3390/ijerph17186666
APA StyleAdly, H. M., AlJahdali, I. A., Garout, M. A., Khafagy, A. A., Saati, A. A., & Saleh, S. A. K. (2020). Correlation of COVID-19 Pandemic with Healthcare System Response and Prevention Measures in Saudi Arabia. International Journal of Environmental Research and Public Health, 17(18), 6666. https://doi.org/10.3390/ijerph17186666